
C3a and C5b-9 Differentially Predict COVID-19 Progression and Outcome
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. C3a and C5b-9 Measurement by Standard Enzyme-Linked Immunosorbent Assay (ELISA) Methodology
2.2. Statistical Analysis
3. Results
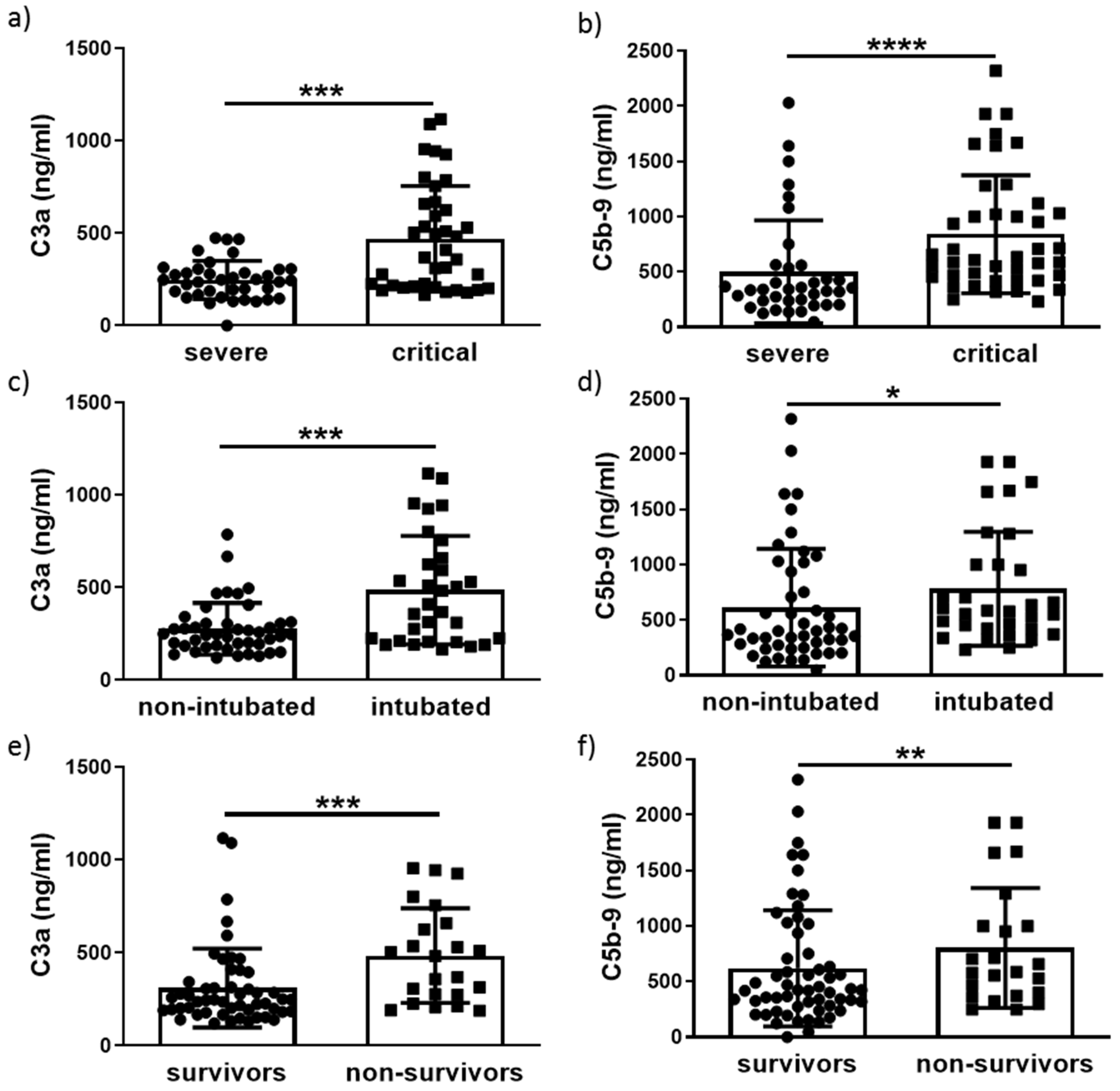
3.1. Increase of C3a and C5b-9 Levels in COVID-19 Patients
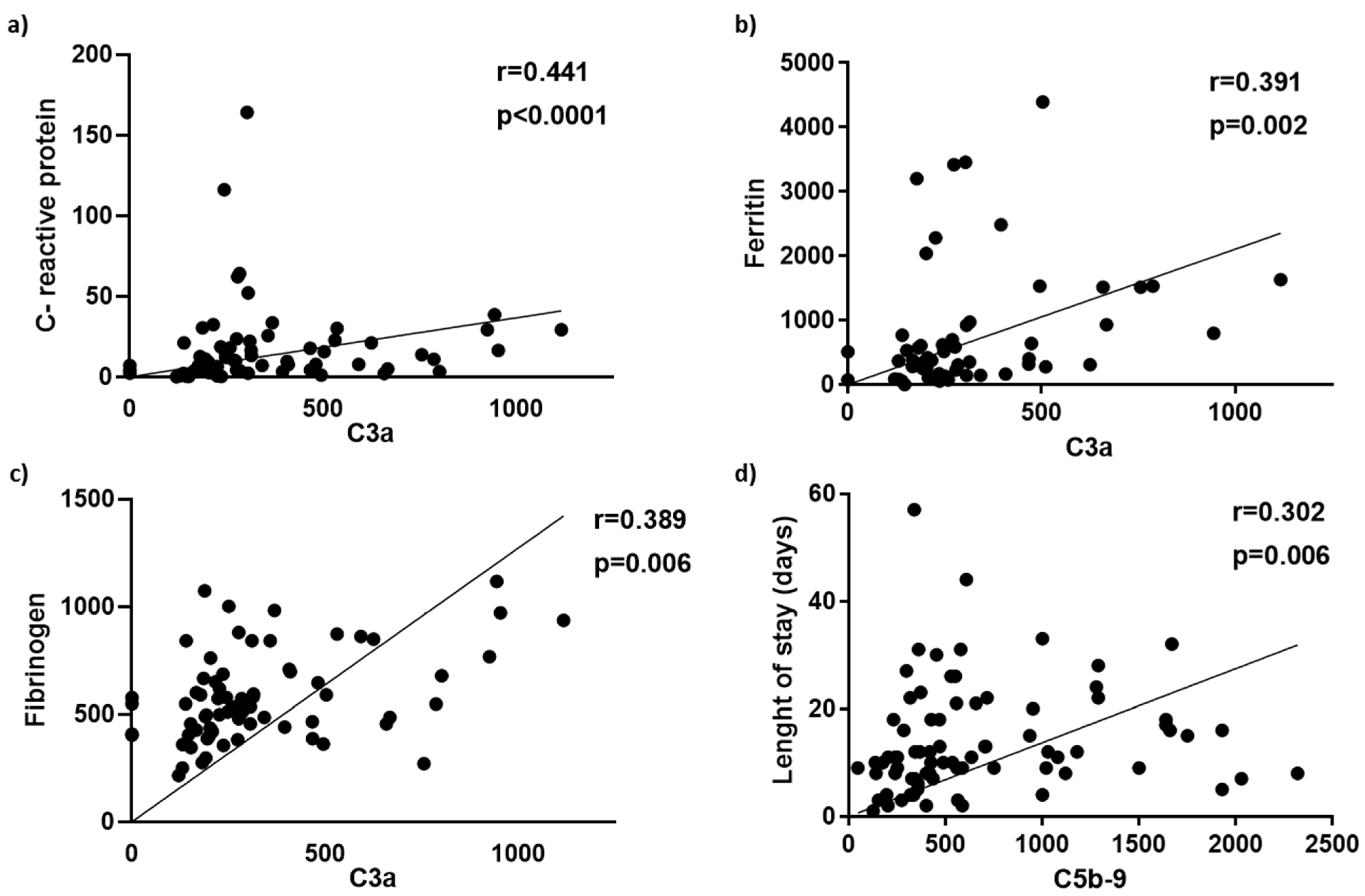
3.2. Differential Prediction of COVID-19 Progression and Outcome by C3a and C5b-9 Levels
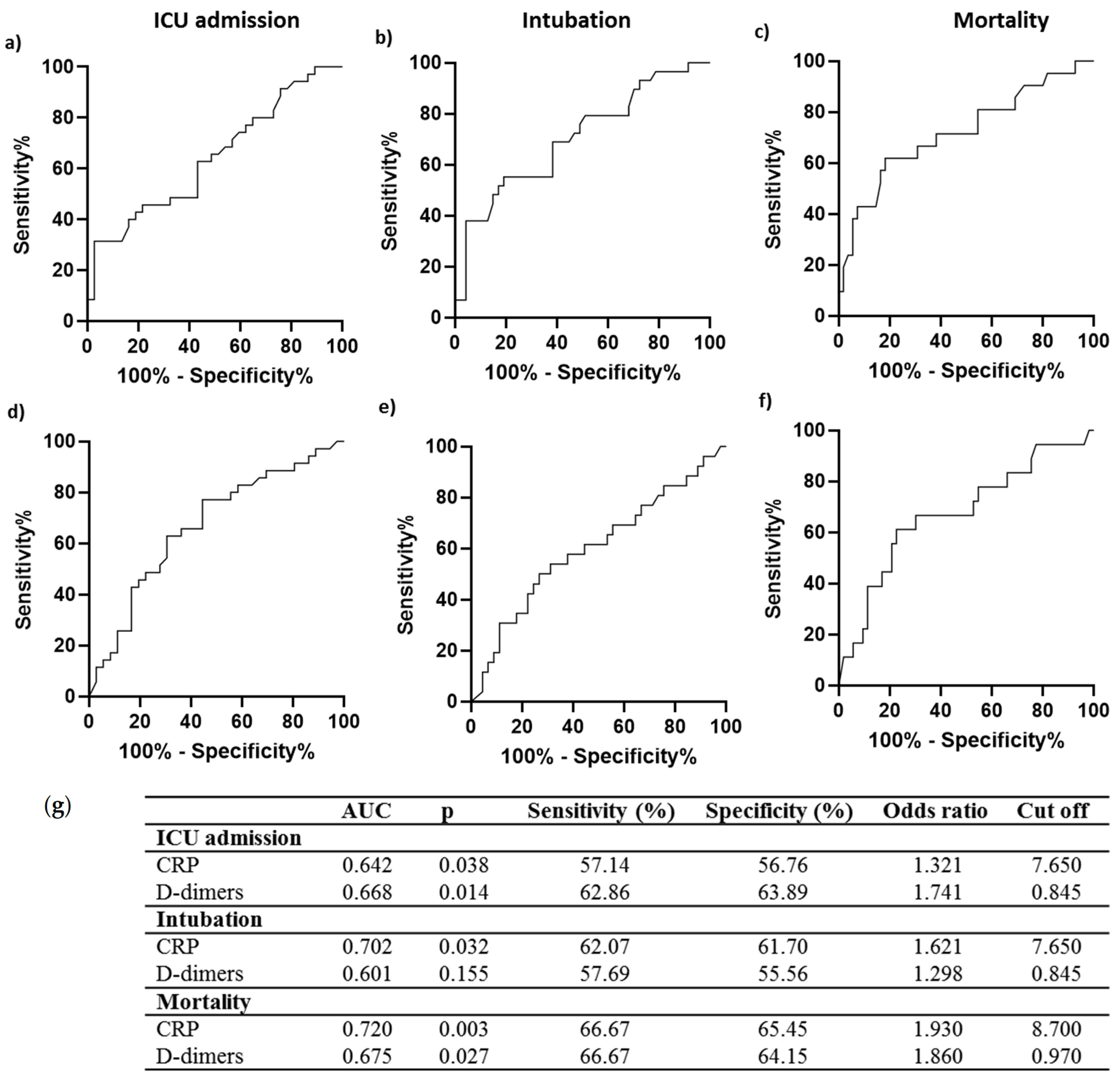
3.3. C3a and C5b-9 Performance as COVID-19 Prognosis Tools
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Jamilloux, Y.; Henry, T.; Belot, A.; Viel, S.; Fauter, M.; El Jammal, T.; Walzer, T.; Francois, B.; Seve, P. Should we stimulate or suppress immune responses in COVID-19? Cytokine and anti-cytokine interventions. Autoimmun. Rev. 2020, 19, 102567. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Thachil, J.; Iba, T.; Levy, J.H. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Haematol. 2020, 7, e438–e440. [Google Scholar] [CrossRef] [PubMed]
- Detsika, M.G.; Lianos, E.A. Regulation of Complement Activation by Heme Oxygenase-1 (HO-1) in Kidney Injury. Antioxidants 2021, 10, 60. [Google Scholar] [CrossRef]
- Merle, N.S.; Church, S.E.; Fremeaux-Bacchi, V.; Roumenina, L.T. Complement System Part I—Molecular Mechanisms of Activation and Regulation. Front. Immunol. 2015, 6, 262. [Google Scholar] [CrossRef] [PubMed]
- Mamidi, S.; Hone, S.; Kirschfink, M. The complement system in cancer: Ambivalence between tumour destruction and promotion. Immunobiology 2017, 222, 45–54. [Google Scholar] [CrossRef]
