
Development of a Medium Care Unit Using an Inexperienced Respiratory Staff: Lessons Learned during the COVID-19 Pandemic

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Methods
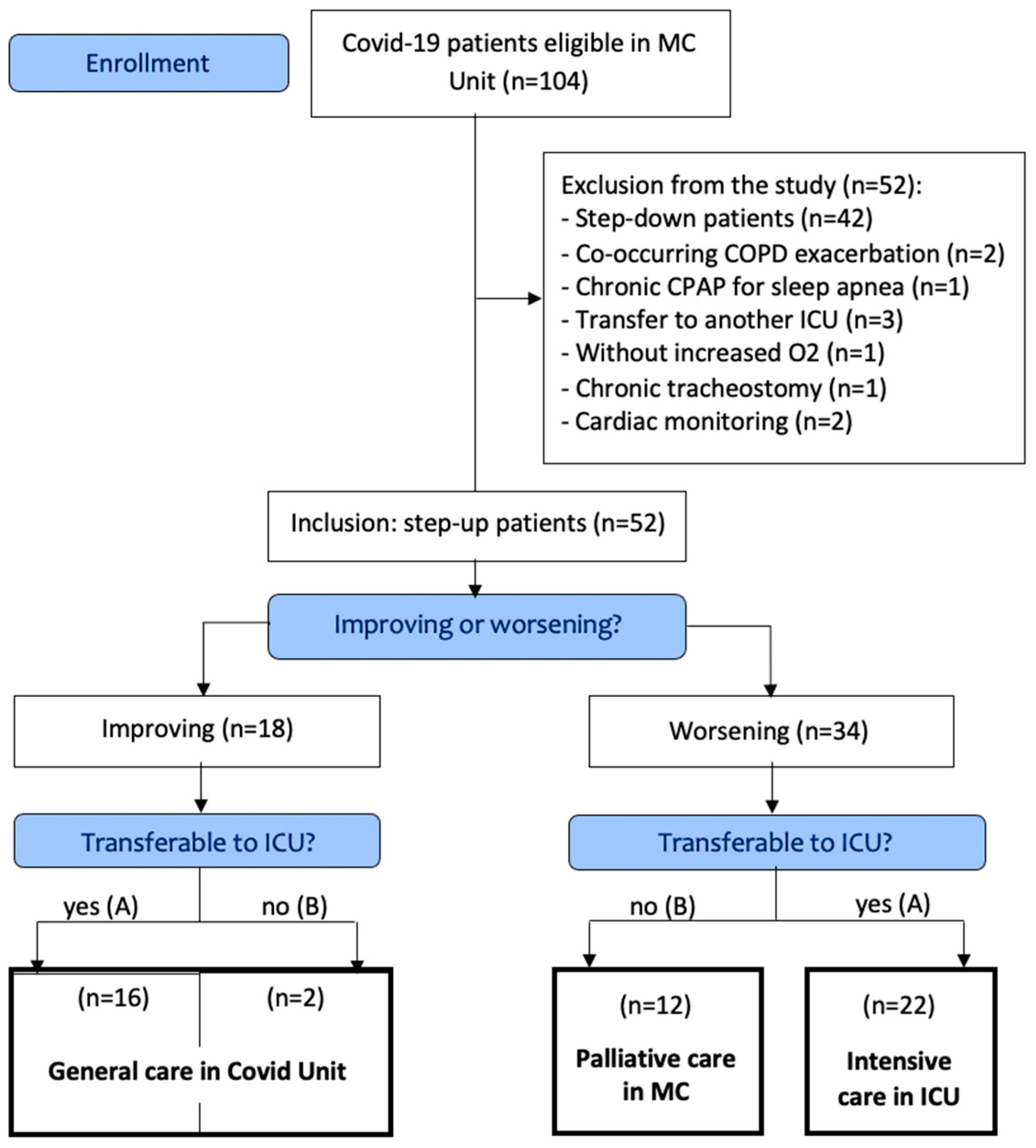
2.1. Population
2.2. Outcomes
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
3.1. Clinical Evolution
