
COVID-19 Quarantine Dramatically Affected Male Sexual Behavior: Is There a Possibility to Go Back to Normality?

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Sexual Function Questionnaires
2.3. Data Analysis
3. Results
3.1. Study Population
3.2. Ten- and Six-Item Questionnaires
3.3. Sexual Distress Schedule
3.4. International Index of Erectile Function Questionnaire
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Han, E.; Tan, M.M.J.; Turk, E.; Sridhar, D.; Leung, G.M.; Shibuya, K.; Asgari, N.; Oh, J.; García-Basteiro, A.L.; Hanefeld, J.; et al. Lessons learnt from easing COVID-19 restrictions: An analysis of countries and regions in Asia Pacific and Europe. Lancet 2020, 396, 1525–1534. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Vaughan, A. Omicron emerges. New Sci. 2021, 252, 7. [Google Scholar] [CrossRef]
- Li, D.; Jin, M.; Bao, P.; Zhao, W.; Zhang, S. Clinical characteristics and results of semen tests among men with coronavirus disease 2019. JAMA Netw. Open 2020, 3, e208292. [Google Scholar] [CrossRef] [PubMed]
- Spirito, L.; Pinchera, B.; Patrì, A.; Delfino, M.; Imbimbo, C.; Salvatore, P.; Gentile, I.; Fabbrocini, G. No Detection of SARS-CoV-2 RNA on Urethral Swab in Patients with Positive Nasopharyngeal Swab. Adv. Virol. 2020, 2020, 8826943. [Google Scholar] [CrossRef] [PubMed]
- Omolaoye, T.S.; Adeniji, A.A.; Maya, W.D.C.; du Plessis, S.S. SARS-CoV-2 (COVID-19) and male fertility: Where are we? Reprod. Toxicol. 2021, 99, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Rosen, R.C.; Riley, A.; Wagner, G.; Osterloh, I.H.; Kirkpatrick, J.; Mishra, A. The international index of erectile function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology 1997, 49, 822–830. [Google Scholar] [CrossRef] [Green Version]
- Santos-Iglesias, P.; Mohamed, B.; Danko, A.; Walker, L.M. Psychometric Validation of the Female Sexual Distress Scale in Male Samples. Arch. Sex. Behav. 2018, 47, 1733–1743. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Li, G.; Xin, C.; Wang, Y.; Yang, S. Challenges in the Practice of Sexual Medicine in the Time of COVID-19 in China. J. Sex. Med. 2020, 17, 1225–1228. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, B.; Ozgor, F. Effect of the COVID-19 pandemic on female sexual behavior. Int. J. Gynecol. Obstet. 2020, 150, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Jannini, E.A. SM = SM: The Interface of Systems Medicine and Sexual Medicine for Facing Non-Communicable Diseases in a Gender-Dependent Manner. Sex. Med. Rev. 2017, 5, 349–364. [Google Scholar] [CrossRef] [PubMed]
