
Effect of Online Training during the COVID-19 Quarantine on the Aerobic Capacity of Youth Soccer Players


Abstract
:1. Introduction
2. Material and Methods
2.1. Participants
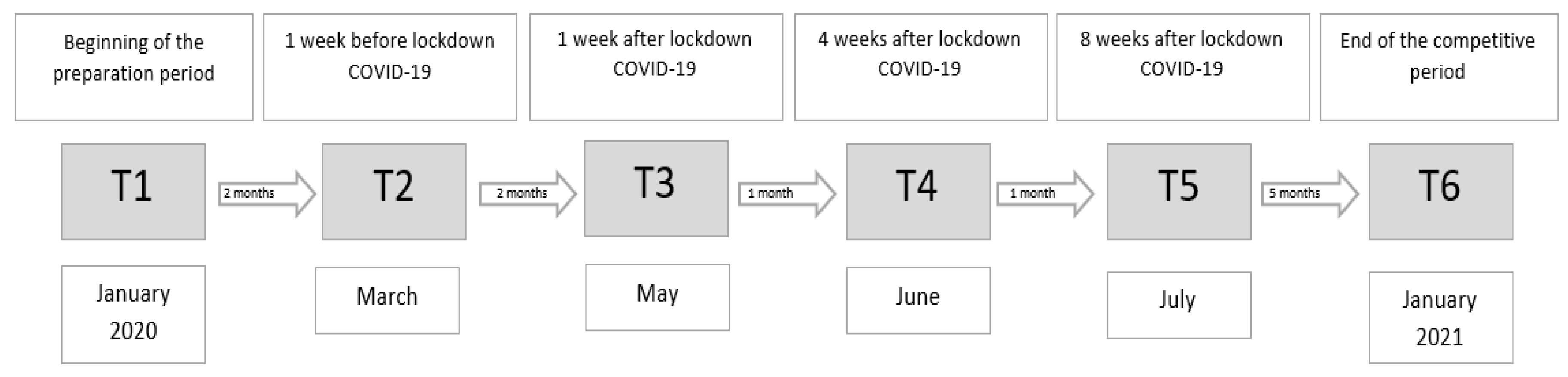
2.2. Experimental Approach to the Problem/Procedures/Design
2.3. Description of the Training Intervention
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Practical Implications
4.2. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 11 March 2020).
- Sarto, F.; Impellizzeri, F.M.; Spörri, J.; Porcelli, S.; Olmo, J.; Requena, B.; Franchi, M.V. Impact of potential physiological changes due to COVID-19 home confinement on athlete health protection in elite sports: A call for awareness in sports programming. Sports Med. 2020, 50, 1417–1419. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Calderón, B. The Effect of Short-Term and Long-Term Coronavirus Quarantine on Physical Performance and Injury Incidence in High-Level Soccer. Soccer Soc. 2020, 22, 85–95. [Google Scholar] [CrossRef]
- Kalinowski, P. Konsekwencje niepowodzeń w piłce nożnej. Asystent Trenera 2020, 40, 58–60. [Google Scholar]
- Fuentes-García, J.P.; Martínez Patiño, M.J.; Villafaina, S.; Clemente-Suárez, V. The Effect of COVID-19 confinement in behavioral, psychological, and training patterns of chess players. Front. Psychol. 2020, 11, 1812. [Google Scholar] [CrossRef] [PubMed]
- Aziz, A.R.; Mukherjee, S.; Chia, M.Y.; Teh, K.C. Relationship between measured maximal oxygen uptake and aerobic endurance performance with running repeated sprint ability in young elite soccer players. J. Sports Med. Phys. Fit. 2007, 47, 401–407. [Google Scholar]
- Castagna, C.; Francini, L.; Povoas, S.C.A.; D’Ottavio, S. Long-sprint abilities in soccer: Ball versus running drills. Int. J. Sports Physiol. Perform. 2017, 12, 1256–1263. [Google Scholar] [CrossRef]
- Slimani, M.; Nikolaidis, P.T. Anthropometric and physiological characteristics of male soccer players according to their competitive level, playing position and age group: A systematic review. J. Sports Med. Phys. Fit. 2019, 59, 141–163. [Google Scholar] [CrossRef]
- Orntoft, C.; Fuller, C.W.; Larsen, M.N.; Bangsbo, J.; Dvorak, J.; Krustrup, P. FIFA 11 for health’ for Europe. II: Effect on health markers and physical fitness in Danish schoolchildren aged 10-12 years. Br. J. Sports Med. 2016, 50, 1394–1399. [Google Scholar] [CrossRef] [Green Version]
- Michailidis, Y.; Chatzimagioglou, A.; Mikikis, D.; Ispirlidis, I.; Metaxas, T. Maximal oxygen consumption and oxygen muscle saturation recovery following repeated anaerobic sprint test in youth soccer players. J. Sports Med. Phys. Fit. 2020, 60, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Reilly, T.; Williams, A.M.; Nevill, A.; Franks, A. A mulitidisciplinary approach to talent identification in soccer. J. Sports Sci. 2000, 18, 695–702. [Google Scholar] [CrossRef]
- Billat, V.L.; Sirvent, P.; Py, G.; Koralsztein, J.P.; Mercier, J. The concept of maximal lactate steady state: A bridge between biochemistry, physiology and sport science. Sports Med. 2003, 33, 407–426. [Google Scholar] [CrossRef]
- European Communities. Handbook for the EUROFIT Tests and Physical Fitness, 2nd ed.; Sports Division Strasbourg, Council of Europe Publishing and Documentation Service: Strasbourg, France, 1993. [Google Scholar]
