
The Impact of the Early COVID-19 Pandemic on ST-Segment Elevation Myocardial Infarction Presentation and Outcomes—A Systematic Review and Meta-Analysis


 and
and
Abstract
:1. Introduction
2. Materials and Methods
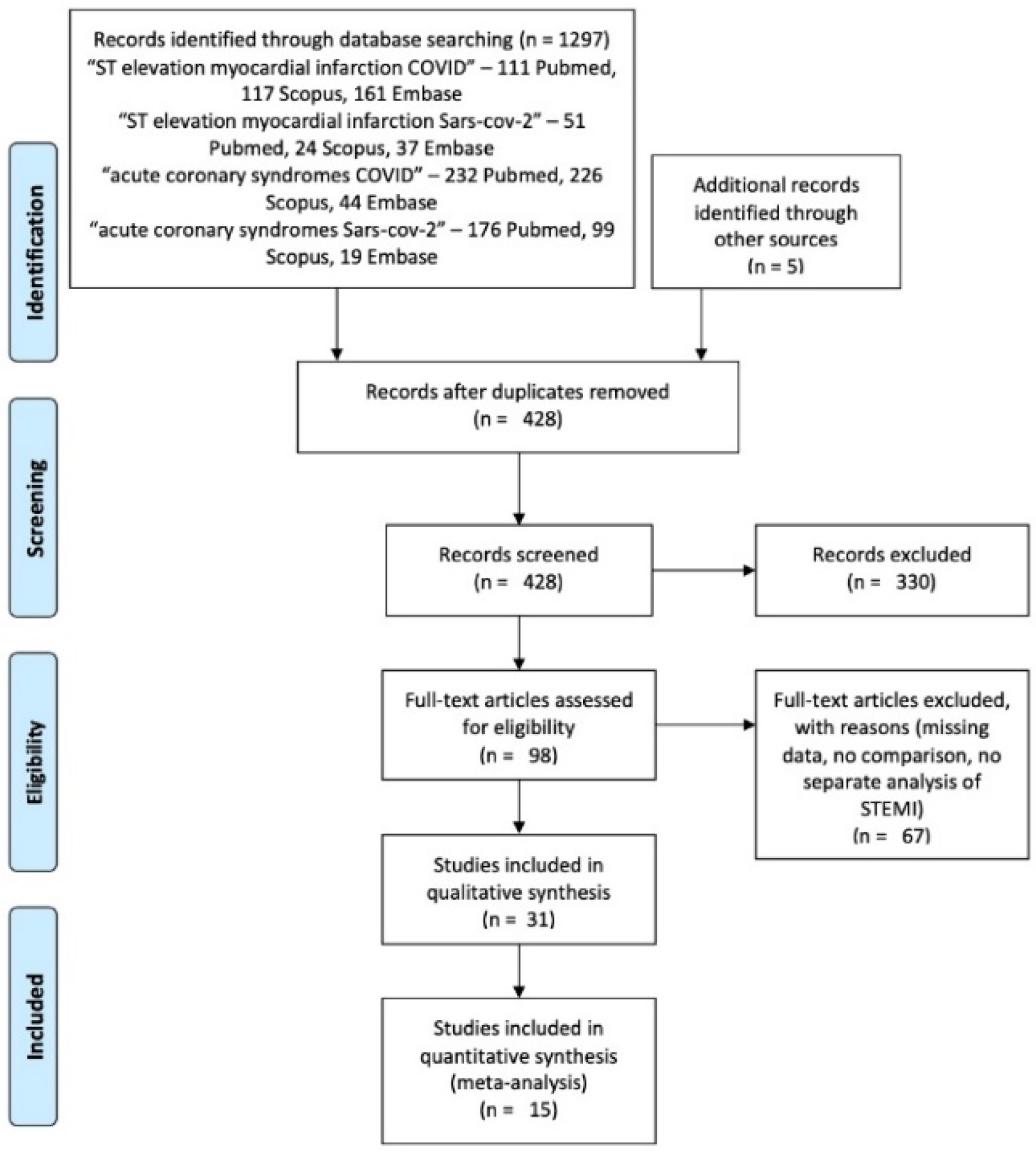
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Patients’ Profile
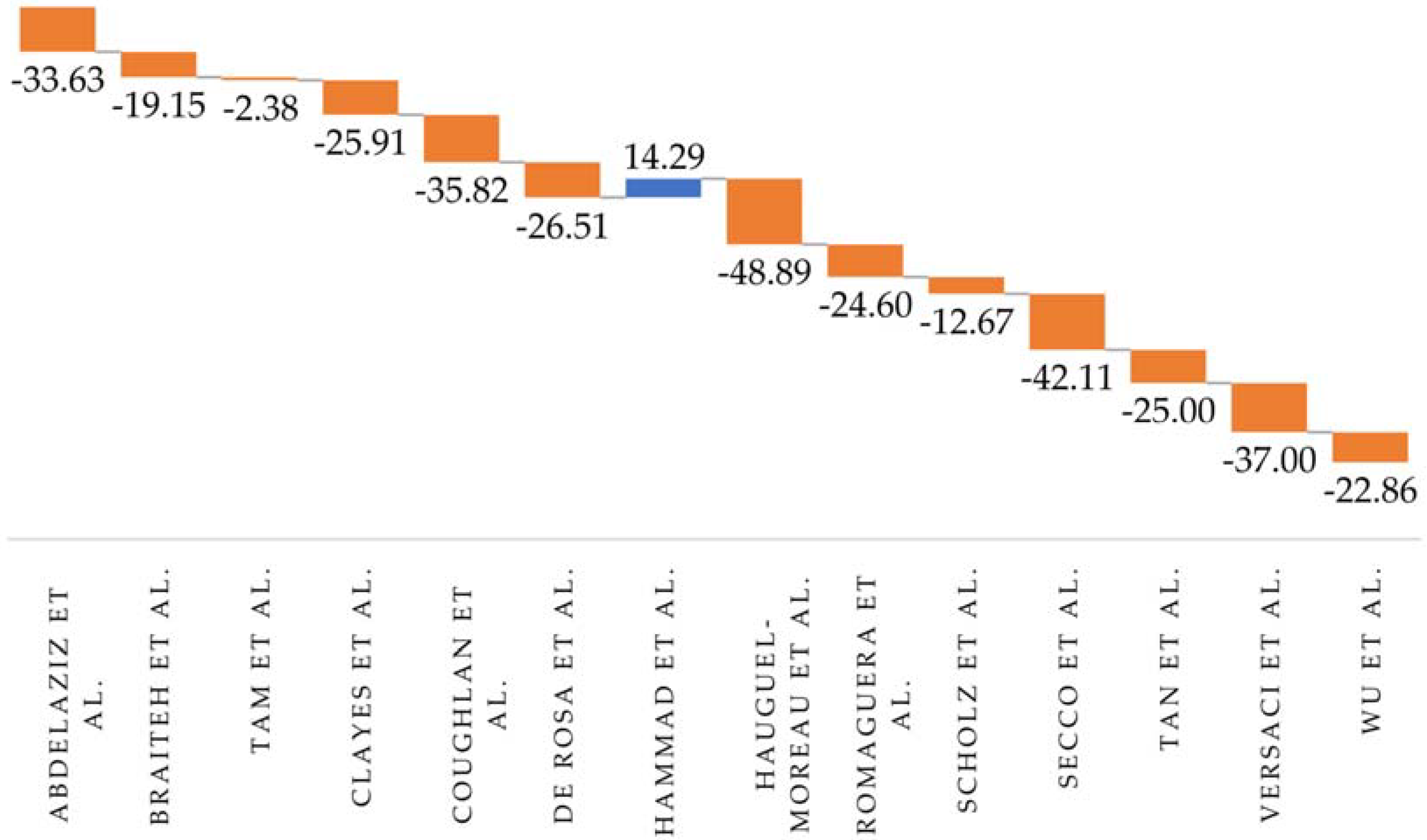
3.2. STEMI Presentation
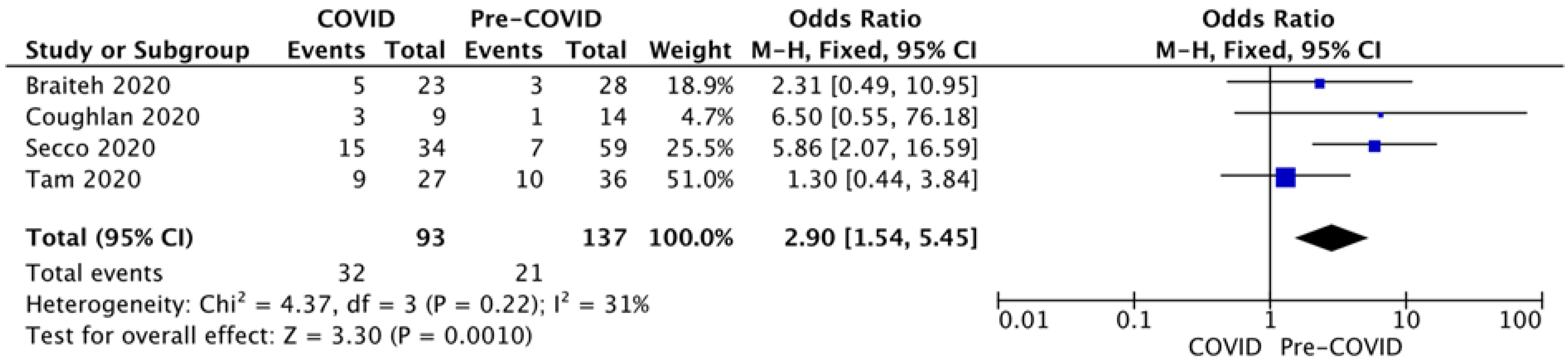
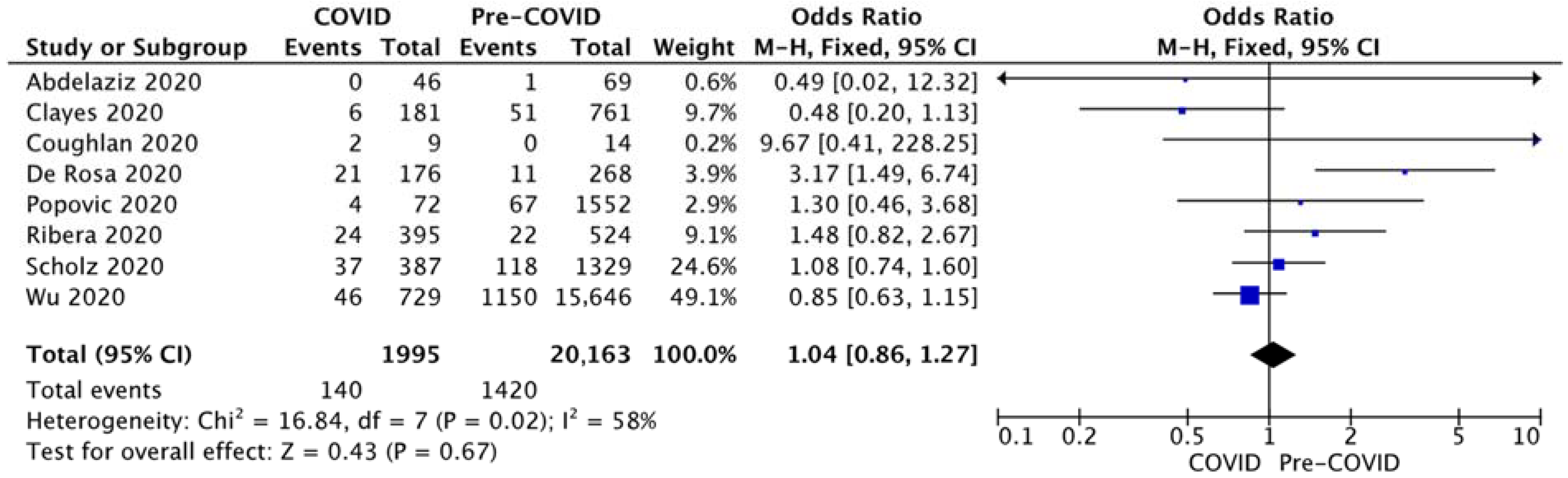
3.3. STEMI Outcome
4. Discussion
4.1. Patients’ Profile
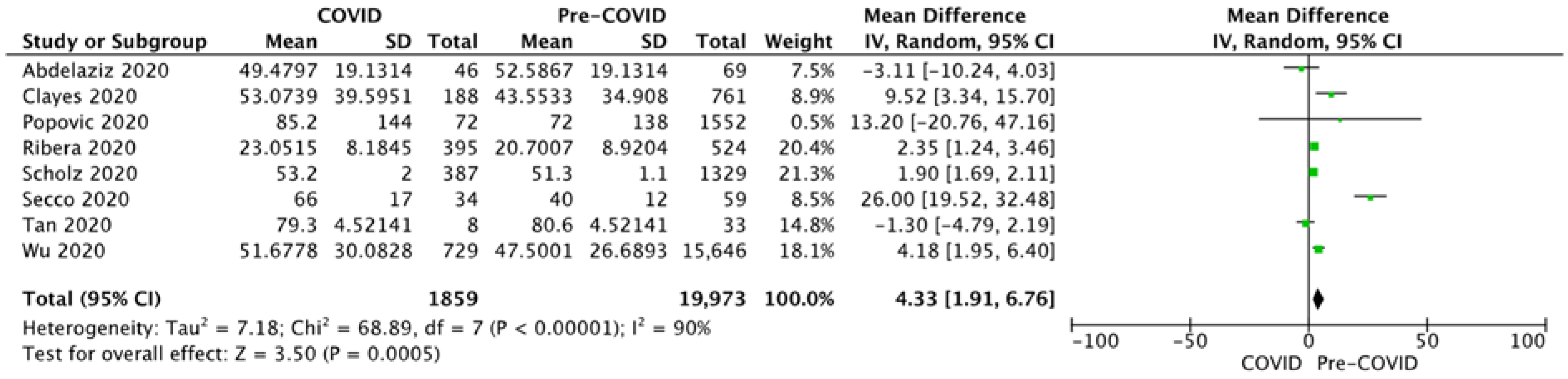
4.2. STEMI Presentation
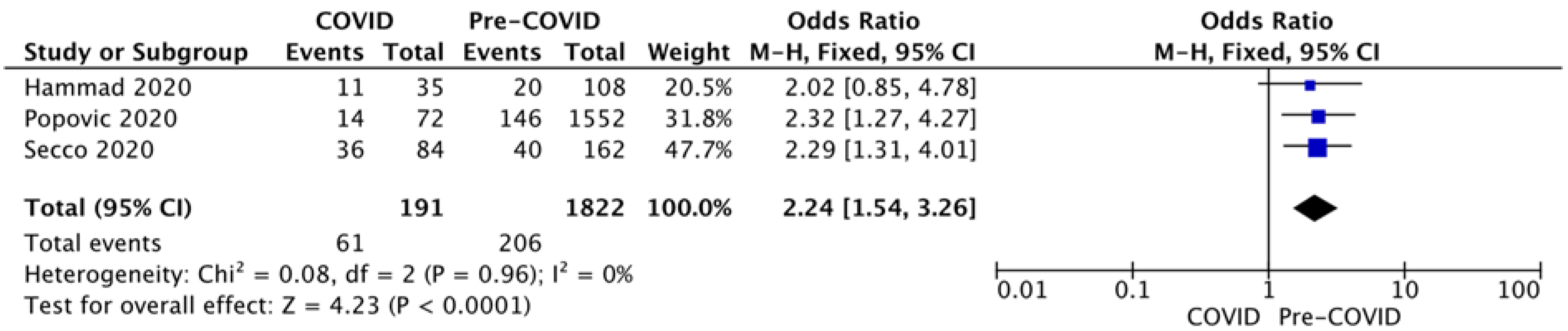
4.3. STEMI Outcome
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Chen, J.; Lu, H.; Melino, G.; Boccia, S.; Piacentini, M.; Ricciardi, W.; Wang, Y.; Shi, Y.; Zhu, T. COVID-19 infection: The China and Italy perspectives. Cell Death Dis. 2020, 11, 438. [Google Scholar] [CrossRef] [PubMed]
- Hammad, T.A.; Parikh, M.; Tashtish, N.; Lowry, C.M.; Gorbey, D.; Forouzandeh, F.; Filby, S.J.; Wolf, W.M.; Costa, M.A.; Simon, D.I.; et al. Impact of COVID-19 pandemic on ST-elevation myocardial infarction in a non-COVID-19 epicenter. Catheter. Cardiovasc. Interv. 