
Reported Adverse Effects and Attitudes among Arab Populations Following COVID-19 Vaccination: A Large-Scale Multinational Study Implementing Machine Learning Tools in Predicting Post-Vaccination Adverse Effects Based on Predisposing Factors

 ,
,  , , ,
, , ,  , ,
, ,  ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Survey Instrument
2.3. Sample Size
2.4. Statistical Analysis
2.5. ML Prediction
3. Results
3.1. Participant Demographics
3.2. Health-Related Information
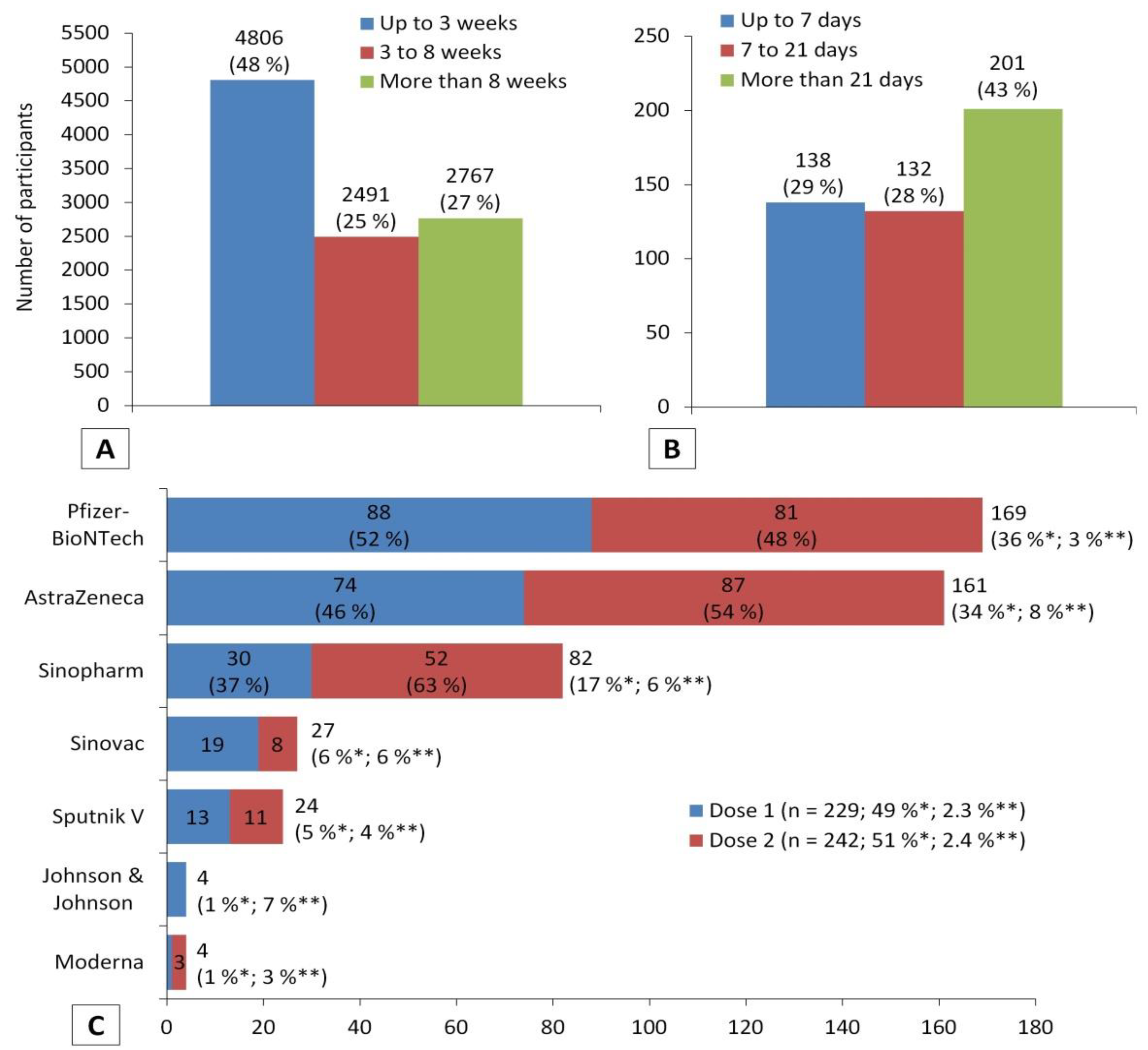
3.3. Vaccination Information
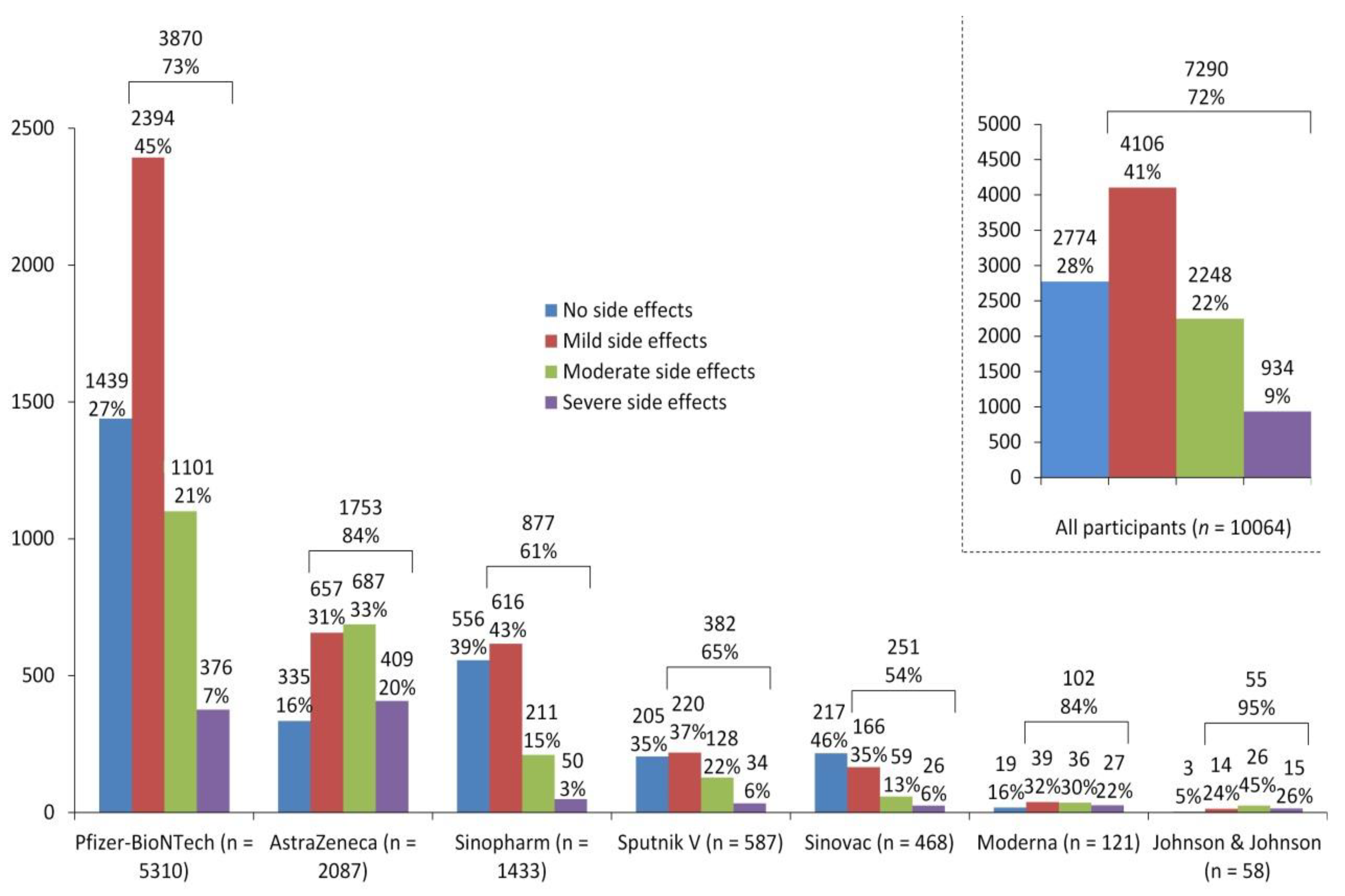
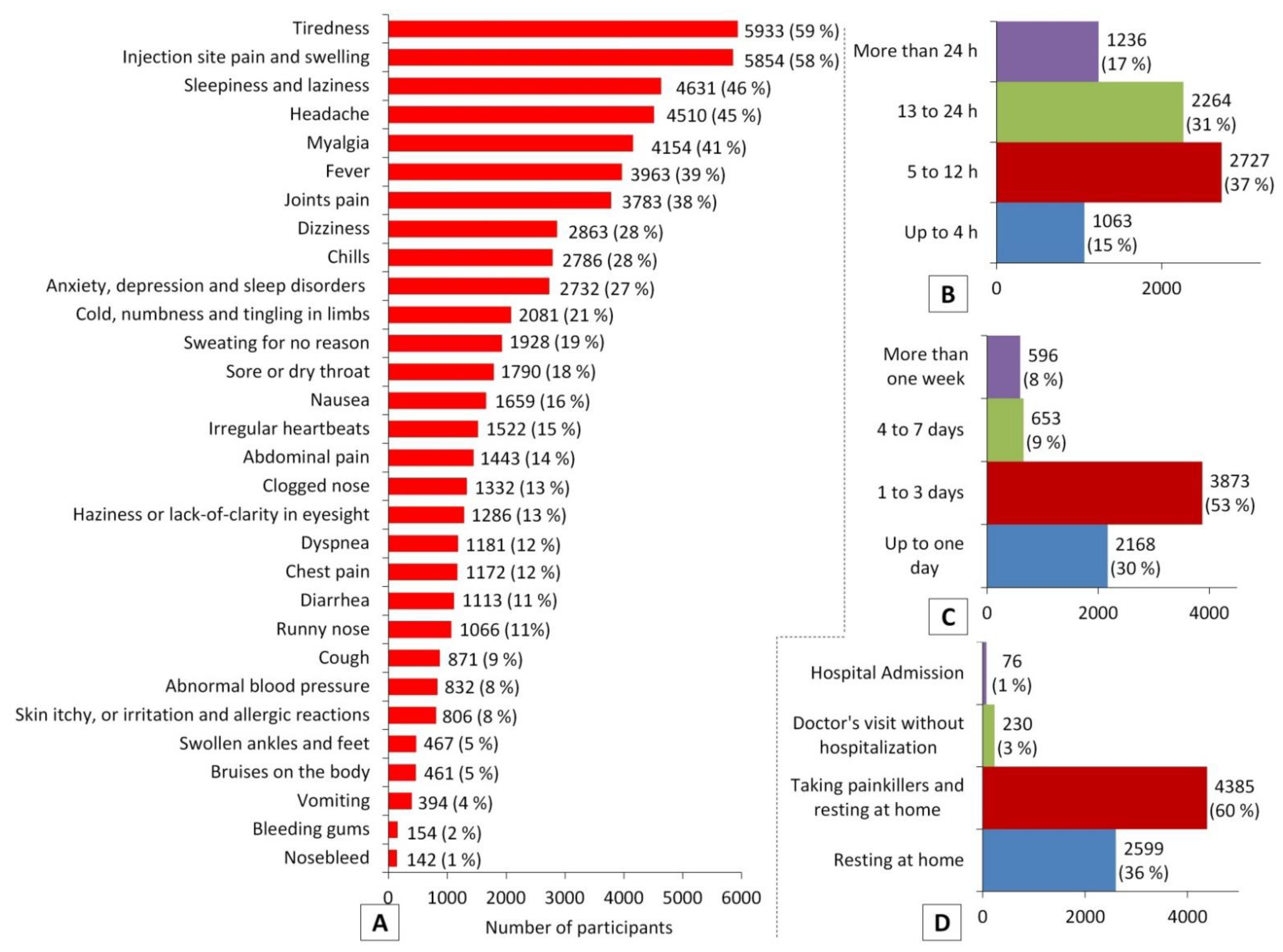
3.4. Post-Vaccination Information
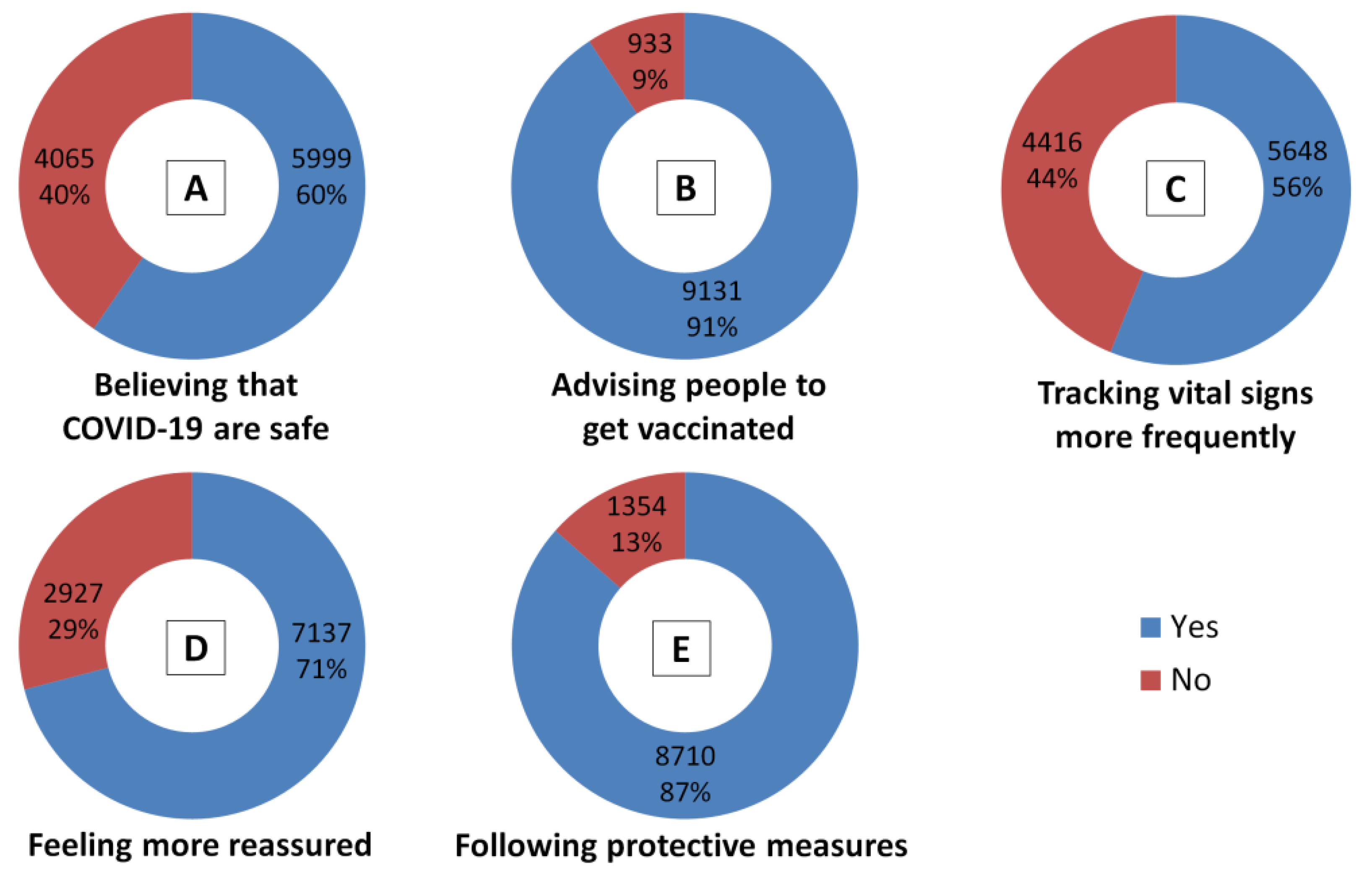
3.5. Participants’ Perceptions
3.6. Association of Predisposing Factors and Post-Vaccination Side Effects
3.7. Prediction of Post-Vaccination Side Effects Based on Predisposing Factors
4. Discussion
5. Study Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hatmal, M.M.; Alshaer, W.; Al-Hatamleh, M.A.I.; Hatmal, M.; Smadi, O.; Taha, M.O.; Oweida, A.J.; Boer, J.C.; Mohamud, R.; Plebanski, M. Comprehensive Structural and Molecular Comparison of Spike Proteins of SARS-CoV-2, SARS-CoV and MERS-CoV, and Their Interactions with ACE2. Cells 2020, 9, 2638. [Google Scholar] [CrossRef]
- Al-Hatamleh, M.A.I.; Hatmal, M.M.; Sattar, K.; Ahmad, S.; Mustafa, M.Z.; Bittencourt, M.D.C.; Mohamud, R. Antiviral and Immunomodulatory Effects of Phytochemicals from Honey against COVID-19: Potential Mechanisms of Action and Future Directions. Molecules 2020, 25, 5017. [Google Scholar] [CrossRef]
- Al-Hatamleh, M.A.I.; Hatmal, M.M.; Alshaer, W.; Rahman, E.N.S.E.A.; Mohd-Zahid, M.H.; Alhaj-Qasem, D.M.; Yean, C.Y.; Alias, I.Z.; Jaafar, J.; Ferji, K.; et al. COVID-19 infection and nanomedicine applications for development of vaccines and therapeutics: An overview and future perspectives based on polymersomes. Eur. J. Pharm. 2021, 896, 173930. [Google Scholar] [CrossRef]
- Rzymski, P.; Borkowski, L.; Drag, M.; Flisiak, R.; Jemielity, J.; Krajewski, J.; Mastalerz-Migas, A.; Matyja, A.; Pyrc, K.; Simon, K.; et al. The Strategies to Support the COVID-19 Vaccination with Evidence-Based Communication and Tackling Misinformation. Vaccines 2021, 9, 109. [Google Scholar] [CrossRef]
- Vignuzzi, M.; Wendt, E.; Andino, R. Engineering attenuated virus vaccines by controlling replication fidelity. Nat. Med. 2008, 14, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Kamal, A.M.; Kabir, A.; Southern, D.L.; Khan, S.H.; Hasan, S.M.M.; Sarkar, T.; Sharmin, S.; Das, S.; Roy, T.; et al. COVID-19 vaccine rumors and conspiracy theories: The need for cognitive inoculation against misinformation to improve vaccine adherence. PLoS ONE 2021, 16, e0251605. [Google Scholar] [CrossRef]
- Joshi, A.; Kaur, M.; Kaur, R.; Grover, A.; Nash, D.; El-Mohandes, A. Predictors of COVID-19 Vaccine Acceptance, Intention, and Hesitancy: A Scoping Review. Front. Public Health 2021, 9, 698111. [Google Scholar] [CrossRef]
- Lai, C.C.; Chen, I.T.; Chao, C.M.; Lee, P.I.; Ko, W.C.; Hsueh, P.R. COVID-19 vaccines: Concerns beyond protective efficacy and safety. Expert Rev. Vaccines 2021, 20, 1013–1025. [Google Scholar] [CrossRef]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Anand, P.; Stahel, V.P. Review the safety of COVID-19 mRNA vaccines: A review. Patient Saf. Surg. 2021, 15, 20. [Google Scholar] [CrossRef]
- Babamahmoodi, F.; Saeedi, M.; Alizadeh-Navaei, R.; Hedayatizadeh-Omran, A.; Mousavi, S.A.; Ovaise, G.; Kordi, S.; Akbari, Z.; Azordeh, M.; Ahangarkani, F.; et al. Side effects and Immunogenicity following administration of the Sputnik V COVID-19 vaccine in health care workers in Iran. Sci. Rep. 2021, 11, 21464. [Google Scholar] [CrossRef]
- Saeed, B.Q.; Al-Shahrabi, R.; Alhaj, S.S.; Alkokhardi, Z.M.; Adrees, A.O. Side effects and perceptions following Sinopharm COVID-19 vaccination. Int. J. Infect. Dis. 2021, 111, 219–226. [Google Scholar] [CrossRef]
- Hatmal, M.M.; Al-Hatamleh, M.A.I.; Olaimat, A.N.; Hatmal, M.; Alhaj-Qasem, D.M.; Olaimat, T.M.; Mohamud, R. Side Effects and Perceptions Following COVID-19 Vaccination in Jordan: A Randomized, Cross-Sectional Study Implementing Machine Learning for Predicting Severity of Side Effects. Vaccines 2021, 9, 556. [Google Scholar] [CrossRef]
- McElfish, P.A.; Willis, D.E.; Shah, S.K.; Bryant-Moore, K.; Rojo, M.O.; Selig, J.P. Sociodemographic Determinants of COVID-19 Vaccine Hesitancy, Fear of Infection, and Protection Self-Efficacy. J. Prim. Care Commun. Health 2021, 12, 21501327211040746. [Google Scholar] [CrossRef]
- Arab World Data. Available online: https://data.worldbank.org/country/1A (accessed on 31 August 2021).
- Statistics and Research: Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations?country=OWID_WRL (accessed on 19 January 2022).
- Kaadan, M.I.; Abdulkarim, J.; Chaar, M.; Zayegh, O.; Keblawi, M.A. Determinants of COVID-19 vaccine acceptance in the Arab world: A cross-sectional study. Glob. Health Res. Policy 2021, 6, 23. [Google Scholar] [CrossRef]
- Qunaibi, E.A.; Helmy, M.; Basheti, I.; Sultan, I. A high rate of COVID-19 vaccine hesitancy in a large-scale survey on Arabs. eLife 2021, 10, e68038. [Google Scholar] [CrossRef]
- Qunaibi, E.; Basheti, I.; Soudy, M.; Sultan, I. Hesitancy of Arab Healthcare Workers towards COVID-19 Vaccination: A Large-Scale Multinational Study. Vaccines 2021, 9, 446. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Hadi Al Kazzaz, H. COVID19 vaccination choice among Iraqi students at Al-Zahraa University for women [version 1; peer review: Awaiting peer review]. F1000Research 2021, 10, 1015. [Google Scholar] [CrossRef]
- Magadmi, R.M.; Kamel, F.O. Beliefs and barriers associated with COVID-19 vaccination among the general population in Saudi Arabia. BMC Public Health 2021, 21, 1438. [Google Scholar] [CrossRef]
- Mohamad, O.; Zamlout, A.; AlKhoury, N.; Mazloum, A.A.; Alsalkini, M.; Shaaban, R. Factors associated with the intention of Syrian adult population to accept COVID19 vaccination: A cross-sectional study. BMC Public Health 2021, 21, 1310. [Google Scholar] [CrossRef]