- Aziz, A.R.; Chia, M.; Singh, R.; Wahid, M.F. Effects of Ramadan Fasting on Perceived Exercise Intensity during High-Intensity Interval Training in Elite Youth Soccer Players. Int. J. Sports Sci. Coach. 2011, 6, 87–98. [Google Scholar] [CrossRef]
- Petrucci, M.; Petrigna, L.; Pomara, F.; Piccione, M.C.; Alesi, M.; Bianco, A. Validation in Young Soccer Players of the Modified Version of the Harre Circuit Test: The Petrucci Ability Test. Monten. J. Sports Sci. Med. 2021, 10, 67–71. [Google Scholar] [CrossRef]
- Mayorga Verga, D.; Aguilar-Soto, P.; Viciana, J. Criterion-Related Validity of the 20-M Shuttle Run Test for Estimating Cardiorespiratory Fitness: A Meta-Analysis. J. Sports Sci. Med. 2015, 14, 536–547. [Google Scholar]
- Beato, M.; Coratella, G.; Bianchi, M.; Costa, E.; Merlini, M. Short-term repeated-sprint training (straight sprint vs. changes of direction) in soccer players. J. Hum. Kinet. 2019, 70, 183–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo, D.; Camara, J.; Lozano, D.; Berzosa, C.; Yanci, J. The association between physical performance and match-play activities of field and assistants soccer referees. Res. Sports Med. 2019, 27, 283–297. [Google Scholar] [CrossRef] [PubMed]
- Christou, M.; Smilios, I.; Sotiropoulos, K.; Volaklis, K.; Pilianidis, T.; Tokmakidis, S.P. Effects of resistance training on the physical capacities of adolescent soccer players. J. Strength Cond. Res. 2006, 20, 783–791. [Google Scholar]
- Joo, C.H. The effects of short-term detraining on exercise performance in soccer players. J. Exerc. Rehabil. 2016, 12, 54–59. [Google Scholar] [CrossRef]
- Rodríguez-Fernández, A.; Sánchez-Sánchez, J.; Ramirez-Campillo, R.; Rodríguez-Marroyo, J.A.; Villa Vicente, J.G.; Nakamura, F.Y. Effects of short-term in-season break detraining on repeated-sprint ability and intermittent endurance according to initial performance of soccer player. PLoS ONE 2018, 13, e0201111. [Google Scholar] [CrossRef] [Green Version]
- Kovacs, M.S.; Pritchett, R.; Wickwire, P.J.; Green, J.M.; Bishop, P. Physical performance changes after unsupervised training during the autumn/spring semester break in competitive tennis players. Br. J. Sports Med. 2007, 41, 705–710. [Google Scholar] [CrossRef]
- Madsen, K.; Pedersen, P.K.; Djurhuus, M.S.; Klitgaard, N.A. Effects of detraining on endurance capacity and metabolic changes during prolonged exhaustive exercise. J. Appl. Physiol. 1993, 75, 1444–1451. [Google Scholar] [CrossRef]
- Korkmaz, S.; Aslan, C.S.; Eyuboğlu, E.; Çelebi, M.; Kır, R.; Karakulak, I.; Akyüz, Ö.; Özer, U.; Geri, S. Impact of detraining process experienced during the COVID-19 pandemic on the selected physical and motor features of football players. Prog. Nutr. 2020, 22, e2020029. [Google Scholar]
- Fardy, P.S. Effects of soccer training and detraining upon selected cardiac and metabolic measures. Res. Q. 1969, 40, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Drinkwater, B.L.; Horvath, S.M. Detraining effects on young women. Med. Sci. Sports 1972, 4, 91–95. [Google Scholar] [CrossRef]