2020, 97, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Abdelaziz, H.K.; Abdelrahman, A.; Nabi, A.; Debski, M.; Mentias, A.; Choudhury, T.; Patel, B.; Saad, M. Impact of COVID-19 pandemic on patients with ST-segment elevation myocardial infarction: Insights from a British cardiac center. Am. Heart J. 2020, 226, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Braiteh, N.; Rehman, W.U.; Alom, M.; Skovira, V.; Breiteh, N.; Rehman, I.; Yarkoni, A.; Kahsou, H.; Rehman, A. Decrease in acute coronary syndrome presentations during the COVID-19 pandemic in upstate New York. Am. Heart J. 2020, 226, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Tam, C.F.; Cheung, K.S.; Lam, S.; Wong, A.; Yung, A.; Sze, M.; Fang, J.; Tse, H.F.; Siu, C.W. Impact of coronavirus disease 2019 (COVID-19) outbreak on outcome of myocardial infarction in Hong Kong, China. Catheter. Cardiovasc. Interv. 2020, 97, E194–E197. [Google Scholar] [CrossRef] [PubMed]
- Claeys, M.J.; Argacha, J.F.; Collart, P.; Carlier, M.; Van Caenegem, O.; Sinnaeve, P.R.; Desmet, W.; Dubois, P.; Stammen, F.; Gevaert, S.; et al. Impact of COVID-19-related public containment measures on the ST elevation myocardial infarction epidemic in Belgium: A nationwide, serial, cross-sectional study. Acta Cardiol. 2020, 76, 863–869. [Google Scholar] [CrossRef]
- Coughlan, J.J.; Chongprasertpon, N.; Arockiam, S.; Arnous, S.; Kiernan, T.J. COVID-19 and STEMI: A snapshot analysis of presentation patterns during a pandemic. Int. J. Cardiol. Heart Vasc. 2020, 30, 100546. [Google Scholar] [CrossRef]
- De Rosa, S.; Spaccarotella, C.; Basso, C.; Calabro, M.P.; Curcio, A.; Filardi, P.P.; Mancone, M.; Mercuro, G.; Muscoli, S.; Nodari, S.; et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur. Heart J. 2020, 41, 2083–2088. [Google Scholar] [CrossRef]
- Hauguel-Moreau, M.; Pillière, R.; Prati, G.; Beaune, S.; Loeb, T.; Lannou, S.; Mallet, S.; Mustafic, H.; Bégué, C.; Dubourg, O.; et al. Impact of Coronavirus Disease 2019 outbreak on acute coronary syndrome admissions: Four weeks to reverse the trend. J. Thromb. Thrombolysis 2021, 51, 31–32. [Google Scholar] [CrossRef]
