
SARS-CoV-2 in the Middle Ear-CovEar: A Prospective Pilot Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
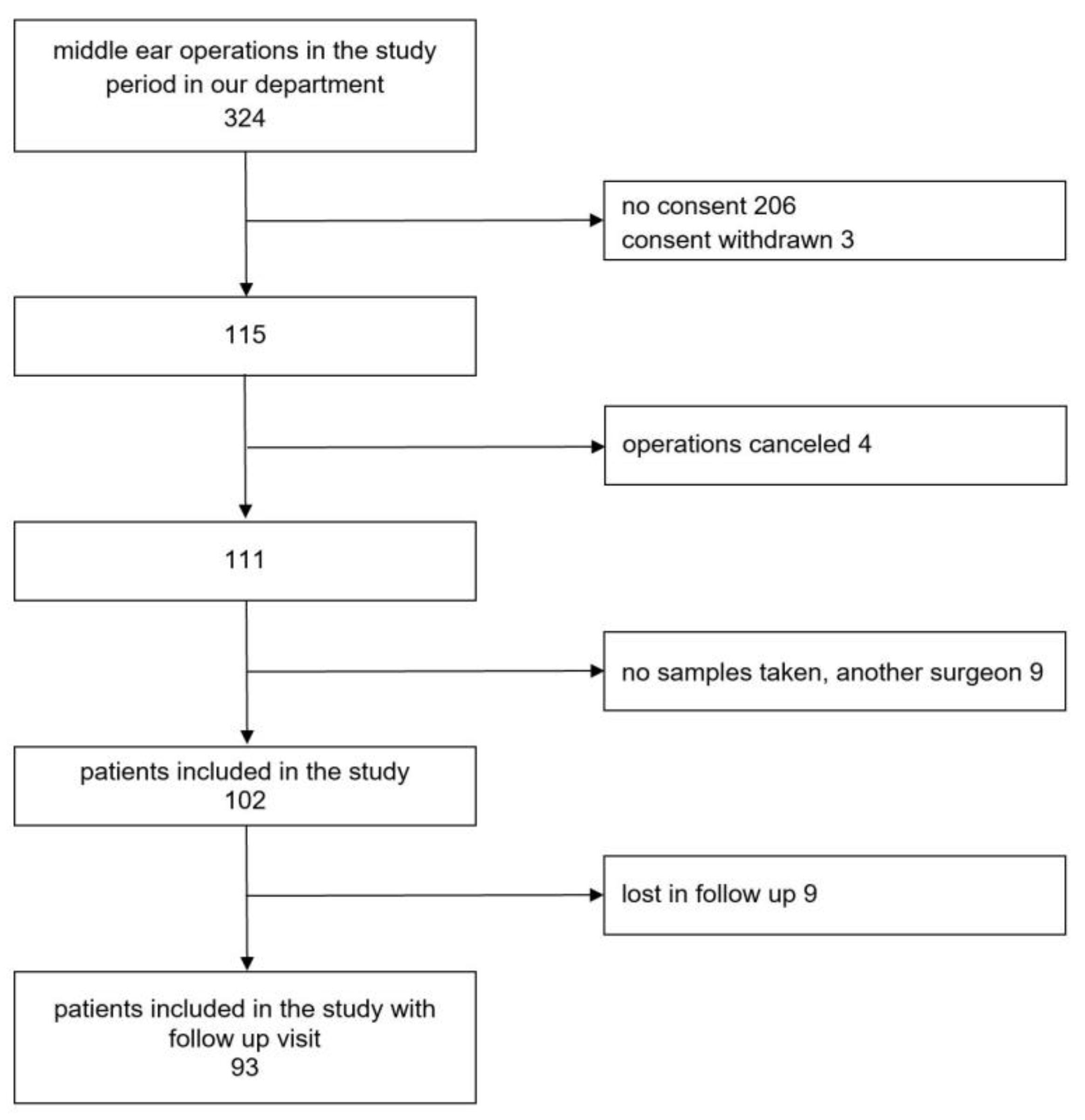
2.1. Study Design, Inclusion Criteria and Ethics Approval