- Coyle, E.F.; Martin, W.H., 3rd; Bloomfield, S.A.; Lowry, O.H.; Holloszy, J.O. Effects of detraining on responses to submaximal exercise. J. Appl. Physiol. 1985, 59, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Al’Hazzaa, H.M.; Almuzaini, K.S.; Al-Refaee, S.A.; Sulaiman, M.A.; Dafterdar, M.Y.; Al-Ghamedi, A.; Al-Khuraiji, K.N. Aerobic and anaerobic power characteristics of Saudi elite soccer players. J. Sports Med. Phys. Fit. 2001, 41, 54–61. [Google Scholar]
- Rodríguez-Fernández, A.; Sanchez-Sanchez, J.; Ramirez-Campillo, R.; Nakamura, F.Y.; Rodríguez-Marroyo, J.A.; Villa-Vicente, J.G. Relationship Between Repeated Sprint Ability, Aerobic Capacity, Intermittent Endurance, and Heart Rate Recovery in Youth Soccer Players. J. Strength Cond. Res. 2019, 33, 3406–3413. [Google Scholar] [CrossRef]
- Mujika, I.; Padilla, S. Detraining: Loss of Training-Induced Physiological and Performance Adaptations. Part II- Long Term Insufficient Training Stimulus. Sports Med. 2000, 30, 145–154. [Google Scholar] [CrossRef]
- Issurin, V. Block periodization versus traditional training theory: A review. J. Sports Med. Phys. Fit. 2008, 48, 65–75. [Google Scholar]
- Albuquerque Freire, L.; Tannure, M.; Sampaio, M.; Slimani, M.; Znazen, H.; Bragazzi, N.L.; Aedo-Muñoz, E.; Sobarzo Soto, D.A.; Brito CJMiarka, B. COVID-19-Related Restrictions and Quarantine COVID-19: Effects on Cardiovascular and Yo-Yo Test Performance in Professional Soccer Players. Front. Psychol. 2020, 11, 589543. [Google Scholar] [CrossRef]
- Bogdanis, G.C.; Nevill, M.E.; Boobis, L.H.; Lakomy, H.K. Contribution of phosphocreatine and aerobic metabolism to energy supply during repeated sprint exercise. J. Appl. Physiol. 1996, 80, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Jeffreys, I. Warm-up revisited: The ramp method of optimizing warm-ups. Prof. Strength Cond. 2007, 6, 12–18. [Google Scholar]
- Mccubbine, J.; Turner, A.; Dos Santos, T.; Bishop, C. Reliability and measurement of inter-limb asymmetries in four unilateral jump tests in elite youth female soccer players. Prof. Strength Cond. J. 2018, 49, 7–12. [Google Scholar]
- Borg, G. An Introduction to Borg’s RPE-Scale; Movement Publications: Ithaca, NY, USA, 1985. [Google Scholar]
- Bucheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle. Part II: Anaerobic energy, neuromuscular load and practical applications. Sports Med. 2013, 43, 927–954. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.; Florhaug, J.A.; Franklin, J.; Gottschall, L.; Hrovatin, L.A.; Parker, S. A new approach to monitoring exercise training. J. Strength Cond. Res. 2001, 15, 109–115. [Google Scholar] [PubMed]
- Billat, L.V. Interval Training for Performance: A Scientific and Empirical Practice. Sports Med. 2001, 31, 13–31. [Google Scholar] [CrossRef]
- McArdle, W.D.; Katch, F.I.; Katch, V.L. Exercise Physiology: Nutrition, Energy, and Human Performance; Wolters Kluwer Health, Lippincot Wiliams and Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Minium, B.M.; King, E.W. Statistical Reasoning in Psychology and Education; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2003. [Google Scholar]
- Fallon, K. Exercise in the time of COVID-19. Aust. J. Gen. Pract. 2020, 22, 49. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Pavon, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020, 63, 386–388. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour. Available online: https://www.who.int/publications/i/item/9789240015128 (accessed on 25 November 2020).