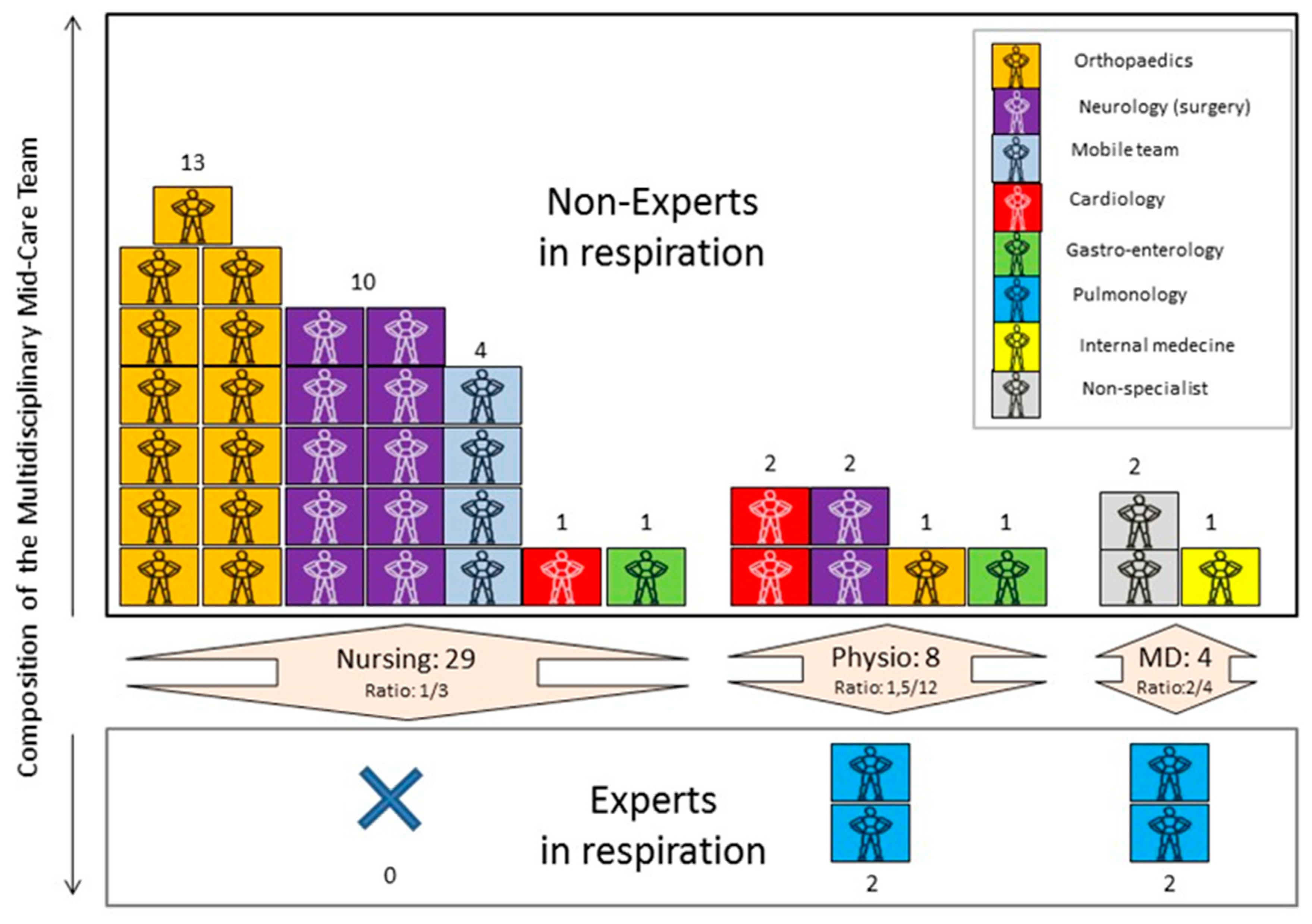
3.2. Establishment of the MC Unit
3.3. Training of the Clinicians
4. Discussion
4.1. General Discussion
4.2. Organizational Description
4.3. Communication and Cooperation
4.4. Training
4.5. Palliative Care
4.6. Perpsectives
4.7. Current Limitations of MCs
4.8. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 18 May 2022).