2.2. Material
Clinical Data
2.3. Sample Collection
2.4. Laboratory Procedures
2.5. Statistical Analysis
3. Results
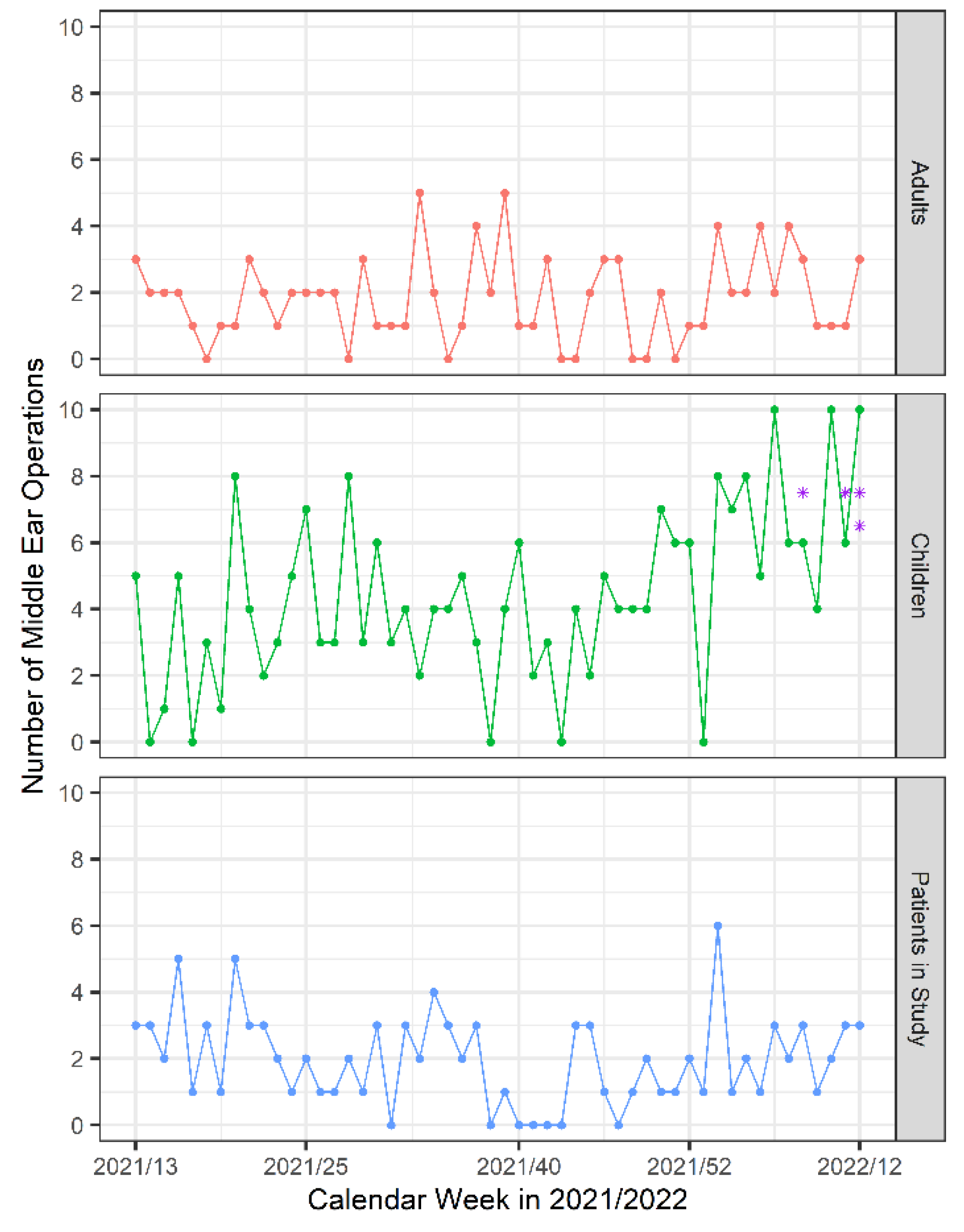
3.1. Demographics
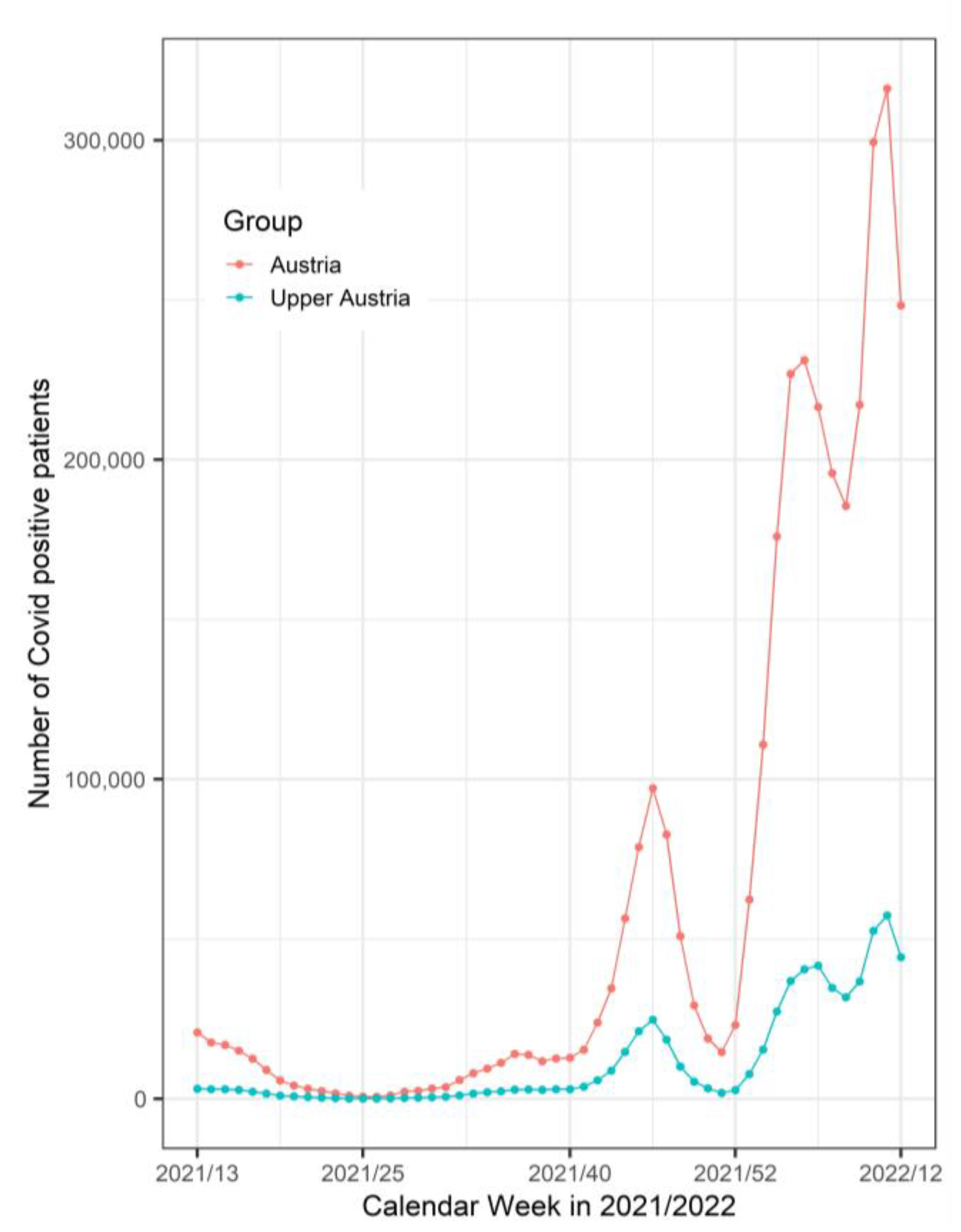
3.2. SARS-CoV-2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- COVID Live—Coronavirus Statistics—Worldometer. Available online: https://www.worldometers.info/coronavirus/ (accessed on 15 September 2022).