- Al-Qerem, W.A.; Jarab, A.S. COVID-19 Vaccination Acceptance and Its Associated Factors Among a Middle Eastern Population. Front. Public Health 2021, 9, 632914. [Google Scholar] [CrossRef]
- Albahri, A.H.; Alnaqbi, S.A.; Alshaali, A.O.; Alnaqbi, S.A.; Shahdoor, S.M. COVID-19 Vaccine Acceptance in a Sample From the United Arab Emirates General Adult Population: A Cross-Sectional Survey, 2020. Front. Public Health 2021, 9, 614499. [Google Scholar] [CrossRef]
- Alibrahim, J.; Awad, A. COVID-19 Vaccine Hesitancy among the Public in Kuwait: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2021, 18, 8836. [Google Scholar] [CrossRef]
- Bitar, A.N.; Zawiah, M.; Al-Ashwal, F.Y.; Kubas, M.; Saeed, R.M.; Abduljabbar, R.; Jaber, A.A.S.; Sulaiman, S.A.S.; Khan, A.H. Misinformation, perceptions towards COVID-19 and willingness to be vaccinated: A population-based survey in Yemen. PLoS ONE 2021, 16, e0248325. [Google Scholar] [CrossRef]
- Nasr, L.; Saleh, N.; Hleyhel, M.; El-Outa, A.; Noujeim, Z. Acceptance of COVID-19 vaccination and its determinants among Lebanese dentists: A cross-sectional study. BMC Oral Health 2021, 21, 484. [Google Scholar] [CrossRef]
- Shehata, W.M.; Elshora, A.A.; Abu-Elenin, M.M. Physicians’ attitudes and acceptance regarding COVID-19 vaccines: A cross-sectional study in mid Delta region of Egypt. Env. Sci. Pollut Res. Int. 2021, 29, 15838–15848. [Google Scholar] [CrossRef]
- Kacimi, S.E.O.; Klouche-Djedid, S.N.; Riffi, O.; Belaouni, H.A.; Yasmin, F.; Taouza, F.A.; Belakhdar, Y.; Fellah, S.C.; Benmelouka, A.Y.; Ahmed, S.; et al. Determinants of SARS-CoV-2 Vaccine Engagement in Algeria: A Population-based Study with Systematic Review of Studies from Arab Countries of the MENA Region. medRxiv 2021. [Google Scholar] [CrossRef]
- Khalis, M.; Hatim, A.; Elmouden, L.; Diakite, M.; Marfak, A.; Ait El Haj, S.; Farah, R.; Jidar, M.; Conde, K.K.; Hassouni, K.; et al. Acceptability of COVID-19 vaccination among health care workers: A cross-sectional survey in Morocco. Hum. Vaccin Immunother. 2021, 17, 5076–5081. [Google Scholar] [CrossRef]
- Kefi, H.E.; Kefi, K.; Krir, M.W.; Brahim, C.B.; Baatout, A.; Bouzouita, I.; Azaiz, M.B.; Bouguerra, C.; Khoufi, M.T.; Gharsallah, H.; et al. Acceptability of COVID-19 vaccine: A cross-sectional study in a Tunisian general hospital. Pan. Afr. Med. J. 2021, 39, 245. [Google Scholar] [CrossRef]
- Fares, S.; Elmnyer, M.M.; Mohamed, S.S.; Elsayed, R. COVID-19 Vaccination Perception and Attitude among Healthcare Workers in Egypt. J. Prim. Care Commun. Health 2021, 12, 21501327211013303. [Google Scholar] [CrossRef]
- Elhadi, M.; Alsoufi, A.; Alhadi, A.; Hmeida, A.; Alshareea, E.; Dokali, M.; Abodabos, S.; Alsadiq, O.; Abdelkabir, M.; Ashini, A.; et al. Knowledge, attitude, and acceptance of healthcare workers and the public regarding the COVID-19 vaccine: A cross-sectional study. BMC Public Health 2021, 21, 955. [Google Scholar] [CrossRef]
- Hamady, A.; Lee, J.; Loboda, Z.A. Waning antibody responses in COVID-19: What can we learn from the analysis of other coronaviruses? Infection 2021, 50, 11–25. [Google Scholar] [CrossRef]
- Zawahrah, H.J.; Saca-Hazboun, H.; Melhem, S.S.; Adwan, R.; Sabateen, A.; Abu-Rmeileh, N.M.E. Acceptance of COVID-19 vaccines in Palestine: A cross-sectional online study. BMJ Open 2021, 11, e053681. [Google Scholar] [CrossRef]
- Hatmal, M.M.; Abderrahman, S.M.; Nimer, W.; Al-Eisawi, Z.; Al-Ameer, H.J.; Al-Hatamleh, M.A.I.; Mohamud, R.; Alshaer, W. Artificial Neural Networks Model for Predicting Type 2 Diabetes Mellitus Based on VDR Gene FokI Polymorphism, Lipid Profile and Demographic Data. Biology 2020, 9, 222. [Google Scholar] [CrossRef]
- Debnath, S.; Barnaby, D.P.; Coppa, K.; Makhnevich, A.; Kim, E.J.; Chatterjee, S.; Toth, V.; Levy, T.J.; Paradis, M.D.; Cohen, S.L.; et al. Machine learning to assist clinical decision-making during the COVID-19 pandemic. Bioelectron. Med. 2020, 6, 14. [Google Scholar] [CrossRef]
- Kumar, V.; Chawla, J.; Kumar, R.; Saxena, A. Modelling COVID-19: Transmission dynamics using machine learning techniques. In Intelligent Healthcare; Bhatia, S., Dubey, A.K., Chhikara, R., Chaudhary, P., Kumar, A., Eds.; Springer: Cham, Switzerland, 2021; pp. 99–108. [Google Scholar]
- Hatmal, M.M.; Abuyman, O.; Taha, M. Docking-Generated Multiple Ligand Poses for Bootstrapping Bioactivity Classifying Machine Learning: Repurposing Covalent Inhibitors for COVID-19-Related TMPRSS2 as Case Study. Comput. Struct. Biotechnol. J. 2021, 19, 4790–4824. [Google Scholar] [CrossRef]
- McCoy, D.; Mgbara, W.; Horvitz, N.; Getz, W.M.; Hubbard, A. Ensemble machine learning of factors influencing COVID-19 across US counties. Sci. Rep. 2021, 11, 11777. [Google Scholar] [CrossRef]
- Prieto, K. Current forecast of COVID-19 in Mexico: A Bayesian and machine learning approaches. PLoS ONE 2022, 17, e0259958. [Google Scholar] [CrossRef]
- Huyut, M.T.; Ustundag, H. Prediction of diagnosis and prognosis of COVID-19 disease by blood gas parameters using decision trees machine learning model: A retrospective observational study. Med. Gas. Res. 2022, 12, 60–66. [Google Scholar] [CrossRef]
- Aghdam, R.; Habibi, M.; Taheri, G. Using informative features in machine learning based method for COVID-19 drug repurposing. J. Cheminform. 2021, 13, 70. [Google Scholar] [CrossRef] [PubMed]
- Ong, E.; Wong, M.U.; Huffman, A.; He, Y. COVID-19 Coronavirus Vaccine Design Using Reverse Vaccinology and Machine Learning. Front. Immunol. 2020, 11, 1581. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Huang, Y.; Abdulqader, H.; Morgado, M.; Domnori, S.; Koščík, M.; Mendes, J.J.; Klugar, M.; Kateeb, E.; IADS-SCORE. Universal Predictors of Dental Students’ Attitudes towards COVID-19 Vaccination: Machine Learning-Based Approach. Vaccines 2021, 9, 1158. [Google Scholar] [CrossRef] [PubMed]
- Ahamad, M.; Aktar, S.; Uddin, J.; Rashed Al, M.; Azad, A.K.M.; Uddin, S.; Alyami, S.A.; Sarker, I.H.; Liò, P.; Quinn, J.M.W.; et al. Adverse effects of COVID-19 vaccination: Machine learning and statistical approach to identify and classify incidences of morbidity and post-vaccination reactogenicity. medRxiv 2021. [Google Scholar] [CrossRef]
- Raosoft Online Sample Size Calculator. Available online: http://www.raosoft.com/samplesize.html (accessed on 31 August 2021).
