
Evaluation of Vulnerability Status of the Infection Risk to COVID-19 Using Geographic Information Systems (GIS) and Multi-Criteria Decision Analysis (MCDA): A Case Study of Addis Ababa City, Ethiopia

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
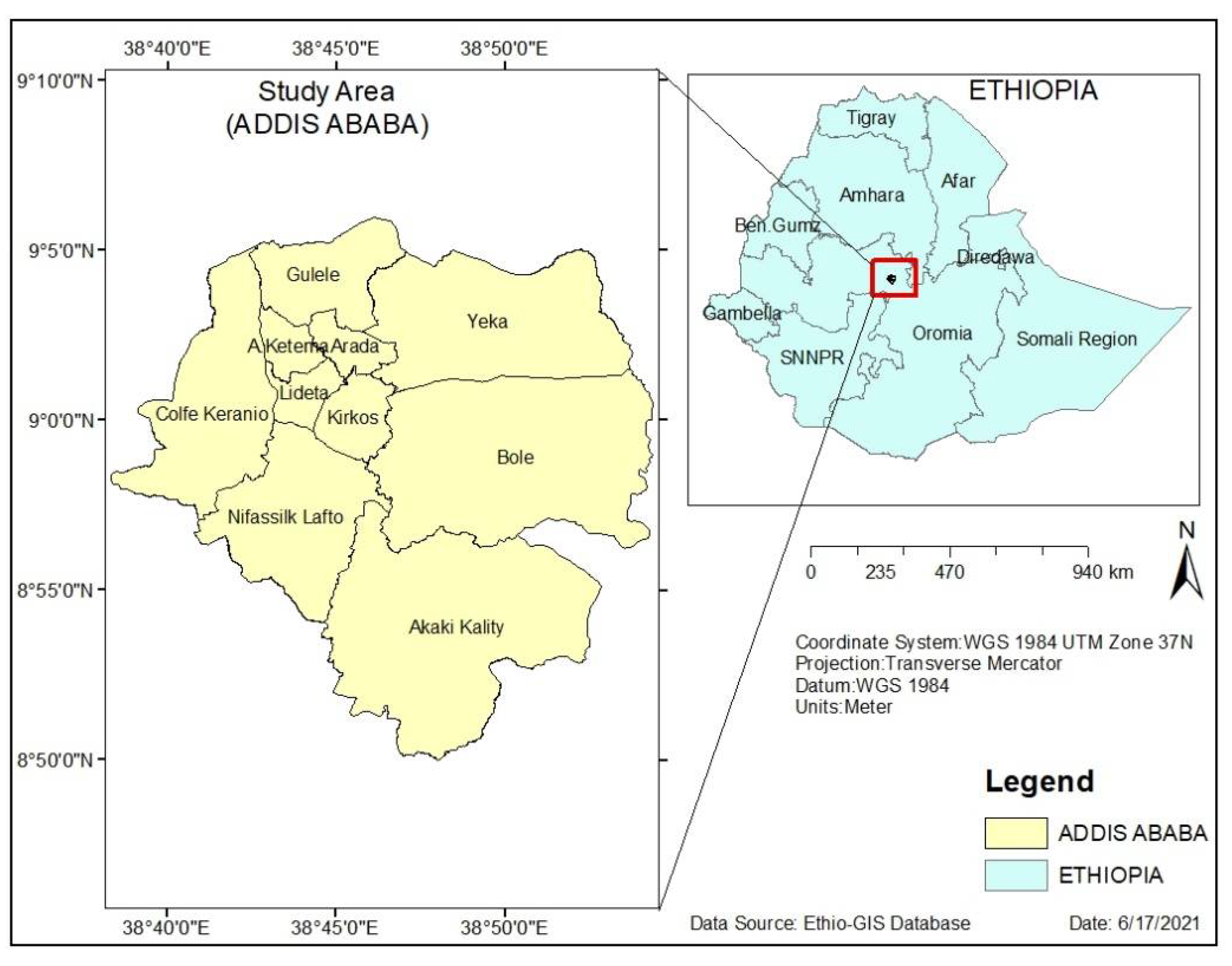