- Padmanabhan, P.; McCullough, A.R. Penile Oxygen Saturation in the Flaccid and Erect Penis in Men with and without Erectile Dysfunction. J. Androl. 2006, 28, 223–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda, E.P.; Nascimento, B.; Torres, L.O.; Glina, S. Challenges in the Practice of Sexual Medicine in the Time of COVID-19 in Brazil. J. Sex. Med. 2020, 17, 1222–1224. [Google Scholar] [CrossRef] [PubMed]
- Aversa, A.; A Jannini, E. COVID-19, or the triumph of monogamy? Minerva Endocrinol. 2020, 45, 77–78. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Tian, J.; He, S.; Zhu, C.; Wang, J.; Liu, C.; Yang, J. Possible Vertical Transmission of SARS-CoV-2 from an Infected Mother to Her Newborn. JAMA 2020, 323, 1846–1848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenberg, M.L. Coronavirus Disease 2019 (COVID-19) and men’s reproductive health. Fertil. Steril. 2020, 113, 1154. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Overall Population | 22 (100) | |
|---|---|---|
| Age (years) | Median (IQR) | 63 (58.2–67) |
| Gender n (%) | Male | 22 (100) |
| Female | 0 (0) | |
| BMI (Kg/m2) | <25 | 9 (40.9) |
| 25–30 | 11 (50.0) | |
| ≥30 | 2 (9.1) | |
| Smoking (sig/day), n (%) | 0 | 10 (45.5) |
| 5 | 1 (4.5) | |
| 10 | 6 (27.3) | |
| 20 | 5 (22.7) | |
| CCS | Median (IQR) | 3 (1–4) |
| No Children, n (%) | 0 | 2 (9.1) |
| 1 | 17 (77.3) | |
| 2 | 3 (13.6) | |
| Educational level, n (%) | Degree | 8 (36.4) |
| Primary school | 4 (18.2) | |
| Secondary school | 10 (45.5) | |
| Working Status, n (%) | Employed | 10 (45.5) |
| Retired | 4 (18.2) | |
| Self-employment | 6 (27.3) | |
| Unemployed | 2 (9.1) | |
| Working from home, n (%) | No | 21 (95.5) |
| Yes | 1 (4.5) | |
| ICU, n (%) | No | 13 (59.1) |
| Yes | 9 (40.9) | |
| LOS (days) | Mean | 11.22 (4.15) |
| Median (IQR) | 10 (8–13) | |
| Housemates COVID-19 positive | No | 17 (77.3) |
| Yes | 5 (22.7) |
| Questions | Answers | Time 1 | Time 2 | Time 3 |
|---|---|---|---|---|
| (1) Did you have complete sexual intercourse (vaginal) during this time? | No | 1 (4.5) | 17 (77.3) | 6 (27.3) |
| Yes | 21 (95.5) | 5 (22.7) | 16 (72.7) | |
| (2) How often did you have sexual intercourse? | Never | 1 (4.5) | 16 (72.7) | 6 (27.3) |
| Less than once per month | 2 (9.1) | 1 (4.5) | 5 (22.7) | |
| Once a month | 6 (27.3) | 2 (9.1) | 6 (27.3) | |