- Zinellu, A.; Mangoni, A.A. Serum Complement C3 and C4 and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis With Meta-Regression. Front. Immunol. 2021, 12, 696085. [Google Scholar] [CrossRef]
- Magro, C.; Mulvey, J.J.; Berlin, D.; Nuovo, G.; Salvatore, S.; Harp, J.; Baxter-Stoltzfus, A.; Laurence, J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Transl. Res. 2020, 220, 1–13. [Google Scholar] [CrossRef]
- Niederreiter, J.; Eck, C.; Ries, T.; Hartmann, A.; Markl, B.; Buttner-Herold, M.; Amann, K.; Daniel, C. Complement Activation via the Lectin and Alternative Pathway in Patients With Severe COVID-19. Front. Immunol. 2022, 13, 835156. [Google Scholar] [CrossRef]
- Ali, Y.M.; Ferrari, M.; Lynch, N.J.; Yaseen, S.; Dudler, T.; Gragerov, S.; Demopulos, G.; Heeney, J.L.; Schwaeble, W.J. Lectin Pathway Mediates Complement Activation by SARS-CoV-2 Proteins. Front. Immunol. 2021, 12, 714511. [Google Scholar] [CrossRef]
- Yang, S.; McGookey, M.; Wang, Y.; Cataland, S.R.; Wu, H.M. Effect of blood sampling, processing, and storage on the measurement of complement activation biomarkers. Am. J. Clin. Pathol. 2015, 143, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Tom, J.; Bao, M.; Tsai, L.; Qamra, A.; Summers, D.; Carrasco-Triguero, M.; McBride, J.; Rosenberger, C.M.; Lin, C.J.F.; Stubbings, W.; et al. Prognostic and Predictive Biomarkers in Patients With Coronavirus Disease 2019 Treated With Tocilizumab in a Randomized Controlled Trial. Crit. Care Med. 2022, 50, 398–409. [Google Scholar] [CrossRef] [PubMed]
