
Von Willebrand Factor and ADAMTS-13 Are Associated with the Severity of COVID-19 Disease

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
- -
- Mild COVID-19:
- body temperature < 38 °C, cough, weakness, sore throat;
- absence of criteria for moderate and severe COVID-19.
- -
- Moderate COVID-19:
- body temperature > 38 °C;
- respiratory rate > 22 per minute;
- shortness of breath during physical exertion;
- changes in CT (radiography), typical of a viral lesion;
- SpO2 < 95%;
- serum CRP > 10 mg/L.
- -
- Severe COVID-19:
- respiratory rate > 30 per minute;
- SpO2 ≤ 93%;
- PaO2/FiO2 ≤ 300 mmHg;
- decreased level of consciousness, agitation;
- unstable hemodynamics (systolic blood pressure less than 90 mm Hg or diastolic blood pressure less than 60 mm Hg, diuresis less than 20 mL/hour)
- arterial blood lactate > 2 mmol/l;
- qSOFA > 2 points.
- National Medical Research Center for Obstetrics, Gynecology and Perinatology, named after Academician V.I.Kulakov of the Ministry of Healthcare of the Russian Federation, Moscow, Russia
- F.I. Inozemtsev City Clinical Hospital, Moscow, Russia
- A database containing information on 18 patients with a severe form of COVID-19 complicated by a feasibility study that was provided by Ataullakhanov Fazoil Inoyatovich (CTP FHF RAS, research work “Use of the Thrombodynamics test in COVID-19: identification of early predictors of the development of severe pneumonia and development of effective measures for its prevention”, registration number: AAAA-A20-120111090014-6) [14].
- Age over 18 years.
- Signed informed consent.
- For women: pregnancy or lactation.
- Hereditary deficiency of blood coagulation factors predisposing to hemorrhagic conditions.
- Purpura and other hemorrhagic conditions.
- Oncological diseases for the period of illness.
- Transplanted organs.
- HIV infection.
- Syphilis.
- Other acute infectious diseases.
- Continuous use of anticoagulants/antiplatelet agents.
- The need for surgery during COVID-19.
- Patient refusal to continue participation in the study.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dolgushina, N.V.; Krechetova, L.V.; Ivanets, T.Y.; Vtorushina, V.V.; Inviyaeva, E.V.; Sukhikh, G.T. The impact of the immune status on COVID- 19 severity. Akush. Ginekol. 2020, 9, 129–137. [Google Scholar] [CrossRef]