2.1. Description of the Study Area
2.2. Materials and Data Collection
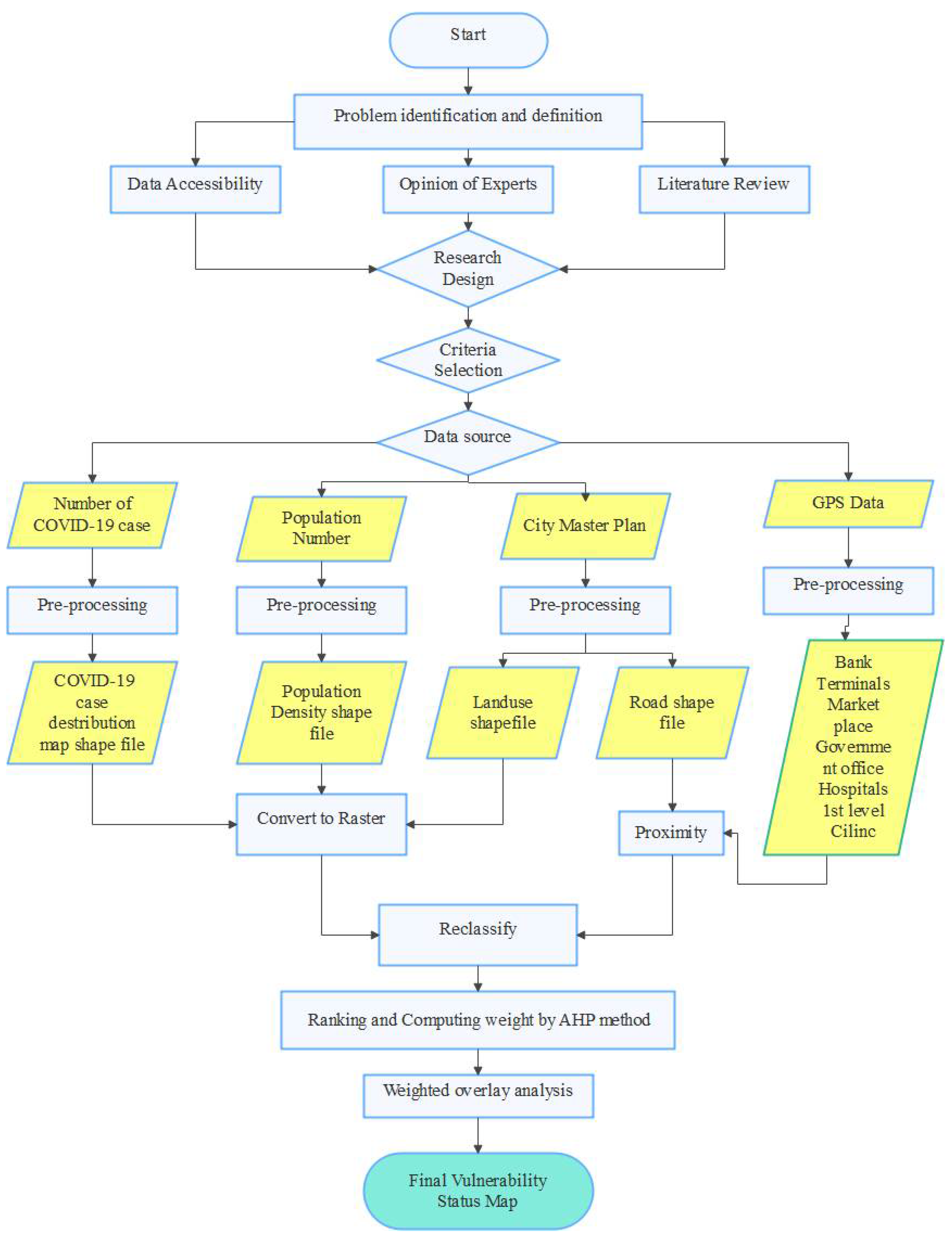
2.3. Method of Data Analysis
3. Results and Discussion
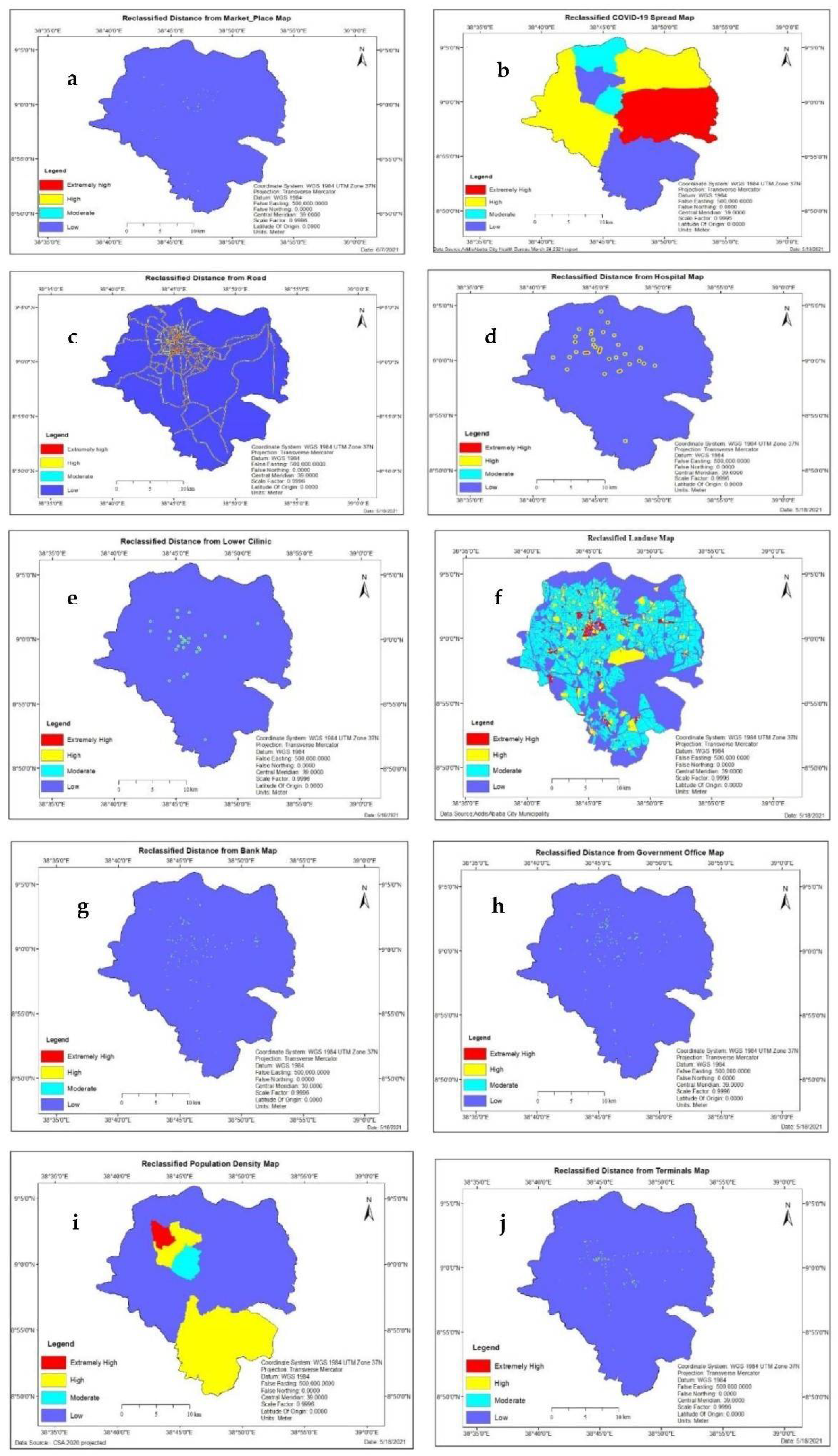
3.1. Factors for COVID-19 Infection Risk Vulnerability Status Evaluation
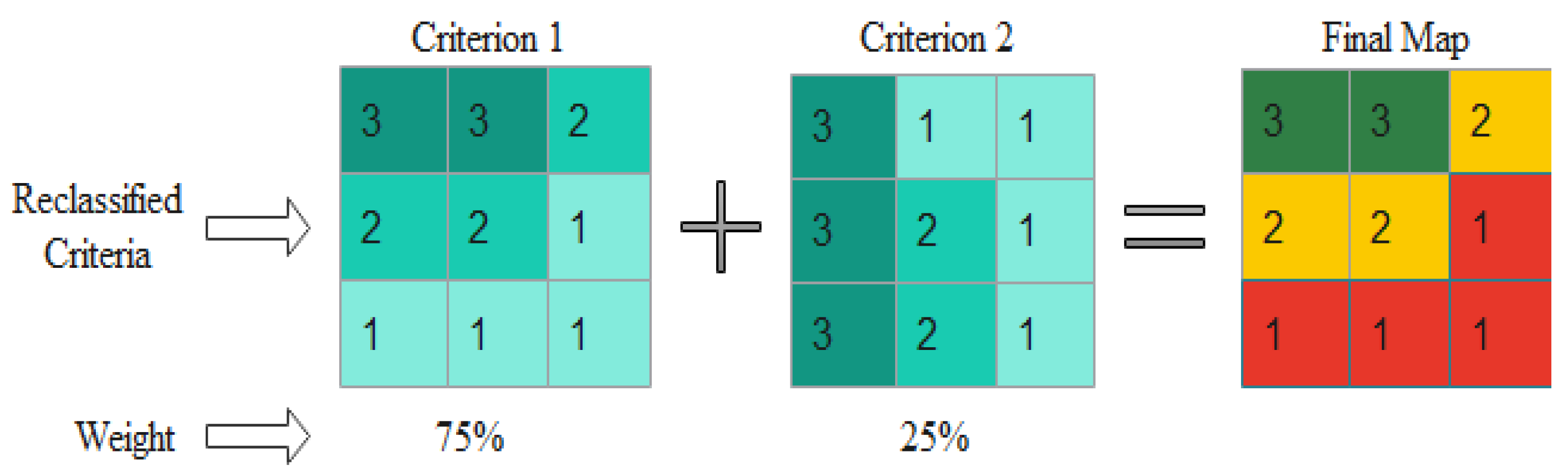