- Fidan, V. New Type of Corona Virus Induced Acute Otitis Media in Adult. Am. J. Otolaryngol. 2020, 41, 102487. [Google Scholar] [CrossRef]
- Almufarrij, I.; Uus, K.; Munro, K.J. Does Coronavirus Affect the Audio-Vestibular System? A Rapid Systematic Review. Int. J. Audiol. 2020, 59, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Liaw, J.; Saadi, R.; Patel, V.A.; Isildak, H. Middle Ear Viral Load Considerations in the COVID-19 Era: A Systematic Review. Otol. Neurotol. 2020, 42, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Deitmer, T.; Dietz, A.; Chaberny, I.F.; Pietsch, C. The nasal and pharyngeal swab techniques during the COVID-19-pandemic—the ENT-perspective—SARS-CoV-2, Coronavirus, nasal swab, pharyngeal swab, complications. Laryngorhinootologie 2021, 100, 517–525. [Google Scholar] [CrossRef]
- Cetinkaya, E.A. COVID-19 Pandemic and Otologic Surgery. J. Craniofac. Surg. 2020, 31, e651–e652. [Google Scholar] [CrossRef] [PubMed]
- Couloigner, V.; Schmerber, S.; Nicollas, R.; Coste, A.; Barry, B.; Makeieff, M.; Boudard, P.; Bequignon, E.; Morel, N.; Lescanne, E.; et al. COVID-19 and ENT Surgery. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2020, 137, 161–166. [Google Scholar] [CrossRef]
- Frazier, K.M.; Hooper, J.E.; Mostafa, H.H.; Stewart, C.M. SARS-CoV-2 Virus Isolated From the Mastoid and Middle Ear: Implications for COVID-19 Precautions During Ear Surgery. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 964–966. [Google Scholar] [CrossRef]
- Kurabi, A.; Pak, K.; DeConde, A.S.; Ryan, A.F.; Yan, C.H. Immunohistochemical and QPCR Detection of SARS-CoV-2 in the Human Middle Ear Versus the Nasal Cavity: Case Series. Head Neck Pathol. 2022, 16, 607–611. [Google Scholar] [CrossRef]
- Jeican, I.I.; Aluaș, M.; Lazăr, M.; Barbu-Tudoran, L.; Gheban, D.; Inișca, P.; Albu, C.; Tripon, S.; Albu, S.; Siserman, C.; et al. Evidence of SARS-CoV-2 Virus in the Middle Ear of Deceased COVID-19 Patients. Diagnostics 2021, 11, 1535. [Google Scholar] [CrossRef]
- Kesser, B.W. News Flash!—SARS-CoV-2 Isolated From the Middle Ear and Mastoid. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 966–967. [Google Scholar] [CrossRef]
- Austrian Agency for Health and Food Safety. AGES Österreichische Agentur Für Gesundheit Und Ernährungssicherheit. Available online: https://www.ages.at/en/ (accessed on 15 September 2022).
- Ripley, B.D. The R Project in Statistical Computing. MSOR Connect. 2001, 1, 23–25. [Google Scholar] [CrossRef]
- Sigrist, C.J.; Bridge, A.; Le Mercier, P. A Potential Role for Integrins in Host Cell Entry by SARS-CoV-2. Antivir. Res. 2020, 177, 104759. [Google Scholar] [CrossRef] [PubMed]
- Wanna, G.B.; Schwam, Z.G.; Kaul, V.F.; Cosetti, M.K.; Perez, E.; Filip, P.; Javaid, W.; Kandel, A.; Paniz-Mondolfi, A.; Govindaraj, S.; et al. COVID-19 Sampling from the Middle Ear and Mastoid: A Case Report. Am. J. Otolaryngol. 2020, 41, 102577. [Google Scholar] [CrossRef] [PubMed]
- Pitkäranta, A.; Virolainen, A.; Jero, J.; Arruda, E.; Hayden, F.G. Detection of Rhinovirus, Respiratory Syncytial Virus, and Coronavirus Infections in Acute Otitis Media by Reverse Transcriptase Polymerase Chain Reaction. Pediatrics 1998, 102, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Ayache, S.; Kutz, W.; Isaacson, B.; Badr-El-Dine, M.; Nogueira, J.F.; Marchioni, D.; Presutti, L. COVID-19 and Ear Endoscopy in Otologic Practices. Eur. Arch. Otorhinolaryngol. 2021, 278, 2133–2135. [Google Scholar] [CrossRef]