| More than once a month | 8 (36.4) | 3 (13.6) | 4 (18.2) | |
| More than once a week | 5 (22.7) | 0 (0) | 1 (4.5) | |
| Once a day | 0 (0) | 0 (0) | 0 (0) | |
| More than one a day | 0 (0) | 0 (0) | 0 (0) | |
| (3) How often did you masturbate? | Never | 11 (50.0) | 14 (63.6) | 9 (40.9) |
| Less than once per month | 7 (31.8) | 2 (9.1) | 10 (45.5) | |
| Once a month | 4 (18.2) | 0 (0) | 3 (13.6) | |
| More than once a month | 0 (0) | 6 (27.3) | 0 (0) | |
| More than once a week | 0 (0) | 0 (0) | 0 (0) | |
| Once a day | 0 (0) | 0 (0) | 0 (0) | |
| More than one a day | 0 (0) | 0 (0) | 0 (0) | |
| (4) How often did you watch porn? | Never | 14 (63.6) | 18 (81.8) | 14 (63.6) |
| Less than once per month | 6 (27.3) | 1 (4.5) | 8 (36.4) | |
| Once a month | 2 (9.1) | 0 (0) | 0 (0) | |
| More than once a month | 0 (0) | 3 (13.6) | 0 (0) | |
| More than once a week | 0 (0) | 0 (0) | 0 (0) | |
| Once a day | 0 (0) | 0 (0) | 0 (0) | |
| More than one a day | 0 (0) | 0 (0) | 0 (0) | |
| (5) Were you having sexual difficulties? | No | 0 (0) | 0 (0) | 0 (0) |
| Yes | 22 (100) | 22 (100) | 22 (100) | |
| (6) If Yes, have you ever had such difficulties? | No | 0 (0) | 0 (0) | 0 (0) |
| Yes | 22 (100) | 22 (100) | 22 (100) | |
| (7) Did you attend a clinic for your difficulties? | No | 20 (90.9) | 22 (100) | 22 (100) |
| Yes | 2 (9.1) | 0 (0) | 0 (0) |
| Questions | 22 (100%) | |
|---|---|---|
| 1. Could you easily self-isolate? | No | 14 (63.6) |
| Yes | 8 (36.4) | |
| 2. Are you worried at the moment for yourself? | No | 13 (59.1) |
| Slightly worried | 6 (27.3) | |
| Moderately worried | 3 (13.6) | |
| Very worried | 0 (0) | |
| 3. Are you worried at the moment for your relatives? | No | 5(22.7) |
| Slightly worried | 4 (18.2) | |
| Moderately worried | 12 (54.5) | |
| Very worried | 1 (4.5) | |
| 4. Have you followed the quarantine protocols? | Completely | 22 (100) |
| 5. Did it impact on your physical health? | Not at all | 1 (4.5) |
| Not very much | 6 (27.3) | |
| Very much | 7 (31.8) | |
| Completely | 8 (36.4) | |
| 6. Did it impact on your mental health? | Not at all | 1 (4.5) |
| Not very much | 7 (31.8) | |
| Very much | 10 (45.5) | |
| Completely | 4 (18.2) | |
| 7. Did the COVID-19 emergency impact on your relationship? | Not at all | 1 (4.5) |
| Not very much | 6 (27.3) | |
| Very much | 9 (40.9) | |
| Completely | 6 (27.3) | |