- de Nooijer, A.H.; Grondman, I.; Janssen, N.A.F.; Netea, M.G.; Willems, L.; van de Veerdonk, F.L.; Giamarellos-Bourboulis, E.J.; Toonen, E.J.M.; Joosten, L.A.B.; RCI-COVID-19 study group. Complement Activation in the Disease Course of Coronavirus Disease 2019 and Its Effects on Clinical Outcomes. J. Infect. Dis. 2021, 223, 214–224. [Google Scholar] [CrossRef]
- Sinkovits, G.; Mezo, B.; Reti, M.; Muller, V.; Ivanyi, Z.; Gal, J.; Gopcsa, L.; Remenyi, P.; Szathmary, B.; Lakatos, B.; et al. Complement Overactivation and Consumption Predicts In-Hospital Mortality in SARS-CoV-2 Infection. Front. Immunol. 2021, 12, 663187. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; Szergyuk, I.; de Oliveira, M.H.S.; Lippi, G.; Benoit, J.L.; Vikse, J.; Benoit, S.W. Complement levels at admission as a reflection of coronavirus disease 2019 (COVID-19) severity state. J. Med. Virol. 2021, 93, 5515–5522. [Google Scholar] [CrossRef]
- Alosaimi, B.; Mubarak, A.; Hamed, M.E.; Almutairi, A.Z.; Alrashed, A.A.; AlJuryyan, A.; Enani, M.; Alenzi, F.Q.; Alturaiki, W. Complement Anaphylatoxins and Inflammatory Cytokines as Prognostic Markers for COVID-19 Severity and In-Hospital Mortality. Front. Immunol. 2021, 12, 668725. [Google Scholar] [CrossRef]
- Cyprian, F.S.; Suleman, M.; Abdelhafez, I.; Doudin, A.; Masud Danjuma, M.; Mir, F.A.; Parray, A.; Yousaf, Z.; Siddiqui, M.Y.A.; Abdelmajid, A.; et al. Complement C5a and Clinical Markers as Predictors of COVID-19 Disease Severity and Mortality in a Multi-Ethnic Population. Front. Immunol. 2021, 12, 707159. [Google Scholar] [CrossRef]
- Carvelli, J.; Demaria, O.; Vely, F.; Batista, L.; Chouaki Benmansour, N.; Fares, J.; Carpentier, S.; Thibult, M.L.; Morel, A.; Remark, R.; et al. Association of COVID-19 inflammation with activation of the C5a-C5aR1 axis. Nature 2020, 588, 146–150. [Google Scholar] [CrossRef]