- Gabutti, G.; d’Anchera, E.; Sandri, F.; Savio, M.; Stefanati, A. Coronavirus: Update Related to the Current Outbreak of COVID-19. Infect. Dis. Ther. 2020, 9, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Novel Coronavirus COVID-19 (2019-NCoV) Data Repository by Johns Hopkins CSSE. 2019. Available online: https://github.com/CSSEGISandData/COVID-19 (accessed on 15 May 2022).
- Moghadas, S.M.; Vilches, T.N.; Zhang, K.; Wells, C.R.; Shoukat, A.; Singer, B.H.; Meyers, L.A.; Neuzil, K.M.; Langley, J.M.; Fitzpatrick, M.C.; et al. The Impact of Vaccination on Coronavirus Disease 2019 (COVID-19) Outbreaks in the United States. Clin. Infect. Dis. 2021, 73, 2257–2264. [Google Scholar] [CrossRef] [PubMed]
- Tzotzos, S.J.; Fischer, B.; Fischer, H.; Zeitlinger, M. Incidence of ARDS and Outcomes in Hospitalized Patients with COVID-19: A Global Literature Survey. Crit. Care 2020, 24, 516. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.E.; Patel, N.G.; Levy, M.A.; Storeygard, A.; Balk, D.; Gittleman, J.L.; Daszak, P. Global Trends in Emerging Infectious Diseases. Nature 2008, 451, 990–993. [Google Scholar] [CrossRef] [PubMed]
- Piot, P.; Spencer, J. Towards Societies Living with COVID-19. China CDC Wkly. 2021, 3, 144–145. [Google Scholar] [CrossRef]
- COVID-19 Map. Available online: https://coronavirus.jhu.edu/map.html (accessed on 18 May 2021).
- Alviset, S.; Riller, Q.; Aboab, J.; Dilworth, K.; Billy, P.-A.; Lombardi, Y.; Azzi, M.; Ferreira Vargas, L.; Laine, L.; Lermuzeaux, M.; et al. Continuous Positive Airway Pressure (CPAP) Face-Mask Ventilation Is an Easy and Cheap Option to Manage a Massive Influx of Patients Presenting Acute Respiratory Failure during the SARS-CoV-2 Outbreak: A Retrospective Cohort Study. PLoS ONE 2020, 15, e0240645. [Google Scholar] [CrossRef]
- Rabec, C.; Gonzalez-Bermejo, J.; Respiratory Support Chronic Care Group AVO2 of the French Society of Respiratory Diseases SPLF. GAVO2 collaborators Respiratory Support in Patients with COVID-19 (Outside Intensive Care Unit). A Position Paper of the Respiratory Support and Chronic Care Group of the French Society of Respiratory Diseases. Respir Med. Res. 2020, 78, 100768. [Google Scholar] [CrossRef]
- Oranger, M.; Gonzalez-Bermejo, J.; Dacosta-Noble, P.; Llontop, C.; Guerder, A.; Trosini-Desert, V.; Faure, M.; Raux, M.; Decavele, M.; Demoule, A.; et al. Continuous Positive Airway Pressure to Avoid Intubation in SARS-CoV-2 Pneumonia: A Two-Period Retrospective Case-Control Study. Eur. Respir. J. 2020, 56, 2001692. [Google Scholar] [CrossRef]
- Brusasco, C.; Corradi, F.; Di Domenico, A.; Raggi, F.; Timossi, G.; Santori, G.; Brusasco, V.; Galliera CPAP-COVID-19 Study Group. Continuous Positive Airway Pressure in COVID-19 Patients with Moderate-to-Severe Respiratory Failure. Eur. Respir. J. 2021, 57, 2002524. [Google Scholar] [CrossRef]
- Beck, D.H.; McQuillan, P.; Smith, G.B. Waiting for the Break of Dawn? The Effects of Discharge Time, Discharge TISS Scores and Discharge Facility on Hospital Mortality after Intensive Care. Intensive Care Med. 2002, 28, 1287–1293. [Google Scholar] [CrossRef]