- Popovic, B.; Varlot, J.; Metzdorf, P.A.; Jeulin, H.; Goehringer, F.; Camenzind, E. Changes in characteristics and management among patients with ST-elevation myocardial infarction due to COVID-19 infection. Catheter. Cardiovasc. Interv. 2021, 97, E319–E326. [Google Scholar] [CrossRef]
- Romaguera, R.; Ribera, A.; Güell-Viaplana, F.; Tomás-Querol, C.; Muñoz-Camacho, J.F.; Agudelo, V. Decrease in ST-segment elevation myocardial infarction admissions in Catalonia during the COVID-19 pandemic. Rev. Esp. Cardiol. 2020, 73, 778–780. [Google Scholar] [CrossRef] [PubMed]
- Scholz, K.H.; Lengenfelder, B.; Thilo, C.; Jeron, A.; Stefanow, S.; Janssens, U.; Bauersachs, J.; Schulze, P.C.; Winter, K.D.; Schröder, J.; et al. Impact of COVID-19 outbreak on regional STEMI care in Germany. Clin. Res. Cardiol. 2020, 109, 1511–1521. [Google Scholar] [CrossRef] [PubMed]
- Secco, G.G.; Zocchi, C.; Parisi, R.; Roveta, A.; Mirabella, F.; Vercellino, M.; Pistis, G.; Reale, M.; Maggio, S.; Audo, A.; et al. Decrease and Delay in Hospitalization for Acute Coronary Syndromes during the 2020 SARS-CoV-2 Pandemic. Can. J. Cardiol. 2020, 36, 1152–1155. [Google Scholar] [CrossRef]
- Tan, W.; Parikh, R.V.; Chester, R.; Harrell, J.; Franco, V.; Aksoy, O.; Dave, R.; Rafique, A.; Press, M. Single Center Trends in Acute Coronary Syndrome Volume and Outcomes during the COVID-19 Pandemic. Cardiol. Res. 2020, 11, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Versaci, F.; Gaspardone, A.; Danesi, A.; Ferranti, F.; Mancone, M.; Mariano, E.; Rotolo, F.L.; Musto, C.; Proietti, I.; Berni, A.; et al. Interplay between COVID-19, pollution, and weather features on changes in the incidence of acute coronary syndromes in early 2020. Int. J. Cardiol. 2021, 329, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Mamas, M.; Rashid, M.; Weston, C.; Hains, J.; Luescher, T.; de Belder, M.A.; Deanfield, J.E.; Gale, C.P. Patient response, treatments, and mortality for acute myocardial infarction during the COVID-19 pandemic. Eur. Heart J. Qual. Care Clin. Outcomes 2020, 7, 238–246. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; Updated March 2011; The Cochrane Collaboration: London, UK, 2011; Available online: www.handbook.cochrane.org (accessed on 28 August 2021).