- Kappel, B.A.; De Angelis, L.; Heiser, M.; Ballanti, M.; Stoehr, R.; Goettsch, C.; Mavilio, M.; Artati, A.; Paoluzi, O.A.; Adamski, J.; et al. Cross-omics analysis revealed gut microbiome-related metabolic pathways underlying atherosclerosis development after antibiotics treatment. Mol. Metab 2020, 36, 100976. [Google Scholar] [CrossRef]
- Nunez Lopez, Y.O.; Retnakaran, R.; Zinman, B.; Pratley, R.E.; Seyhan, A.A. Predicting and understanding the response to short-term intensive insulin therapy in people with early type 2 diabetes. Mol. Metab. 2019, 20, 63–78. [Google Scholar] [CrossRef]
- Tao, C.; Pan, H.; Li, Y.; Zou, Z. Unsupervised Spectral–Spatial Feature Learning With Stacked Sparse Autoencoder for Hyperspectral Imagery Classification. IEEE Geosci. Remote Sens. Lett. 2015, 12, 2438–2442. [Google Scholar] [CrossRef]
- Ren, X.; Guo, H.; Li, S.; Wang, S.; Li, J. A Novel Image Classification Method with CNN-XGBoost Model. In Digital Forensics and Watermarking; Kraetzer, C., Shi, Y.Q., Dittmann, J., Kim, H., Eds.; Springer: Cham, Switzerland, 2017; Volume 10431, pp. 378–390. [Google Scholar]
- Rozinajová, V.; Ezzeddine, A.B.; Lóderer, M.; Loebl, J.; Magyar, R.; Vrablecová, P. Computational intelligence in smart grid environment. In Computational Intelligence for Multimedia Big Data on the Cloud with Engineering Applications; Sangaiah, A.K., Sheng, M., Zhang, Z., Eds.; Academic Press: Cambridge, MA, USA, 2018; pp. 23–59. [Google Scholar]
- Hartstra, A.V.; Schuppel, V.; Imangaliyev, S.; Schrantee, A.; Prodan, A.; Collard, D.; Levin, E.; Dallinga-Thie, G.; Ackermans, M.T.; Winkelmeijer, M.; et al. Infusion of donor feces affects the gut-brain axis in humans with metabolic syndrome. Mol. Metab. 2020, 42, 101076. [Google Scholar] [CrossRef]
- Sainlez, M.; Heyen, G. Recurrent neural network prediction of steam production in a Kraft recovery boiler. In Computer Aided Chemical Engineering; Pistikopoulos, E.N., Georgiadis, M.C., Kokossis, A.C., Eds.; Elsevier: Amsterdam, The Netherlands, 2011; Volume 29, pp. 1784–1788. [Google Scholar]
- Tsamardinos, I.; Greasidou, E.; Borboudakis, G. Bootstrapping the out-of-sample predictions for efficient and accurate cross-validation. Mach. Learn. 2018, 107, 1895–1922. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, J.D.; Matias-Guiu, J.A.; Cabrera-Martin, M.N.; Risco-Martin, J.L.; Ayala, J.L. An application of machine learning with feature selection to improve diagnosis and classification of neurodegenerative disorders. BMC Bioinform. 2019, 20, 491. [Google Scholar] [CrossRef] [Green Version]
- Larabi-Marie-Sainte, S.; Aburahmah, L.; Almohaini, R.; Saba, T. Current Techniques for Diabetes Prediction: Review and Case Study. Appl. Sci. 2019, 9, 4604. [Google Scholar] [CrossRef] [Green Version]
- Hatmal, M.M.; Alshaer, W.; Mahmoud, I.S.; Al-Hatamleh, M.A.I.; Al-Ameer, H.J.; Abuyaman, O.; Zihlif, M.; Mohamud, R.; Darras, M.; Al Shhab, M.; et al. Investigating the association of CD36 gene polymorphisms (rs1761667 and rs1527483) with T2DM and dyslipidemia: Statistical analysis, machine learning based prediction, and meta-analysis. PLoS ONE 2021, 16, e0257857. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Le, T.T.; Fu, W.; Moore, J.H. Scaling tree-based automated machine learning to biomedical big data with a feature set selector. Bioinformatics 2019, 36, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Liu, G.; Lu, D.; Lu, J. Pharm-AutoML: An open-source, end-to-end automated machine learning package for clinical outcome prediction. CPT Pharmacomet. Syst Pharm. 2021, 10, 478–488. [Google Scholar] [CrossRef]
- Mohebali, B.; Tahmassebi, A.; Meyer-Baese, A.; Gandomi, A.H. Probabilistic neural networks: A brief overview of theory, implementation, and application. In Handbook of Probabilistic Models; Samui, P., Tien Bui, D., Chakraborty, S., Deo, R.C., Eds.; Butterworth-Heinemann: Oxford, UK, 2020; pp. 347–367. [Google Scholar]
- Zeinali, Y.; Story, B.A. Competitive probabilistic neural network. Integr. Comput.—Aided Eng. 2017, 24, 105–118. [Google Scholar] [CrossRef]
- Chang, C.-C.; Lin, C.-J. LIBSVM: A library for support vector machines. ACM Trans. Intell. Syst. Technol. 2011, 2, 27. [Google Scholar] [CrossRef]
- Rajendra Acharya, U.; Faust, O.; Adib Kadri, N.; Suri, J.S.; Yu, W. Automated identification of normal and diabetes heart rate signals using nonlinear measures. Comput. Biol. Med. 2013, 43, 1523–1529. [Google Scholar] [CrossRef]
- Hajmeer, M.; Basheer, I. A probabilistic neural network approach for modeling and classification of bacterial growth/no-growth data. J. Microbiol. Methods 2002, 51, 217–226. [Google Scholar] [CrossRef]
- Khosravanian, A.; Ayat, S. Diagnosing Breast Cancer Type by Using Probabilistic Neural Network in Decision Support System. Int. J. Knowl. Eng. 2016, 2, 73–76. [Google Scholar] [CrossRef] [Green Version]
- Anand, P.K.; Shin, D.R.; Memon, M.L. Adaptive Boosting Based Personalized Glucose Monitoring System (PGMS) for Non-Invasive Blood Glucose Prediction with Improved Accuracy. Diagnostics 2020, 10, 285. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Pan, C. Diabetes classification model based on boosting algorithms. BMC Bioinform. 2018, 19, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piryonesi, S.M.; El-Diraby, T.E. Data Analytics in Asset Management: Cost-Effective Prediction of the Pavement Condition Index. J. Infrastruct. Syst. 2020, 26, 04019036. [Google Scholar] [CrossRef]
- Hastie, T.; Tibshirani, R.; Friedman, J. Boosting and Additive Trees. In The Elements of Statistical Learning; Springer Series in Statistics; Springer: New York, NY, USA, 2009. [Google Scholar]
- Piryonesi, S.M.; El-Diraby, T.E. Using Machine Learning to Examine Impact of Type of Performance Indicator on Flexible Pavement Deterioration Modeling. J. Infrastruct. Syst. 2021, 27, 04021005. [Google Scholar] [CrossRef]
- Hall, P.; Park, B.U.; Samworth, R.J. Choice of Neighbor Order in Nearest-Neighbor Classification. Ann. Stat. 2008, 36, 2135–2152. [Google Scholar] [CrossRef]
- KNN and Potential Energy: Applet. Available online: http://www.math.le.ac.uk/people/ag153/homepage/KNN/KNN3.html (accessed on 10 December 2021).