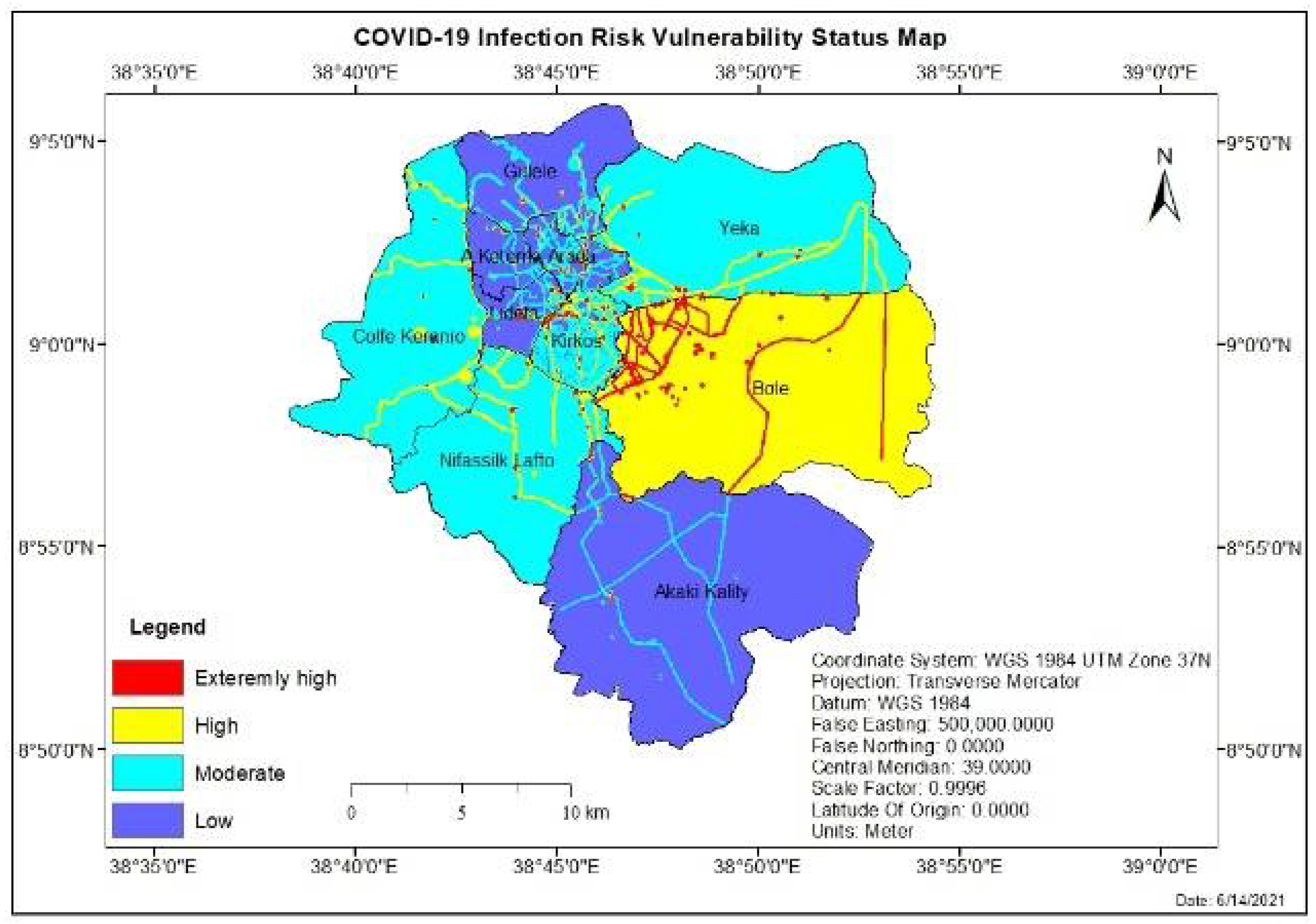
3.2. Overlaying and COVID-19 Infection Risk Vulnerability Status Evaluation
4. Conclusions
5. Recommendations
- One of the results noticed in this study was that an area with a cluster of services and high mobility is at a status of extremely high vulnerability to infection risk of COVID-19. Therefore, proper strategies have to be implemented to halt the spread of the disease with special attention in those areas.
- The city should develop the capacity to use GIS and MCDA to identify the vulnerability status of infection risk of COVID-19 and related activity in the city.