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Toner, L.; Koshy, A.N.; Hamilton, G.W.; Clark, D.; Farouque, O.; Yudi, M.B. Acute coronary syndromes undergoing percutaneous coronary intervention in the COVID-19 era: Comparable case volumes but delayed symptom onset to hospital presentation. Eur. Heart J. Qual. Care Clin. Outcomes 2020, 6, 225–226. [Google Scholar] [CrossRef]
- Rattka, M.; Baumhardt, M.; Dreyhaupt, J.; Rothenbacher, D.; Thiessen, K.; Markovic, S.; Rottbauer, W.; Imhof, A. 31 days of COVID-19-cardiac events during restriction of public life—A comparative study. Clin. Res. Cardiol 2020, 109, 1476–1482. [Google Scholar] [CrossRef]
- Huet, F.; Prieur, C.; Schurtz, G.; Gerbaud, E.; Manzo-Silberman, S.; Vanzetto, G.; Elbaz, M.; Tea, V.; Mercier, G.; Lattuca, B.; et al. One train may hide another: Acute cardiovascular diseases could be neglected because of the COVID-19 pandemic. Arch. Cardiovasc. Dis. 2020, 113, 303–307. [Google Scholar] [CrossRef] [PubMed]
- De Filippo, O.; D’Ascenzo, F.; Angelini, F.; Bocchino, P.P.; Conrotto, F.; Saglietto, A.; Secco, G.G.; Campo, G.; Gallone, G.; Verardi, R.; et al. Reduced Rate of Hospital Admissions for ACS during COVID-19 Outbreak in Northern Italy. N. Engl. J. Med. 2020, 383, 88–89. [Google Scholar] [CrossRef] [PubMed]
- Papafaklis, M.I.; Katsouras, C.S.; Tsigkas, G.; Toutouzas, K.; Davlouros, P.; Hahalis, G.N.; Kousta, M.S.; Styliadis, I.G.; Triantafyllou, K.; Pappas, L.; et al. “Missing” acute coronary syndrome hospitalizations during the COVID-19 era in Greece: Medical care avoidance combined with a true reduction in incidence? Clin. Cardiol. 2020, 43, 1142–1149. [Google Scholar] [CrossRef] [PubMed]
- Kessler, T.; Graf, T.; Hilgendorf, I.; Rizas, K.; Martens, E.; Muhlen, C.V.Z.; Kraemer, P.; Meyer-Saraei, R.; Neumann, F.J.; Bode, C.; et al. Hospital Admissions with Acute Coronary Syndromes during the COVID-19 Pandemic in German Cardiac Care Units. Cardiovasc. Res. 2020, 116, 1800–1801. [Google Scholar] [CrossRef]
- Wilson, S.J.; Connolly, M.J.; Elghamry, Z.; Cosgrove, C.; Firoozi, S.; Lim, P.; Sharma, R.; Spratt, J.C. Effect of the COVID-19 Pandemic on ST-Segment-Elevation Myocardial Infarction Presentations and In-Hospital Outcomes. Circ. Cardiovasc. Interv. 2020, 13, e009438. [Google Scholar] [CrossRef]
- Firouzi, A.; Baay, M.; Mazayanimonfared, A.; Pouraliakbar, H.; Sadeghipour, P.; Noohi, F.; Maleki, M.; Peighambari, M.M.; Kiavar, M.; Abdi, S.; et al. Effects of the COVID-19 Pandemic on the Management of Patients With ST-elevation Myocardial Infarction in a Tertiary Cardiovascular Center. Crit. Pathw. Cardiol. 2021, 20, 53–55. [Google Scholar] [CrossRef]
- Reinstadler, S.J.; Reindl, M.; Lechner, I.; Holzknecht, M.; Tiller, C.; Roithinger, F.X.; Frick, M.; Hoppe, U.C.; Jirak, P.; Berger, R.; et al. Effect of the COVID-19 Pandemic on Treatment Delays in Patients with ST-Segment Elevation Myocardial Infarction. J. Clin. Med. 2020, 9, 2183. [Google Scholar] [CrossRef]
- Perelshtein Brezinov, O.; Klempfner, R.; Zekry, S.B.; Goldenberg, I.; Kuperstein, R. Prognostic value of ejection fraction in patients admitted with acute coronary syndrome: A real world study. Medicine 2017, 96, e6226. [Google Scholar] [CrossRef]
- De Luca, G.; Suryapranata, H.; Ottervanger, J.P.; Antman, E.M. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: Every minute of delay counts. Circulation 2004, 109, 1223–1225. [Google Scholar] [CrossRef] [Green Version]
- Pessoa-Amorim, G.; Camm, C.F.; Gajendragadkar, P.; De Maria, G.L.; Arsac, C.; Laroche, C.; Zamorano, J.L.; Weidinger, F.; Achenbach, S.; Maggioni, A.P.; et al. Admission of patients with STEMI since the outbreak of the COVID-19 pandemic: A survey by the European Society of Cardiology. Eur. Heart J. Qual. Care Clin. Outcomes 2020, 6, 210–216. [Google Scholar] [CrossRef]
