
Simple Disposable Odor Identification Tests for Predicting SARS-CoV-2 Positivity


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Settings
2.2. Clinical Outcomes
- (1)
- General demographic data;
- (2)
- Medical history (comorbidities, chronic medication use, tobacco addiction, and pre-existing OD);
- (3)
- COVID-19 course (date of first symptoms, nasal, and general symptoms), and;
- (4)
- Olfactory function—participants rated their sense of smell at its worst since the onset of the disease (“recent OD”) as “normal”, “decreased”, or “none at all”, as well as using the visual analogue scale (VAS), from 0 (normal sense of smell) to 10 (no sense of smell).
2.3. Psychophysical Evaluation
2.4. Ethical Concerns
2.5. Statistical Analyses and ROC Analysis of COVID-19 Predictors
3. Results
3.1. Clinical Outcomes
3.2. Self-Reported Olfactory Function
3.3. Psychophysical Evaluation
- 10-SDOIT, evaluating the number of correct answers (correct identification of nine odors and reporting of no odor detection in an odorless sample);
- 9-SDOIT evaluating the number of identified odors out of nine odorants;
- 8-SDOIT evaluating the number of identified odors out of eight odorants (cinnamon, mint, lemon, coffee, clove, anise, camphor, and alcohol)—excluding odorant showing no significant differences between cases and controls (rose), and;
- 4-SDOIT evaluating the number of identified odors out of four odorants (cinnamon, mint, lemon, and alcohol)—showing the highest intergroup differences (with p ≤ 0.001).
3.4. Correlations between OD and Patient Characteristics
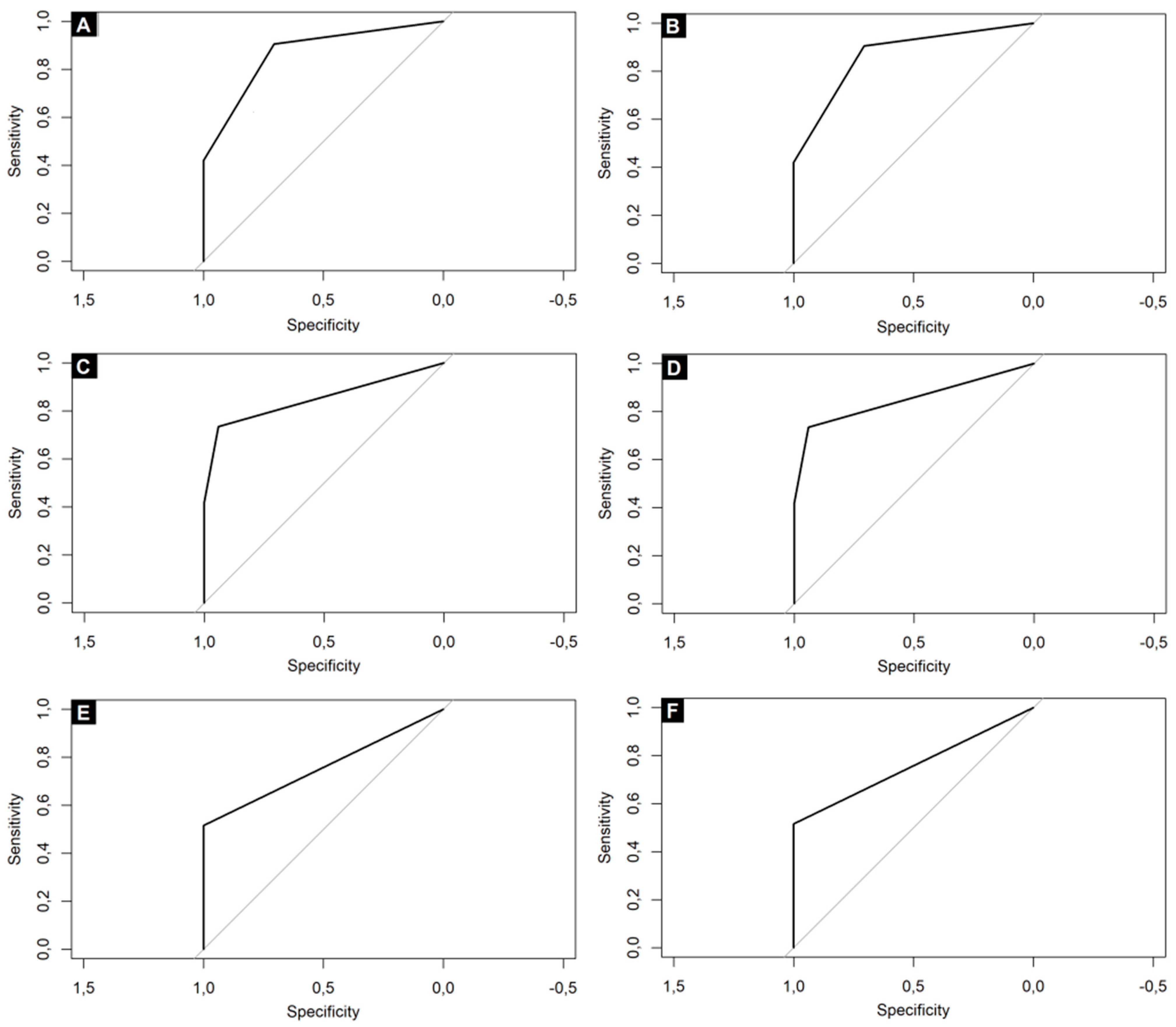
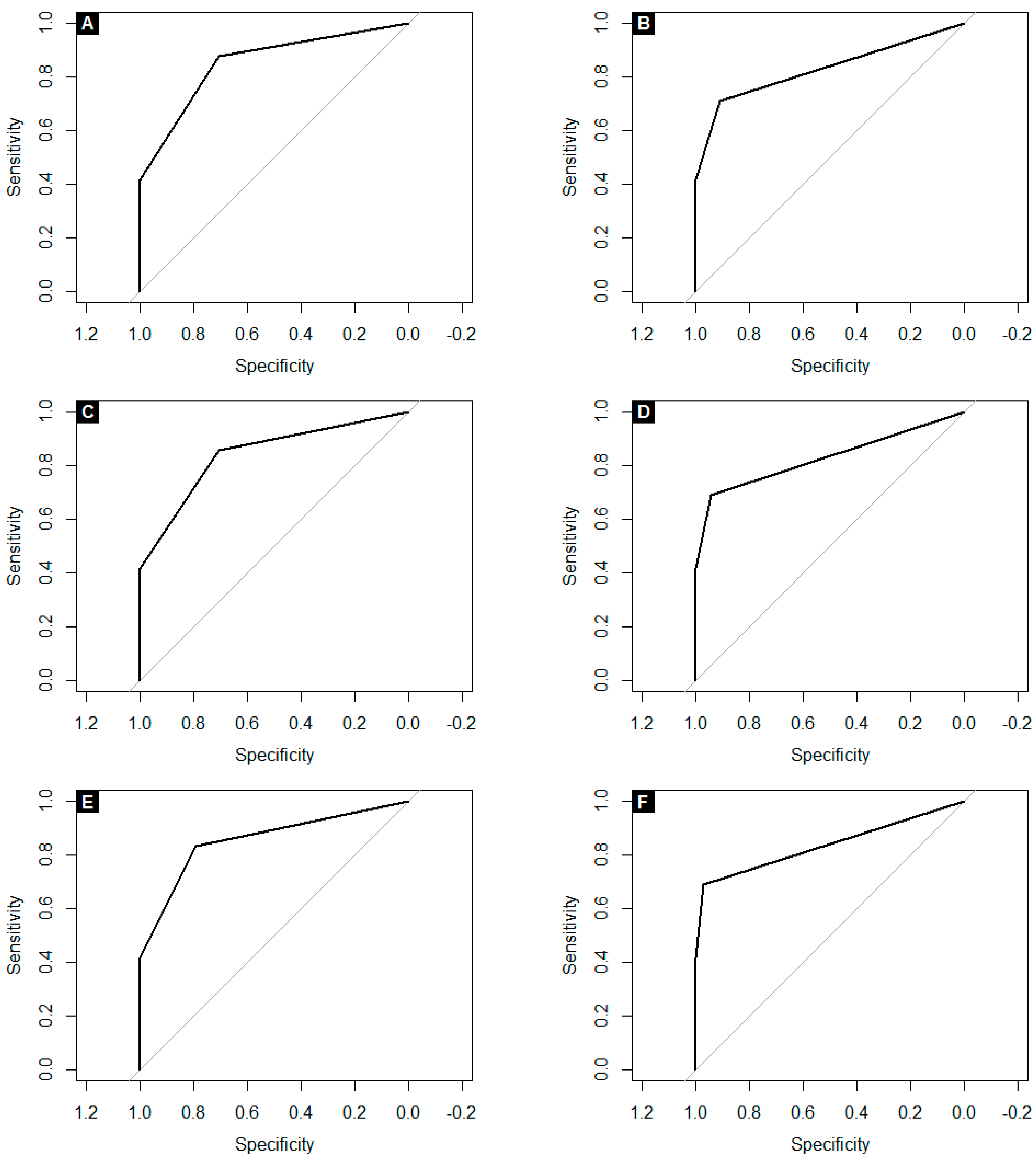
3.5. Assessment of COVID-19 Predictors and ROC Analysis
- (1)
- 0-9/10 correct answers in 10-SDOIT (with AUC of 0.87, sensitivity of 91%, specificity of 71%, PPV of 85% and NPV of 80%), and;
- (2)
- 0-7/8 identified odors in 8-SDOIT (with AUC of 0.87, sensitivity of 86%, specificity of 79%, PPV of 89% and NPV of 75%).
- (1)
- 0-9/10 correct answers in 10-SDOIT (with AUC of 0.85, sensitivity of 88%, specificity of 71%, PPV of 81% and NPV of 80%), and;
- (2)
- 0-7/8 identified odors in 8-SDOIT (with AUC of 0.86, sensitivity of 83%, specificity of 79%, PPV of 85% and NPV of 77%).
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients with Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Moein, S.T.; Hashemian, S.M.; Mansourafshar, B.; Khorram-Tousi, A.; Tabarsi, P.; Doty, R.L. Smell dysfunction: A biomarker for COVID-19. Int. Forum Allergy Rhinol. 2020, 10, 944–950. [Google Scholar] [CrossRef]
- Kaye, R.; Chang, C.; Kazahaya, K.; Brereton, J.; Denneny, J.C., 3rd. COVID-19 Anosmia Reporting Tool: Initial Findings. Otolaryngol. Head Neck Surg. 2020, 163, 132–134. [Google Scholar] [CrossRef]
- Klopfenstein, T.; Kadiane-Oussou, N.J.; Toko, L.; Royer, P.Y.; Lepiller, Q.; Gendrin, V.; Zayet, S. Features of anosmia in COVID-19. Med. Mal. Infect. 2020, 50, 436–439. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Lee, Y.; Min, P.; Lee, S.; Kim, S.W. Prevalence and Duration of Acute Loss of Smell or Taste in COVID-19 Patients. J. Korean Med. Sci. 2020, 35, e174. [Google Scholar] [CrossRef]