- Bhardwaj, R.; Sharma, A.; Singhal, B. Covid-19 and Ear Surgery: Treatment Strategies and Triage during the Post-Lockdown Period. Indian J. Otolaryngol. Head Neck Surg. 2021, 73, 480–485. [Google Scholar] [CrossRef]
- van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Jewett, D.L.; Heinsohn, P.; Bennett, C.; Rosen, A.; Neuilly, C. Blood-Containing Aerosols Generated by Surgical Techniques: A Possible Infectious Hazard. Am. Ind. Hyg. Assoc. J. 1992, 53, 228–231. [Google Scholar] [CrossRef]
- El-Anwar, M.W.; Elzayat, S.; Fouad, Y.A. ENT Manifestation in COVID-19 Patients. Auris Nasus Larynx 2020, 47, 559–564. [Google Scholar] [CrossRef]
- Munro, K.J.; Uus, K.; Almufarrij, I.; Chaudhuri, N.; Yioe, V. Persistent Self-Reported Changes in Hearing and Tinnitus in Post-Hospitalisation COVID-19 Cases. Int. J. Audiol. 2020, 59, 889–890. [Google Scholar] [CrossRef]
- Mustafa, M.W.M. Audiological Profile of Asymptomatic Covid-19 PCR-Positive Cases. Am. J. Otolaryngol. 2020, 41, 102483. [Google Scholar] [CrossRef] [PubMed]
- Maharaj, S.; Bello Alvarez, M.; Mungul, S.; Hari, K. Otologic Dysfunction in Patients with COVID-19: A Systematic Review. Laryngoscope Investig. Otolaryngol. 2020, 5, 1192–1196. [Google Scholar] [CrossRef] [PubMed]
- Almufarrij, I.; Munro, K.J. One Year on: An Updated Systematic Review of SARS-CoV-2, COVID-19 and Audio-Vestibular Symptoms. Int. J. Audiol. 2021, 60, 935–945. [Google Scholar] [CrossRef]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Total | Children | Adults |
|---|---|---|---|
| Number of Patients (%) | 102 (100) | 63 (61.76) | 39 (38.24) |
| Female (%) | 45 (44.12) | 32 (50.79) | 13 (33.33) |
| Male (%) | 57 (55.88) | 31 (49.21) | 26 (66.67) |
| Age Median; (IQR) [y] | 5.50 (43) | 4 (2) | 51 (18.50) |
| Weight Median (IQR) [kg] | 25.50 (56.12) | 18 (6) | 80 (22) |
| Type of Surgery | |||
| Acute Surgery (%) | 3 (2.94) | 0 (0) | 3 (7.69) |
| Elective Surgery (%) | 99 (97.06) | 63 (100) | 36 (92.31) |
| Tympanic Membrane Incision, Tympanostomy Tube Insertion or Removal (%) | 75 (73.53) | 60 (95.24) | 15 (38.46) |
| Tympanoplasty ± Mastoidectomy (%) | 18 (17.65) | 3 (4.76) | 15 (38.46) |
| Stapesplasty (%) | 3 (2.94) | 0 (0) | 3 (7.69) |
| Implantation CI, VSB; (%) | 6 (5.88) | 0 (0) | 6 (15.38) |
| Indication for Operation | |||
| Otosclerosis (%) | 3 (2.94) | 0 (0) | 3 (7.69) |
| Hearing Loss (%) | 7 (6.86) | 0 (0) | 7 (17.95) |
| OME, AOM, Eustachian Tube Dysfunction (%) | 67 (65.69) | 53 (84.13) | 14 (35.90) |
| CSOM (%) | 17 (16.67) | 8 (12.70) | 9 (23.08) |
| CHOL (%) | 8 (7.84) | 2 (3.17) | 6 (15.38) |
| Parameters | Total (%) | Children (%) | Adults (%) | p-Value |
|---|---|---|---|---|
| ASA Score | ||||
| I | 70 (68.63) | 57 (90.48) | 13 (33.33) | |
| II | 29 (28.43) | 6 (9.52) | 23 (58.97) | <0.001 |
| III | 3 (2.94) | 0 | 3 (7.69) | |
| IV–VI | 0 | 0 | 0 | |
| Cardiovascular Diseases | 15 (14.71) | 2 (3.17) | 13 (33.33) | <0.001 |
| Reflux | 11(10.78) | 1 (1.59) | 10 (25.64) | <0.001 |
| Respiratory Diseases | 8 (7.84) | 1 (1.59) | 7 (17.95) | <0.005 |
| Obstructive Sleep Apnea | 4 (3.92) | 3 (4.76) | 1 (2.56) | NA |
| Craniofacial Anomalies | 4 (3.92) | 2 (3.17) a | 2 (5.13) b | NA |
| Thyroid Gland Disease | 4 (3.92) | 0 (0) | 4 (10.26) | NA |
| Diabetes Mellitus | 3 (2.94) | 0 (0) | 3 (7.69) | NA |
| Wegener Disease | 1 (0.98) | 0 (0) | 1(2.56) | NA |
