
Factors That Shape People’s Attitudes towards the COVID-19 Pandemic in Germany—The Influence of MEDIA, Politics and Personal Characteristics


Abstract
:1. Introduction
2. Theory
3. Data and Methodology
3.1. Survey Structure
- Demographic characteristics: age, residency, level of education, employment.
- Political views.
- Media consumption: social networks and messenger services, information seeking behavior (television, print media, radio). Public media in Germany is an independent source of information without any influence of state or private sector. Public media is financed through broadcasting fees by the German population and includes television, radio, and social media channels. In our analyses we included public media TV channels (e.g., ARD, ZDF) under the term “public media”, since they are the most important source of news in Germany.
- Knowledge about SARS-CoV-2 and personal experience with SARS-CoV-2.
- Risk perception: we considered that respondents perceived the virus as a threat to health when they answered to the statement “I am concerned that an infection with the SARS-CoV-2 could damage my health or a relative’s health” with “agree” or “strongly agree”.
- Satisfaction with public health education about the pandemic by certain institutions.
- Assessment of the necessity of SARS-CoV-2-specific health-protective measures and willingness to get vaccinated.
- Implementation of SARS-CoV-2-specific health-protective measures.
- Trust in health authorities and governmental institutions.
- Attitudes towards vaccinations in general.
- Attitudes towards alternative medicine in general.
3.2. Statistical Analysis
4. Results
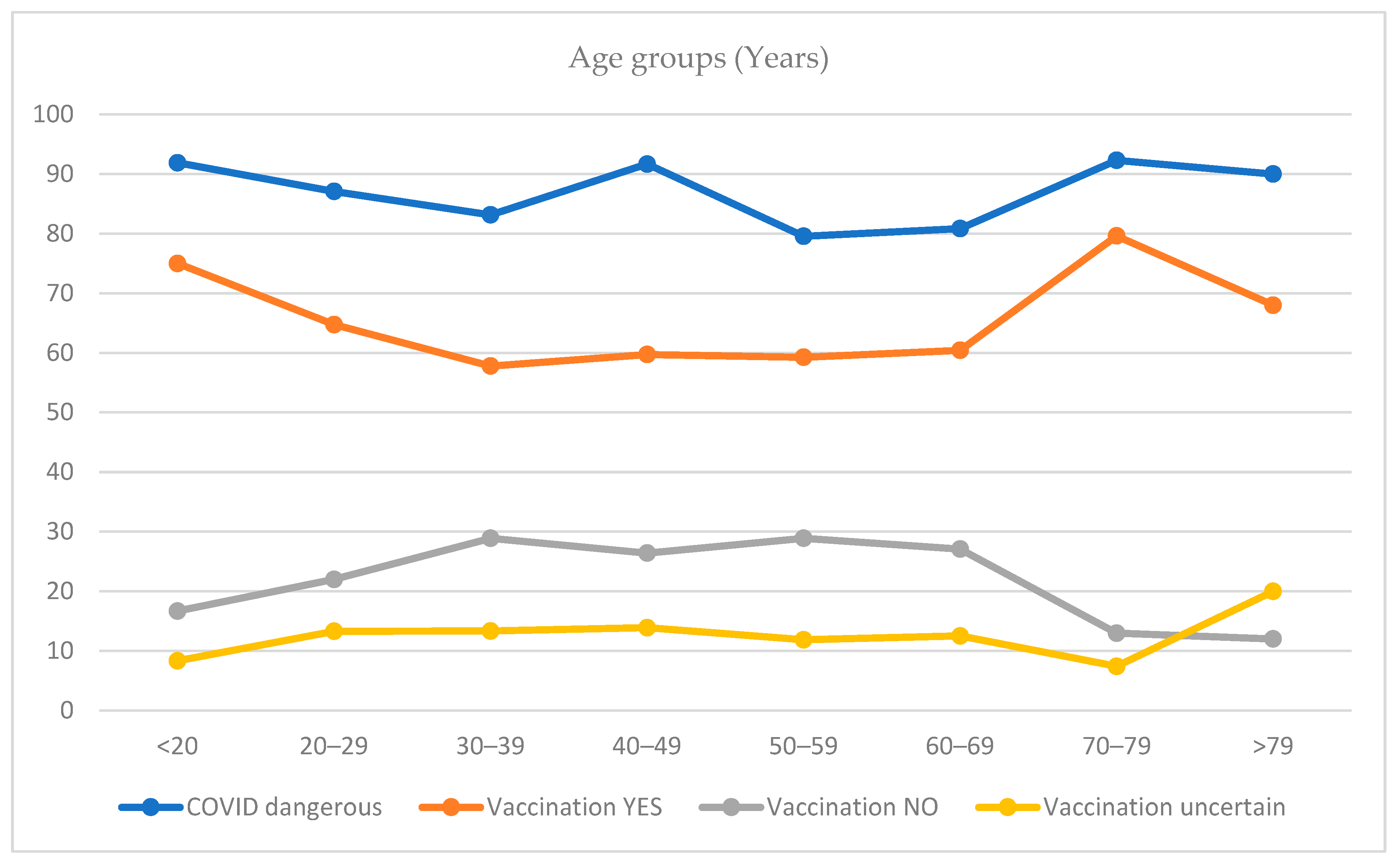
4.1. Risk Perception
4.2. Health Protective Behavior
4.3. Trust in Institutions
4.4. Media
4.5. Political Attitude
4.6. Own Experience
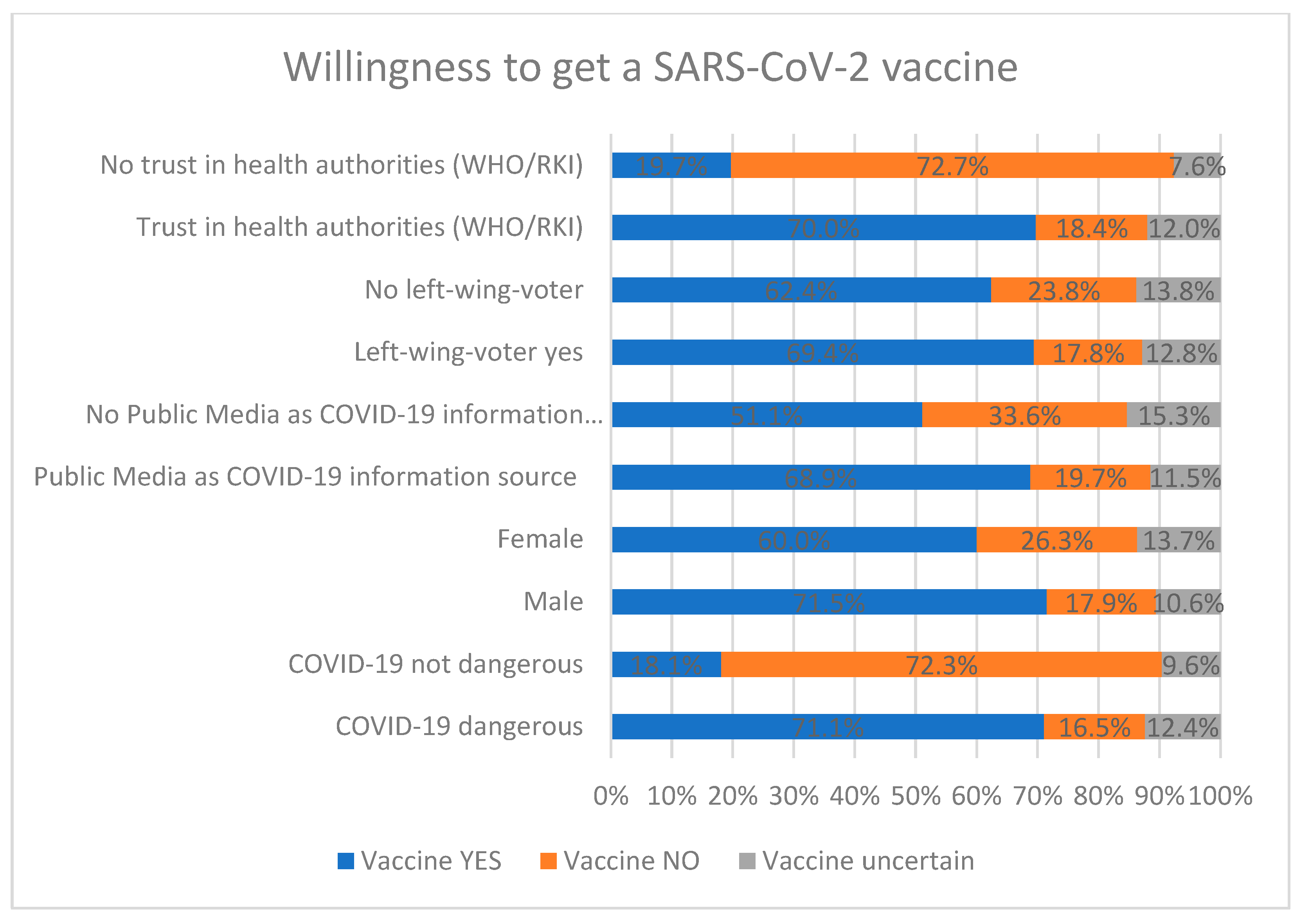
4.7. Vaccination Intention
5. Discussion
Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID 19 Public Health Emergency of International Concern (PHEIC). Available online: https://www.who.int/publications/m/item/covid-19-public-health-emergency-of-international-concern-(pheic)-global-research-and-innovation-forum (accessed on 25 April 2021).