- Qiu, C.; Cui, C.; Hautefort, C.; Haehner, A.; Zhao, J.; Yao, Q.; Zeng, H.; Nisenbaum, E.J.; Liu, L.; Zhao, Y.; et al. Olfactory and Gustatory Dysfunction as an Early Identifier of COVID-19 in Adults and Children: An International Multicenter Study. Otolaryngol. Head Neck Surg. 2020, 163, 714–721. [Google Scholar] [CrossRef]
- Yan, C.H.; Faraji, F.; Prajapati, D.P.; Boone, C.E.; DeConde, A.S. Association of chemosensory dysfunction and COVID-19 in patients presenting with influenza-like symptoms. Int. Forum Allergy Rhinol. 2020, 10, 806–813. [Google Scholar] [CrossRef] [Green Version]
- Menni, C.; Valdes, A.M.; Freidin, M.B.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Ganesh, S.; Varsavsky, T.; Cardoso, M.J.; El-Sayed Moustafa, J.S.; et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat. Med. 2020, 26, 1037–1040. [Google Scholar] [CrossRef]
- Hummel, T.; Whitcroft, K.L.; Andrews, P.; Altundag, A.; Cinghi, C.; Costanzo, R.M.; Damm, M.; Frasnelli, J.; Gudziol, H.; Gupta, N.; et al. Position paper on olfactory dysfunction. Rhinology 2016, 56, 1–30. [Google Scholar] [CrossRef]
- Pang, K.W.; Chee, J.; Subramaniam, S.; Ng, C.L. Frequency and Clinical Utility of Olfactory Dysfunction in COVID-19: A Systematic Review and Meta-analysis. Curr. Allergy Asthma Rep. 2020, 20, 76. [Google Scholar] [CrossRef] [PubMed]
- Vaira, L.A.; Hopkins, C.; Salzano, G.; Petrocelli, M.; Melis, A.; Cucurullo, M.; Ferrari, M.; Gagliardini, L.; Pipolo, C.; Deiana, G.; et al. Olfactory and gustatory function impairment in COVID-19 patients: Italian objective multicenter-study. Head Neck 2020, 42, 1560–1569. [Google Scholar] [CrossRef] [PubMed]
- Hannum, M.E.; Ramirez, V.A.; Lipson, S.J.; Herriman, R.D.; Toskala, A.K.; Lin, C.; Joseph, P.V.; Reed, D.R. Objective sensory testing methods reveal a higher prevalence of olfactory loss in COVID-19 positive patients compared to subjective methods: A systematic review and metaanalysis. Chem. Senses 2020, 45, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Saniasiaya, J.; Islam, M.A.; Abdullah, B. Prevalence of Olfactory Dysfunction in Coronavirus Disease 2019 (COVID-19): A Meta-analysis of 27,492 Patients. Laryngoscope 2020, 131, 865–878. [Google Scholar] [CrossRef] [PubMed]
- Marchese-Ragona, R.; Restivo, D.A.; De Corso, E.; Vianello, A.; Nicolai, P.; Ottaviano, G. Loss of smell in COVID-19 patients: A critical review with emphasis on the use of olfactory tests. Acta Otorhinolaryngol. Ital. 2020, 40, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Iravani, B.; Arshamian, A.; Ravia, A.; Mishor, E.; Snitz, K.; Shushan, S.; Roth, Y.; Perl, O.; Honigstein, D.; Weissgross, R.; et al. Relationship between odor intensity estimates and COVID-19 prevalence prediction in a Swedish population. Chem. Senses 2020, 45, 449–456. [Google Scholar] [CrossRef]
- Vaira, L.A.; Deiana, G.; Fois, A.G.; Pirina, P.; Madeddu, G.; De Vito, A.; Babudieri, S.; Petrocelli, M.; Serra, A.; Bussu, F.; et al. Objective evaluation of anosmia and ageusia in COVID-19 patients: Single-center experience on 72 cases. Head Neck 2020, 42, 1252–1258. [Google Scholar] [CrossRef]
- Vaira, L.A.; Salzano, G.; Petrocelli, M.; Deiana, G.; Salzano, F.A.; De Riu, G. Validation of a self-administered olfactory and gustatory test for the remotely evaluation of COVID-19 patients in home quarantine. Head Neck 2020, 42, 1570–1576. [Google Scholar] [CrossRef]