- Osman, A.H.; Aljahdali, H.M.; Altarrazi, S.M.; Ahmed, A. SOM-LWL method for identification of COVID-19 on chest X-rays. PLoS ONE 2021, 16, e0247176. [Google Scholar] [CrossRef] [PubMed]
- Almufty, H.B.; Mohammed, S.A.; Abdullah, A.M.; Merza, M.A. Potential adverse effects of COVID19 vaccines among Iraqi population; a comparison between the three available vaccines in Iraq; a retrospective cross-sectional study. Diabetes Metab. Syndr. 2021, 15, 102207. [Google Scholar] [CrossRef]
- Omeish, H.; Najadat, A.; Al-Azzam, S.; Tarabin, N.; Abu Hameed, A.; Al-Gallab, N.; Abbas, H.; Rababah, L.; Rabadi, M.; Karasneh, R.; et al. Reported COVID-19 vaccines side effects among Jordanian population: A cross sectional study. Hum. Vaccin Immunother. 2021, 1–8. [Google Scholar] [CrossRef]
- Abu-Halaweh, S.; Alqassieh, R.; Suleiman, A.; Al-Sabbagh, M.Q.; AbuHalaweh, M.; AlKhader, D.; Abu-Nejem, R.; Nabulsi, R.A.; Al-Tamimi, M.; Alwreikat, M.; et al. Qualitative Assessment of Early Adverse Effects of Pfizer–BioNTech and Sinopharm COVID-19 Vaccines by Telephone Interviews. Vaccines 2021, 9, 950. [Google Scholar] [CrossRef]
- Abu-Hammad, O.; Alduraidi, H.; Abu-Hammad, S.; Alnazzawi, A.; Babkair, H.; Abu-Hammad, A.; Nourwali, I.; Qasem, F.; Dar-Odeh, N. Side Effects Reported by Jordanian Healthcare Workers Who Received COVID-19 Vaccines. Vaccines 2021, 9, 577. [Google Scholar] [CrossRef]
- Massoud, F.; Ahmad, S.F.; Hassan, A.M.; Alexander, K.J.; Al-Hashel, J.; Arabi, M. Safety and tolerability of the novel 2019 coronavirus disease (COVID-19) vaccines among people with epilepsy (PwE): A cross-sectional study. Seizure 2021, 92, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Al Ghafri, T.S.; Al Balushi, L.; Al Balushi, Z.; Al Hinai, F.; Al Hasani, S.; Anwar, H.; Al Lawati, M.; Al Harthi, S. Reporting at Least One Adverse Effect Post-COVID-19 Vaccination From Primary Health Care in Muscat. Cureus 2021, 13, e17055. [Google Scholar] [CrossRef]
- Alharbi, N.K.; Al-Tawfiq, J.A.; Alghnam, S.; Alwehaibe, A.; Alasmari, A.; Alsagaby, S.A.; Alotaibi, F.; Alsubaie, F.; Alshomrani, M.; Farahat, F.M.; et al. Effectiveness of COVID-19 Vaccines: Eight Months Post Single Dose Vaccination. medRxiv 2021. [Google Scholar] [CrossRef]
- Alghamdi, A.N.; Alotaibi, M.I.; Alqahtani, A.S.; Al Aboud, D.; Abdel-Moneim, A.S. BNT162b2 and ChAdOx1 SARS-CoV-2 Post-vaccination Side-Effects Among Saudi Vaccinees. Front. Med. 2021, 8, 760047. [Google Scholar] [CrossRef]
- Al Bahrani, S.; Albarrak, A.; Alghamdi, O.A.; Alghamdi, M.A.; Hakami, F.H.; Al Abaadi, A.K.; Alkhrashi, S.A.; Alghamdi, M.Y.; Almershad, M.M.; Alenazi, M.M.; et al. Safety and Reactogenicity of the ChAdOx1 (AZD1222) COVID-19 Vaccine in Saudi Arabia. Int. J. Infect. Dis 2021, 110, 359–362. [Google Scholar] [CrossRef]
- Alhazmi, A.; Alamer, E.; Daws, D.; Hakami, M.; Darraj, M.; Abdelwahab, S.; Maghfuri, A.; Algaissi, A. Evaluation of Side Effects Associated with COVID-19 Vaccines in Saudi Arabia. Vaccines 2021, 9, 674. [Google Scholar] [CrossRef] [PubMed]
- El-Shitany, N.A.; Harakeh, S.; Badr-Eldin, S.M.; Bagher, A.M.; Eid, B.; Almukadi, H.; Alghamdi, B.S.; Alahmadi, A.A.; Hassan, N.A.; Sindi, N.; et al. Minor to Moderate Side Effects of Pfizer-BioNTech COVID-19 Vaccine Among Saudi Residents: A Retrospective Cross-Sectional Study. Int. J. Gen. Med. 2021, 14, 1389–1401. [Google Scholar] [CrossRef] [PubMed]
- Adam, M.; Gameraddin, M.; Alelyani, M.; Alshahrani, M.Y.; Gareeballah, A.; Ahmad, I.; Azzawi, A.; Komit, B.; Musa, A. Evaluation of Post-Vaccination Symptoms of Two Common COVID-19 Vaccines Used in Abha, Aseer Region, Kingdom of Saudi Arabia. Patient Prefer. Adherence 2021, 15, 1963–1970. [Google Scholar] [CrossRef]
- Fink, A.L.; Klein, S.L. Sex and Gender Impact Immune Responses to Vaccines Among the Elderly. Physiology 2015, 30, 408–416. [Google Scholar] [CrossRef]
- Iguacel, I.; Maldonado, A.L.; Ruiz-Cabello, A.L.; Casaus, M.; Moreno, L.A.; Martinez-Jarreta, B. Association between COVID-19 Vaccine Side Effects and Body Mass Index in Spain. Vaccines 2021, 9, 1321. [Google Scholar] [CrossRef]
- Elnaem, M.H.; Mohd Taufek, N.H.; Ab Rahman, N.S.; Mohd Nazar, N.I.; Zin, C.S.; Nuffer, W.; Turner, C.J. COVID-19 Vaccination Attitudes, Perceptions, and Side Effect Experiences in Malaysia: Do Age, Gender, and Vaccine Type Matter? Vaccines 2021, 9, 1156. [Google Scholar] [CrossRef] [PubMed]
- Jahan, N.; Rahman, F.I.; Saha, P.; Ether, S.A.; Roknuzzaman, A.; Sarker, R.; Kalam, K.T.; Haq, K.; Nyeen, J.; Himi, H.Z.; et al. Side Effects Following Administration of the First Dose of Oxford-AstraZeneca’s Covishield Vaccine in Bangladesh: A Cross-Sectional Study. Infect. Dis. Rep. 2021, 13, 888–901. [Google Scholar] [CrossRef]
- Zhu, J.S.; Zhang, M.X.; Chien, C.W.; Yang, W.Y.; Shi, G.F.; Qiu, S.; Tung, T.H.; Chen, H.X. Sex Differences in Adverse Reactions to an Inactivated SARS-CoV-2 Vaccine Among Medical Staff in China. Front. Med. 2021, 8, 731593. [Google Scholar] [CrossRef] [PubMed]
- Ciarambino, T.; Barbagelata, E.; Corbi, G.; Ambrosino, I.; Politi, C.; Lavalle, F.; Ruggieri, A.; Moretti, A. Gender differences in vaccine therapy: Where are we in COVID-19 pandemic? Monaldi Arch. Chest. Dis. 2021, 91. [Google Scholar] [CrossRef] [PubMed]
- Hajure, M.; Tariku, M.; Bekele, F.; Abdu, Z.; Dule, A.; Mohammedhussein, M.; Tsegaye, T. Attitude Towards COVID-19 Vaccination Among Healthcare Workers: A Systematic Review. Infect. Drug Resist. 2021, 14, 3883–3897. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Du, J.; Duan, R.; Zhang, X.; Tao, C.; Chen, Y. Characterization of the Differential Adverse Event Rates by Race/Ethnicity Groups for HPV Vaccine by Integrating Data From Different Sources. Front. Pharm. 2018, 9, 539. [Google Scholar] [CrossRef]
- Kenzaka, T.; Yahata, S.; Goda, K.; Kumabe, A.; Kamada, M.; Okayama, M. Effects of Vaccination Day Routine Activities on Influenza Vaccine Efficacy and Vaccination-Induced Adverse Reaction Incidence: A Cohort Study. Vaccines 2021, 9, 753. [Google Scholar] [CrossRef]
- Andrzejczak-Grządko, S.; Czudy, Z.; Donderska, M. Side effects after COVID-19 vaccinations among residents of Poland. Eur. Rev. Med. Pharm. Sci. 2021, 25, 4418–4421. [Google Scholar] [CrossRef]
- Possible Side Effects after Getting a COVID-19 Vaccine. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/expect/after.html (accessed on 25 April 2021).
- Winter, A.P.; Follett, E.A.; McIntyre, J.; Stewart, J.; Symington, I.S. Influence of smoking on immunological responses to hepatitis B vaccine. Vaccine 1994, 12, 771–772. [Google Scholar] [CrossRef]
- Cruijff, M.; Thijs, C.; Govaert, T.; Aretz, K.; Dinant, G.J.; Knottnerus, A. The effect of smoking on influenza, influenza vaccination efficacy and on the antibody response to influenza vaccination. Vaccine 1999, 17, 426–432. [Google Scholar] [CrossRef]
- Shavit, R.; Maoz-Segal, R.; Iancovici-Kidon, M.; Offengenden, I.; Haj Yahia, S.; Machnes Maayan, D.; Lifshitz-Tunitsky, Y.; Niznik, S.; Frizinsky, S.; Deutch, M.; et al. Prevalence of Allergic Reactions After Pfizer-BioNTech COVID-19 Vaccination Among Adults with High Allergy Risk. JAMA Netw. Open 2021, 4, e2122255. [Google Scholar] [CrossRef] [PubMed]
- Alhumaid, S.; Al Mutair, A.; Al Alawi, Z.; Rabaan, A.A.; Tirupathi, R.; Alomari, M.A.; Alshakhes, A.S.; Alshawi, A.M.; Ahmed, G.Y.; Almusabeh, H.M.; et al. Anaphylactic and nonanaphylactic reactions to SARS-CoV-2 vaccines: A systematic review and meta-analysis. Allergy Asthma Clin. Immunol. 2021, 17, 109. [Google Scholar] [CrossRef] [PubMed]
- Ossato, A.; Tessari, R.; Trabucchi, C.; Zuppini, T.; Realdon, N.; Marchesini, F. Comparison of medium-term adverse reactions induced by the first and second dose of mRNA BNT162b2 (Comirnaty, Pfizer-BioNTech) vaccine: A post-marketing Italian study conducted between 1 January and 28 February 2021. Eur. J. Hosp. Pharm. 2021, 28. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Lee, S.B.; Lee, S.W.; Lee, M.H.; Koyanagi, A.; Jacob, L.; Tizaoui, K.; Yon, D.K.; Shin, J.I.; Smith, L. Comparison of vaccine-induced thrombotic events between ChAdOx1 nCoV-19 and Ad26.COV.2.S vaccines. J. Autoimmun. 2021, 122, 102681. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Patone, M.; Mei, X.W.; Saatci, D.; Dixon, S.; Khunti, K.; Zaccardi, F.; Watkinson, P.; Shankar-Hari, M.; Doidge, J.; et al. Risk of thrombocytopenia and thromboembolism after COVID-19 vaccination and SARS-CoV-2 positive testing: Self-controlled case series study. BMJ 2021, 374, n1931. [Google Scholar] [CrossRef]
- Lee, E.J.; Cines, D.B.; Gernsheimer, T.; Kessler, C.; Michel, M.; Tarantino, M.D.; Semple, J.W.; Arnold, D.M.; Godeau, B.; Lambert, M.P.; et al. Thrombocytopenia following Pfizer and Moderna SARS-CoV-2 vaccination. Am. J. Hematol. 2021, 96, 534–537. [Google Scholar] [CrossRef]
- Crous-Bou, M.; Harrington, L.B.; Kabrhel, C. Environmental and Genetic Risk Factors Associated with Venous Thromboembolism. Semin Thromb. Hemost. 2016, 42, 808–820. [Google Scholar] [CrossRef] [Green Version]
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 31 August 2021).
- Esba, L.C.A.; Al Jeraisy, M. Reported adverse effects following COVID-19 vaccination at a tertiary care hospital, focus on cerebral venous sinus thrombosis (CVST). Expert Rev. Vaccines 2021, 20, 1037–1042. [Google Scholar] [CrossRef]
- Schultz, N.H.; Sorvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.H.; Skattor, T.H.; Tjonnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2124–2130. [Google Scholar] [CrossRef]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef]
- Carli, G.; Nichele, I.; Ruggeri, M.; Barra, S.; Tosetto, A. Deep vein thrombosis (DVT) occurring shortly after the second dose of mRNA SARS-CoV-2 vaccine. Intern. Emer. Med. 2021, 16, 803–804. [Google Scholar] [CrossRef]
- Xu, S.; Huang, R.; Sy, L.S.; Glenn, S.C.; Ryan, D.S.; Morrissette, K.; Shay, D.K.; Vazquez-Benitez, G.; Glanz, J.M.; Klein, N.P.; et al. COVID-19 Vaccination and Non-COVID-19 Mortality Risk—Seven Integrated Health Care Organizations, United States, 14 December 2020–31 July 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1520–1524. [Google Scholar] [CrossRef]
- Bhattacharjee, S.; Banerjee, M. Immune Thrombocytopenia Secondary to COVID-19: A Systematic Review. SN Compr. Clin. Med. 2020, 2, 2048–2058. [Google Scholar] [CrossRef] [PubMed]
- Wool, G.D.; Miller, J.L. The Impact of COVID-19 Disease on Platelets and Coagulation. Pathobiology 2021, 88, 15–27. [Google Scholar] [CrossRef]
- Chen, F.; Zhu, S.; Dai, Z.; Hao, L.; Luan, C.; Guo, Q.; Meng, C.; Zhang, Y. Effects of COVID-19 and mRNA vaccines on human fertility. Hum. Reprod. 2021, 37, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Salamonsen, L.A.; Zhang, J.; Brasted, M. Leukocyte networks and human endometrial remodelling. J. Reprod. Immunol. 2002, 57, 95–108. [Google Scholar] [CrossRef]
- Fajrin, I.; Alam, G.; Usman, A.N. Prostaglandin level of primary dysmenorrhea pain sufferers. Enferm. Clín. 2020, 30, 5–9. [Google Scholar] [CrossRef]
- MacDonald, N.E.; The SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Riad, A.; Abdulqader, H.; Morgado, M.; Domnori, S.; Koscik, M.; Mendes, J.J.; Klugar, M.; Kateeb, E.; Iads-Score, O.B.O. Global Prevalence and Drivers of Dental Students’ COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 566. [Google Scholar] [CrossRef]
- Kateeb, E.; Danadneh, M.; Pokorna, A.; Klugarova, J.; Abdulqader, H.; Klugar, M.; Riad, A. Predictors of Willingness to Receive COVID-19 Vaccine: Cross-Sectional Study of Palestinian Dental Students. Vaccines 2021, 9, 954. [Google Scholar] [CrossRef] [PubMed]
- Trent, M.; Seale, H.; Chughtai, A.A.; Salmon, D.; MacIntyre, C.R. Trust in government, intention to vaccinate and COVID-19 vaccine hesitancy: A comparative survey of five large cities in the United States, United Kingdom, and Australia. Vaccine 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Vaccine Breakthrough Infections Reported to CDC—United States. 1 January–30 April 2021. Available online: https://www.cdc.gov/mmwr/volumes/70/wr/mm7021e3.htm (accessed on 31 August 2021).