- Lekwijit, S.; Chan, C.W.; Green, L.V.; Liu, V.X.; Escobar, G.J. The Impact of Step-Down Unit Care on Patient Outcomes After ICU Discharge. Crit. Care Explor. 2020, 2, e0114. [Google Scholar] [CrossRef] [PubMed]
- Grosgurin, O.; Leidi, A.; Farhoumand, P.D.; Carballo, S.; Adler, D.; Reny, J.-L.; Pinto, B.B.; Rossel, A.; Serratrice, J.; Agoritsas, T.; et al. Role of Intermediate Care Unit Admission and Noninvasive Respiratory Support during the COVID-19 Pandemic: A Retrospective Cohort Study. Respiration 2021, 100, 786–793. [Google Scholar] [CrossRef] [PubMed]
- González-Calle, D.; Villacorta, E.; Sánchez-Serrano, A.; León, M.; Sanchez, P.L. Coronavirus Disease 2019 Intermediate Care Units: Containing Escalation of ICUs. Crit. Care Med. 2020, 48, e1372–e1374. [Google Scholar] [CrossRef] [PubMed]
- Higgins, V.; Sohaei, D.; Diamandis, E.P.; Prassas, I. COVID-19: From an Acute to Chronic Disease? Potential Long-Term Health Consequences. Crit. Rev. Clin. Lab. Sci. 2021, 58, 297–310. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V.; WHO Clinical Case Definition Working Group on Post-COVID-19 Condition. A Clinical Case Definition of Post-COVID-19 Condition by a Delphi Consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Stefano, G.B.; Büttiker, P.; Weissenberger, S.; Ptacek, R.; Wang, F.; Esch, T.; Bilfinger, T.V.; Kream, R.M. Biomedical Perspectives of Acute and Chronic Neurological and Neuropsychiatric Sequelae of COVID-19. Curr. Neuropharmacol. 2021, 20, 1229–1240. [Google Scholar] [CrossRef]
- Fugazzaro, S.; Contri, A.; Esseroukh, O.; Kaleci, S.; Croci, S.; Massari, M.; Facciolongo, N.C.; Besutti, G.; Iori, M.; Salvarani, C.; et al. Rehabilitation Interventions for Post-Acute COVID-19 Syndrome: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 5185. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Azoulay, E.; Al-Dorzi, H.M.; Phua, J.; Salluh, J.; Binnie, A.; Hodgson, C.; Angus, D.C.; Cecconi, M.; Du, B.; et al. How the COVID-19 Pandemic Will Change the Future of Critical Care. Intensive Care Med. 2021, 47, 282–291. [Google Scholar] [CrossRef]
- Simpson, S.; Kaufmann, M.C.; Glozman, V.; Chakrabarti, A. Disease X: Accelerating the Development of Medical Countermeasures for the next Pandemic. Lancet Infect. Dis. 2020, 20, e108–e115. [Google Scholar] [CrossRef] [Green Version]
- Medrinal, C.; Gillet, A.; Boujibar, F.; Dugernier, J.; Zwahlen, M.; Lamia, B.; Girault, C.; Creteur, J.; Fellrath, J.-M.; Haesler, L.; et al. Role of Non-Invasive Respiratory Supports in COVID-19 Acute Respiratory Failure Patients with Do Not Intubate Orders. J. Clin. Med. 2021, 10, 2783. [Google Scholar] [CrossRef]
- Zhan, H.; Chen, H.; Liu, C.; Cheng, L.; Yan, S.; Li, H.; Li, Y. Diagnostic Value of D-Dimer in COVID-19: A Meta-Analysis and Meta-Regression. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211010976. [Google Scholar] [CrossRef] [PubMed]
- LOI-WET. Available online: https://www.ejustice.just.fgov.be/cgi_loi/change_lg.pl?language=fr&la=F&cn=1998042740&table_name=loi (accessed on 18 May 2021).