- Nioi, M.; Napoli, P.E.; Finco, G.; Demontis, R.; Fossarello, M.; d’Aloja, E. Fear of the COVID-19 and medical liability. Insights from a series of 130 consecutives medico-legal claims evaluated in a single institution during SARS-CoV-2-related pandemic. Signa Vitae 2021, 17, 79–85. [Google Scholar] [CrossRef]
- Lee, A.; Morling, J. COVID19: The need for public health in a time of emergency. Public Health 2020, 182, 188–189. [Google Scholar] [CrossRef] [PubMed]
- Nioi, M.; Napoli, P.E.; Lobina, J.; Fossarello, M.; d’Aloja, E. COVID-19 and Italian Healthcare Workers from the Initial Sacrifice to the mRNA Vaccine: Pandemic Chrono-History, Epidemiological Data, Ethical Dilemmas, and Future Challenges. Front. Public Health 2020, 8, 591900. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Author | Type | No of Centres | Equivalent Time Periods | Groups | Number of STEMI Patients | SARS-CoV-2 Positive | Age, Years | Male, % |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Abdelaziz et al. [3] | Retrospective cross-sectional observational (STEMI) | 1 (UK) | Yes, 1–31 March 2019 1–31 March 2020 | Pre-COVID COVID | 69 46 | No/Not indicated | 66.6 ± 11.9 63.2 ± 11.1 | 76.8 69.6 |
| 2 | Braiteh et al. [4] | Retrospective cross-sectional observational (ACS, STEMI extracted) | 4 (NY, USA) | Yes, 1 March–30 April 2019 1 March–30 April 2020 | Pre-COVID COVID | 28 23 | No/Not indicated | 67.4 ± 16 58.6 ± 13 | 64.3 60.9 |
| 3 | Tam et al. [5] | Retrospective cross-sectional observational (ACS, STEMI extracted) | 1 (Hong-Kong) | No, 1 November 2019–24 January 2020 25 January 2020–31 March 2020 | Pre-COVID COVID | 36 27 | - | Not specified for STEMI | Not specified for STEMI |
| 4 | Clayes et al. [6] | Retrospective cross-sectional observational (STEMI) | Multiple (Belgium, national registry) | No, 13 March–3 April 2017, 2018, 2019 13 March–3 April 2020 | Pre-COVID COVID | 761 188 | 7 (3.72%)—excluded from mortality | 63 ± 15 63 ± 12 | 74 80 |
| 5 | Coughlan et al. [7] | Retrospective cross-sectional observational (STEMI) | 1 (Ireland) | Yes, 27 March–17 April 2019 27 March–17 April 2020 | Pre-COVID COVID | 14 9 | No/Not indicated | 59 ± 10 58 ± 17 | 100 55 |
| 6 | De Rosa et al. [8] | Retrospective cross-sectional observational (ACS, STEMI extracted) | 54 (Italy, national survey) | Yes, 12–19 March 2019 12–19 March 2020 | Pre-COVID COVID | 268 197 | 21 (10.7%)—excluded from mortality | 65.4 ± 9.7 66.5 ± 10.2 | 75 79.69 |
| 7 | Hammad et al. [2] | Retrospective cross-sectional observational (STEMI) | 18 (OH, USA) | No, 1 January–22 March 2020 23 March 2020–15 April 2020 | Pre-COVID COVID | 108 35 | No/Not indicated | 61.8 ± 12.6 66 ± 10 | 72 49 |
| 8 | Hauguel-Moreau et al. [9] | Retrospective cross-sectional observational (ACS, STEMI extracted) | 1 (France) | No, 17 February–26 April 2018, 2019 17 February–26 April 2020 | Pre-COVID COVID | 63 16 | 1 (6.25%) | Not mentioned | Not mentioned |
| 9 | Popovic et al. [10] | Prospective cross-sectional observational (STEMI) | 1 (France) | No, All patients 2008–2017 26 February–10.05.2020 | Pre-COVID COVID | 1552 72 | No/Not indicated | 59.6 ± 12.9 62.5 ± 12.6 | 76.10 73.60 |
| 10 | Romaguera et al. [11] | Retrospective cross-sectional observational (STEMI) | 10 (Spain) | Yes, 1 March–19 April 2019 1 March–19 April 2020 | Pre-COVID COVID | 524 395 | No/Not indicated | 63.4 ± 0.6 61.9 ± 0.7 | 79.20 80.25 |
| 11 | Scholz et al. [12] | Retrospective cross-sectional observational (STEMI) | 41 (Germany) | No, 1–31 March 2017–2019 1–31 March 2020 | Pre-COVID COVID | 1329 387 | No/Not indicated | 63.6 ± 0.4 64.5 ± 0.7 | 73 72 |