- Saward, C.; Hulse, M.; Morris, J.G.; Goto, H.; Sunderland, C.; Nevill, M.E. Longitudinal Physical Development of Future Professional Male Soccer Players: Implications for Talent Identification and Development? Front. Sports Act. Living 2020, 2, 578203. [Google Scholar] [CrossRef]
- Bangsbo, J. Sprawność Fizyczna Piłkarza; Centralny Ośrodek Sportu: Warszawa, Poland, 1999. [Google Scholar]
- Śliwowski, R.; Jóźwiak, J.; Pietrzak, M.; Wieczorek, A.; Wieczorek, J. Aerobic performance of young soccer players in the preparatory period. Stud. Phys. Cult. Tour. 2007, 14, 293–297. [Google Scholar]
- Chtourou, H.; Hammouda, O.; Souissi, H.; Chamari, K.; Chaouachi, A.; Souissi, N. The effect of ramadan fasting on physical performances, mood state and perceived exertion in young footballers. Asian J. Sports Med. 2011, 2, 177–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, P.; Duffield, R.; Vaile, J. Effects of simulated domestic and international air travel on sleep, performance, and recovery for team sports. Scand. J. Med. Sci. Sports 2015, 25, 441–451. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Week | Number of Training Sessions per Week | Duration of a Training Session | Aim | Training Measures | Methods of Control |
|---|---|---|---|---|---|
| 1–3 | 4/week | 60 min | Stability/ROM Low intensity | Individual training | Video analysis, RPE |
| 4 | 5/week | 60 min | Stability/ROM Low intensity | Individual training | Video analysis, RPE |
| 5–6 | 6/week | 60–75 min | Stability/aerobic endurance High intensity | Running/individual training | Distance, time, map, RPE |
| 7–8 | 6/week | 60–75 min | Stability/aerobic endurance High intensity | Running/individual training | Distance, time, map, RPE |
| Part of the Training Unit | Exercises/Goal/Execution (Volume) |
|---|---|
| Warm-up (15min) | Running in place (2′) Raising knees (12 rep) Forward shoulder circulation (20″) Back arm circulation (20″) Core activation (2 exercises) Glute activation (2 × 12 rep each leg) Ground mobility (3 exercises) Dynamic stretching (12 rep × 7 exercises) A-skip (10″) Butt kicks (10″) Running rhythm in place (10″) |
| Main Part (35 min) | Balance and coordination exercises (2 ex.) Lower body pull exercises—hip and knee dominant (2 ex.) Upper body push and pull exercises (2 ex.) Hip abductor and adductor exercises (2 ex.) Core stability—lumbo-pelvic control |
| Cool Down (10min) | Foam rolling (10′) |