- Declercq, J.; Van Damme, K.F.A.; De Leeuw, E.; Maes, B.; Bosteels, C.; Tavernier, S.J.; De Buyser, S.; Colman, R.; Hites, M.; Verschelden, G.; et al. Effect of anti-interleukin drugs in patients with COVID-19 and signs of cytokine release syndrome (COV-AID): A factorial, randomised, controlled trial. Lancet. Respir. Med. 2021, 9, 1427–1438. [Google Scholar] [CrossRef]
- Mastaglio, S.; Ruggeri, A.; Risitano, A.M.; Angelillo, P.; Yancopoulou, D.; Mastellos, D.C.; Huber-Lang, M.; Piemontese, S.; Assanelli, A.; Garlanda, C.; et al. The first case of COVID-19 treated with the complement C3 inhibitor AMY-101. Clin. Immunol. 2020, 215, 108450. [Google Scholar] [CrossRef]
- Laurence, J.; Mulvey, J.J.; Seshadri, M.; Racanelli, A.; Harp, J.; Schenck, E.J.; Zappetti, D.; Horn, E.M.; Magro, C.M. Anti-complement C5 therapy with eculizumab in three cases of critical COVID-19. Clin. Immunol. 2020, 219, 108555. [Google Scholar] [CrossRef] [PubMed]
- Diurno, F.; Numis, F.G.; Porta, G.; Cirillo, F.; Maddaluno, S.; Ragozzino, A.; De Negri, P.; Di Gennaro, C.; Pagano, A.; Allegorico, E.; et al. Eculizumab treatment in patients with COVID-19: Preliminary results from real life ASL Napoli 2 Nord experience. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 4040–4047. [Google Scholar] [CrossRef] [PubMed]
- Vlaar, A.P.J.; de Bruin, S.; Busch, M.; Timmermans, S.; van Zeggeren, I.E.; Koning, R.; Ter Horst, L.; Bulle, E.B.; van Baarle, F.; van de Poll, M.C.G.; et al. Anti-C5a antibody IFX-1 (vilobelimab) treatment versus best supportive care for patients with severe COVID-19 (PANAMO): An exploratory, open-label, phase 2 randomised controlled trial. Lancet Rheumatol. 2020, 2, e764–e773. [Google Scholar] [CrossRef]