| 12 | Secco et al. [13] | Retrospective cross-sectional observational (ACS, STEMI extracted) | 3 (Italy) | Yes, 1–31 March 2019 1–31 March 2020 | Pre-COVID COVID | 59 34 | Yes (number not mentioned for STEMI) | Not mentioned for STEMI | Not mentioned for STEMI |
| 13 | Tan et al. [14] | Retrospective cross-sectional observational (ACS, STEMI extracted) | 1 (CA, USA) | No, 23 December 2019–18 March 2020 19 March–12 April 2020 | Pre-COVID COVID | 33 8 | No/Not indicated | Not mentioned for STEMI | Not mentioned for STEMI |
| 14 | Versaci et al. [15] | Retrospective cross-sectional observational (STEMI) | 1 (Italy) | Yes, 1–19 March 2019 1–19 March 2020 | Pre-COVID COVID | 38 24 | No/Not indicated | Not mentioned | Not mentioned |
| 15 | Wu et al. [16] | Prospective cross-sectional observational (STEMI) | 99 (UK) | No, 1 January 2019–22 March 2020 23 March–19 April 2020 | Pre-COVID COVID | 15,646 729 | No/Not indicated | 65.76 ± 13.44 64.64 ± 13.11 | 72 72 |
| No | Author | Selection | Comparability | Exposure | Score | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5.1 | 5.2 | 6 | 7 | N.A. | |||
| 1 | Abdelaziz et al. [3] | x | x | x | x | x | x | x | 7 | ||
| 2 | Braiteh et al. [4] | x | x | x | x | x | x | x | 7 | ||
| 3 | Tam et al. [5] | x | x | x | x | x | x | 6 | |||
| 4 | Clayes et al. [6] | x | x | x | x | x | x | 6 | |||
| 5 | Coughlan et al. [7] | x | x | x | x | x | x | 6 | |||
| 6 | De Rosa et al. [8] | x | x | x | x | x | x | x | 7 | ||
| 7 | Hammad et al. [2] | x | x | x | x | x | x | x | 7 | ||
| 8 | Hauguel-Moreau et al. [9] | x | x | x | x | x | x | 6 | |||
| 9 | Popovic et al. [10] | x | x | x | x | x | x | x | 7 | ||
| 10 | Romaguera et al. [11] | x | x | x | x | x | x | x | 7 | ||
| 11 | Scholz et al. [12] | x | x | x | x | x | x | x | 7 | ||
| 12 | Secco et al. [13] | x | x | x | x | x | x | 6 | |||
| 13 | Tan et al. [14] | x | x | x | x | x | x | 6 | |||
| 14 | Versaci et al. [15] | x | x | x | x | x | x | 6 | |||
| 15 | Wu et al. [16] | x | x | x | x | x | x | x | 7 | ||
| Pre-COVID-19 | COVID-19 | p | |
|---|---|---|---|
| Age (mean ± SD) (10 studies) | 64.96 ± 12.90 | 63.98 ± 9.9 | 0.0008 |
| Male patients (n, %) (10 studies) | 14,732 (72.58) | 1545 (74.24) | 0.103 |
| Arterial hypertension (n, %) (7 studies) | 7942 (40.77) | 660 (45.02) | 0.00143 |
| Diabetes mellitus (n, %) (7 studies) | 3662 (18.80) | 307 (20.94) | <0.001 |
| Smoking (n, %) (6 studies) | 6239 (33.33) | 452 (35.36) | <0.001 |
| Dyslipidaemia (n, %) (5 studies) | 4576 (24.59) | 3232 (25.98) | <0.001 |
| Family history (n, %) (3 studies) | 242 (17.14%) | 88 (19.91%) | 0.18 |
| Known coronary artery disease (n, %) (3 studies) | 229 (11.91) | 102 (12.32) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Furnica, C.; Chistol, R.O.; Chiran, D.A.; Stan, C.I.; Sargu, G.D.; Girlescu, N.; Tinica, G. The Impact of the Early COVID-19 Pandemic on ST-Segment Elevation Myocardial Infarction Presentation and Outcomes—A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 588. https://doi.org/10.3390/diagnostics12030588
Furnica C, Chistol RO, Chiran DA, Stan CI, Sargu GD, Girlescu N, Tinica G. The Impact of the Early COVID-19 Pandemic on ST-Segment Elevation Myocardial Infarction Presentation and Outcomes—A Systematic Review and Meta-Analysis. Diagnostics. 2022; 12(3):588. https://doi.org/10.3390/diagnostics12030588
Chicago/Turabian StyleFurnica, Cristina, Raluca Ozana Chistol, Dragos Andrei Chiran, Cristinel Ionel Stan, Gabriela Dumachita Sargu, Nona Girlescu, and Grigore Tinica. 2022. "The Impact of the Early COVID-19 Pandemic on ST-Segment Elevation Myocardial Infarction Presentation and Outcomes—A Systematic Review and Meta-Analysis" Diagnostics 12, no. 3: 588. https://doi.org/10.3390/diagnostics12030588