- Durrheim, D.N.; Gostin, L.O.; Moodley, K. When does a major outbreak become a Public Health Emergency of International Concern? Lancet Infect. Dis. 2020, 20, 887–889. [Google Scholar] [CrossRef]
- Bundesministerium fur Gesundheit (BMG). Coronavirus-Pandemie (SARS-CoV-2): Chronik bisheriger Maßnahmen und Ereignisse. Available online: https://www.bundesgesundheitsministerium.de/coronavirus/chronik-coronavirus.html (accessed on 24 April 2021).
- Gastaldelli, A.; Gastaldelli, M.; Bastianoni, S. COVID-19 Infection Pandemic: From the Frontline in Italy. J. Am. Coll. Nutr. 2020, 39, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Balbierer, T. Entschuldigung, Aber Ich Muss Weinen. Available online: https://www.sueddeutsche.de/panorama/coronavirus-italien-bergamo-1.4851056 (accessed on 25 April 2021).
- Senni, M. COVID-19 experience in Bergamo, Italy. Eur. Heart J. 2020, 41, 1783–1784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert Koch Institut. Täglicher Lagebericht des RKI zur Coronavirus-Krankheit-2019 (COVID-19). Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/2020-06-15-de.pdf?__blob=publicationFile (accessed on 7 May 2021).
- Robert Koch Institut. Täglicher Lagebericht des RKI zur Coronavirus-Krankheit 2019 (COVID-19). Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Dez_2020/2020-12-10-de.pdf?__blob=publicationFile (accessed on 25 April 2021).
- Bundesregierung. Einzelhandel Geschlossen, Supermärkte Bleiben Offen. Available online: https://www.bundesregierung.de/breg-de/themen/coronavirus/bundesweiter-lockdown-1829134 (accessed on 25 April 2021).
- Evanega, S.; Lynas, M.; Adams, J.; Smolenyak, K. Quantifying Sources and Themes in the COVID-19 ‘Infodemic’. Available online: https://allianceforscience.cornell.edu/wp-content/uploads/2020/09/Evanega-et-al-Coronavirus-misinformationFINAL.pdf (accessed on 25 April 2021).
- John Hopkins University. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. Available online: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed on 25 April 2021).
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Deutsche Presse-Agentur (dpa). Genesener Bolsonaro geht auf Tuchfühlung. Available online: https://www.spiegel.de/ausland/corona-krise-in-brasilien-jair-bolsonaro-schuettelt-haende-in-der-menschenmenge-a-3f7af07f-a867-4aac-bfc5-14518504c7bd (accessed on 25 April 2021).
- Shokoohi, M.; Nasiri, N.; Sharifi, H.; Baral, S.; Stranges, S. A syndemic of COVID-19 and methanol poisoning in Iran: Time for Iran to consider alcohol use as a public health challenge? Alcohol 2020, 87, 25–27. [Google Scholar] [CrossRef]
- Gensing, P. Angstmache, Falschmeldungen und Gerüchte. Available online: https://www.tagesschau.de/faktenfinder/impfen-fakenews-101.html (accessed on 25 April 2021).
- World Health Organization. Working together to tackle the “infodemic”. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/6/working-together-to-tackle-the-infodemic (accessed on 25 April 2021).