- Urwyler, P.; Moser, S.; Charitos, P.; Heijnen, I.; Rudin, M.; Sommer, G.; Giannetti, B.M.; Bassetti, S.; Sendi, P.; Trendelenburg, M.; et al. Treatment of COVID-19 With Conestat Alfa, a Regulator of the Complement, Contact Activation and Kallikrein-Kinin System. Front. Immunol. 2020, 11, 2072. [Google Scholar] [CrossRef]
- Rambaldi, A.; Gritti, G.; Mico, M.C.; Frigeni, M.; Borleri, G.; Salvi, A.; Landi, F.; Pavoni, C.; Sonzogni, A.; Gianatti, A.; et al. Endothelial injury and thrombotic microangiopathy in COVID-19: Treatment with the lectin-pathway inhibitor narsoplimab. Immunobiology 2020, 225, 152001. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Severe COVID-19 | Critical COVID-19 | p Value | |
|---|---|---|---|
| Age (years) | 58.46 ± 15.80 | 65.65 ± 13.14 | 0.022 |
| Male | 21 (55.26%) | 29 (76.31%) | 0.154 |
| Diabetes | 3 (7.89%) | 7 (18.42%) | 0.398 |
| Cardiovascular disease | 2 (5.26%) | 7 (18.42%) | 0.206 |
| Chronic obstructive pulmonary disease | 1 (2.63%) | 2 (5.26%) | 0.840 |
| Symptoms | |||
| Temperature (>37.3 °C) | 18 (47.36%) | 22 (57.89%) | 0.655 |
| paO2/FIO2 | 320.20 ± 60.09 | 119.13 ± 67.71 | <0.0001 |
| Days of illness before admission | 6.27 ± 2.60 | 6.41 ± 3.37 | 0.819 |
| Laboratory baseline | |||
| White blood cells | 6887.00 ± 3749 | 13136 ± 1106 | <0.0001 |
| Neutrophils | 69.44 ± 14.88 | 80.72 ± 15.67 | <0.0001 |
| Lymphocytes | 25.80 ± 16.86 | 12.28 ± 12.89 | <0.0001 |