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Kustin, T.; Harel, N.; Finkel, U.; Perchik, S.; Harari, S.; Tahor, M.; Caspi, I.; Levy, R.; Leshchinsky, M.; Ken Dror, S.; et al. Evidence for increased breakthrough rates of SARS-CoV-2 variants of concern in BNT162b2-mRNA-vaccinated individuals. Nat. Med. 2021, 27, 1379–1384. [Google Scholar] [CrossRef] [PubMed]
- Hacisuleyman, E.; Hale, C.; Saito, Y.; Blachere, N.E.; Bergh, M.; Conlon, E.G.; Schaefer-Babajew, D.J.; DaSilva, J.; Muecksch, F.; Gaebler, C.; et al. Vaccine Breakthrough Infections with SARS-CoV-2 Variants. N. Engl. J. Med. 2021, 384, 2212–2218. [Google Scholar] [CrossRef]
- Philomina, J.B.; Jolly, B.; John, N.; Bhoyar, R.C.; Majeed, N.; Senthivel, V.; Cp, F.; Rophina, M.; Vasudevan, B.; Imran, M.; et al. Genomic survey of SARS-CoV-2 vaccine breakthrough infections in healthcare workers from Kerala, India. J. Infect. 2021, 83, 237–279. [Google Scholar] [CrossRef] [PubMed]
- Bouton, T.C.; Lodi, S.; Turcinovic, J.; Weber, S.E.; Quinn, E.; Korn, C.; Steiner, J.; Schechter-Perkins, E.M.; Duffy, E.; Ragan, E.J.; et al. COVID-19 vaccine impact on rates of SARS-CoV-2 cases and post vaccination strain sequences among healthcare workers at an urban academic medical center: A prospective cohort study. medRxiv 2021, 8, ofab465. [Google Scholar] [CrossRef]
- Thompson, C.N.; Hughes, S.; Ngai, S.; Baumgartner, J.; Wang, J.C.; McGibbon, E.; Devinney, K.; Luoma, E.; Bertolino, D.; Hwang, C.; et al. Rapid Emergence and Epidemiologic Characteristics of the SARS-CoV-2 B.1.526 Variant—New York City, New York, 1 January–5 April 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 712–716. [Google Scholar] [CrossRef]
- Fleiss, J.L.; Levin, B.; Paik, M.C. Statistical Methods for Rates and Proportions, 3rd ed.; John Wiley & Sons, Inc.: New York, NY, USA, 2003. [Google Scholar]
- Satapathy, S.K.; Dehuri, S.; Jagadev, A.K.; Mishra, S. EEG Brain Signal. Classification for Epileptic Seizure Disorder Detection; Elsevier Inc.: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Natekin, A.; Knoll, A. Gradient boosting machines, a tutorial. Front. Neurorobot. 2013, 7, 21. [Google Scholar] [CrossRef] [Green Version]
- Sarker, I.H. Machine Learning: Algorithms, Real-World Applications and Research Directions. SN Comput. Sci. 2021, 2, 160. [Google Scholar] [CrossRef]
- Alyasseri, Z.A.A.; Al-Betar, M.A.; Doush, I.A.; Awadallah, M.A.; Abasi, A.K.; Makhadmeh, S.N.; Alomari, O.A.; Abdulkareem, K.H.; Adam, A.; Damasevicius, R.; et al. Review on COVID-19 diagnosis models based on machine learning and deep learning approaches. Expert Syst. 2021, 39, e12759. [Google Scholar] [CrossRef] [PubMed]
- Syeda, H.B.; Syed, M.; Sexton, K.W.; Syed, S.; Begum, S.; Syed, F.; Prior, F.; Yu, F., Jr. Role of Machine Learning Techniques to Tackle the COVID-19 Crisis: Systematic Review. JMIR Med. Inf. 2021, 9, e23811. [Google Scholar] [CrossRef] [PubMed]
- Shahid, O.; Nasajpour, M.; Pouriyeh, S.; Parizi, R.M.; Han, M.; Valero, M.; Li, F.; Aledhari, M.; Sheng, Q.Z. Machine learning research towards combating COVID-19: Virus detection, spread prevention, and medical assistance. J. Biomed. Inform. 2021, 117, 103751. [Google Scholar] [CrossRef]
- Gutierrez, J.M.; Volkovs, M.; Poutanen, T.; Watson, T.; Rosella, L.C. Risk stratification for COVID-19 hospitalization: A multivariable model based on gradient-boosting decision trees. CMAJ Open 2021, 9, E1223–E1231. [Google Scholar] [CrossRef] [PubMed]
- Kaliappan, J.; Srinivasan, K.; Mian Qaisar, S.; Sundararajan, K.; Chang, C.-Y. Performance Evaluation of Regression Models for the Prediction of the COVID-19 Reproduction Rate. Front. Public Health 2021, 9, 1319. [Google Scholar] [CrossRef]
- Shrivastav, L.K.; Jha, S.K. A gradient boosting machine learning approach in modeling the impact of temperature and humidity on the transmission rate of COVID-19 in India. Appl. Intell. 2021, 51, 2727–2739. [Google Scholar] [CrossRef]
- Aktar, S.; Ahamad, M.M.; Rashed-Al-Mahfuz, M.; Azad, A.; Uddin, S.; Kamal, A.; Alyami, S.A.; Lin, P.I.; Islam, S.M.S.; Quinn, J.M.; et al. Machine Learning Approach to Predicting COVID-19 Disease Severity Based on Clinical Blood Test Data: Statistical Analysis and Model Development. JMIR Med. Inf. 2021, 9, e25884. [Google Scholar] [CrossRef]
- Iwendi, C.; Bashir, A.K.; Peshkar, A.; Sujatha, R.; Chatterjee, J.M.; Pasupuleti, S.; Mishra, R.; Pillai, S.; Jo, O. COVID-19 Patient Health Prediction Using Boosted Random Forest Algorithm. Front. Public Health 2020, 8, 357. [Google Scholar] [CrossRef]
- Cornelius, E.; Akman, O.; Hrozencik, D. COVID-19 Mortality Prediction Using Machine Learning-Integrated Random Forest Algorithm under Varying Patient Frailty. Mathematics 2021, 9, 2043. [Google Scholar] [CrossRef]
- Sharma, D.K.; Subramanian, M.; Malyadri, P.; Reddy, B.S.; Sharma, M.; Tahreem, M. Classification of COVID-19 by using supervised optimized machine learning technique. Mater. Today Proc. 2021. [Google Scholar] [CrossRef]
- Ahamad, M.M.; Aktar, S.; Rashed-Al-Mahfuz, M.; Uddin, S.; Lio, P.; Xu, H.; Summers, M.A.; Quinn, J.M.W.; Moni, M.A. A machine learning model to identify early stage symptoms of SARS-Cov-2 infected patients. Expert Syst. Appl. 2020, 160, 113661. [Google Scholar] [CrossRef]
- Canas, L.S.; Osterdahl, M.F.; Deng, J.; Hu, C.; Selvachandran, S.; Polidori, L.; May, A.; Molteni, E.; Murray, B.; Chen, L.; et al. Disentangling post-vaccination symptoms from early COVID-19. EClinicalMedicine 2021, 42, 101212. [Google Scholar] [CrossRef]
- Uddin, S.; Khan, A.; Hossain, M.E.; Moni, M.A. Comparing different supervised machine learning algorithms for disease prediction. BMC Med. Inf. Decis. Mak. 2019, 19, 281. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ML/Evaluation Tool | Principle | Settings | References |
|---|---|---|---|
| Random Forest (RF) | A multipurpose ML method for classification. RF is based on an ensemble of decision trees (DTs). Each tree predicts a classification independently and “votes” for the related class, and the majority of votes decide the overall RF predictions. | Splitting criterion is the information gain ratio; the number of trees is 100. No limitations were imposed on the number of levels or minimum node size. The accuracy was calculated using out-of-bag internal validation. | [49,50,51] |
| eXtreme Gradient Boosting (XGBoost) | XGBoost depends on the ensemble of weak DT-type models to create boosted, DT-type models. This system includes a new tree learning algorithm, a theoretically justified weighted quantile sketch procedure with parallel, and distributed computing. | Tree booster was implemented with depth wise grow policy, boosting rounds = 100, Eta = 0.3, Gamma = 0, maximum depth = 6, minimum child weight = 1, maximum delta step = 0, sub-sampling rate = 1, column sampling rate by tree = 1, column sampling rate by level = 1, lambda = 1, Alpha = 0, sketch epsilon = 0.03, scaled position weight = 1, maximum number of bins = 256, sample type (uniform), normalize type (tree), and dropout rate = 0. | [52,53,54] |
| Multilayer Perceptron (MLP) | An implementation of the RProp algorithm for multilayer feed forward networks. MLP has the capability to learn nonlinear models in real-time. MLP can have one or more nonlinear hidden layers between the input and output layers. For each hidden layer, diverse numbers of hidden neurons can be assigned. Each hidden neuron grants a weighted linear summation for the values from the previous layer, and the nonlinear activation function is followed. The output values were determined after the output layer transforms the values from the last hidden layer. | Maximum number of iterations = 100, number of hidden layers = 3, and number of hidden neurons per layer = 10. | [55,56] |
| K-Star (K*) | It is an instance-based classifier. The class of a test instance is dependent upon the class of those training instances similar to, as determined by some similarity function. It varies from other instance-based learners by using an entropy-based distance function. | Average column entropy curve is used for missing mode, and manual blend setting is 20%. | [57,58] |
| Accuracy | Evaluation of ML models | Accuracy = (TP + TN)/N TP is the true positive (correctly classified predictions), TN is true negative (truly classified predictions), and N is the total number of evaluated cases. | [37,59] |
| Cohen’s kappa (κ) value | Evaluation of ML models | Cohen’s κ = (P0 + Pe)/(1 − Pe) P0 is the relative observed agreement among raters (i.e., accuracy), and Pe is the hypothetical probability of chance agreement. This was carried out by using the observed data to calculate the probabilities of each observer randomly seeing each category. If the raters are in complete agreement, then Cohen’s κ = 1. If there is no agreement among the raters other than what would be expected by chance (as given by Pe), Cohen’s κ = 0. Negative Cohen’s κ value implies the agreement is worse than random. | [59,60] |
| Compute Global Feature Importance | This application is a simple example of inspecting global feature importance for binary classification. In this example, the symptom data set is partitioned to training and test samples. Then, the black box model is trained on the pre-processed training data using the automated machine learning (AutoML) component. The Workflow Object capturing the pre-processing and the model is provided as an input for the global feature importance component together with the test data. The component provides the global feature importance according to interpretable global surrogate random forest models or generalized linear models (GLM). | AutoML: Models to train in AutoML = Gradient Boost, Metric for auto selection = Cohen’s κ value, hot encoding is used. Number of folds in cross validation = 4, Size of training set partition (%) = 80, Maximum amount of unique values in a categorical column = 100. Global feature Importance: Importance methods = Surrogate random forest and surrogate generalized linear model. Performance metric = Cohen’s κ value. The number of permutations = 3, Show top n features = 10, and maximum percentage of unique values in a categorical column = 100. | [61,62] |