- Betsch, C.; Wieler, L.; Bosnjak, M.; Ramharter, M.; Stollorz, V.; Omer, S.; Korn, L.; Sprengholz, P.; Felgendreff, L.; Eitze, S.; et al. COVID-19 Snapshot MOnitoring (COSMO): Monitoring Knowledge, Risk Perceptions, Preventive Behaviours, and Public Trust in the Current Coronavirus Outbreak; PsychArchives: Trier, Germany, 2020. [Google Scholar] [CrossRef]
- Betsch, C. How behavioural science data helps mitigate the COVID-19 crisis. Nat. Hum. Behav. 2020, 4, 438. [Google Scholar] [CrossRef] [Green Version]
- Brewer, N.T.; Weinstein, N.D.; Cuite, C.L.; Herrington, J.E. Risk perceptions and their relation to risk behavior. Ann. Behav. Med. 2004, 27, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Bish, A.; Michie, S. Demographic and attitudinal determinants of protective behaviours during a pandemic: A review. Br. J. Health Psychol. 2010, 15, 797–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glöckner, A.; Dorrough, A.R.; Wingen, T.; Dohle, S. The Perception of Infection Risks during the Early and Later Outbreak of COVID-19 in Germany: Consequences and Recommendations. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Brewer, N.T.; Chapman, G.B.; Gibbons, F.X.; Gerrard, M.; McCaul, K.D.; Weinstein, N.D. Meta-analysis of the relationship between risk perception and health behavior: The example of vaccination. Health Psychol. 2007, 26, 136–145. [Google Scholar] [CrossRef] [Green Version]
- Ferrer, R.; Klein, W.M. Risk perceptions and health behavior. Curr. Opin. Psychol. 2015, 5, 85–89. [Google Scholar] [CrossRef] [Green Version]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; Spiegelhalter, D.; van der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Majid, U.; Wasim, A.; Bakshi, S.; Truong, J. Knowledge, (mis-)conceptions, risk perception, and behavior change during pandemics: A scoping review of 149 studies. Public Underst. Sci. 2020, 29, 777–799. [Google Scholar] [CrossRef] [PubMed]
- Rohrmann, B. Risk Perception, Risk Attitude, Risk Communication, Risk Management: A Conceptual Appraisal. In Proceedings of the International Emergency Management Society Annual Conference, Prague, Czech Republic, 17–19 June 2008. [Google Scholar]
- Slovic, P. Perception of risk. Science 1987, 236, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Eitze, S.; Felgendreff, L.; Korn, L.; Sprengholz, P.; Allen, J.; Jenny, M.A.; Wieler, L.H.; Thaiss, H.; De Bock, F.; Betsch, C. Public trust in institutions in the first half of the Corona pandemic: Findings from the COVID-19 Snapshot Monitoring (COSMO) project. Bundesgesundheitsblatt Gesundh. Gesundh. 2021. [Google Scholar] [CrossRef]
- Dohle, S.; Wingen, T.; Schreiber, M. Acceptance and Adoption of Protective Measures During the COVID-19 Pandemic: The Role of Trust in Politics and Trust in Science. PsychArchives 2020. [Google Scholar] [CrossRef]
- Moran, C.; Campbell, D.J.T.; Campbell, T.S.; Roach, P.; Bourassa, L.; Collins, Z.; Stasiewicz, M.; McLane, P. Predictors of attitudes and adherence to COVID-19 public health guidelines in Western countries: A rapid review of the emerging literature. J. Public Health 2021. [Google Scholar] [CrossRef]
- Roozenbeek, J.; Schneider, C.R.; Dryhurst, S.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; van der Linden, S. Susceptibility to misinformation about COVID-19 around the world. R. Soc. Open Sci. 2020, 7, 201199. [Google Scholar] [CrossRef]
- Allington, D.; Duffy, B.; Wessely, S.; Dhavan, N.; Rubin, J. Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency. Psychol. Med. 2020, 1–7. [Google Scholar] [CrossRef]
- Ruiz, J.B.; Bell, R.A. Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 2021, 39, 1080–1086. [Google Scholar] [CrossRef]
- Karlsson, L.C.; Soveri, A.; Lewandowsky, S.; Karlsson, L.; Karlsson, H.; Nolvi, S.; Karukivi, M.; Lindfelt, M.; Antfolk, J. Fearing the disease or the vaccine: The case of COVID-19. Pers. Individ. Dif. 2021, 172, 110590. [Google Scholar] [CrossRef]
- Koos, S. Die “Querdenker“. Wer nimmt an Corona-Protesten teil und warum? Ergebnisse einer Befragung während der “Corona-Proteste” am 4.10.2020 in Konstanz. Available online: http://nbn-resolving.de/urn:nbn:de:bsz:352-2-bnrddxo8opad0 (accessed on 19 January 2021).