- It will be efficient if the city will incorporate the infection risk vulnerability status maps, which are the results of this study, in the current ongoing pandemic control activities to target the priority areas identified by the study;
- The establishment of health centers and other pandemic control facilities should be made in high and extremely high-vulnerable areas at a reasonable distance away from the existing facilities so that people at a distance can easily access the service.
- Proper databases about detailed patient data, the spatial spread of epidemics, and other related aspects of the pandemic should be made using GIS.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO/Europe|Coronavirus Disease (COVID-19) Outbreak-WHO Announces COVID-19 Outbreak a Pandemic; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Hui, D.S.; Azhar, E.I.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; Mchugh, T.D.; Memish, Z.A.; Drosten, C.; et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—The latest 2019 novel coronavirus outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coccia, M. Science of the Total Environment Factors determining the diffusion of COVID-19 and suggested strategy to prevent future accelerated viral infectivity similar to COVID. Sci. Total Environ. 2020, 729, 138474. [Google Scholar] [CrossRef] [PubMed]
- Sabarathinam, C.; Mohan Viswanathan, P.; Senapathi, V.; Karuppannan, S.; Samayamanthula, D.R.; Gopalakrishnan, G.; Alagappan, R.; Bhattacharya, P. SARS-CoV-2 phase I transmission and mutability linked to the interplay of climatic variables: A global observation on the pandemic spread. Environ. Sci. Pollut. Res. 2022, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, P.M.; Sabarathinam, C.; Karuppannan, S.; Gopalakrishnan, G. Determination of vulnerable regions of SARS-CoV-2 in Malaysia using meteorology and air quality data. Environ. Dev. Sustain. 2021, 24, 8856–8882. [Google Scholar] [CrossRef] [PubMed]
- Karuppasamy, M.B.; Seshachalam, S.; Natesan, U.; Ayyamperumal, R.; Karuppannan, S.; Gopalakrishnan, G.; Nazir, N. Air pollution improvement and mortality rate during COVID-19 pandemic in India: Global intersectional study. Air Qual. Atmos. Health 2020, 13, 1375–1384. [Google Scholar] [CrossRef] [PubMed]
- Africa CDC. Coronavirus Disease 2019 (COVID-19)–Africa CDC; Africa CDC: Addis Ababa, Ethiopia, 2020. [Google Scholar]
- World Health Organization. WHO Housing and Health Guidelines; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Mohammed, H.; Oljira, L.; Roba, K.T.; Yimer, G.; Fekadu, A.; Manyazewal, T. Containment of COVID-19 in Ethiopia and implications for tuberculosis care and research. Infect. Dis. Poverty 2020, 9, 1–8. [Google Scholar] [CrossRef]
- Lia. Lia Tadesse on Twitter: “Ethiopia Confirms It’s First Positive Test for #Covid_19. The Patient is a 48 Year Old Japanese Citizen Who Came to Ethiopia on March 4th from Burkina Faso and Is Currently Isolated at Our Facility Undergoing Medical Follow Up. ht”. 2020. Available online: https://twitter.com/lia_tadesse/status/1238430393994534917/photo/1 (accessed on 18 December 2020).
- Federal Republic of Ethiopia Office Prime Minister 2020. National Ministerial Committee Press Release 20 March; Federal Republic of Ethiopia Office Prime Minister: Addis Ababa, Ethiopia, 2020. [Google Scholar]
- Baye, K. COVID-19 prevention measures in Ethiopia Current realities and prospects. Int. Food Policy Res. Inst. 2020, 141, 14. [Google Scholar]
- Ministry of Health, Ethiopia. Posts|Faceboo; Ministry of Health, Ethiopia: Addis Ababa, Ethiopia, 2020; Available online: https://www.facebook.com/EthiopiaFMoH/posts/1703984719772324 (accessed on 18 December 2020).