| 8. How did the COVID-19 emergency impact on all aspects of your relationship? | Made them much worse | 8 (36.4) |
| Made them worse | 12 (54.5) | |
| Stayed the same | 2 (9.1) | |
| Made them better | 0 (0) | |
| Made them much better | 0 (0) | |
| 9. How did the COVID-19 emergency impact on your sexuality? | Very badly | 13 (59.1) |
| Badly | 7 (31.8) | |
| No difference | 2 (9.1) | |
| Improved | 0 (0) | |
| Much improved | 0 (0) | |
| 10. Did you receive any information or advice regarding the sexual intercourse during COVID-19 emergency? | No | 22 (100) |
| 11. Did you receive any information or advice regarding having pregnancy during COVID-19 emergency? | No | 22 (100) |
| Wilcoxon Sign Rank Test p-Value | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Time 1 | Time 2 | Time 3 | Time 4 | Time 1 vs. Time 2 | Time 2 vs. Time 3 | Time 3 vs. Time 4 | Time 1 vs. Time 3 | Time 1 vs. Time 4 | Time 2 vs. Time 4 | ||
| SD 1 | Median | 2 | 3 | 2 | 2 | 0.001 | 0.001 | 0.3 | 0.3 | 1.0 | 0.001 |
| IQR | 2–2.8 | 2.2–4.0 | 2.0–2.0 | 2.0–2.8 | |||||||
| SD 2 | Median | 2 | 3 | 2 | 2 | <0.001 | 0.001 | 0.2 | 0.2 | 1.0 | <0.001 |
| IQR | 2.0–2.8 | 3.0–4.0 | 2.0–3.0 | 2.0–2.8 | |||||||
| SD 3 | Median | 2 | 3 | 2 | 2 | 0.002 | <0.001 | 1.0 | 0.3 | 0.3 | 0.001 |
| IQR | 2.0–3.0 | 3.0–4.0 | 2.0–3.0 | 2.0–3.0 | |||||||
| SD 4 | Median | 2 | 3 | 2 | 2 | 0.001 | 0.001 | 0.2 | 0.5 | 0.3 | <0.001 |
| IQR | 2.0–3.0 | 3.0–4.0 | 2.0–3.0 | 2.0–2.8 | |||||||
| SD 5 | Median | 2 | 3.5 | 2 | 2 | 0.004 | 0.01 | 0.2 | 0.2 | 1.0 | <0.01 |
| IQR | 2.0–3.0 | 3.0–4.0 | 2.0–3.8 | 2.0–3.0 | |||||||
| SD 6 | Median | 2 | 3 | 2 | 2 | 0.005 | <0.001 | 0.8 | 0.3 | 1.0 | <0.01 |
| IQR | 2.0–3.0 | 3.0–4.0 | 2.0–3.0 | 2.0–3.0 | |||||||
| SD 7 | Median | 2 | 3 | 2 | 2 | 0.03 | 0.09 | 0.2 | 0.2 | 1.0 | 0.03 |
| IQR | 2.0–3.0 | 2.0–4.0 | 2.0–3.0 | 2.0–2.8 | |||||||
| SD 8 | Median | 2 | 3 | 2 | 2 | <0.001 | <0.001 | 0.2 | 1.0 | 0.1 | <0.001 |
| IQR | 2.0–2.0 | 3.0–4.0 | 2.0–2.0 | 2.0–2.0 | |||||||
| SD 9 | Median | 2.5 | 3 | 2 | 2.5 | 0.04 | 0.01 | 0.4 | 0.1 | 1.0 | 0.03 |
| IQR | 2.0–3.0 | 3.0–4.0 | 2.0–3.0 | 2.0–3.0 | |||||||
| SD 10 | Median | 2 | 3 | 2 | 2 | <0.01 | 0.01 | 0.07 | 0.1 | 1.0 | <0.01 |
| IQR | 2.0–3.0 | 2.2–4.0 | 2.0–3.0 | 2.0–3.0 | |||||||
| SD 11 | Median | 2 | 3 | 2 | 2 | <0.001 | 0.01 | 0.01 | 0.03 | 1.0 | <0.001 |
| IQR | 2.0–2.0 | 3.0–4.0 | 2.0–3.0 | 2.0–2.0 | |||||||
| SD 12 | Median | 2 | 3 | 2 | 2 | <0.01 | <0.01 | 0.1 | 1.0 | 0.1 | <0.001 |
| IQR | 2.0–3.0 | 3.0–4.0 | 2.0–3.0 | 2.0–3.0 | |||||||