- COVID-19 Snapshot Monitoring (COSMO). Available online: https://projekte.uni-erfurt.de/cosmo2020/web/topic/impfung/10-impfungen/#impfabsicht-impfpflicht (accessed on 11 July 2020).
- Leiner, D.J. SoSci Survey (Version 3.1.06). Available online: www.soscisurvey.de (accessed on 25 April 2021).
- Faasse, K.; Newby, J. Public Perceptions of COVID-19 in Australia: Perceived Risk, Knowledge, Health-Protective Behaviors, and Vaccine Intentions. Front. Psychol. 2020, 11, 551004. [Google Scholar] [CrossRef]
- Livingston, E.; Bucher, K. Coronavirus Disease 2019 (COVID-19) in Italy. JAMA 2020, 323, 1335. [Google Scholar] [CrossRef] [Green Version]
- Aerzteblatt. Drei Viertel der Ärzte Wollen Sich Gegen SARS-CoV-2 Impfen Lassen. Available online: https://www.aerzteblatt.de/nachrichten/119400/Drei-Viertel-der-Aerzte-wollen-sich-gegen-SARS-CoV-2-impfen-lassen (accessed on 13 July 2021).
- Falcone, R.; Sapienza, A. How COVID-19 Changed the Information Needs of Italian Citizens. Int. J. Environ. Res. Public Health 2020, 17, 6988. [Google Scholar] [CrossRef]
- Oksanen, A.; Kaakinen, M.; Latikka, R.; Savolainen, I.; Savela, N.; Koivula, A. Regulation and Trust: 3-Month Follow-up Study on COVID-19 Mortality in 25 European Countries. JMIR Public Health Surveill. 2020, 6, e19218. [Google Scholar] [CrossRef] [PubMed]
- Loss, J.; Boklage, E.; Jordan, S.; Jenny, M.A.; Weishaar, H.; El Bcheraoui, C. Risk communication in the containment of the COVID-19 pandemic: Challenges and promising approaches. Bundesgesundheitsblatt Gesundh. Gesundh. 2021, 64, 294–303. [Google Scholar] [CrossRef]
- Schaefer, C.; Bitzer, E. Dealing with Misinformation in Media. Available online: https://www.public-health-covid19.de/images/2020/Ergebnisse/200526-Fake-News-V2-engl.pdf (accessed on 25 April 2021).
- Habersaat, K.B.; Betsch, C.; Danchin, M.; Sunstein, C.R.; Bohm, R.; Falk, A.; Brewer, N.T.; Omer, S.B.; Scherzer, M.; Sah, S.; et al. Ten considerations for effectively managing the COVID-19 transition. Nat. Hum. Behav. 2020, 4, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.W.; Chen, Y.L.; Chang, Y.P.; Wu, C.F.; Lu, W.H.; Yen, C.F. Sources of COVID-19-Related Information in People with Various Levels of Risk Perception and Preventive Behaviors in Taiwan: A Latent Profile Analysis. Int. J. Environ. Res. Public Health 2021, 18, 2091. [Google Scholar] [CrossRef]
- Rosenberg, H.; Syed, S.; Rezaie, S. The Twitter pandemic: The critical role of Twitter in the dissemination of medical information and misinformation during the COVID-19 pandemic. CJEM 2020, 22, 418–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atehortua, N.A.; Patino, S. COVID-19, a tale of two pandemics: Novel coronavirus and fake news messaging. Health Promot. Int. 2020. [Google Scholar] [CrossRef]
- Larson, H.J. Blocking information on COVID-19 can fuel the spread of misinformation. Nature 2020, 580, 306. [Google Scholar] [CrossRef] [Green Version]
- Larson, H.J. The biggest pandemic risk? Viral misinformation. Nature 2018, 562, 309. [Google Scholar] [CrossRef] [Green Version]
- Bavel, J.J.V.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Thomson, A.; Robinson, K.; Vallee-Tourangeau, G. The 5As: A practical taxonomy for the determinants of vaccine uptake. Vaccine 2016, 34, 1018–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Frequency (n) | Percentage (%) |
|---|---|---|