| Probabilistic Neural Network (PNN) | A probabilistic neural network (PNN) is a type of feedforward neural network that is usually used to solve classification and pattern recognition tasks. A Parzen window and a non-parametric function are utilized to approximate the parent probability distribution function (PDF) of each class in the PNN method. The class probability of test data (new input data) is then estimated depending on the PDF of each class, and Bayes’ rule is used to allocate the class with the highest posterior probability to new input data. The risk of misclassification is reduced with this strategy. | PNN theta minus = 0.2 and theta plus = 0.4 and without specifying maximum number of epochs so that the PNN process is repeated until stable rule model is achieved. | [63,64] |
| Library for Support Vector Machines (LibSVM) | LIBSVM supports classification and regression by performing the sequential minimum optimization (SMO) algorithm for kernelized support vector machines (SVMs). SVM is an effective tool for both classification and regression. This operator supports the C-SVC and nu-SVC SVM types for classification tasks. The standard SVM uses a set of input data and predicts which of two potential classes the input belongs to for each given input, considering it a non-probabilistic binary linear classifier. An SVM training algorithm builds a model that allocates new examples to one of two categories based on a set of training examples that have been labeled as belonging to one of two categories. An SVM model is a representation of the examples as points in space, mapped so that the examples of the different categories are separated by a large distance. New examples are then mapped into the same space and classified according to which side of the gap they fall on. | C-SVM and nu-SVM. C methods were attempted, C and nu are regularization parameters that penalize misclassifications. C ranges from 0 to infinity while nu ranges between 0 and 1 and represents the lower and upper bound on the number of examples that are support vectors and that lie on the wrong side of the hyperplane. The following default settings were used in both SVM methods as implemented in the WEKA-KNIME (version 4.1.3) LibSVM node, these include: Kernel Cache (Cache Size = 40.0), kernel type is radial basis function: exp (−gamma×|u − v|2), and loss function is 0.1, kernel coefficients epsilon = 0.001 and Gamma = 0.00. However, in nu-SVM the optimized nu value of 0.1 was used (identified using Bayesian Optimization (TPE) implemented in KNIME). | [65,66,67,68] |
| Adaptive Boosting (AdaBoost) | AdaBoost algorithm is used as a statistical classification meta-algorithm. AdaBoost is adaptive in that it tweaks succeeding weak learners in favor of instances misclassified by earlier classifiers. It may be less likely to face the overfitting problem than other learning algorithms in particular situations. Individual learners may be poor, but as long as their performance is marginally better than random guessing, the final model will converge to a powerful learner. | Percentage of weight mass to base training on = 100, Random number seed = 1, Number of iterations = 10, and base is DecisionStump. | [69,70] |
| Gradient Boosting (GB) | GB is a machine learning technique that can be utilized for different applications, including regression and classification. It returns a prediction model in the form of an ensemble of weak prediction models, most commonly decision trees. The occurring approach is called GB trees when a decision tree is the weak learner; it usually outperforms random forest. A GB trees model is constructed in the same stage-wise manner as other boosting approaches, but it varies in that it allows optimization of any differentiable loss function. | Limit number of levels (tree depth) = 4, number of models = 10, and learning rate = 0.1 | [71,72,73] |
| K-Nearest Neighbor (KNN) | KNN is either used for classification and regression, the input includes the k closest training examples in a data set. The output depends on whether KNN is employed for classification or regression. In classification, the output is a class membership. An object is classified by the overall vote of its neighbors, with the object being assigned to the class most common among its k nearest neighbors (k is a positive integer). | Number of neighbors to consider (k) = 5, weight neighbors by distance is on. | [74,75] |
| Locally Weighted Learning (LWL) | Locally Weighted Learning methods are non-parametric and the current prediction is done by local functions. The basic idea behind LWL is that instead of building a global model for the whole function space, for each point of interest a local model is created based on neighboring data of the query point. | The nearest neighbor search algorithm to use = LinearNNSearch, the number of neighbors used to set the kernel bandwidth = all, the weighting kernel shape to use = Linear, and base classifier is a Decision Stump. | [76] |
| Country | Participants n (%) | Gender n (%) | Age (Year). n (%) | Education n (%) | Healthcare Worker n (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | <20 | 20–39 | 40–59 | >60 | High School or Less | Undergraduate | Postgraduate | Yes | No | ||
| Lebanon | 1946 (19) | 843 (43) | 1103 (57) | 501 (26) | 1156 (59) | 247 (13) | 42 (2) | 187 (9) | 1300 (67) | 459 (24) | 654 (34) | 1292 (66) |
| Jordan | 1714 (17) | 523 (31) | 1191 (69) | 28 (2) | 1211 (70) | 442 (26) | 33 (2) | 179 (11) | 1219 (71) | 316 (18) | 423 (25) | 1291 (75) |
| Saudi Arabia | 1561 (16) | 665 (43) | 896 (57) | 32 (2) | 825 (53) | 576 (37) | 128 (8) | 211 (14) | 980 (62) | 370 (24) | 537 (34) | 1024 (66) |
| Iraq | 934 (9) | 501 (54) | 433 (46) | 48 (5) | 633 (68) | 233 (25) | 20 (2) | 111 (12) | 704 (75) | 119 (13) | 252 (27) | 682 (73) |
| Egypt | 751 (7) | 311 (41) | 440 (59) | 7 (1) | 449 (60) | 266 (35) | 29 (4) | 37 (5) | 515 (69) | 199 (26) | 171 (23) | 580 (77) |
| Palestine | 531 (5) | 187 (35) | 344 (65) | 37 (7) | 360 (68) | 117 (22) | 17 (3) | 31 (6) | 419 (79) | 81 (15) | 250 (47) | 281 (53) |
| Algeria | 407 (4) | 231 (57) | 176 (43) | 3 (1) | 226 (55) | 158 (39) | 20 (5) | 66 (16) | 80 (20) | 261 (64) | 90 (22) | 317 (78) |
| Tunisia | 376 (4) | 158 (42) | 218 (58) | 1 | 119 (32) | 201 (53) | 55 (15) | 75 (20) | 81 (22) | 220 (58) | 61 (16) | 315 (84) |
| Syria | 339 (3) | 247 (73) | 92 (27) | 5 (1) | 133 (39) | 152 (45) | 49 (15) | 41 (12) | 144 (43) | 154 (45) | 247 (73) | 92 (27) |
| Libya | 316 (3) | 164 (52) | 152 (48) | 3 (1) | 115 (36) | 154 (49) | 44 (14) | 42 (13) | 208 (66) | 66 (21) | 69 (22) | 247 (78) |
| Qatar | 263 (3) | 160 (61) | 103 (39) | 1 | 142 (54) | 111 (42) | 9 (3) | 14 (5) | 188 (72) | 61 (23) | 63 (24) | 200 (76) |
| Kuwait | 239 (2) | 126 (53) | 113 (47) | 0 | 121 (51) | 113 (47) | 5 (2) | 36 (15) | 167 (70) | 36 (15) | 36 (15) | 203 (85) |
| Morocco | 196 (2) | 105 (54) | 91 (46) | 3 (2) | 130 (66) | 53 (27) | 10 (5) | 14 (7) | 61 (31) | 121 (62) | 32 (16) | 164 (84) |
| Bahrain | 179 (2) | 66 (37) | 113 (63) | 1 | 90 (50) | 56 (31) | 32 (18) | 30 (17) | 106 (59) | 43 (24) | 28 (16) | 151 (84) |
| UAE | 112 (1) | 66 (59) | 46 (41) | 1 | 55 (49) | 52 (46) | 4 (4) | 18 (16) | 59 (53) | 35 (31) | 22 (20) | 90 (80) |
| Oman | 76 (1) | 43 (57) | 33 (43) | 1 (1) | 35 (46) | 35 (46) | 5 (7) | 1 (1) | 47 (62) | 28 (37) | 9 (12) | 67 (88) |
| Sudan | 63 (1) | 33 (52) | 30 (48) | 0 | 50 (79) | 12 (19) | 1 (2) | 10 (16) | 32 (51) | 21 (33) | 14 (22) | 49 (78) |
| Yemen | 50 | 18 (36) | 32 (64) | 2 (4) | 34 (68) | 13 (26) | 1 (2) | 13 (26) | 22 (44) | 15 (30) | 14 (28) | 36 (72) |
| Mauritania | 11 | 5 (45) | 6 (55) | 0 | 8 (73) | 2 (18) | 1 (9) | 3 (27) | 5 (45) | 3 (27) | 3 (27) | 8 (73) |
| Total | 10,064 | 4466 (44) | 5598 (56) | 674 (6) | 5892 (59) | 2992 (30) | 505 (5) | 1119 (11) | 6337 (63) | 2608 (26) | 2975 (30) | 7089 (70) |
| Vaccine | Participants n (%) | Dose n (%) | |
|---|---|---|---|
| One | Two | ||
| Pfizer-BioNTech 1 | 5310 (52.8) | 2948 (56) | 2362 (44) |
| AstraZeneca 2 | 2087 (20.7) | 1200 (57) | 887 (43) |
| Sinopharm 3 | 1433 (14.2) | 511 (36) | 922 (64) |
| Sputnik V 4 | 587 (5.8) | 299 (51) | 288 (49) |
| SinoVac 5 | 468 (4.6) | 306 (65) | 162 (35) |
| Moderna 6 | 121 (1.2) | 35 (29) | 86 (71) |
| Johnson & Johnson 7 | 58 (0.6) | 57 (98) | 1 (2) |
| Total | 10,064 | 5356 (53) | 4708 (47) |
| Post-Vaccination Side Effects | Statistical Values | Predisposing Factors | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | Age | Education Level | Being a Healthcare Worker | Country | Type of COVID-19 Vaccine | Number of Doses | Suffering from Chronic Diseases | Being Smoker | Suffering from Food and/or Drug Allergies | Experiencing COVID-19 Vaccine Hesitancy and Related Fears before Vaccination | Experiencing COVID-19 Infection before Vaccination | ||
| Tiredness | χ2 | 348.81 | 216.92 | 50.86 | 3.48 | 470.66 | 381.94 | 23.71 | 48.16 | 5.88 | 10.41 | 214.27 | 59.66 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.062 | 0.000 | 0.000 | 0.000 | 0.000 | 0.015 | 0.001 | 0.000 | 0.000 | |
| Anxiety, depression and sleep disorders | χ2 | 93.64 | 98.68 | 26.43 | 5.54 | 298.51 | 162.81 | 3.97 | 35.31 | 0.57 | 11.31 | 318.11 | 55.97 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.019 | 0.000 | 0.000 | 0.046 | 0.000 | 0.452 | 0.001 | 0.000 | 0.000 | |
| Fever | χ2 | 66.59 | 114.72 | 15.32 | 9.05 | 492.59 | 706.12 | 57.02 | 21.30 | 3.72 | 11.58 | 84.99 | 13.84 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.003 | 0.000 | 0.000 | 0.000 | 0.019 | 0.054 | 0.001 | 0.000 | 0.000 | |
| Headache | χ2 | 243.11 | 107.78 | 27.07 | 0.01 | 307.95 | 271.56 | 32.42 | 30.95 | 3.70 | 27.64 | 176.27 | 39.54 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.910 | 0.000 | 0.000 | 0.000 | 0.001 | 0.054 | 0.000 | 0.000 | 0.000 | |
| Haziness or lack-of-clarity in eyesight | χ2 | 64.72 | 30.74 | 12.97 | 15.70 | 215.74 | 66.93 | 1.13 | 46.56 | 3.49 | 16.80 | 171.83 | 9.72 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.002 | 0.000 | 0.000 | 0.000 | 0.287 | 0.000 | 0.062 | 0.000 | 0.000 | 0.002 | |