- The Number of Infections in Poland–Historical Data from the Beginning of the Pandemic. Available online: https://arcgis.com/sharing/rest/content/items/b03b454aed9b4154ba50df4ba9e1143b/data? (accessed on 12 June 2021).
- Subbe, C.P.; Kruger, M.; Rutherford, P.; Gemmel, L. Validation of a modified Early Warning Score in medical admissions. QJM 2001, 94, 521–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Bartheld, C.S.; Hagen, M.M.; Butowt, R. Prevalence of Chemosensory Dysfunction in COVID-19 Patients: A Systematic Review and Meta-analysis Reveals Significant Ethnic Differences. ACS Chem. Neurosci. 2020, 11, 2944–2961. [Google Scholar] [CrossRef] [PubMed]
- Abdullahi, A.; Candan, S.A.; Abba, M.A.; Bello, A.H.; Alshehri, M.A.; Afamefuna Victor, E.; Umar, N.A.; Kundakci, B. Neurological and Musculoskeletal Features of COVID-19: A Systematic Review and Meta-Analysis. Front. Neurol. 2020, 11, 687. [Google Scholar] [CrossRef]
- Hopkins, C.; Surda, P.; Whitehead, E.; Kumar, B.N. Early recovery following new onset anosmia during the COVID-19 pandemic—An observational cohort study. J. Otolaryngol. Head Neck Surg. 2020, 49, 26. [Google Scholar] [CrossRef]
- Romero-Sánchez, C.M.; Díaz-Maroto, I.; Fernández-Díaz, E.; Sánchez-Larsen, Á.; Layos-Romero, A.; García-García, J.; González, E.; Redondo-Peñas, I.; Perona-Moratalla, A.B.; Del Valle-Pérez, J.A.; et al. Neurologic manifestations in hospitalized patients with COVID-19: The ALBACOVID registry. Neurology 2020, 95, e1060–e1070. [Google Scholar] [CrossRef]
- Le Bon, S.D.; Pisarski, N.; Verbeke, J.; Prunier, L.; Cavelier, G.; Thill, M.P.; Rodriguez, A.; Dequanter, D.; Lechien, J.R.; Le Bon, O.; et al. Psychophysical evaluation of chemosensory functions 5 weeks after olfactory loss due to COVID-19: A prospective cohort study on 72 patients. Eur. Arch. Otorhinolaryngol. 2021, 278, 101–108. [Google Scholar] [CrossRef]
- Lee, D.J.; Lockwood, J.; Das, P.; Wang, R.; Grinspun, E.; Lee, J.M. Self-reported anosmia and dysgeusia as key symptoms of coronavirus disease 2019. CJEM 2020, 22, 595–602. [Google Scholar] [CrossRef]
- Vaira, L.A.; Salzano, G.; Fois, A.G.; Piombino, P.; De Riu, G. Potential pathogenesis of ageusia and anosmia in COVID-19 patients. Int. Forum Allergy Rhinol. 2020, 10, 1103–1104. [Google Scholar] [CrossRef]
- Xu, H.; Zhong, L.; Deng, J.; Peng, J.; Dan, H.; Zeng, X.; Li, T.; Chen, Q. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int. J. Oral Sci. 2020, 12, 8. [Google Scholar] [CrossRef]
- Wee, L.E.; Chan, Y.; Teo, N.; Cherng, B.; Thien, S.Y.; Wong, H.M.; Wijaya, L.; Toh, S.T.; Tan, T.T. The role of self-reported olfactory and gustatory dysfunction as a screening criterion for suspected COVID-19. Eur. Arch. Otorhinolaryngol. 2020, 277, 2389–2390. [Google Scholar] [CrossRef] [Green Version]
- Karni, N.; Klein, H.; Asseo, K.; Benjamini, Y.; Israel, S.; Nammary, M.; Olshtain-Pops, K.; Nir-Paz, R.; Hershko, A.; Muszkat, M.; et al. Self-rated smell ability enables highly specific predictors of COVID-19 status: A case control study in Israel. Open Forum Infect. Dis. 2020, 8, ofaa589. [Google Scholar] [CrossRef]
- Huart, C.; Philpott, C.; Konstantinidis, I.; Altundag, A.; Whitcroft, K.L.; Trecca, E.; Cassano, M.; Rombaux, P.; Hummel, T. Comparison of COVID-19 and common cold chemosensory dysfunction. Rhinology 2020, 58, 623–625. [Google Scholar] [CrossRef]