| Part of the Training Unit | Exercises/Goal/Execution (Volume) |
|---|---|
| Warm-up (15 min) | Running in place (2′) Raising knees (12 rep) Cross step (interlace) (12 rep) Forward shoulder circulation (30″) Back arm circulation (30″) Core activation (2 exercises) Glute activation with a mini band (2 × 12 rep each side) Ground mobility (3 exercises) Dynamic stretching (12 rep × 7 exercises) A-skip (10″) Butt kicks (10″) Running rhythm in place (10″) |
| Main Part (45 min) | Core stability—lumbo-pelvic control (3 ex.) Exercises with bands, global patterns (2 ex.) Balance and coordination exercises (2 ex.) Running in place <14 RPE: Running in place/Jump rope skipping (5 × 2 min of work, 1.5 min (passive) break RPE 15–18) |
| Cool Down (10 min) | Foam rolling (10′) |
| Measurements | Mean Cardiorespiratory Endurance among the Six Time Periods | ||||||
|---|---|---|---|---|---|---|---|
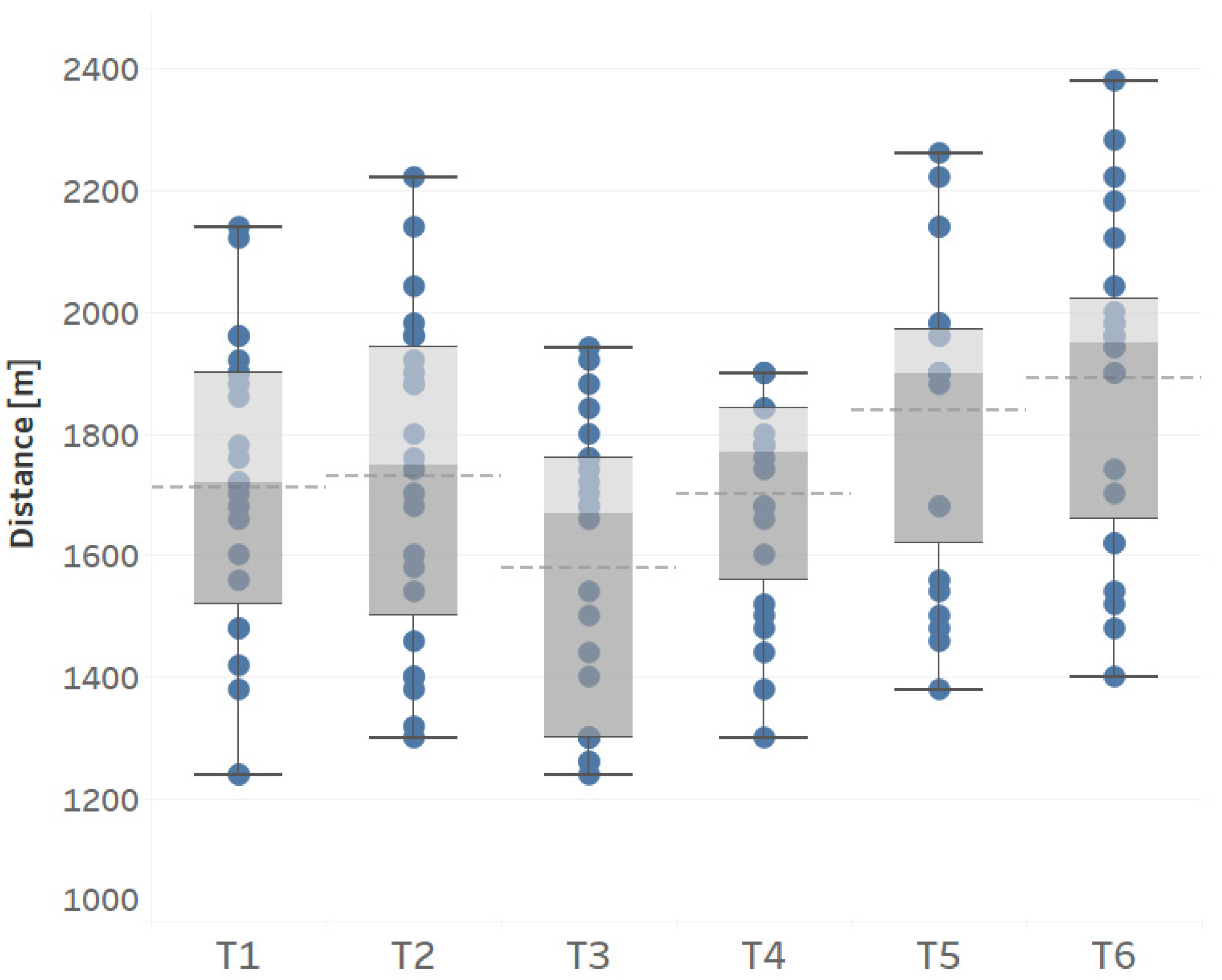
| Months | T 1 M = 1710.8 (m) ±294.52 (m) | T 2 M = 1730.8 (m) ±266.50 (m) | T 3 M = 1580.0 (m) ±237.38 (m) | T 4 M = 1701.7 (m) ±179.75 (m) | T 5 M = 1837.5 (m) ±248.14 (m) | T 6 M = 1890.0 (m) ±262.16 (m) | |
| T 1 | January 2020 | - | - | - | - | - | |
| T 2 | March 2020 | p > 0.05 | - | - | - | - | |
| T 3 | May 2020 | p< 0.01 | p< 0.001 | - | - | ||
| T 4 | June 2020 | p > 0.05 | p > 0.05 | p< 0.01 | - | - | |
| T 5 | July 2020 | p< 0.01 | p< 0.05 | p< 0.001 | p< 0.001 | - | |
| T 6 | January 2021 | p< 0.001 | p< 0.001 | p< 0.001 | p< 0.001 | p > 0.05 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalinowski, P.; Myszkowski, J.; Marynowicz, J. Effect of Online Training during the COVID-19 Quarantine on the Aerobic Capacity of Youth Soccer Players. Int. J. Environ. Res. Public Health 2021, 18, 6195. https://doi.org/10.3390/ijerph18126195
Kalinowski P, Myszkowski J, Marynowicz J. Effect of Online Training during the COVID-19 Quarantine on the Aerobic Capacity of Youth Soccer Players. International Journal of Environmental Research and Public Health. 2021; 18(12):6195. https://doi.org/10.3390/ijerph18126195
Chicago/Turabian StyleKalinowski, Paweł, Jakub Myszkowski, and Jakub Marynowicz. 2021. "Effect of Online Training during the COVID-19 Quarantine on the Aerobic Capacity of Youth Soccer Players" International Journal of Environmental Research and Public Health 18, no. 12: 6195. https://doi.org/10.3390/ijerph18126195