| Injection site pain and swelling | χ2 | 387.31 | 181.27 | 61.68 | 5.79 | 461.47 | 508.68 | 7.11 | 35.63 | 9.89 | 15.91 | 132.81 | 29.94 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.016 | 0.000 | 0.000 | 0.008 | 0.000 | 0.002 | 0.000 | 0.000 | 0.000 | |
| Joint pain | χ2 | 187.85 | 122.97 | 22.08 | 4.04 | 389.40 | 327.40 | 42.95 | 63.59 | 0.09 | 16.66 | 189.04 | 38.26 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.045 | 0.000 | 0.000 | 0.000 | 0.000 | 0.761 | 0.000 | 0.000 | 0.000 | |
| Swollen ankles and feet | χ2 | 117.35 | 22.95 | 7.01 | 18.60 | 120.82 | 7.89 | 1.43 | 124.63 | 0.71 | 10.89 | 112.60 | 6.18 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.030 | 0.000 | 0.000 | 0.246 | 0.231 | 0.000 | 0.400 | 0.001 | 0.000 | 0.013 | |
| Myalgia | χ2 | 179.21 | 138.21 | 39.27 | 1.63 | 368.75 | 321.06 | 32.88 | 41.58 | 0.24 | 10.39 | 159.93 | 19.34 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.201 | 0.000 | 0.000 | 0.000 | 0.000 | 0.627 | 0.001 | 0.000 | 0.000 | |
| Nausea | χ2 | 274.59 | 72.92 | 16.38 | 3.50 | 104.42 | 83.96 | 0.44 | 28.65 | 4.53 | 25.38 | 155.06 | 20.94 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.061 | 0.000 | 0.000 | 0.507 | 0.001 | 0.033 | 0.000 | 0.000 | 0.000 | |
| Abdominal pain | χ2 | 134.48 | 72.89 | 9.14 | 14.43 | 151.04 | 44.69 | 4.51 | 34.72 | 0.08 | 13.60 | 142.77 | 33.27 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.010 | 0.000 | 0.000 | 0.000 | 0.034 | 0.000 | 0.778 | 0.000 | 0.000 | 0.000 | |
| Diarrhea | χ2 | 33.21 | 43.37 | 4.60 | 17.71 | 143.62 | 22.58 | 2.51 | 30.88 | 0.05 | 5.38 | 78.07 | 39.61 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.100 | 0.000 | 0.000 | 0.001 | 0.113 | 0.001 | 0.828 | 0.020 | 0.000 | 0.000 | |
| Vomiting | χ2 | 41.27 | 20.50 | 2.55 | 0.60 | 51.06 | 53.68 | 0.00 | 6.06 | 0.00 | 12.34 | 22.14 | 3.52 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.279 | 0.438 | 0.000 | 0.000 | 0.966 | 0.810 | 0.972 | 0.000 | 0.000 | 0.061 | |
| Bruises on the body | χ2 | 90.06 | 20.69 | 5.77 | 2.05 | 101.13 | 33.58 | 0.01 | 24.71 | 0.03 | 12.77 | 35.97 | 15.82 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.056 | 0.152 | 0.000 | 0.000 | 0.906 | 0.006 | 0.854 | 0.000 | 0.000 | 0.000 | |
| Bleeding gums | χ2 | 1.50 | 3.49 | 0.88 | 1.13 | 28.95 | 12.13 | 2.12 | 52.34 | 0.02 | 9.50 | 29.27 | 0.21 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.220 | 0.322 | 0.643 | 0.288 | 0.049 | 0.059 | 0.146 | 0.000 | 0.876 | 0.002 | 0.000 | 0.650 | |
| Nosebleed | χ2 | 0.00 | 2.34 | 0.54 | 3.22 | 60.02 | 8.73 | 6.98 | 27.03 | 5.36 | 1.45 | 148.50 | 2.15 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.983 | 0.504 | 0.763 | 0.073 | 0.000 | 0.190 | 0.008 | 0.003 | 0.021 | 0.229 | 0.000 | 0.143 | |
| Chills | χ2 | 158.18 | 102.65 | 16.33 | 0.97 | 433.68 | 454.30 | 77.70 | 37.08 | 0.04 | 13.95 | 87.51 | 11.70 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.325 | 0.000 | 0.000 | 0.000 | 0.000 | 0.840 | 0.000 | 0.000 | 0.001 | |
| Itchy skin, or irritation and allergic reactions | χ2 | 58.98 | 12.02 | 0.60 | 12.36 | 92.68 | 18.55 | 0.18 | 52.73 | 0.81 | 59.50 | 81.86 | 9.47 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.007 | 0.739 | 0.000 | 0.000 | 0.005 | 0.669 | 0.000 | 0.369 | 0.000 | 0.000 | 0.002 | |
| Sweating for no reason | χ2 | 37.25 | 28.36 | 8.14 | 10.11 | 155.91 | 177.94 | 0.85 | 45.68 | 14.80 | 21.38 | 144.52 | 39.40 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.017 | 0.001 | 0.000 | 0.000 | 0.356 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| Cold, numbness and tingling in limbs | χ2 | 109.93 | 64.64 | 20.86 | 8.64 | 192.88 | 199.45 | 0.09 | 38.75 | 0.64 | 19.52 | 231.80 | 16.26 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.003 | 0.000 | 0.000 | 0.758 | 0.000 | 0.424 | 0.000 | 0.000 | 0.000 | |
| Dizziness | χ2 | 285.06 | 94.20 | 25.85 | 11.04 | 335.10 | 145.06 | 1.50 | 27.40 | 5.69 | 16.35 | 56.85 | 29.22 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.001 | 0.000 | 0.000 | 0.221 | 0.002 | 0.017 | 0.000 | 0.000 | 0.000 | |
| Clogged nose | χ2 | 32.47 | 37.68 | 11.81 | 1.52 | 148.96 | 31.09 | 0.00 | 35.31 | 1.00 | 19.87 | 40.92 | 18.33 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.003 | 0.218 | 0.000 | 0.000 | 0.986 | 0.000 | 0.317 | 0.000 | 0.000 | 0.000 | |
| Runny nose | χ2 | 37.74 | 18.53 | 5.57 | 0.21 | 93.77 | 17.16 | 0.01 | 41.96 | 0.08 | 19.64 | 101.46 | 14.23 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.062 | 0.645 | 0.000 | 0.009 | 0.940 | 0.000 | 0.774 | 0.000 | 0.000 | 0.000 | |
| Dyspnea | χ2 | 64.95 | 44.31 | 16.76 | 10.40 | 176.86 | 43.71 | 0.83 | 44.31 | 0.95 | 20.91 | 119.88 | 15.16 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.001 | 0.000 | 0.000 | 0.363 | 0.000 | 0.329 | 0.000 | 0.000 | 0.000 | |
| Chest pain | χ2 | 33.30 | 57.66 | 13.37 | 12.47 | 246.59 | 59.47 | 0.28 | 53.52 | 2.46 | 22.91 | 208.47 | 24.24 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.001 | 0.000 | 0.000 | 0.000 | 0.599 | 0.000 | 0.117 | 0.000 | 0.000 | 0.000 | |
| Sleepiness and laziness | χ2 | 284.72 | 173.50 | 38.46 | 4.84 | 309.15 | 135.99 | 7.45 | 34.98 | 1.01 | 11.35 | 204.67 | 35.19 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.028 | 0.000 | 0.000 | 0.006 | 0.000 | 0.315 | 0.001 | 0.000 | 0.000 | |
| Irregular heartbeats | χ2 | 117.55 | 56.90 | 12.73 | 4.63 | 306.14 | 86.46 | 0.72 | 70.05 | 0.42 | 33.00 | 101.57 | 32.87 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.002 | 0.031 | 0.000 | 0.000 | 0.396 | 0.000 | 0.515 | 0.000 | 0.000 | 0.000 | |
| Abnormal blood pressure | χ2 | 56.78 | 17.41 | 12.73 | 3.43 | 199.35 | 57.09 | 0.31 | 114.06 | 0.81 | 12.57 | 148.15 | 12.59 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.001 | 0.002 | 0.064 | 0.000 | 0.000 | 0.579 | 0.000 | 0.367 | 0.000 | 0.000 | 0.000 | |
| Sore or dry throat | χ2 | 102.02 | 43.03 | 16.45 | 23.87 | 213.90 | 52.52 | 5.43 | 36.76 | 0.01 | 34.92 | 49.70 | 31.62 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 1 | 1 | |
| p | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.020 | 0.000 | 0.917 | 0.000 | 0.000 | 0.000 | |
| Cough | χ2 | 22.65 | 27.59 | 14.40 | 2.63 | 112.21 | 21.98 | 0.57 | 41.05 | 0.15 | 15.67 | 227.95 | 4.36 |
| DF | 1 | 3 | 2 | 1 | 18 | 6 | 1 | 10 | 1 | 1 | 3 | 1 | |
| p | 0.000 | 0.000 | 0.001 | 0.105 | 0.000 | 0.001 | 0.451 | 0.000 | 0.694 | 0.000 | 0.000 | 0.037 | |
| Severity of post-vaccination side effects | χ2 | 345.78 | 199.75 | 32.52 | 0.46 | 788.45 | 888.54 | 36.81 | 72.85 | 11.86 | 28.11 | 214.27 | 40.93 |
| DF | 3 | 9 | 6 | 3 | 54 | 18 | 3 | 30 | 3 | 3 | 1 | 3 | |
| p | 0.000 | 0.000 | 0.000 | 0.928 | 0.000 | 0.000 | 0.000 | 0.000 | 0.008 | 0.000 | 0.000 | 0.000 | |
| Variable | COVID-19 Vaccine Breakthrough Infection | Real Value | Expected Value | DF | χ2 | p | |
|---|---|---|---|---|---|---|---|
| Vaccine type | AstraZeneca | No | 1925 | 1988.56 | 6 | 76.98 | 0.000 |
| Yes | 161 | 97.43 | |||||
| Pfizer-BioNTech | No | 5141 | 5061.01 | ||||
| Yes | 169 | 247.98 | |||||
| Sinopharm | No | 1351 | 1366.06 | ||||
| Yes | 82 | 66.93 | |||||
| Johnson & Johnson | No | 54 | 55.29 | ||||
| Yes | 4 | 2.70 | |||||
| Moderna | No | 117 | 115.34 | ||||
| Yes | 4 | 5.65 | |||||
| Sputnik V | No | 563 | 559.58 | ||||
| Yes | 24 | 27.41 | |||||
| SinoVac | No | 441 | 446.13 | ||||
| Yes | 27 | 21.86 | |||||
| Number of doses | One | No | 5126 | 5103.91 | 1 | 4.37 | 0.036 |
| Yes | 229 | 250.08 | |||||
| Two | No | 4466 | 4488.08 | ||||
| Yes | 242 | 219.91 | |||||
| Post-Vaccination Side Effects | ML Tools | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| XGBoost | RF | MLP | PNN | LibSVM (nu) | LibSVM (c) | AdaBoost | GB | KNN | K* | LWL | |
| Tiredness | 68 (32) * | 68 (33) * | 66 (27) * | 59 (0) | 59 (17) | 59 (16) | 66 (24) * | 69 (33) * | 62 (17) | 66 (29) * | 63 (23) * |
| Injection site pain and swelling | 66 (29) * | 66 (31) * | 65 (27) * | 58 (0) | 59 (15) | 58 (15) | 64 (25) * | 67 (31) * | 61 (17) | 66 (28) * | 61 (20) * |
| Sleepiness and laziness | 61 (22) * | 63 (23) * | 61 (21) * | 54 (0) | 56 (11) | 56 (11) | 62 (22) * | 63 (25) * | 59 (16) | 62 (23) * | 58 (17) |
| Headache | 63 (25) * | 64 (25) * | 62 (22) * | 55 (0) | 55 (10) | 56 (11) | 61 (20) | 64 (26) * | 59 (16) | 63 (24) * | 59 (18) |
| Myalgia | 65 (25) * | 65 (23) * | 64 (23) * | 59 (0) | 57 (11) | 57 (11) | 63 (20) * | 66 (27) * | 61 (16) | 64 (23) * | 62 (14) |
| Fever | 67 (30) * | 68 (28) * | 66 (26) * | 61 (0) | 59 (14) | 58 (14) | 67 (26) * | 69 (31) * | 62 (18) | 67 (28) * | 65 (21) |
| Joint pain | 66 (24) * | 67 (21) * | 66 (23) * | 62 (0) | 58 (11) | 58 (12) | 65 (18) | 67 (26) * | 63 (13) | 65 (19) | 64 (15) |
| Dizziness | 71 (16) | 72 (10) | 72 (13) | 72 (0) | 62 (10) | 62 (10) | 72 (7) | 72 (15) | 70 (12) | 71 (16) | 72 (0) |
| Chills | 78 (11) | 79 (3) | 79 (2) | 79 (0) | 67 (8) | 66 (7) | 79 (0) | 79 (6) | 77 (9) | 78 (9) | 79 (0) |
| Anxiety, depression and sleep disorders | 72 (16) | 73 (10) | 73 (8) | 73 (0) | 61 (7) | 61 (7) | 73 (6) | 73 (14) | 71 (15) | 72 (14) | 73 (0) |
| Cold, numbness and tingling in limbs | 73 (22) * | 74 (16) | 73 (17) | 72 (0) | 62 (10) | 63 (13) | 73 (9) | 74 (22) * | 70 (13) | 72 (18) | 72 (0) |
| Sweating for no reason | 79 (7) | 81 (2) | 80 (2) | 81 (0) | 70 (7) | 66 (5) | 81 (0) | 80 (4) | 79 (8) | 80 (7) | 81 (0) |
| Sore or dry throat | 81 (6) | 82 (2) | 82 (4) | 82 (0) | 70 (6) | 70 (6) | 82 (0) | 82 (3) | 80 (6) | 81 (5) | 82 (0) |
| Nausea | 82 (8) | 84 (2) | 83 (1) | 84 (0) | 73 (11) | 74 (8) | 84 (0) | 83 (4) | 80 (8) | 83 (7) | 84 (0) |
| Irregular heartbeats | 84 (8) | 85 (2) | 84 (6) | 85 (0) | 75 (9) | 76 (10) | 85 (0) | 85 (5) | 84 (8) | 84 (9) | 85 (0) |
| Abdominal pain | 85 (6) | 86 (1) | 86 (1) | 86 (0) | 77 (9) | 77 (8) | 86 (0) | 85 (1) | 84 (9) | 85 (7) | 86 (0) |
| Clogged nose | 86 (4) | 87 (0) | 86 (1) | 87 (0) | 77 (4) | 78 (5) | 87 (0) | 87 (1) | 86 (8) | 86 (4) | 87 (0) |
| Haziness or lack-of-clarity in eyesight | 86 (7) | 87 (2) | 87 (0) | 87 (0) | 56 (11) | 78 (8) | 87 (0) | 87 (0) | 85 (8) | 87 (7) | 87 (0) |
| Dyspnea | 87 (4) | 88 (0) | 88 (2) | 88 (0) | 81 (9) | 81 (7) | 88 (0) | 88 (2) | 87 (7) | 88 (4) | 88 (0) |
| Chest pain | 88 (6) | 88 (2) | 88 (5) | 88 (0) | 80 (7) | 81 (8) | 88 (0) | 88 (3) | 87 (6) | 88 (5) | 88 (0) |