- von Leupoldt, A. Treating Anxious Expectations Can Improve Dyspnoea in Patients with COPD. Eur. Respir. J. 2017, 50, 1701352. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Boutmy-Deslandes, E.; Perbet, S.; Mongardon, N.; Dres, M.; Razazi, K.; Guerot, E.; Terzi, N.; Andrivet, P.; Alves, M.; et al. Differential Perceptions of Noninvasive Ventilation in Intensive Care among Medical Caregivers, Patients, and Their Relatives: A Multicenter Prospective Study-The PARVENIR Study. Anesthesiology 2016, 124, 1347–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, H.M.; Huniche, L.; Titlestad, I.L. Involvement of Patients’ Perspectives on Treatment with Noninvasive Ventilation in Patients with Chronic Obstructive Pulmonary Disease-A Qualitative Study. J. Clin. Nurs. 2018, 27, e61–e69. [Google Scholar] [CrossRef] [Green Version]
- Mukhtar, S. Psychological Health during the Coronavirus Disease 2019 Pandemic Outbreak. Int. J. Soc. Psychiatry 2020, 66, 512–516. [Google Scholar] [CrossRef]
- Lee, S.M.; Kang, W.S.; Cho, A.-R.; Kim, T.; Park, J.K. Psychological Impact of the 2015 MERS Outbreak on Hospital Workers and Quarantined Hemodialysis Patients. Compr. Psychiatry 2018, 87, 123–127. [Google Scholar] [CrossRef]
- Hoyois, A.; Ballarin, A.; Thomas, J.; Lheureux, O.; Preiser, J.-C.; Coppens, E.; Perez-Bogerd, S.; Taton, O.; Farine, S.; Ouytsel, P.V.; et al. Nutrition Evaluation and Management of Critically Ill Patients with COVID-19 during Post–Intensive Care Rehabilitation. J. Parenter. Enter. Nutr. N/A 2021, 45, 1153–1163. [Google Scholar] [CrossRef]
- 20 Fiches Pratiques COVID 19—Disponibles En Téléchargement. Available online: https://www.sfncm.org/1212-fiches-covid-19-a-telecharger (accessed on 17 May 2021).
- Tulaimat, A.; Trick, W.E. DiapHRaGM: A Mnemonic to Describe the Work of Breathing in Patients with Respiratory Failure. PLoS ONE 2017, 12, e0179641. [Google Scholar] [CrossRef] [Green Version]
- Tobin, M.J. Why Physiology Is Critical to the Practice of Medicine: A 40-Year Personal Perspective. Clin. Chest Med. 2019, 40, 243–257. [Google Scholar] [CrossRef]
- Banzett, R.B.; O’Donnell, C.R.; Guilfoyle, T.E.; Parshall, M.B.; Schwartzstein, R.M.; Meek, P.M.; Gracely, R.H.; Lansing, R.W. Multidimensional Dyspnea Profile: An Instrument for Clinical and Laboratory Research. Eur. Respir. J. 2015, 45, 1681–1691. [Google Scholar] [CrossRef]
- Persichini, R.; Gay, F.; Schmidt, M.; Mayaux, J.; Demoule, A.; Morélot-Panzini, C.; Similowski, T. Diagnostic Accuracy of Respiratory Distress Observation Scales as Surrogates of Dyspnea Self-Report in Intensive Care Unit Patients. Anesthesiology 2015, 123, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Cates, C.J.; Welsh, E.J.; Rowe, B.H. Holding Chambers (Spacers) versus Nebulisers for Beta-Agonist Treatment of Acute Asthma. Cochrane Database Syst. Rev. 2013, 9, CD000052. [Google Scholar] [CrossRef] [Green Version]