- Biadgilign, S.; Yigzaw, M. COVID-19 in ethiopia: Current situation, missed opportunities, and the risk of health system disruptions. Pan Afr. Med. J. 2020, 35, 1–2. [Google Scholar] [CrossRef]
- Sánchez-Sánchez, J.A.; Chuc, V.M.K.; Canché, E.A.R.; Uscanga, F.J.L. Using Geographic Information Systems and Multi-Criteria Decision Analysis:Vulnerability Assessing Contagion Risk of Covid-19 Case Study Chetumal, México. Commun. Comput. Inf. Sci. 2020, 1276, 1–17. [Google Scholar] [CrossRef]
- Qayum, A.; Arya, R.; Kumar, P.; Lynn, A.M. Features based on GIS-integrated mapping to identify malarial hotspots Socio-economic, epidemiological and geographic features based on GIS-integrated mapping to identify malarial hotspots. Malar. J. 2015, 14, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, F.; Goparaju, L.; Qayum, A. Studying Malaria Epidemic for Vulnerability Zones: Multi-Criteria Approach of Geospatial Tools. J. Geosci. Environ. Prot. 2017, 5, 30–53. [Google Scholar] [CrossRef]
- Martel, J.-M.; Chakhar, S. Enhancing geographical information systems capabilities with multi-criteria evaluation functions. J. Geogr. Inf. Decis. Anal. 2003, 7, 47–71. [Google Scholar]
- Malczewski, J. GIS-based multicriteria decision analysis: A survey of the literature. Int. J. Geogr. Inf. Sci. 2006, 20, 703–726. [Google Scholar] [CrossRef]
- Cowen, D.J. GIS versus CAD versus DBMS: What are the differences? Introd. Read. Geogr. Inf. Syst. 1990, 54, 52–61. [Google Scholar]
- Heylin, M. Disaster. Chem. Eng. News 1986, 64, 3. [Google Scholar] [CrossRef] [Green Version]
- Saaty, T.L.; Vargas, L.G. Hierarchical analysis of behavior in competition: Prediction in chess. Behav. Sci. 1980, 25, 180–191. [Google Scholar] [CrossRef]
- Ng, C.Y. Evidential reasoning-based Fuzzy AHP approach for the evaluation of design alternatives’ environmental performances. Appl. Soft Comput. J. 2016, 46, 381–397. [Google Scholar] [CrossRef]
- Chen, Z.; Chen, T.; Qu, Z.; Yang, Z.; Ji, X.; Zhou, Y.; Zhang, H. Use of evidential reasoning and AHP to assess regional industrial safety. PLoS ONE 2018, 13, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Garner, B.J.; Zhou, Q.; Parolin, B.P. The Application of GIS in the Health Sector: Problems and Prospects. In Proceedings of the Fourth European Conference on Geographical Information Systems, EGIS ‘93, Genoa, Italy, 29 March–1 April 1993. [Google Scholar]
- Murugesan, B.; Karuppannan, S.; Mengistie, A.T.; Ranganathan, M.; Gopalakrishnan, G. Distribution and Trend Analysis of COVID-19 in India: Geospatial Approach. J. Geogr. Stud. 2020, 4, 1–9. [Google Scholar] [CrossRef]
- Sarfo, A.K.; Karuppannan, S. Application of Geospatial Technologies in the COVID-19 Fight of Ghana. Trans. Indian Natl. Acad. Eng. 2020, 5, 193–204. [Google Scholar] [CrossRef]
- Davenhall, W.F.; Kinabrew, C. GIS in Health; Springer: Berlin/Heidelberg, Germany, 1970; pp. 911–937. [Google Scholar]
- Wang, H.; Liu, Q.; Hu, J.; Zhou, M.; Yu, M.Q.; Li, K.Y.; Xu, D.; Xiao, Y.; Yang, J.Y.; Lu, Y.J.; et al. Nasopharyngeal Swabs Are More Sensitive Than Oropharyngeal Swabs for COVID-19 Diagnosis and Monitoring the SARS-CoV-2 Load. Front. Med. 2020, 7, 334. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Su, F.; Pei, T.; Zhang, A.; Du, Y.; Luo, B.; Cao, Z.; Wang, J.; Yuan, W.; Zhu, Y.; et al. COVID-19: Challenges to GIS with Big Data. Geogr. Sustain. 2020, 1, 77–87. [Google Scholar] [CrossRef]
- WHO. Using Geographical Information Systems (GIS) to Identify Vulnerable Populations in Brazil; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- United Nations Environment Programme. Addis Ababa City Air Quality Policy and Regulatory Situational Analysis; United Nations Environment Programme: Addis Ababa, Ethiopia, 2018. [Google Scholar]