- Carignan, A.; Valiquette, L.; Grenier, C.; Musonera, J.B.; Nkengurutse, D.; Marcil-Héguy, A.; Vettese, K.; Marcoux, D.; Valiquette, C.; Xiong, W.T.; et al. Anosmia and dysgeusia associated with SARS-CoV-2 infection: An age-matched case-control study. CMAJ 2020, 192, E702–E707. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Henriquez, C.; Maldonado-Alvarado, B.; Chiesa-Estomba, C.; Rivero-Fernández, I.; Sanz-Rodriguez, M.; Villarreal, I.M.; Rodriguez-Iglesias, M.; Mariño-Sánchez, F.; Rivero-de-Aguilar, A.; Lechien, J.R.; et al. Ethyl alcohol threshold test: A fast, reliable and affordable olfactory Assessment tool for COVID-19 patients. Eur. Arch. Otorhinolaryngol. 2020, 277, 2783–2792. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Title 1 | Title 2 |
|---|---|
| cinnamon | honey, vanilla, chocolate |
| mint | onion, gasoline, garlic |
| lemon | peach, apple, plum |
| coffee | tobacco, wine, smoke |
| clove | grass, garlic, chocolate |
| rose | green tea, strawberry, cherry |
| anise | peach, rose, mint |
| camphor | gas, caramel, onion |
| alcohol (disinfectant) | gasoline, cucumber, burned rubber |
| odorless sample | rose, garlic, lemon, mint |
| Characteristic | Total (N = 98) | COVID-19 Patients (N = 64) | Control Patients (N = 34) | |
|---|---|---|---|---|
| Age, years | mean ± SD | 48.4 ± 18.8 | 52.3 ± 20.9 | 40.9 ± 10.7 |
| median (IQR) | 47 (32–64) | 55 (33–68.5) | 40.5 (32–49.8) | |
| range | 20–91 | 20–91 | 27–61 | |
| Gender, N (%) | female | 55 (56.1%) | 29 (45.3%) | 26 (76.5%) |
| male | 43 (43.9%) | 35 (54.7%) | 8 (23.5%) | |
| Smoking history | nonsmoker, N (%) | 64 (65.3%) | 35 (54.7%) | 29 (85.3%) |
| former smoker, N (%) | 23 (23.5%) | 21 (32.8%) | 2 (5.9%) | |
| current smoker, N (%) | 11 (11.2%) | 8 (12.5%) | 3 (8.8%) | |
| Variable | Self-Reported OD | ||||||
|---|---|---|---|---|---|---|---|
| Presence of Self-Reported OD at the Time of the Survey | Presence of Self-Reported OD at Any Time since the Onset of COVID-19 | ||||||
| Yes (N = 21) | No (N = 43) | p-Value | Yes (N = 27) | No (N = 37) | p-Value | ||
| Nasal congestion, N (%) | yes | 11 (52.4) | 10 (23.3) | 0.041 1 | 14 (51.9) | 7 (18.9) | 0.012 1 |
| no | 10 (47.6) | 33 (76.7) | 13 (48.1) | 30 (81.1) | |||
| Rhinorrhea, N (%) | yes | 9 (42.9) | 10 (23.3) | 0.187 1 | 14 (51.9) | 5 (13.5) | 0.002 1 |
| no | 12 (57.1) | 33 (76.7) | 13 (48.1) | 32 (86.5) | |||
| Current smoking, N (%) | yes | 3 (14.3) | 5 (11.6) | 1 2 | 3 (11.1) | 5 (13.5) | 1 2 |
| no | 18 (85.7) | 38 (88.4) | 24 (88.9) | 32 (86.5) | |||
| Former or current smoking, N (%) | yes | 8 (38.1) | 21 (48.8) | 0.587 1 | 8 (29.6) | 21 (56.8) | 0.058 1 |
| no | 13 (61.9) | 22 (51.2) | 19 (70.4) | 16 (43.2) | |||
| Death, N (%) | yes | 2 (9.5) | 6 (14) | 1 2 | 2 (7.4) | 6 (16.2) | 0.450 2 |
| no | 19 (90.5) | 37 (86) | 25 (92.6) | 31 (83.8) | |||
| Need for oxygen therapy, N (%) | yes | 7 (33.3) | 21 (48.8) | 0.365 1 | 7 (25.9) | 21 (56.8) | 0.028 1 |
| no | 14 (66.7) | 22 (51.2) | 20 (74.1) | 16 (43.2) | |||
| Need for ICU stay, N (%) | yes | 1 (4.8) | 5 (11.6) | 0.654 2 | 1 (3.7) | 5 (13.5) | 0.388 2 |
| no | 20 (95.2) | 38 (88.4) | 26 (96.3) | 32 (86.5) | |||
| Time interval between first positive PCR result and time of the survey, days | Mean ± SD | 5.1 ± 4.2 | 7.6 ± 6.7 | 0.290 3 | 6.7 ± 4.8 | 7.1 ± 7 | 0.615 3 |
| Median (IQR) | 3 (2–8) | 6 (2–12) | 5 (2.5–12) | 4 (2–12) | |||