- Rice, T.W.; Wheeler, A.P.; Bernard, G.R.; Hayden, D.L.; Schoenfeld, D.A.; Ware, L.B.; National Institutes of Health, National Heart, Lung, and Blood Institute ARDS Network. Comparison of the SpO2/FIO2 Ratio and the PaO2/FIO2 Ratio in Patients with Acute Lung Injury or ARDS. Chest 2007, 132, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Roca, O.; Messika, J.; Caralt, B.; García-de-Acilu, M.; Sztrymf, B.; Ricard, J.-D.; Masclans, J.R. Predicting Success of High-Flow Nasal Cannula in Pneumonia Patients with Hypoxemic Respiratory Failure: The Utility of the ROX Index. J. Crit. Care 2016, 35, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Plate, J.D.J.; Leenen, L.P.H.; Houwert, M.; Hietbrink, F. Utilisation of Intermediate Care Units: A Systematic Review. Crit. Care Res. Pract. 2017, 2017, 8038460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devroey, M.; Buyse, C.; Norrenberg, M.; Ros, A.-M.; Vincent, J.-L. Cardiorespiratory Physiotherapy around the Clock: Experience at a University Hospital. Physiother. Can. 2016, 68, 254–258. [Google Scholar] [CrossRef] [Green Version]
- Taccone, F.S.; Goethem, N.V.; Pauw, R.D.; Wittebole, X.; Blot, K.; Oyen, H.V.; Lernout, T.; Montourcy, M.; Meyfroidt, G.; Beckhoven, D.V. The Role of Organizational Characteristics on the Outcome of COVID-19 Patients Admitted to the ICU in Belgium. Lancet Reg. Health—Eur. 2021, 2, 100019. [Google Scholar] [CrossRef]
- Janssen, D.J.A.; Ekström, M.; Currow, D.C.; Johnson, M.J.; Maddocks, M.; Simonds, A.K.; Tonia, T.; Marsaa, K. COVID-19: Guidance on Palliative Care from a European Respiratory Society International Task Force. Eur. Respir. J. 2020, 56, 2002583. [Google Scholar] [CrossRef]
- Stroebe, M.; Schut, H. Bereavement in Times of COVID-19: A Review and Theoretical Framework. Omega 2021, 82, 500–522. [Google Scholar] [CrossRef]
- Akgün, K.M.; Shamas, T.L.; Feder, S.L.; Schulman-Green, D. Communication Strategies to Mitigate Fear and Suffering among COVID-19 Patients Isolated in the ICU and Their Families. Heart Lung 2020, 49, 344–345. [Google Scholar] [CrossRef]
- Beckl, R. Use of Helmet-Based Noninvasive Ventilation in Air Medical Transport of Coronavirus Disease 2019 Patients. Air Med. J. 2021, 40, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; Rubenfeld, G.D. Does Intermediate Care Improve Patient Outcomes or Reduce Costs? Crit Care 2015, 19, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| All Patients | ICU Transferable (A) | ICU Non-Transferable (B) | p-Value | |
|---|---|---|---|---|
| Patients, N [%] | 52 | 38 [73%] | 14 [27%] | / |
| Sex; female [%] | 25 [48%] | 31 [82%] | 8 [54%] | 0.148 |
| Age (years), mean (SD) | 65 (12) | 61 (11) | 75 (11) | <0.001 |
| BMI (kg/m2), mean (SD) | 27.4 (5) | 35 (5) | 26.9 (6) | 0.655 |
| Intubated, N [%] | 15 [29%] | 15 [39%] | 0 | / |
| Death, N [%] | 21 [40%] | 9 [24%] | 12 [86%] | <0.001 |
| COMORBIDITIES | ||||
| Comorbidities (10 points scale), mean (SD) | 1.9 (1.2) | 1.7 (1) | 2.5 (1.2) | 0.025 |
| CRF, N [%] | 12 [23%] | 8 [21%] | 4 [28%] | 0.842 |
| CHF, N [%] | 6 [12%] | 2 [5%] | 4 [28%] | 0.065 |
| ATH, N [%] | 33 [63%] | 21 [55%] | 12 [86%] | 0.089 |
| Diabetes, N [%] | 23 [44%] | 18 [47%] | 5 [36%] | 0.663 |
| Obesity, N [%] | 15 [29%] | 11 [29%] | 4 [28%] | 1 |
| Cancer, N [%] | 3 [6%] | 1 [3%] | 2 [14%] | 0.353 |
| Neuro., N [%] | 4 [8%] | 2 [5%] | 2 [14%] | 0.619 |
| Cognitive disorders, N [%] | 6 [12%] | 3 [8%] | 3 [21%] | 0.387 |
| Transplantation, N [%] | 6 [12%] | 5 [13%] | 1 [7%] | 0.910 |
| Respiratory disorders, N [%] | 16 [31%] | 7 [18%] | 9 [64%] | 0.004 |
| MEDICATIONS | ||||
| Remdesivir, N [%] | 7 [13%] | 5 [13%] | 2 [14%] | 1 |
| Tocilizumab, N [%] | 6 [11%] | 5 [13%] | 1 [7%] | 0.910 |