- Panigada, M.; Bottino, N.; Tagliabue, P.; Grasselli, G.; Novembrino, C.; Chantarangkul, V.; Pesenti, A.; Peyvandi, F.; Tripodi, A. Hypercoagulability of COVID-19 patients in intensive care unit: A report of thromboelastography findings and other parameters of hemostasis. J. Thromb. Haemost. 2020, 18, 1738–1742. [Google Scholar] [CrossRef] [PubMed]
- Beznoshchenko, O.S.; Shpilyuk, M.A.; Ivanets, T.Y.; Krechetova, L.V.; Pyregov, A.V.; Kodatsky, D.S.; Tavluyeva, E.V.; Melkumyan, A.R.; Gorodnova, E.A.; Dolgushina, N.V. Detection frequency and duration of lupus anticoagulant circulation in COVID-19 patients. Russ. J. Immunol. 2021, 24, 413–418. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Furlan, M.; Robles, R.; Solenthaler, M.; Wassmer, M.; Sandoz, P.; Lämmle, B. Deficient Activity of von Willebrand Factor–Cleaving Protease in Chronic Relapsing Thrombotic Thrombocytopenic Purpura. Blood 1997, 89, 3097–3103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, H.M.; Lian, E.C. Antibodies to von Willebrand factor-cleaving protease in acute thrombotic thrombocytopenic purpura. N. Engl. J. Med. 1998, 339, 1585–1594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neave, L.; Scully, M. Microangiopathic Hemolytic Anemia in Pregnancy. Transfus. Med. Rev. 2018, 32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Mancini, I.; Baronciani, L.; Artoni, A.; Colpani, P.; Biganzoli, M.; Cozzi, G.; Novembrino, C.; Boscolo Anzoletti, M.; De Zan, V.; Pagliari, M.T.; et al. The ADAMTS13-von Willebrand factor axis in COVID-19 patients. J. Thromb. Haemost. 2021, 19, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Bazzan, M.; Montaruli, B.; Sciascia, S.; Cosseddu, D.; Norbiato, C.; Roccatello, D. Low ADAMTS 13 plasma levels are predictors of mortality in COVID-19 patients. Intern. Emerg. Med. 2020, 15, 861–863. [Google Scholar] [CrossRef] [PubMed]
- Tiscia, G.L.; Favuzzi, G.; De Laurenzo, A.; Cappucci, F.; Fischetti, L.; di Mauro, L.; Miscio, G.; Mirijello, A.; Chinni, E.; Grandone, E. CSS COVID-19 Group. Reduction of ADAMTS13 Levels Predicts Mortality in SARS-CoV-2 Patients. TH open companion. J. Thromb. Haemost. 2020, 4, e203–e206. [Google Scholar] [CrossRef]