| Diarrhea | 88 (2) | 89 (1) | 89 (2) | 89 (0) | 82 (6) | 81 (5) | 89 (0) | 89 (1) | 87 (5) | 88 (5) | 89 (0) |
| Runny nose | 89 (4) | 89 (1) | 89 (2) | 89 (0) | 83 (6) | 83 (6) | 89 (0) | 89 (0) | 89 (5) | 89 (5) | 89 (0) |
| Cough | 91 (7) | 91 (1) | 91 (2) | 91 (0) | 87 (8) | 87 (8) | 91 (0) | 91 (3) | 91 (6) | 91 (7) | 91 (0) |
| Abnormal blood pressure | 91 (7) | 92 (0) | 91 (2) | 92 (0) | 88 (8) | 88 (8) | 92 (0) | 92 (3) | 91 (4) | 91 (5) | 92 (0) |
| Itchy skin, or irritation and allergic reactions | 92 (4) | 92 (1) | 92 (1) | 92 (0) | 89 (8) | 89 (8) | 92 (0) | 92 (3) | 91 (6) | 92 (5) | 92 (0) |
| Swollen ankles and feet | 95 (7) | 95 (1) | 95 (3) | 95 (0) | 93 (8) | 93 (12) | 95 (0) | 95 (4) | 95 (6) | 95 (7) | 95 (0) |
| Bruises on the body | 95 (4) | 92 (2) | 95 (2) | 95 (0) | 93 (8) | 93 (7) | 95 (0) | 95 (4) | 95 (9) | 95 (5) | 95 (0) |
| Vomiting | 96 (1) | 96 (0) | 96 (0) | 96 (0) | 95 (6) | 94 (5) | 96 (0) | 96 (1) | 96 (4) | 96 (5) | 96 (0) |
| Bleeding gums | 98 (0) | 99 (0) | 98 (2) | 99 (0) | 98 (5) | 98 (4) | 99 (0) | 98 (0) | 98 (7) | 98 (4) | 99 (0) |
| Nosebleed | 98 (4) | 99 (0) | 98 (2) | 99 (0) | 98 (4) | 98 (6) | 99 (0) | 99 (1) | 99 (5) | 99 (5) | 99 (0) |
| Severity of post-vaccination side effects | 45 (17) | 46 (17) | 44 (13) | 41 (0) | 38 (11) | 38 (11) | 41 (5) | 45 (17) | 42 (12) | 43 (15) | 41 (6) |
| Predisposing Factors | Post-Vaccination Side Effects | ||||||
|---|---|---|---|---|---|---|---|
| Tiredness | Fever | Headache | Injection Site Pain and Swelling | Myalgia | Numbness and Tingling in Limbs | Sleepiness and Laziness | |
| Gender | 1.86 | 0.82 | 1.56 | 1.71 | 1.05 | 0.71 | 1.81 |
| Age | 1.25 | 1.53 | 1.28 | 1.43 | 1.55 | 1.08 | 1.83 |
| Education level | 0.63 | 0.71 | 0.58 | 1.05 | 0.75 | 0.91 | 0.64 |
| Being a healthcare worker | 0.23 | 0.18 | 0.11 | 0.32 | 0.08 | 0.14 | 0.18 |
| Country | 2.33 | 2.18 | 2.10 | 2.18 | 2.24 | 2.12 | 2.03 |
| Suffering from chronic diseases | 1.45 | 1.69 | 1.23 | 1.47 | 1.67 | 1.69 | 1.69 |
| Being smoker | 0.11 | 0.19 | 0.16 | 0.24 | 0.04 | 0.31 | 0.09 |
| Suffering from food and/or drug allergies | 0.17 | 0.51 | 0.11 | 0.43 | 0.40 | 0.20 | 0.46 |
| Experiencing COVID-19 infection before receiving any vaccine dose | 0.52 | 0.057 | 0.73 | 0.32 | 0.26 | 0.15 | 0.75 |
| Experiencing COVID-19 vaccine hesitancy and related fears before vaccination | 1.22 | 0.91 | 1.03 | 0.92 | 0.89 | 1.08 | 1.2 |
| Type of COVID-19 vaccine | 2.03 | 2.58 | 2.34 | 2.48 | 2.15 | 2.44 | 1.65 |
| Interval between receiving a COVID-19 vaccine and participating in this study | 0.60 | 0.66 | 0.59 | 0.27 | 0.54 | 0.56 | 0.57 |
| Number of doses | 0.77 | 1.13 | 0.83 | 0.28 | 0.80 | 0.34 | 0.24 |
| Experiencing COVID-19 vaccine breakthrough infection | 0.16 | 0.44 | 0.48 | 0.45 | 0.25 | 0.78 | 0.17 |
| Time of breakthrough infection | 0.90 | 1.01 | 1.48 | 0.90 | 1.16 | 1.67 | 0.64 |
| Predisposing Factors | Post-Vaccination Side Effects | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tiredness | Fever | Headache | Injection Site Pain and Swelling | Myalgia | Sleepiness and Laziness | ||||||||
| GLM | RF | GLM | RF | GLM | RF | GLM | RF | GLM | RF | GLM | RF | ||
| Number of doses | Two | 9.93 | 0.6 | - | - | 7.1 | 0.93 | - | - | 3.72 | 0.91 | - | - |
| Gender | Female | 40.69 | 1.97 | - | - | - | - | 34.92 | 1.16 | 2.82 | 0.73 | - | - |
| Experiencing COVID-19 vaccine hesitancy and related fears before vaccination | Yes | 28.05 | 1.19 | - | - | 4.84 | 1.05 | 18.65 | 0.76 | 3.08 | 0.94 | 0.69 | 1.59 |
| Type of COVID-19 vaccine | AstraZeneca | 34.72 | 1.57 | 23.76 | 1.51 | 19.45 | 1.71 | 19.67 | 1.53 | 4.58 | 1.7 | 0.18 | 0.59 |
| Pfizer-BioNTech | −14.82 | 0.47 | −0.17 | 1.15 | 4.3 | 0.74 | 0.1 | 0.81 | −1.31 | 0.53 | 0.19 | 0.85 | |
| Sinopharm | −22.12 | 0.38 | −0.1 | 0.87 | −6.71 | 1.4 | −54.27 | 1.86 | −10.67 | 1.32 | −0.4 | 1.55 | |
| Moderna | 28.78 | 0.87 | 23.7 | 1.23 | 11.09 | 0.78 | 19.85 | 1.00 | 2.34 | 0.89 | 0.46 | 1.06 | |
| Sputnik V | −3.82 | 0.17 | −0.1 | 0.52 | −6.46 | 1.05 | −17.1 | 0.49 | 0.06 | 0.26 | −0.35 | 1.16 | |
| SinoVac | −28.84 | 0.62 | −0.1 | 0.35 | −6.16 | 0.91 | −54.07 | 1.48 | −8.76 | 0.74 | −0.37 | 0.87 | |
| Age (years) | <20 | - | - | - | - | - | - | - | - | −3.91 | 0.64 | - | - |
| 20–39 | - | - | - | - | - | - | - | - | −1.09 | 0.92 | - | - | |
| 40–59 | - | - | - | - | - | - | - | - | −4.55 | 0.44 | - | - | |
| >60 | - | - | - | - | - | - | - | - | −11.29 | 0.92 | - | - | |
| Country | Population | Sample Size | Vaccines (%) | Reference |
|---|---|---|---|---|
| Iraq | General population | 1012 | AstraZeneca (60.1) Pfizer-BioNTech (29.2) Sinopharm (10.7) | [77] |
| Jordan | General population | 2213 | Sinopharm (38.2) AstraZeneca (31) Pfizer-BioNTech (27.3) Sputnik V (2.9) Moderna, Coaxin, and Johnson & Johnson (0.6) | [13] |
| Jordan | General population | 1086 | Sinopharm (26.4) | [78] |
| Jordan | General population | 1004 | Sinopharm (51.1) Pfizer-BioNTech (48.9) | [79] |
| Jordan | Healthcare workers | 409 | AstraZeneca (43.8) Pfizer-BioNTech (34.5) Sinopharm (21.8) | [80] |
| Kuwait | People with epilepsy | 82 | Pfizer-BioNTech (62) AstraZeneca (38) | [81] |
| Oman | General population | 753 | AstraZeneca (78) Pfizer-BioNTech (22) | [82] |
| Saudi Arabia | General population | 18,543 | AstraZeneca (97.8) Pfizer-BioNTech (2.3) | [83] |
| Saudi Arabia | General population | 4170 | Pfizer-BioNTech (61) AstraZeneca (39) | [84] |
| Saudi Arabia | General population | 1592 | AstraZeneca | [85] |
| Saudi Arabia | General population | 515 | AstraZeneca (75) Pfizer-BioNTech (25) | [86] |
| Saudi Arabia | General population | 455 | Pfizer-BioNTech | [87] |
| Saudi Arabia | General population | 330 | AstraZeneca (50.6) Pfizer-BioNTech (49.4) | [88] |
| UAE | General population | 1080 | Sinopharm | [12] |
| Gender | Age Category (Year) | Country | Chronic Diseases | Smoking Status | Vaccine | Dose | Interval between Receiving a COVID-19 Vaccine and Thrombosis | Thrombocytopenia | Causes of Hospitalization/Type of Thrombosis (If Known) |
|---|---|---|---|---|---|---|---|---|---|
| Female | 20–39 | Egypt | Arthritis | No | AstraZeneca | 1 | 12–24 h | Yes | Cerebral venous thrombosis |
| Female | 40–59 | Egypt | Autoimmune diseases | No | AstraZeneca | 1 | Up to 4 h | Yes | Chest pain and dyspnea |
| Female | 40–59 | Egypt | Diabetes | No | AstraZeneca | 1 | More than 24 h | No | Chest pain and dyspnea |
| Male | 20–39 | Saudi Arabia | Obesity | No | AstraZeneca | 1 | More than 24 h | No | Chest pain and dyspnea |
| Female | 40–59 | Algeria | Thyroid disorders | No | AstraZeneca | 1 | Up to 4 h | Yes | - |
| Female | 40–59 | Algeria | - | No | AstraZeneca | 1 | More than 24 h | No | Numbness and tingling in the limbs, palpitation and hypertension |
| Female | 20–39 | Jordan | - | No | AstraZeneca | 1 | 5–12 h | No | Chest pain |
| Male | More than 60 | Egypt | Obesity and hypertension | No | AstraZeneca | 1 | More than 24 h | No | - |
| Male | 20–39 | Saudi Arabia | - | No | AstraZeneca | 2 | 5–12 h | Yes | Cerebral venous thrombosis |
| Female | 20–39 | Algeria | Hypertension | No | AstraZeneca | 2 | More than 24 h | Yes | Chest pain and hypoxemia |
| Female | 40–59 | Egypt | Autoimmune diseases and hypertension | No | AstraZeneca | 2 | Up to 4 h | Yes | Chest pain and dyspnea |
| Male | 20–39 | Jordan | - | Yes | AstraZeneca | 2 | More than 24 h | Yes | Fever |
| Female | 20–39 | Jordan | Respiratory diseases | No | AstraZeneca | 2 | 5–12 h | No | Chest pain, headache, blurry vision and dyspnea |
| Female | 40–59 | Jordan | Obesity, diabetes, cardiovascular diseases, thyroid disorders | No | Pfizer-BioNTech | 1 | Up to 4 h | No | Deep vein thrombosis in the leg, dyspnea, tachycardia and vomiting |
| Female | 40–59 | Tunisia | Arthritis | No | Pfizer-BioNTech | 1 | 12–24 h | No | Numbness in the left side of the body and hypertension |
| Male | 40–59 | Jordan | Diabetes, hypertension and obesity | Yes | Pfizer-BioNTech | 1 | More than 24 h | No | Pulmonary embolism and unconsciousness |
| Female | More than 60 | Saudi Arabia | Hypertension | No | Pfizer-BioNTech | 1 | More than 24 h | No | Cerebral venous thrombosis |
| Male | 20–39 | Iraq | - | Yes | Pfizer-BioNTech | 1 | 12–24 h | Yes | - |
| Male | 20–39 | Jordan | - | No | Pfizer-BioNTech | 2 | More than 24 h | No | Supraventricular tachycardia and elevated cardiac enzymes |
| Male | 20–39 | Iraq | Obesity | Yes | Pfizer-BioNTech | 2 | More than 24 h | No | - |
| Male | More than 60 | Jordan | Diabetes | Yes | Pfizer-BioNTech | 2 | 5–12 h | Yes | Dizziness |
| Female | More than 60 | Tunisia | Hypertension, obesity, diabetes, cardiovascular diseases, thyroid disorders and arthritis | Yes | Johnson & Johnson | 1 | Up to 4 h | Yes | Chest pain and dyspnea |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hatmal, M.M.; Al-Hatamleh, M.A.I.; Olaimat, A.N.; Mohamud, R.; Fawaz, M.; Kateeb, E.T.; Alkhairy, O.K.; Tayyem, R.; Lounis, M.; Al-Raeei, M.; et al. Reported Adverse Effects and Attitudes among Arab Populations Following COVID-19 Vaccination: A Large-Scale Multinational Study Implementing Machine Learning Tools in Predicting Post-Vaccination Adverse Effects Based on Predisposing Factors. Vaccines 2022, 10, 366. https://doi.org/10.3390/vaccines10030366
Hatmal MM, Al-Hatamleh MAI, Olaimat AN, Mohamud R, Fawaz M, Kateeb ET, Alkhairy OK, Tayyem R, Lounis M, Al-Raeei M, et al. Reported Adverse Effects and Attitudes among Arab Populations Following COVID-19 Vaccination: A Large-Scale Multinational Study Implementing Machine Learning Tools in Predicting Post-Vaccination Adverse Effects Based on Predisposing Factors. Vaccines. 2022; 10(3):366. https://doi.org/10.3390/vaccines10030366
Chicago/Turabian StyleHatmal, Ma’mon M., Mohammad A. I. Al-Hatamleh, Amin N. Olaimat, Rohimah Mohamud, Mirna Fawaz, Elham T. Kateeb, Omar K. Alkhairy, Reema Tayyem, Mohamed Lounis, Marwan Al-Raeei, and et al. 2022. "Reported Adverse Effects and Attitudes among Arab Populations Following COVID-19 Vaccination: A Large-Scale Multinational Study Implementing Machine Learning Tools in Predicting Post-Vaccination Adverse Effects Based on Predisposing Factors" Vaccines 10, no. 3: 366. https://doi.org/10.3390/vaccines10030366