| Gender | n = 808 | |
| Female | 557 | 68.9 |
| Male | 250 | 30.9 |
| Divers | 1 | 0.1 |
| Political attitude | n = 674 | |
| Left-wing | 449 | 66.6 |
| Conservative-liberal | 118 | 17.5 |
| Right-wing populism | 17 | 2.5 |
| Non-voter | 90 | 13.4 |
| Level of education | n = 791 | |
| Scholar | 24 | 3.0 |
| Student | 145 | 18.3 |
| General secondary school | 83 | 10.5 |
| Intermediate secondary school | 114 | 14.4 |
| Technical college | 55 | 7.0 |
| Grammar school | 92 | 11.6 |
| University of Applied Sciences | 61 | 7.7 |
| University degree | 217 | 27.4 |
| Working status | n = 801 | |
| Working | 481 | 60.1 |
| Seeking work | 46 | 5.7 |
| Pension | 146 | 18.2 |
| No, other | 128 | 16.0 |
| Working sector | n = 591 | |
| Education | 77 | 9.5 |
| Hospitality industry | 19 | 2.3 |
| Health industry | 166 | 20.4 |
| Marketing | 53 | 6.5 |
| Arts, wellness, leisure | 29 | 3.6 |
| Public administration | 63 | 5.3 |
| Manufacturing | 35 | 4.3 |
| Other | 149 | 18.4 |
| COVID-19 Information Sources | n = 795 | |
| Public media | 564 | 68.7 |
| Private TV-channels | 101 | 12.7 |
| Daily Journals | 254 | 32.0 |
| Online news | 276 | 34.7 |
| Family and relatives | 192 | 24.2 |
| Search engines | 228 | 28.7 |
| Health authorities | 422 | 53.1 |
| Social media | 166 | 20.9 |
| Celebrities | 5 | 0.6 |
| Radio | 252 | 31.7 |
| Podcasts | 107 | 13.5 |
| Risk perception | When the global pandemic was declared by the WHO in March 2020, what was your attitude towards the Coronavirus? | ||
| I was worried about my health or the health of my relatives | 270 (34.6%) | ||
| I didn’t feel threated | 511 (65.4%) | ||
| If your perception changed since then, what did change? | |||
| I currently perceive the Coronavirus as less dangerous | 142 (38.1%) | ||
| I currently perceive the Coronavirus as more dangerous | 231 (61.9%) | ||
| Please indicate whether you agree on the following statements or not | Strongly agree or agree | Strongly disagree or disagree | |
| I am worried that I may get infected with the virus | 417 (56.5%) | 321 (43.5%) | |
| I am worried that an infection with the Coronavirus could threat my health or the health of my relatives | 634 (85.7%) | 106 (14.3%) | |
| I think that the Coronavirus gets too much attention | 203 (27.7%) | 530 (72.3%) | |
| Vaccination Intention * | As soon as a Coronavirus vaccine is available, I would get vaccinated with the new vaccine | 478 (63.5%) | 180 (23.9%) |
| Trust in Institutions/ persons for reliable medical information | German Federal Ministry of Health (BMG) | 616 (87.3%) | 90 (12.7%) |
| World health organization/Robert Koch institute (WHO/RKI) | 621 (86.7%) | 68 (9.5%) | |
| Family physicians | 598 (88.6%) | 77 (11.4%) | |
| Family/friends | 334 (51.1%) | 320 (48.9%) | |
| Own research | 496 (77.9%) | 141 (22.1%) | |
| Health Protective Measures | Which SARS-CoV-2 health protective measures do you apply in your daily life? | ||
| Wearing face mask | 690 (92.7%) | ||
| Regular hand-disinfection | 511 (68.9%) | ||
| Washing hands for 20 s | 584 (78.5%) | ||
| Staying at least 1.50 m apart from anyone outside of the own household | 644 (86.6%) | ||
| Staying home when feeling sick | 580 (78.0%) | ||
| None | 5 (0.7%) | ||
| SARS-CoV-2 as a Health Threat n (%) | p-Value * | Vaccination Yes n (%) | Vaccination No n (%) | Vaccination Uncertain n (%) | p-Value * | |