- Ono, T.; Mimuro, J.; Madoiwa, S.; Soejima, K.; Kashiwakura, Y.; Ishiwata, A.; Takano, K.; Ohmori, T.; Sakata, Y. Severe secondary deficiency of von Willebrand factor–cleaving protease (ADAMTS13) in patients with sepsis-induced disseminated intravascular coagulation: Its correlation with development of renal failure. Blood 2006, 107, 528–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiscia, G.; Favuzzi, G.; De Laurenzo, A.; Cappucci, F.; Fischetti, L.; Colaizzo, D.; Chinni, E.; Florio, L.; Miscio, G.; Piscitelli, A.P.; et al. The Prognostic Value of ADAMTS-13 and von Willebrand Factor in COVID-19 Patients: Prospective Evaluation by Care Setting. Diagnostics 2021, 11, 1648. [Google Scholar] [CrossRef] [PubMed]
- Krechetova, L.V.; Nechipurenko, D.Y.; Shpilyuk, M.A.; Beznoshchenko, O.S.; Beresneva, E.A.; Markelov, M.I.; Ivanets, T.Y.; Gavrilova, T.Y.; Kozachenko, I.F.; Esayan, R.M.; et al. The use of the thrombodynamics test in the diagnostics of hemostasis disorders in patients with COVID-19 of varying severity. J. Clin. Pract. 2021, 12, 23–37. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | MILD (n = 39) | MODERATE (n = 65) | SEVERE (n = 37) | p-Value |
|---|---|---|---|---|
| Gender male | 7 (17.9%) | 24 (36.9%) | 22 (59.5%) | 0.0009 *** |
| Gender female | 32 (82.1%) | 41 (63.1%) | 15 (40.5%) | |
| Age, years | 38 (34–54) | 60 (43–78) | 63 (53–71) | 0.0001 ** |
| Height, m | 1.67 ± 0.09 | 1.68 ± 0.08 | 1.69 ± 0.07 | 0.5664 * |
| Body weight, kg | 71.3 ± 15.4 | 78.5 ± 20.3 | 83.3 ± 12.5 | 0.0094 * |
| BMI, kg/m2 | 25.2 ± 4.4 | 27.4 ± 6.2 | 29.1 ± 5.3 | 0.0092 * |
| Smoking | 4 (10.3%) | 10 (15.4%) | 1 (2.7%) | 0.1355 *** |
| Alcohol consumption | 13 (33.3%) | 12 (18.5%) | 9 (24.3%) |
| Point of Study (Reference) | MILD (n = 39) | MODERATE (n = 65) | SEVERE (n = 37) | p-Value |
|---|---|---|---|---|
| ADAMTS-13 Point 1 (0.41–1.41 mU/mL) | 0.83 ± 0.22 | 0.75 ± 0.26 | 0.70 ± 0.3 | 0.1678 |
| 0.1584 *; 0.0662 **; | ||||
| 0.4461 *** | ||||
| ADAMTS-13 Point 2 (0.41–1.41 mU/mL) | 0.78 ± 0.22 | 0.73 ± 0.29 | 0.46 ± 0.23 | <0.0001 |
| p = 0.4095 ^ | p = 0.6458 ^ | p = 0.0002 ^ | 0.2952 *; <0.0001 **; | |
| <0.0001 *** | ||||
| ADAMTS-13 activity Point 1 (0.4–1.3 mU/mL) | 1.02 ± 0.18 | 0.89 ± 0.20 | 0.89 ± 0.23 | 0.0093 |
| 0.0027 *; 0.0116 **; | ||||
| 0.9720 *** | ||||
| ADAMTS-13 activity Point 2 (0.4–1.3 mU/mL) | 0.95 ± 0.12 | 0.89 ± 0.15 | 0.79 ± 0.22 | 0.0007 |
| p = 0.0533 ^ | p = 0.9541 ^ | p = 0.0970 ^ | 0.0391 *; 0.0005 **; | |
| 0.0228 *** | ||||
| ADAMTS-13 inhibitor Point 1 (<12 mU/mL) | 7.60 ± 3.42 | 7.51 ± 4.47 | 9.36 ± 4.49 | 0.0815 |
| 0.9089 *; 0.0578 **; | ||||