- Bui, Q.T.; Nguyen, Q.H.; Pham, V.M.; Pham, M.H.; Tran, A.T. Understanding spatial variations of malaria in Vietnam using remotely sensed data integrated into GIS and machine learning classifiers. Geocarto Int. 2019, 34, 1300–1314. [Google Scholar] [CrossRef]
- Chen, S.; Yang, J.; Yang, W.; Wang, C.; Bärnighausen, T. COVID-19 control in China during mass population movements at New Year. Lancet 2020, 395, 764–766. [Google Scholar] [CrossRef] [Green Version]
- Pourghasemi, H.R.; Pouyan, S.; Farajzadeh, Z.; Sadhasivam, N.; Heidari, B.; Babaei, S.; Tiefenbacher, J.P. Assessment of the outbreak risk, mapping and infection behavior of COVID-19: Application of the autoregressive integrated-moving average (ARIMA) and polynomial models. PLoS ONE 2020, 15, e0236238. [Google Scholar] [CrossRef]
- Alzamili, H.H.; El-Mewafi, M.; Beshr, A.A.A.; Awad, A. GIS-Based-Multi-Criteria-Dicesion-Analysis-for-Industrial-Site-Selection-in-Al-Nasiriyah-City-in-Iraq.doc. Int. J. Sci. Eng. Res. 2015, 6, 1330–1337. [Google Scholar]
- CDC. Operational Considerations for Markets; CDC: Atlanta, GA, USA, 2021. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S.No | Data | Source | Data Type |
|---|---|---|---|
| 1 | Addis Ababa City boundary | Urban planning office | Shapefile |
| 2 | Coordinate data | Google Earth and filed work | CSV |
| 3 | Population data | Central Statistical Agency (CSA) 2020 Projected. | Text |
| 4 | Addis Ababa City Master Plan | Addis Ababa City Municipality | Shapefile/CAD file |
| No. | Material/Software Name | Purpose |
|---|---|---|
| 1 | Handheld GPS eTrex 10 | To collect the coordinate of a point |
| 2 | Esri ArcGIS 10.8 | For data analysis and mapping; For Editing spatial data in arc Map and non-spatial data in arc catalog. |
| 3 | IDRISI Selva 17 | To calculate the weight of each layer. |
| 4 | Google Earth Pro | To visualize spatial features in the study area and get coordinates points. |
| 5 | MS-Excel and MS-Word 2019 | Integrating attribute data and preparing a thesis report |
| Rank | Criteria | Proximity Distance (m) and Classification Parameters Extremely High to Low Vulnerable | Percent |
|---|---|---|---|
| 1 | Market place | >30, 30–60, 60–90, 90< | 31 |
| 2 | Terminals | >30, 30–60, 60–90, 90< | 19 |
| 3 | COVID-19 case till 24 March 2021 | 14,850–28,735, 10,769–14,850, 8145–10,769, 6874–8145 | 18 |
| 4 | Road | >30, 30–60, 60–90, 90< | 9 |
| 5 | Government office | >30, 30–60, 60–90, 90< | 6 |
| 6 | Hospitals | >30, 30–60, 60–90, 90< | 5 |
| 7 | Lower Clinics | >30, 30–60, 60–90, 90< | 4 |
| 8 | Banks | >30, 30–60, 60–90, 90< | 3 |
| 9 | Population density | 20,287–39,801, 11,456–20,287, 5615–11,456, 3479–5615 | 3 |
| 10 | Land use | Commerce, Mixed residence, Service, Miscellaneous | 2 |
| Less Important | More Important | |||||||
|---|---|---|---|---|---|---|---|---|
| Extremely | Very Strong | Strong | Moderately | Equal | Moderately | Strong | Very Strong | Extremely |
| 1/9 | 1/7 | 1/5 | 1/3 | 1 | 3 | 5 | 7 | 9 |
| Factors | Mp | T | C | R | Go | H | LC | B | Pd | LU | Weight | % of Weight |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Market place (Mp) | 1 | 0.3100 | 31 | |||||||||
| Terminals (T) | 1/3 | 1 | 0.1938 | 19 | ||||||||
| COVID-19 case (C) | 1/3 | 1/2 | 1 | 0.1748 | 18 | |||||||
| Road (R) | 1/5 | 1/3 | 1/3 | 1 | 0.0872 | 9 | ||||||
| Government office (Go) | 1/5 | 1/3 | 1/5 | 1/2 | 1 | 0.0643 | 6 | |||||
| Hospitals (H) | 1/7 | 1/5 | 1/5 | 1/3 | 1/2 | 1 | 0.0509 | 5 | ||||
| Lower Clinics (LC) | 1/7 | 1/5 | 1/5 | 1/3 | 1/3 | 1/2 | 1 | 0.0436 | 4 | |||
| Banks (B) | 1/7 | 1/7 | 1/5 | 1/3 | 1/2 | 1/3 | 1/3 | 1 | 0.0311 | 3 | ||