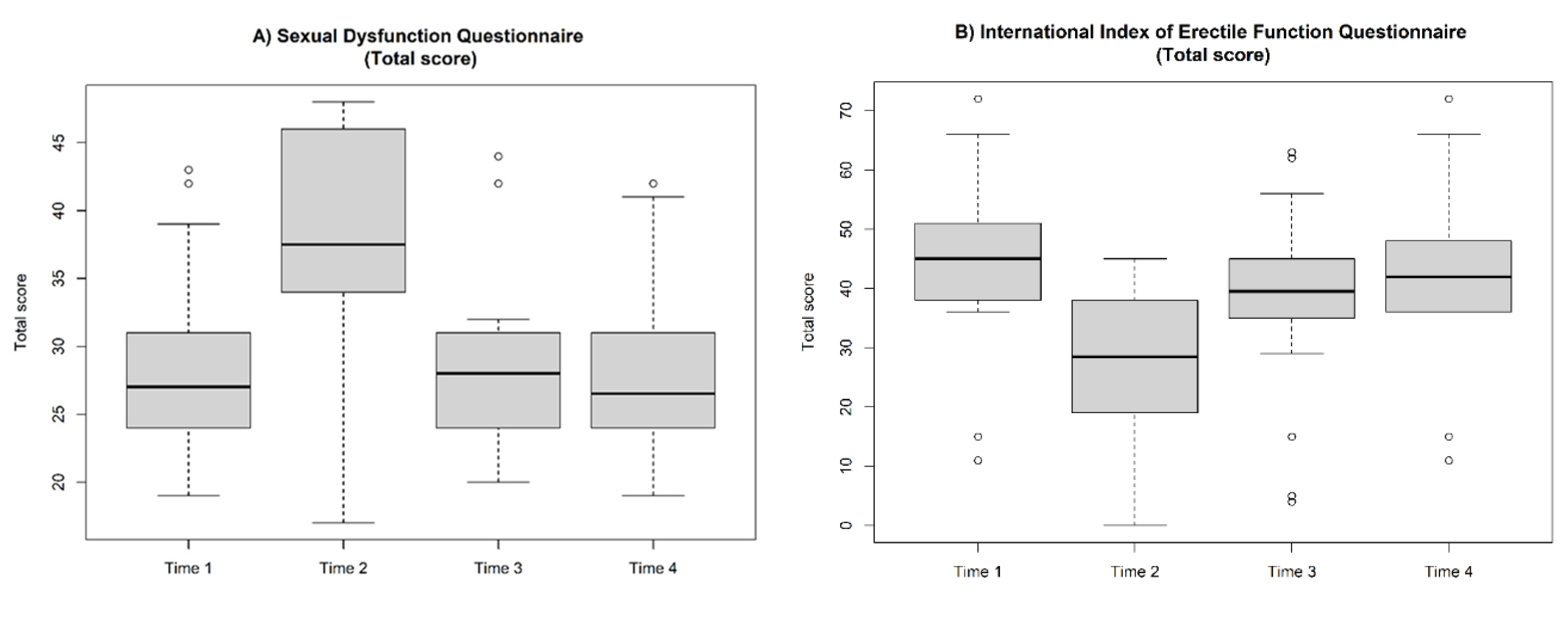
| SD TOT | Median | 27 | 37.5 | 28 | 26.5 | <0.001 | <0.001 | 0.06 | 0.8 | 0.1 | <0.001 |
| IQR | 24–30.2 | 34.2–45.5 | 24.0–31.0 | 24.0–30.2 | |||||||
| Wilcoxon Sign Rank Test p-Value | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Time 1 | Time 2 | Time 3 | Time 4 | Time 1 vs. Time 2 | Time 2 vs. Time 3 | Time 3 vs. Time 4 | Time 1 vs. Time 3 | Time 1 vs. Time 4 | Time 2 vs. Time 4 | ||
| IIEF-EF | Median | 15 | 10 | 13 | 14 | <0.001 | <0.001 | 0.07 | <0.001 | 0.07 | <0.001 |
| IQR | 12.2–18.5 | 5.0–12.0 | 10.2–15.8 | 10.0–18.5 | |||||||
| IIEF-OF | Median | 5 | 4.5 | 5 | 5 | <0.001 | <0.001 | 0.5 | 0.01 | 0.3 | <0.001 |
| IQR | 5.0–6.8 | 2.0.2–5 | 5.0–5.8 | 5.0–6.0 | |||||||
| IIEF-SD | Median | 7 | 5 | 5 | 5.5 | <0.001 | 0.3 | 0.01 | <0.001 | 0.1 | <0.01 |
| IQR | 5.0–8.0 | 2.2–6.8 | 3.2–7.0 | 5.0–8.0 | |||||||
| IIEF-IS | Median | 10 | 5 | 9 | 10 | <0.001 | 0.001 | 0.06 | 0.01 | 1.0 | <0.001 |
| IQR | 8.0–10.8 | 5.0–7.8 | 7.2–10.0 | 8.0–10.0 | |||||||
| IIEF-OS | Median | 7 | 5 | 7 | 7 | <0.001 | 0.004 | 0.5 | 0.053 | 0.2 | 0.001 |
| IQR | 6.0–8.0 | 3.0–6.8 | 6.0–8.0 | 6.0–8.0 | |||||||
| IIEF-TOT | Median | 45 | 28.5 | 39.5 | 42 | <0.001 | <0.001 | <0.01 | <0.001 | 0.09 | <0.001 |
| IQR | 38.0–50.2 | 19.5–38.0 | 35.5–44.2 | 36.0–48.0 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spirito, L.; Morelli, M.; La Rocca, R.; Napolitano, L.; Ruvolo, C.C.; Romano, L.; di Giovanni, A.; Sciorio, C.; Concetti, S.; Montanari, E.; et al. COVID-19 Quarantine Dramatically Affected Male Sexual Behavior: Is There a Possibility to Go Back to Normality? J. Clin. Med. 2022, 11, 2645. https://doi.org/10.3390/jcm11092645
Spirito L, Morelli M, La Rocca R, Napolitano L, Ruvolo CC, Romano L, di Giovanni A, Sciorio C, Concetti S, Montanari E, et al. COVID-19 Quarantine Dramatically Affected Male Sexual Behavior: Is There a Possibility to Go Back to Normality? Journal of Clinical Medicine. 2022; 11(9):2645. https://doi.org/10.3390/jcm11092645
Chicago/Turabian StyleSpirito, Lorenzo, Michele Morelli, Roberto La Rocca, Luigi Napolitano, Claudia Collà Ruvolo, Lorenzo Romano, Angelo di Giovanni, Carmine Sciorio, Sergio Concetti, Emanuele Montanari, and et al. 2022. "COVID-19 Quarantine Dramatically Affected Male Sexual Behavior: Is There a Possibility to Go Back to Normality?" Journal of Clinical Medicine 11, no. 9: 2645. https://doi.org/10.3390/jcm11092645