| Methylprednisolone, N [%] | 52 [100%] | 38 [100%] | 14 [100%] | 1 |
| Piperacillin/Tazobactam, N [%] | 20 [38%] | 14 [37%] | 6 [43%] | 0.941 |
| Meronem, N [%] | 4 [8%] | 3 [8%] | 1 [7%] | 1 |
| Amoxicillin, N [%] | 12 [23%] | 8 [21%] | 4 [28%] | 0.841 |
| Profession | N | Timetable | Original Department | Caregivers/Patients Ratio |
|---|---|---|---|---|
| Nurse | 29 | 24/7 | Orthopedic and ORL (n = 13) Neurology (n = 10) Mobile Team (n = 4) Cardiology (n = 1) Gastroenterology (n = 1) | 1/3 |
| Physiotherapists | 8 | 24/7 | Pneumology (n = 2) Cardiology (n = 2) Gastroenterology (n = 2) Neurology (n = 2) Orthopedic (n = 1) | 1.5/12 |
| Night physiotherapist | 2 per night | Night | Intensive Care Unit (n = 2) | 1 for ICU (30 beds) 1 for MC and COVID unit |
| Occupational therapist | 2 | Day | Neurology (n = 2) | 1/12 |
| Medical doctor | 5 | 24/7 | Pneumology (n = 2) Internal medicine (n = 1) Postgraduate (n = 2) | 2/4 |
| Psychologist | 2 | Day | / | / |
| Social worker | 2 | Day | / | / |
| Cleaning and maintenance | 1 | Day | / | / |
| Domain | Theme | Items | Theory | Demo. | Coaching | Video |
|---|---|---|---|---|---|---|
| Physiology | Respiratory system and anatomy | Lung, ventilation | X | |||
| Theoretical basis of ventilatory supports | CPAP, invasive and non-invasive ventilation | X | ||||
| Respiratory distress | Respiratory rate | Range [33] | X | X | X | |
| Use of accessory inspiratory muscles | Palpation of phasic contraction [34] | X | X | X | ||
| Paradoxical breathing | Visual and palpation [34] | X | X | X | ||
| Face examination | Fear, effort [34] | X | X | X | ||
| Respiratory pattern | Thoracoabdominal regularity [34] | X | X | X | ||
| Dyspnea | Communicating patient | Borg, part of MDP (work, air hunger) [35] | X | X | ||
| Non-communicating patient | IC-RDOS [36] | X | X | |||
| Respiratory support and Oxygenotherapy | HFNO | FiO2, flow | X | X | X | X |
| CPAP | Boussignac, Sleep apnea, Drager, Nasobuccal mask, helmet | X | X | X | X | |
| Hygiene | Aerosolizing procedure | X | X | X | X | |
| Aerosolized treatment [37] | X | X | X | X | ||
| Parameters | SPO2/FiO2 [38] | X | ||||
| ROX index [39] | X | |||||
| PAO2/FiO2 | X |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Hove, O.; Gillet, A.; Tack, J.; Reychler, G.; Guatteri, M.; Ballarin, A.; Thomas, J.; Espinoza, R.; Bonnier, F.; Norrenberg, M.; et al. Development of a Medium Care Unit Using an Inexperienced Respiratory Staff: Lessons Learned during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 7349. https://doi.org/10.3390/ijerph19127349
Van Hove O, Gillet A, Tack J, Reychler G, Guatteri M, Ballarin A, Thomas J, Espinoza R, Bonnier F, Norrenberg M, et al. Development of a Medium Care Unit Using an Inexperienced Respiratory Staff: Lessons Learned during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(12):7349. https://doi.org/10.3390/ijerph19127349
Chicago/Turabian StyleVan Hove, Olivier, Alexis Gillet, Jérôme Tack, Gregory Reychler, Magda Guatteri, Asuncion Ballarin, Justine Thomas, Rolando Espinoza, Frédéric Bonnier, Michelle Norrenberg, and et al. 2022. "Development of a Medium Care Unit Using an Inexperienced Respiratory Staff: Lessons Learned during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 12: 7349. https://doi.org/10.3390/ijerph19127349