| Duration of hospitalisation (excluding deceased patients) | N | 19 | 37 | 0.862 3 | 25 | 31 | 0.060 3 |
| Mean ± SD | 19 ± 10.6 | 20.7 ± 14.2 | 16.6 ± 10.5 | 23 ± 14.3 | |||
| Median (IQR) | 17 (12–23.5) | 18 (10–24) | 13 (10–19) | 18 (15–28) | |||
| MEWS score at the time of the survey | Mean ± SD | 0.9 ± 1.3 | 0.9 ± 1.7 | 0.837 3 | 0.7 ± 1.1 | 1 ± 1.8 | 0.254 3 |
| Median (IQR) | 0 (0–1) | 0 (0–1) | 0 (0–1) | 1 (0–1) | |||
| Avarage MEWS score | Mean ± SD | 0.9 ± 1.5 | 1 ± 1.3 | 0.481 3 | 0.7 ± 1.4 | 1.1 ± 1.4 | 0.081 3 |
| Median (IQR) | 0 (0–1) | 1 (0–1) | 0 (0–1) | 1 (0–2) | |||
| Variable | SDOIT, % of Correct Answers | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 10-SDOIT | 9-SDOIT | 8-SDOIT | 4-SDOIT | ||||||
| Mean ± SD | Median (IQR) | Mean ± SD | Median (IQR) | Mean ± SD | Median (IQR) | Mean ± SD | Median (IQR) | ||
| Nasal congestion | yes | 72.9 ± 30.4 | 90 (50–100) | 72 ± 33.5 | 88.9 (55.6–100) | 71.4± 33.1 | 87.5 (50–100) | 70.2 ± 40 | 100 (25–100) |
| no | 63 ± 32.3 | 70 (45–90) | 62.5 ± 34.6 | 77.8 (44.4–88.9) | 62.8 ± 34.9 | 75 (37.5–87.5) | 55.8 ± 38.1 | 75 (25–87.5) | |
| p-value | 0.188 | 0.197 | 0.240 | 0.081 | |||||
| Rhinorrhea | yes | 73.7 ± 30.4 | 90 (50–100) | 73.1 ± 32.4 | 88.9 (56–100) | 73.3 ± 32.1 | 87.5 (56.3–100) | 69.7 ± 37.8 | 100 (37.5–100) |
| no | 63.1 ± 32.2 | 80 (40–90) | 62.5 ± 34.9 | 77.8 (44.4–88.9) | 62.5 ± 35.1 | 75 (37.5–87.5) | 56.7 ± 39.3 | 75 (25–100) | |
| p-value | 0.110 | 0.152 | 0.179 | 0.153 | |||||
| Current smoking | yes | 70 ± 31.2 | 85 (55–90) | 68.1 ± 35.9 | 83.3 (50–91.7) | 68.8 ± 34.7 | 81.3 (56.4–90.6) | 65.6 ± 37.7 | 75 (43.8–100) |
| no | 65.7 ± 32.1 | 80 (47.5–90) | 65.3 ± 34.4 | 77.8 (44.4–88.9) | 65.2 ± 34.5 | 75 (37.5–90.6) | 59.8 ± 39.5 | 75 (25–100) | |
| p-value | 0.806 | 0.837 | 0.829 | 0.745 | |||||
| Former or current smoking | yes | 63.1 ± 30.7 | 80 (40–90) | 62.8 ± 32.8 | 77.8 (44.4–88.9) | 62.9 ± 32.8 | 75 (37.5–87.5) | 55.2 ± 40.3 | 75 (25–100) |
| no | 68.9 ± 32.9 | 80 (50–100) | 67.9 ± 35.7 | 77.8 (55.6–100) | 67.9 ± 35.8 | 75 (56.3–100) | 65 ± 38 | 75 (37.5–100) | |
| p-value | 0.241 | 0.259 | 0.308 | 0.335 | |||||
| Death | yes | 51.2 ± 22.3 | 60 (55–60) | 50 ± 21.4 | 55.6 (52.8–58.3) | 51.6 ± 23.6 | 62.5 (46.9–62.5) | 40.6 ± 29.7 | 37.5 (25–50) |
| no | 68.4 ± 32.5 | 8 (47.5–90) | 67.9 ± 35.3 | 88.9 (44.4–100) | 67.6 ± 35.3 | 87.5 (37.5–100) | 63.4 ± 39.6 | 75 (25–100) | |
| p-value | 0.066 | 0.048 | 0.047 | 0.108 | |||||
| Need for oxygen therapy | yes | 58.9 ± 30.6 | 6 (47.5–80) | 58.3 ± 32.3 | 61.1 (52.8–80.6) | 58.9 ± 32.4 | 62.5 (46.9–78.1) | 49.1 ± 35.7 | 50 (18.8–75) |
| no | 71.9 ± 32 | 90 (47.5–100) | 71.3 ± 35.2 | 88.9 (44.4–100) | 70.8 ± 35.2 | 87.5 (37.5–100) | 69.4 ± 39.7 | 100 (25–100) | |
| p-value | 0.032 | 0.026 | 0.035 | 0.013 | |||||
| Need for ICU stay | yes | 68.3 ± 16 | 60 (60–67.5) | 66.7 ± 17.2 | 61.1 (55.6–66.7) | 68.8 ± 17.2 | 62.5 (62.5–71.9) | 58.3 ± 34.2 | 50 (31.3–87.5) |
| no | 66 ± 33.1 | 80 (40–90) | 65.5 ± 35.7 | 77.8 (44.4–88.9) | 65.3 ± 35.7 | 75 (37.5–96.9) | 60.8 ± 39.8 | 75 (25–100) | |
| p-value | 0.852 | 0.700 | 0.682 | 0.877 | |||||
| Variable | SDOIT | ||||
|---|---|---|---|---|---|
| 10-SDOIT | 9-SDOIT | 8-SDOIT | 4-SDOIT | ||
| Time interval between first positive PCR result and time of the survey, days | ρ | 0.19 | 0.18 | 0.19 | 0.1 |