| Down Syndrome | 1 (0.98) | 0 (0) | 1(2.56) | NA |
| Muscle Hypotonia | 1 (0.98) | 1(1.59) | 0 (0) | NA |
| Allergy | 9 (8.82) | 6 (9.52) | 3 (7.69) | 1 |
| Parameters | Total (%) | Children (%) | Adults (%) |
|---|---|---|---|
| Vaccinated Patients | 25 (24.51) | 2 (3.17) | 23 (58.97) |
| 1. Comirnaty (BioNTech/Pfizer) | 19 (18.63) | 19 (18.63) | 19 (18.63) |
| 2. Jannsen (Johnson & Johnson) | 1 (0.98) | 1 (0.98) | 1 (0.98) |
| 3. Spikevax (Moderna) | 1 (0.98) | 1 (0.98) | 1 (0.98) |
| 1. + 2. Comirnaty + Jannsen | 1 (0.98) | 1 (0.98) | 1 (0.98) |
| Vaccination of unknown kind | 3 (2.94) | 3 (2.94) | 3 (2.94) |
| No vaccination | 77 (75.49) | 77 (75.49) | 77 (75.49) |
| Time between last vaccination and operation | |||
| Min (d) | 6 | 95 | 6 |
| Max (d) | 154 | 130 | 154 |
| Median (d) | 48 | 44 | |
| IQR (d) | 61 | 59 | |
| Mittelwert (d) | 62 | 113 | 57 |
| NA | 1 | 0 | 1 |
| Patients with COVID-19 Infection History | 13 (12.75) | 9 (14.29) | 4 (10.26) |
| Time between the last COVID-19 infection and operation | |||
| Min (d) | 7 | 7 | 8 |
| Max (d) | 495 | 495 | 408 |
| Median (d) | 132 | 103 | 272 |
| IQR (d) | 318 | 140 | 295 |
| Mittelwert (d) | 189 | 166 | 240 |
| NA | 0 | 0 | 0 |
| Patients with Proven Contact | 34 (33.33) | 27 (42.86) | 7 (17.95) |
| Time between the last proven contact and operation | |||
| Min (d) | 9 | 45 | 9 |
| Max (d) | 667 | 667 | 353 |
| Median (d) | 129 | 131 | 127 |
| IQR (d) | 127 | 129 | 97 |
| Mittelwert (d) | 173 | 185 | 130 |
| NA | 0 | 0 | 0 |
| SARS-CoV-2 in the Ear | 2 (1.96) | 2 (3.17) | 0 (0) |
| SARS-CoV-2 in the Nasopharynx | 4 (3.92) | 4 (6.35) | 0 (0) |
| SARS-CoV-2 in the Filter | 0 (0) | 0 (0) | 0 (0) |
| Parameters | Patient No. 72 | Patient No. 95 | Patient No. 99 | Patient No. 101 |
|---|---|---|---|---|
| Sex and Age [y] | M 4 | M 5 | F 8 | F 4 |
| Weight [kg] | 18 | 20 | 30 | 17 |
| Type of Surgery | Elective | Elective | Elective | Elective |
| Type of Procedure | PC | PC | G | G |
| Indication for Operation | OME | OME | OME | OME |
| SARS-CoV-2 in Ear (ct) | +(29.77) | +(30.03) | No | No |
| SARS-CoV-2 in Nasopharynx (ct) | +(25.94) | +(32.15) | +(32.11) | +(37.06) |
| SARS-CoV-2 in Filter Sample | No | No | No | No |
| Vaccination Against SARS-CoV-2 | No | No | No | No |
| COVID-19 Infection Preoperatively [Days Before Operation] | 7 | No | 51 | 50 |
| Proven Contact with SARS-CoV-2-Positive Person [Days Before Operation] | No | 15 | 68 | No |
| COVID-19 Infection After Surgery | No | No | No | No |
| Additional Diseases: | No | No | No | No |
| ASA Score | I | I | I | I |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rubicz, N.; Poier-Fabian, N.; Paar, C.; Winkler-Zamani, M.; Hermann, P.; Raidl, S.; Zwittag, P.M. SARS-CoV-2 in the Middle Ear-CovEar: A Prospective Pilot Study. J. Pers. Med. 2023, 13, 905. https://doi.org/10.3390/jpm13060905
Rubicz N, Poier-Fabian N, Paar C, Winkler-Zamani M, Hermann P, Raidl S, Zwittag PM. SARS-CoV-2 in the Middle Ear-CovEar: A Prospective Pilot Study. Journal of Personalized Medicine. 2023; 13(6):905. https://doi.org/10.3390/jpm13060905
Chicago/Turabian StyleRubicz, Nina, Nikolaus Poier-Fabian, Christian Paar, Markus Winkler-Zamani, Philipp Hermann, Stefan Raidl, and Paul Martin Zwittag. 2023. "SARS-CoV-2 in the Middle Ear-CovEar: A Prospective Pilot Study" Journal of Personalized Medicine 13, no. 6: 905. https://doi.org/10.3390/jpm13060905