| Population density (Pd) | 1/7 | 1/7 | 1/7 | 1/3 | 1/3 | 1/2 | 1/2 | 1/2 | 1 | 0.0267 | 3 | |
| Landuse (LU) | 1/7 | 1/7 | 1/7 | 1/5 | 1/3 | 1/5 | 1/5 | 1/3 | 1/3 | 1 | 0.0177 | 2 |
| Total | 1 | 100 | ||||||||||
| No | Factors | Proximity to Market Place (m) | Vulnerability Status | Area Coverage (km2) | % of Area Coverage | Rank |
|---|---|---|---|---|---|---|
| 1. | Distance from marketplace | >90 | Low | 520.20 | 99.87 | 1 |
| 60–90 | Moderate | 0.4 | 0.08 | 2 | ||
| 30–60 | High | 0.25 | 0.05 | 3 | ||
| <30 | Extremely high | 0.07 | 0.01 | 4 | ||
| 2. | Distance from terminals | >90 | Low | 518.6 | 99.56 | 1 |
| 60–90 | Moderate | 1.17 | 0.22 | 2 | ||
| 30–60 | High | 0.68 | 0.13 | 3 | ||
| <30 | Extremely high | 0.46 | 0.09 | 4 | ||
| 3. | COVID-19 spread | 6874–8145 | Low | 151.56 | 29.1 | 1 |
| 8145–10,769 | Moderate | 45.84 | 8.8 | 2 | ||
| 10,769–14,850 | High | 203.85 | 39.13 | 3 | ||
| 14,850–28,735 | Extremely high | 119.66 | 22.97 | 4 | ||
| 4. | Distance from road | >90 | Low | 481.32 | 92.4 | 1 |
| 60–90 | Moderate | 17.14 | 3.29 | 2 | ||
| 30–60 | High | 13.35 | 2.56 | 3 | ||
| <30 | Extremely high | 9.1 | 1.75 | 4 | ||
| 5. | Distance from hospitals | >90 | Low | 508.68 | 97.65 | 1 |
| 60–90 | Moderate | 2.91 | 0.56 | 2 | ||
| 30–60 | High | 6.79 | 1.3 | 3 | ||
| <30 | Extremely high | 2.56 | 0.49 | 4 | ||
| 6. | Distance from lower clinics | >90 | Low | 516.86 | 99.22 | 1 |
| 60–90 | Moderate | 2.14 | 0.41 | 2 | ||
| 30–60 | High | 1.46 | 0.28 | 3 | ||
| <30 | Extremely high | 0.48 | 0.09 | 4 | ||
| 7. | Distance from banks | >90 | Low | 518.62 | 99.56 | 1 |
| 60–90 | Moderate | 1.19 | 0.23 | 2 | ||
| 30–60 | High | 0.67 | 0.13 | 3 | ||
| <30 | Extremely high | 0.43 | 0.08 | 4 | ||
| 8. | Distance from government office | >90 | Low | 518.35 | 99.51 | 1 |
| 60–90 | Moderate | 1.37 | 0.26 | 2 | ||
| 30–60 | High | 0.9 | 0.17 | 3 | ||
| <30 | Extremely high | 0.29 | 0.06 | 4 | ||
| 9. | Population density | 3479–5615 | Low | 354.69 | 68.09 | 1 |
| 5615–11,456 | Moderate | 14.65 | 2.81 | 2 | ||
| 11,456–20,287 | High | 142.93 | 27.44 | 3 | ||
| 20,287–39,801 | Extremely high | 8.63 | 1.66 | 4 | ||
| 10. | Land use | Miscellaneous | Low | 252.69 | 48.50 | 1 |
| Service | Moderate | 220.78 | 42.38 | 2 | ||
| Mixed residence | High | 40.03 | 7.68 | 3 | ||
| Commerce | Extremely high | 7.48 | 1.44 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asfaw, H.; Karuppannan, S.; Erduno, T.; Almohamad, H.; Dughairi, A.A.A.; Al-Mutiry, M.; Abdo, H.G. Evaluation of Vulnerability Status of the Infection Risk to COVID-19 Using Geographic Information Systems (GIS) and Multi-Criteria Decision Analysis (MCDA): A Case Study of Addis Ababa City, Ethiopia. Int. J. Environ. Res. Public Health 2022, 19, 7811. https://doi.org/10.3390/ijerph19137811
Asfaw H, Karuppannan S, Erduno T, Almohamad H, Dughairi AAA, Al-Mutiry M, Abdo HG. Evaluation of Vulnerability Status of the Infection Risk to COVID-19 Using Geographic Information Systems (GIS) and Multi-Criteria Decision Analysis (MCDA): A Case Study of Addis Ababa City, Ethiopia. International Journal of Environmental Research and Public Health. 2022; 19(13):7811. https://doi.org/10.3390/ijerph19137811
Chicago/Turabian StyleAsfaw, Hizkel, Shankar Karuppannan, Tilahun Erduno, Hussein Almohamad, Ahmed Abdullah Al Dughairi, Motrih Al-Mutiry, and Hazem Ghassan Abdo. 2022. "Evaluation of Vulnerability Status of the Infection Risk to COVID-19 Using Geographic Information Systems (GIS) and Multi-Criteria Decision Analysis (MCDA): A Case Study of Addis Ababa City, Ethiopia" International Journal of Environmental Research and Public Health 19, no. 13: 7811. https://doi.org/10.3390/ijerph19137811