| p-value | 0.123 | 0.163 | 0.141 | 0.447 | |
| Duration of hospitalisation (excluding deceased) | ρ | −0.43 | −0.42 | −0.41 | −0.36 |
| p-value | <0.001 | 0.002 | 0.002 | 0.007 | |
| MEWS score at the time of the survey | ρ | −0.29 | −0.32 | −0.32 | −0.25 |
| p-value | 0.02 | 0.011 | 0.011 | 0.043 | |
| Avarage MEWS score | ρ | −0.29 | −0.3 | −0.29 | −0.24 |
| p-value | 0.02 | 0.016 | 0.018 | 0.054 | |
| Characteristic | COVID-19 Patients (N = 64) | Control Patients (N = 34) | p-Value | |
|---|---|---|---|---|
| Reported smell at the time of maximum deterioration, N (%) | normosmia | 37 (57.8) | 34 (100) | <0.001 1 |
| hyposmia | 21 (32.8) | 0 (0) | ||
| anosmia | 6 (9.4) | 0 (0) | ||
| Reported smell at the time of the survey, N (%) | normosmia | 43 (67.2) | 34 (100) | <0.001 1 |
| hyposmia | 18 (28.1) | 0 (0) | ||
| anosmia | 3 (4.7) | 0 (0) | ||
| VAS score of smell deterioration (at the time of maximum deterioration) | mean ± SD | 3.4 ± 3.6 | 0 ± 0 | <0.001 2 |
| median (IQR) | 2 (0–7) | 0 (0–0) | ||
| VAS score of smell deterioration (at the time of the survey) | mean ± SD | 2.6 ± 3.2 | 0 ± 0 | <0.001 2 |
| median (IQR) | 2 (0–5) | 0 (0–0) | ||
| SDOIT—detected odors, N | mean ± SD | 7.5 ± 2.7 (83.5% ± 29.4%) | 9 ± 0 (100% ± 0%) | <0.001 2 |
| median (IQR) | 9 (7–9) (100% (77.8%–100%)) | 9 (9–9) (100% (100%–100%)) | ||
| 10-SDOIT, correct answers, N (%) | mean ± SD | 6.6 ± 3.2 (66.3% ± 31.8%) | 9.6 ± 0.8 (95.6% ± 8.2%) | <0.001 2 |
| median (IQR) | 8 (4.8–9) (80% (47.5%–90%)) | 10 (9–10) (100% (90%–100%)) | ||
| 9-SDOIT, correct answers, N (%) | mean ± SD | 5.9 ± 3.1 (65.6% ± 34.3%) | 8.6 ± 0.7 (95.8% ± 7.7%) | <0.001 2 |
| median (IQR) | 7 (4–8) (77.8% (44.4%–88.9%)) | 9 (8–9) (100% (88.9%–100%)) | ||
| 8-SDOIT, correct answers, N (%) | mean ± SD | 5.3 ± 2.7 (65.6 % ± 34.3%) | 7.8 ± 0.5 (97.1% ± 6.2%) | <0.001 2 |
| median (IQR) | 6 (3–7.3) (75% (37.5%–90.6%)) | 8 (8–8) (100% (100%–100%)) | ||
| 4-SDOIT, correct answers, N (%) | mean ± SD | 2.4 ± 1.6 (60.6% ± 39%) | 3.9 ± 0.2 (98.5% ± 6%) | <0.001 2 |
| median (IQR) | 3 (1–4) (75% (25%–100%)) | 4 (4–4) (100% (100%–100%)) | ||
| Characteristic | COVID-19 Patients (N = 48) | Control Patients (N = 34) | p-Value | |
|---|---|---|---|---|
| Reported smell at the time of maximum deterioration, N (%) | normosmia | 28 (58.3) | 34 (100) | <0.001 1 |
| hyposmia | 15 (31.2) | 0 (0) | ||
| anosmia | 5 (10.4) | 0 (0) | ||
| Reported smell at the time of the survey, N (%) | normosmia | 34 (70.8) | 34 (100) | <0.001 1 |
| hyposmia | 12 (25) | 0 (0) | ||
| anosmia | 2 (4.2) | 0 (0) | ||
| VAS score of smell deterioration (at the time of maximum deterioration) | mean ± SD | 3.4 ± 3.7 | 0 ± 0 | <0.001 2 |
| median [IQR] | 2 (0–7) | 0 (0–0) | ||
| VAS score of smell deterioration (at the time of the survey) | mean ± SD | 2.3 ± 3.1 | 0 ± 0 | <0.001 2 |
| median [IQR] | 0 (0–3) | 0 (0–0) | ||
| SDOIT-detected odors, N | mean ± SD | 7.7 ± 2.5 (85.4% ± 28.1%) | 9 ± 0 (100% ± 0%) | <0.001 2 |
| median (IQR) | 9 (8–9) (100% (88.9%–100%)) | 9 (9–9) (100% (100%–100%)) | ||
| 10-SDOIT, correct answers, N (%) | mean ± SD | 7.4 ± 3 (74.2% ± 29.5%) | 9.56 ± 0.82 (95.6% ± 8.2%) | <0.001 2 |
| median (IQR) | 9 (6–10) (90% (60%–100%)) | 10 (9–10) (100% (90%–100%) | ||
| 9-SDOIT, correct answers, N (%) | mean ± SD | 6.6 ± 2.93 (72.9% ± 32.6%) | 8.6 ± 0.7 (95.8% ± 7.7%) | <0.001 2 |