|---|---|---|---|---|---|---|
| Gender | ||||||
| Male | 193 (83.2) | <0.05 | 168 (71.5) | 42 (17.9) | 25 (10.6) | |
| Female | 437 (86.9) | 308 (60.0) | 135 (26.3) | 70 (13.7) | <0.05 | |
| Diverse | 0(0) | 0 (0) | 1 (100) | 0 (0) | ||
| Political Ideology | ||||||
| Conservative-liberal | 148 (87.6) | <0.01 | 114 (65.1) | 36 (20.6) | 25 (14.3) | |
| Left | 376 (89.7) | 293 (69.4) | 75 (17.8) | 54 (12.8) | <0.01 | |
| Right-voter | 5 (38.5) | 4 (28.6) | 9 (64.3) | 1 (7.1) | ||
| Non-voter # | 56 (69.1) | <0.01 | 29 (34.9) | 44 (53.0) | 10 (12.1) | <0.01 |
| COVID Information Sources | ||||||
| Public media yes | 457 (88.4) | <0.01 | 361 (68.9) | 103 (19.7) | 60 (11.5) | |
| Public media no | 177 (79.4) | 117 (51.1) | 77 (33.6) | 35 (15.3) | <0.01 | |
| Daily journal yes | 213 (89.9) | 176 (71.8) | 41 (16.7) | 28 (11.4) | ||
| Daily journal no | 421 (83.7) | <0.05 | 302 (59.5) | 139 (27.4) | 67 (13.2) | <0.01 |
| Online news yes | 229 (87.7) | 173 (65.5) | 48 (18.2) | 43 (16.3) | ||
| Online news no | 405 (84.6) | 0.24 | 305 (62.4) | 132 (27.0) | 52 (10.6) | <0.01 |
| Health authorities yes | 360 (89.6) | 276 (67.8) | 84 (20.6) | 47 (11.6) | ||
| Health authorities no | 274 (81.1) | <0.01 | 202 (58.4) | 96 (27.8) | 48 (13.9) | <0.05 |
| Social media yes | 127 (81.4) | 82 (52.2) | 49 (31.2) | 26 (16.6) | ||
| Social media no | 507(86.8) | 0.09 | 396 (66.4) | 131 (22.0) | 69 (12.0) | <0.01 |
| Trust in Institutions | ||||||
| BMG yes | 543 (89.9) | 428 (70.0) | 111 (18.2) | 72 (11.8) | ||
| BMG no | 47 (53.4) | <0.01 | 26 (29.2) | 55 (61.8) | 8 (9.0) | <0.01 |
| WHO/RKI yes | 573 (90.4) | 448 (69.7) | 118 (18.4) | 77 (12.0) | ||
| WHO/RKI no | 25 (37.9) | <0.01 | 13 (19.7) | 48 (72.7) | 5 (7.6) | <0.01 |
| Family physician yes | 506 (86.9) | 398 (67.0) | 124 (20.9) | 72 (12.1) | ||
| Family physician no | 62 (81.6) | <0.05 | 39 (53.4) | 27 (37.0) | 7 (9.6) | <0.01 |
| Use of social networks and messenger services | ||||||
| Telegram yes | 119 (78.3) | 90 (58.8) | 48 (31.4) | 15 (9.8) | ||
| Telegram no | 515 (87.6) | <0.01 | 388 (64.7) | 132 (22.0) | 80 (13.3) | <0.05 |
| Facebook yes | 353 (83.7) | 256 (60.4) | 118 (27.8) | 50 (11.8) | ||
| Facebook no | 281 (88.4) | 0.07 | 222 (67.5) | 62 (18.8) | 45 (13.7) | <0.05 |
| Twitter yes | 72 (87.8) | 54 (64.3) | 17 (20.2) | 13 (15.5) | ||
| Twitter no | 562 (85.4) | 0.56 | 424 (63.4) | 163 (24.4) | 82 (12.3) | 0.56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Far Cardo, A.; Kraus, T.; Kaifie, A. Factors That Shape People’s Attitudes towards the COVID-19 Pandemic in Germany—The Influence of MEDIA, Politics and Personal Characteristics. Int. J. Environ. Res. Public Health 2021, 18, 7772. https://doi.org/10.3390/ijerph18157772
El-Far Cardo A, Kraus T, Kaifie A. Factors That Shape People’s Attitudes towards the COVID-19 Pandemic in Germany—The Influence of MEDIA, Politics and Personal Characteristics. International Journal of Environmental Research and Public Health. 2021; 18(15):7772. https://doi.org/10.3390/ijerph18157772
Chicago/Turabian StyleEl-Far Cardo, Aida, Thomas Kraus, and Andrea Kaifie. 2021. "Factors That Shape People’s Attitudes towards the COVID-19 Pandemic in Germany—The Influence of MEDIA, Politics and Personal Characteristics" International Journal of Environmental Research and Public Health 18, no. 15: 7772. https://doi.org/10.3390/ijerph18157772