| Platelets | 221216 ± 97386 | 236912 ± 125951 | 0.523 |
| C-reactive protein | 8.314 ± 6.993 | 13.76 ± 10.95 | 0.037 |
| Troponin | 29.14 ± 93.72 | 481.20 ± 1404 | <0.0001 |
| Urea | 31.16 ± 18.40 | 59.00 ± 47.47 | <0.0001 |
| Creatinine | 0.843 ± 0.196 | 1.414 ± 1.835 | 0.122 |
| Aspartate aminotransferase | 40.62 ± 33.03 | 34.76 ± 22.94 | 0.424 |
| Alanine transaminase | 34.76 ± 22.94 | 62.17 ± 74.60 | 0.028 |
| Gamma-Glutamyltransferase | 44.05 ± 34.49 | 84.60 ± 97.36 | 0.082 |
| Lactate Dehydrogenase | 293.5 ± 116.1 | 517.0 ± 447.5 | 0.0001 |
| Albumin | 3.891 ± 0.403 | 3.214 ± 0.480 | <0.0001 |
| Days of hospital stay | 10.14 ± 6.204 | 19.14 ± 11.48 | <0.0001 |
| Survival | 35 (92.10%) | 18 (47.36%) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Detsika, M.G.; Diamanti, E.; Ampelakiotou, K.; Jahaj, E.; Tsipilis, S.; Athanasiou, N.; Dimopoulou, I.; Orfanos, S.E.; Tsirogianni, A.; Kotanidou, A. C3a and C5b-9 Differentially Predict COVID-19 Progression and Outcome. Life 2022, 12, 1335. https://doi.org/10.3390/life12091335
Detsika MG, Diamanti E, Ampelakiotou K, Jahaj E, Tsipilis S, Athanasiou N, Dimopoulou I, Orfanos SE, Tsirogianni A, Kotanidou A. C3a and C5b-9 Differentially Predict COVID-19 Progression and Outcome. Life. 2022; 12(9):1335. https://doi.org/10.3390/life12091335
Chicago/Turabian StyleDetsika, Maria G., Elpida Diamanti, Kleio Ampelakiotou, Edison Jahaj, Stamatis Tsipilis, Nikolaos Athanasiou, Ioanna Dimopoulou, Stylianos E. Orfanos, Alexandra Tsirogianni, and Anastasia Kotanidou. 2022. "C3a and C5b-9 Differentially Predict COVID-19 Progression and Outcome" Life 12, no. 9: 1335. https://doi.org/10.3390/life12091335