| median (IQR) | 8 (5.8–9) (88.9% (63.9%–100%)) | 9 (8–9) (100% (88.9%–100%)) | ||
| 8-SDOIT, correct answers, N (%) | mean ± SD | 5.8 ± 2.6 (72.7 % ± 32.6%) | 7.8 ± 0.5 (97.1% ± 6.2%) | <0.001 2 |
| median (IQR) | 7 (5–8) (87.5% (62.5%–100%)) | 8 (8–8) (100% (100%–100%)) | ||
| 4-SDOIT, correct answers, N (%) | mean ± SD | 2.8 ± 1.5 (69.8% ± 36.5%) | 3.9 ± 0.2 (98.5% ± 6%) | <0.001 2 |
| median (IQR) | 3 (2–4) (75% (50%–100%)) | 4 (4–4) (100% (100%–100%)) | ||
| SDOIT Score | Self-Reported Olfactory Function at the Time of the Survey (Normosmia/OD), N (%) | VAS Score (Maximum), N (%) | |||||
|---|---|---|---|---|---|---|---|
| Normosmia (N = 77) | OD (N = 21) | p-Value | <5 (N = 75) | ≥5 (N = 23) | p-Value | ||
| 10-SDOIT | 0–8 | 25 (32.5) | 16 (76.2) | <0.001 | 27 (36) | 27 (60.9) | 0.061 |
| 9–10 | 52 (67.5) | 5 (23.8) | 48 (64) | 9 (39.1) | |||
| 9-SDOIT | 0–7 | 22 (28.6) | 15 (71.4) | <0.001 | 24 (32) | 13 (56.5) | 0.049 |
| 8–9 | 55 (71.4) | 6 (28.6) | 51 (68) | 10 (43.5) | |||
| 8-SDOIT | 0–6 | 6 (7.8) | 11 (52.4) | <0.001 | 7 (9.3) | 10 (43.5) | <0.001 |
| 7–8 | 71 (92.2) | 10 (47.6) | 68 (90.7) | 13 (56.5) | |||
| 4-SDOIT | 0–3 | 26 (33.8) | 17 (81) | <0.001 | 26 (34.7) | 17 (73.9) | 0.002 |
| 4 | 51 (66.2) | 4 (19) | 49 (65.3) | 6 (26.1) | |||
| Classifier | Sensitivity | Specifity | PPV | NPV | AUC |
|---|---|---|---|---|---|
| Self-reported OD at the time maximum deterioration | 0.42 (CI95% 0.3–0.55) | 1 (CI95% 1–1) | 1 (CI95% 1–1) | 0.48 (CI95% 0.43–0.54 | 0.71 (CI95% 0.65–0.77) |
| Maximum VAS | 0.64 (CI95% 0.53–0.75) | 1 (CI95% 1–1) | 1 (CI95% 1–1) | 0.6 (CI95% 0.53–0.68) | 0.82 (CI95% 0.76–0.88) |
| 10-SDOIT (OD ≥ 1 incorrect) | 0.8 (CI95% 0.56–0.78) | 0.71 (CI95% 0.62–0.76) | 0.84 (CI95% 0.79–0.86) | 0.65 (CI95% 0.52–0.77) | 0.82 (CI95% 0.74–0.9) |
| 10-SDOIT (OD ≥ 1 incorrect 0-9/10) + self-reported OD | 0.91 (CI95% 0.83-0.97) | 0.71 (CI95% 0.56–0.85) | 0.85 (CI95% 0.79–0.92) | 0.8 (CI95% 0.67–0.93) | 0.87 (CI95% 0.8–0.93) |
| 10-SDOIT (OD 0-8/10) + self-reported OD | 0.77 (CI95% 0.66–0.86) | 0.91 (CI95% 0.82–1) | 0.94 (CI95% 0.88–1) | 0.67 (CI95% 0.58–0.78) | 0.86 (CI95% 0.80–0.92) |
| 9-SDOIT (OD ≥ 1 incorrect) | 0.77 (CI95% 0.55–0.86) | 0.71 (CI95% 0.59–0.97) | 0.83 (CI95% 0.77–0.97) | 0.62 (CI95% 0.5–0.74) | 0.80 (CI95% 0.73–0.88) |
| 9-SDOIT (OD ≥ 1 incorrect 0-8/9) + self-reported OD | 0.88 (CI95% 0.83–0.97) | 0.71 (CI95% 0.56–0.85) | 0.85 (CI955 0.79–0.92) | 0.75 (CI95% 0.68–0.93) | 0.85 (CI95% 0.79–0.92) |
| 9-SDOIT (OD 0-7/9) + self-reported OD | 0.73 (CI95% 0.83–0.97) | 0.94 (CI95% 0.56–0.85) | 0.96 (CI95% 0.79–0.92) | 0.65 (CI95% 0.67–0.93) | 0.85 (CI95% 0.79–0.91) |
| 8-SDOIT (OD ≥ 1 incorrect) | 0.75 (CI95% 0.61–0.86) | 0.79 (CI95% 0.68–0.94) | 0.87 (CI95% 0.81–0.96) | 0.63 (CI95% 0.53–0.74) | 0.82 (CI95% 0.75–0.89) |
| 8-SDOIT (OD ≥ 1 incorrect 0-7/8) + self-reported OD | 0.86 (CI95% 0.77–0.94) | 0.79 (CI95% 0.65–0.91) | 0.89 (CI95% 0.82–0.95) | 0.75 (CI95% 0.64–0.88) | 0.87 (CI95% 0.81–0.93) |
| 8-SDOIT (OD 0-6/8) + self-reported OD | 0.73 (CI95% 0.62–0.84) | 0.97 (CI95% 0.91–1) | 0.98 (CI95% 0.93–1) | 0.66 (CI95% 0.58–0.76) | 0.86 (CI95% 0.8–0.92) |
| 4-SDOIT (OD ≥ 1 incorrect) | 0.64 (CI95% 0.53–0.75) | 0.94 (CI95% 0.85–1) | 0.95 (CI95% 0.89–1) | 0.58 (CI95% 0.51–0.67) | 0.80 (CI95% 0.74–0.87) |