| 0.0567 *** | ||||
| ADAMTS-13 inhibitor Point 2 (<12 mU/mL) | 10.49 ± 5.26 | 8.42 ± 4.89 | 11.91 ± 7.07 | 0.0134 |
| p = 0.0052 ^ | p = 0.2763 ^ | p = 0.0734 ^ | 0.0479 *; 0.3328 **; | |
| 0.0060 *** |
| Point of Study (Reference) | MILD (n = 39) | MODERATE (n = 65) | SEVERE (n = 37) | p-Value |
|---|---|---|---|---|
| Point 1 | 1 (2.6%) | 12 (18.5%) | 8 (21.6%) | 0.0180 * |
| 0.0110 ** | ||||
| Point 2 | 3 (7.7%) | 10 (15.4%) | 18 (48.6%) | 0.2500 * |
| 0.0001 ** |
| Point of Study | MILD (n = 39) | MODERATE (n = 65) | SEVERE (n = 37) | p-Value |
|---|---|---|---|---|
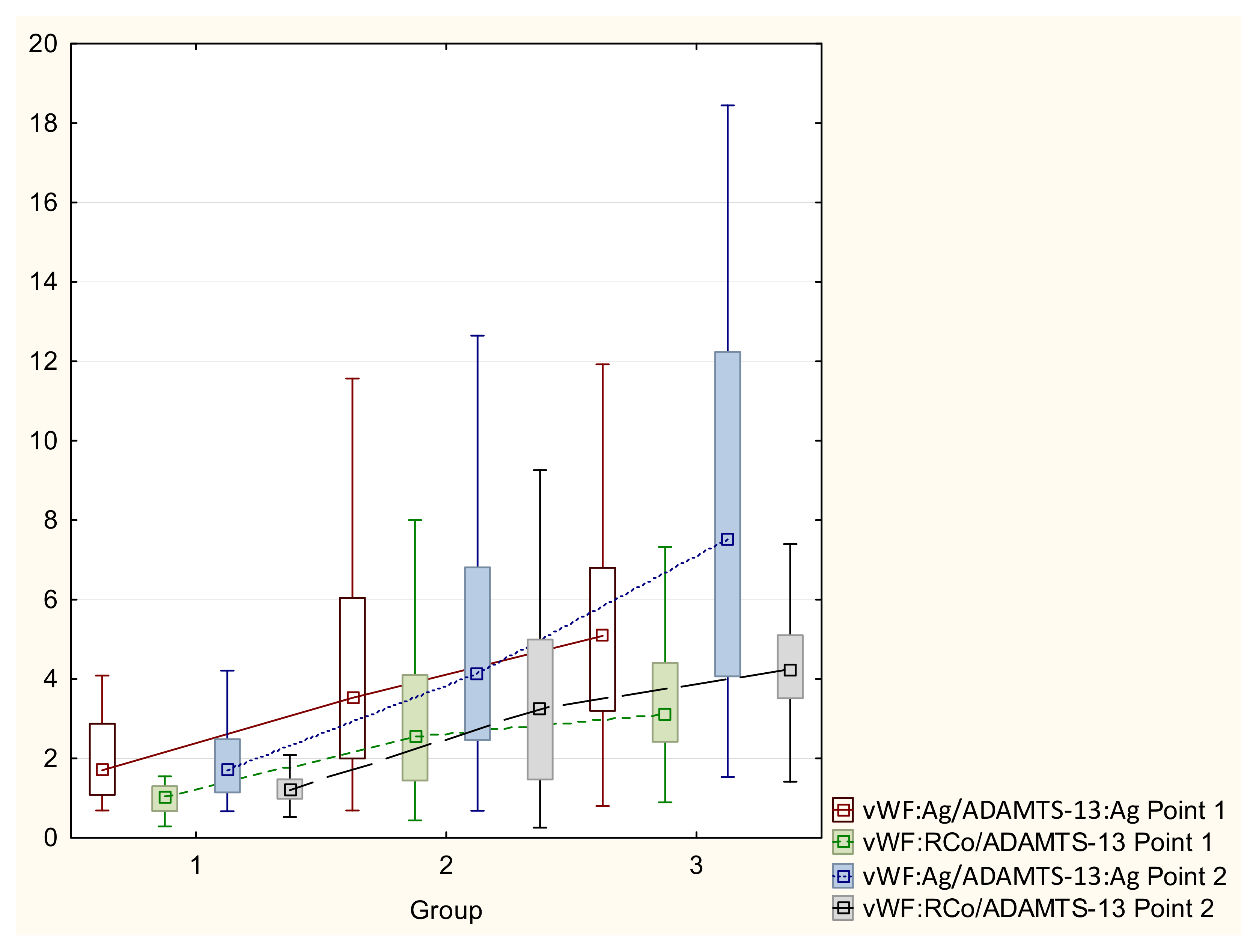
| vWF/ADAMTS-13 Point 1 | 2.7 ± 3.2 | 5.7 ± 9.7 | 5.6 ± 3.7 | 0.1428 0.1184 *; 0.1054 **; 0.2154 *** |
| vWF:RCo/ADAMTS-13:activity Point 1 | 1.5 ± 1.8 p = 0.0248 ^ | 3.1 ± 2.1 p = 0.0378 ^ | 3.6 ± 2.2 p = 0.0217 ^ | 0.0005 0.0127 *; 0.0097 **; 0.4478 *** |
| vWF/ADAMTS-13 Point 2 | 2.2 ± 1.9 | 6.9 ± 12.3 | 10.3 ± 9.9 | 0.0065 0.0195 *; 0.0054 **; 0.0845 *** |
| vWF:RCo/ADAMTS-13:activity Point 2 | 1.5 ± 1.7 p = 0.0298 ^ | 3.5 ± 2.2 p = 0.0281 ^ | 4.5 ± 2.0 p = 0.0285 ^ | <0.0001 0.0065 *; 0.0019 **; 0.0498 *** |
| Point of Study | Threshold | AUC | Se | Sp |
|---|---|---|---|---|
| vWF/ADAMTS-13 Point 1 | 2.45 | 74.2% | 74.5% | 70.0% |
| vWF:RCo/ADAMTS-13:activity Point 1 | 1.55 | 82.6% | 73.3% | 90.0% |
| vWF/ADAMTS-13 Point 2 | 2.55 | 81.7% | 78.5% | 78.9% |
| vWF:RCo/ADAMTS-13:activity Point 2 | 1.55 | 80.4% | 77.1% | 78.9% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dolgushina, N.; Gorodnova, E.; Beznoshenco, O.; Romanov, A.; Menzhinskaya, I.; Krechetova, L.; Sukhikh, G. Von Willebrand Factor and ADAMTS-13 Are Associated with the Severity of COVID-19 Disease. J. Clin. Med. 2022, 11, 4006. https://doi.org/10.3390/jcm11144006
Dolgushina N, Gorodnova E, Beznoshenco O, Romanov A, Menzhinskaya I, Krechetova L, Sukhikh G. Von Willebrand Factor and ADAMTS-13 Are Associated with the Severity of COVID-19 Disease. Journal of Clinical Medicine. 2022; 11(14):4006. https://doi.org/10.3390/jcm11144006
Chicago/Turabian StyleDolgushina, Nataliya, Elena Gorodnova, Olga Beznoshenco, Andrey Romanov, Irina Menzhinskaya, Lyubov Krechetova, and Gennady Sukhikh. 2022. "Von Willebrand Factor and ADAMTS-13 Are Associated with the Severity of COVID-19 Disease" Journal of Clinical Medicine 11, no. 14: 4006. https://doi.org/10.3390/jcm11144006