| 4-SDOIT (OD ≥ 1 incorrect) + self-reported OD | 0.78 (CI95% 0.67–0.88) | 0.94 (C I95% 0.85–1) | 0.96 (CI95% 0.91–1) | 0.7 (CI95% 0.6–0.8) | 0.87 (CI95% 0.82–0.93) |
| Classifier | Sensitivity | Specifity | PPV | NPV | AUC |
|---|---|---|---|---|---|
| Self-reported OD at the time of the maximum deterioration | 0.42 (CI95% 0.29–0.56) | 1 (CI95% 1–1) | 1 (CI95% 1–1) | 0.55 (CI95% 0.5–0.62) | 0.71 (CI95% 0.64–0.78) |
| Maximum VAS | 0.35 (CI95% 0.21–0.5) | 1 (CI95% 1–1) | 1 (CI95% 1–1) | 0.52 (CI95% 0.47–0.59) | 0.68 (CI95% 0.61–0.75) |
| 10-SDOIT (OD ≥ 1 incorrect) | 0.73 (CI95% 0.56–0.83) | 0.71 (CI95% 0.56–0.91) | 0.78 (CI95% 0.7–0.9) | 0.65 (CI95% 0.54–0.76) | 0.76 (CI95% 0.67–0.86) |
| 10-SDOIT (OD ≥ 1 incorrect 0-9/10) + self-reported OD | 0.88 (CI95% 0.77–0.96) | 0.71 (CI95% 0.56–0.85) | 0.81 (CI95% 0.73–0.9) | 0.8 (CI95% 0.67–0.93) | 0.85 (CI95% 0.78–0.92) |
| 10-SDOIT (OD 0-8/10) + self-reported OD | 0.71 (CI95% 0.58–0.83) | 0.91 (CI95% 0.79–1) | 0.92 (CI95% 0.83–1) | 0.69 (CI95% 0.6– 0.79) | 0.83 (CI95% 0.75–0.9) |
| 9-SDOIT (OD ≥ 1 incorrect) | 0.71 (CI95% 0.54–0.83) | 0.71 (CI95% 0.56–0.91) | 0.77 (CI95% 0.69–0.9) | 0.63 (CI95% 0.53–0.75) | 0.76 (CI95% 0.66–0.85) |
| 9-SDOIT (OD ≥ 1 incorrect 0-8/9) + self-reported OD | 0.85 (CI95% 0.75–0.96) | 0.71 (CI95% 0.56–0.85) | 0.8 (CI955 0.72–0.9) | 0.77 (CI95% 0.66–0.91) | 0.84 (CI95% 0.77–0.92) |
| 9-SDOIT (OD 0-7/9) + self-reported OD | 0.69 (CI95% 0.54–0.81) | 0.94 (CI95% 0.85–1) | 0.94 (CI95% 0.86–1) | 0.68 (CI95% 0.59–0.78) | 0.83 (CI95% 0.75–0.9) |
| 8-SDOIT (OD ≥ 1 incorrect) | 0.69 (CI95% 0.54–0.81) | 0.79 (CI95% 0.65–0.91) | 0.82 (CI95% 0.73–0.92) | 0.64 (CI95% 0.55–0.76) | 0.78 (CI95% 0.69–0.87) |
| 8-SDOIT (OD ≥ 1 incorrect 0-7/8) + self-reported OD | 0.83 (CI95% 0.73–0.94) | 0.79 (CI95% 0.65–0.91) | 0.85 (CI95% 0.76–0.93) | 0.77 (CI95% 0.66–0.9) | 0.86 (CI95% 0.78–0.93) |
| 8-SDOIT (OD 0-6/8) + self-reported OD | 0.69 (CI95% 0.54–0.81) | 0.97 (CI95% 0.91–1) | 0.97 (CI95% 0.9–1) | 0.69 (CI95% 0.6–0.79) | 0.84 (CI95% 0.77–0.9) |
| 4-SDOIT (OD ≥ 1 incorrect) | 0.54 (CI95% 0.4–0.69) | 0.94 (CI95% 0.85–1) | 0.93 (CI95% 0.83–1) | 0.59 (CI95% 0.52–0.69) | 0.75 (CI95% 0.67–0.83) |
| 4-SDOIT (OD ≥ 1 incorrect) + self-reported OD | 0.73 (CI95% 0.6–0.85) | 0.94 (C I95% 0.85–1) | 0.95 (CI95% 0.87–1) | 0.71 (CI95% 0.62–0.82) | 0.85 (CI95% 0.78–0.92) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ziuzia-Januszewska, L.; Dobrzyński, P.; Ślączka, K.; Ciszek, J.; Krawiec, Ł.; Wierzba, W.; Zaczyński, A. Simple Disposable Odor Identification Tests for Predicting SARS-CoV-2 Positivity. Int. J. Environ. Res. Public Health 2021, 18, 10185. https://doi.org/10.3390/ijerph181910185
Ziuzia-Januszewska L, Dobrzyński P, Ślączka K, Ciszek J, Krawiec Ł, Wierzba W, Zaczyński A. Simple Disposable Odor Identification Tests for Predicting SARS-CoV-2 Positivity. International Journal of Environmental Research and Public Health. 2021; 18(19):10185. https://doi.org/10.3390/ijerph181910185
Chicago/Turabian StyleZiuzia-Januszewska, Laura, Paweł Dobrzyński, Krzysztof Ślączka, Jaromir Ciszek, Łukasz Krawiec, Waldemar Wierzba, and Artur Zaczyński. 2021. "Simple Disposable Odor Identification Tests for Predicting SARS-CoV-2 Positivity" International Journal of Environmental Research and Public Health 18, no. 19: 10185. https://doi.org/10.3390/ijerph181910185