
The Humoral Immune Response of the ChAdOx1 nCoV-19 Vaccine in Maintenance Dialysis Patients without Prior COVID-19 Infection

 , , , , ,
, , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Flow Cytometry Analysis
2.3. Statistical Analysis
3. Results
3.1. Anti-RBD Antibody Levels at Different Time Points
3.2. Clinical Factors Associated with Poor Immunogenicity of Dialysis Patients
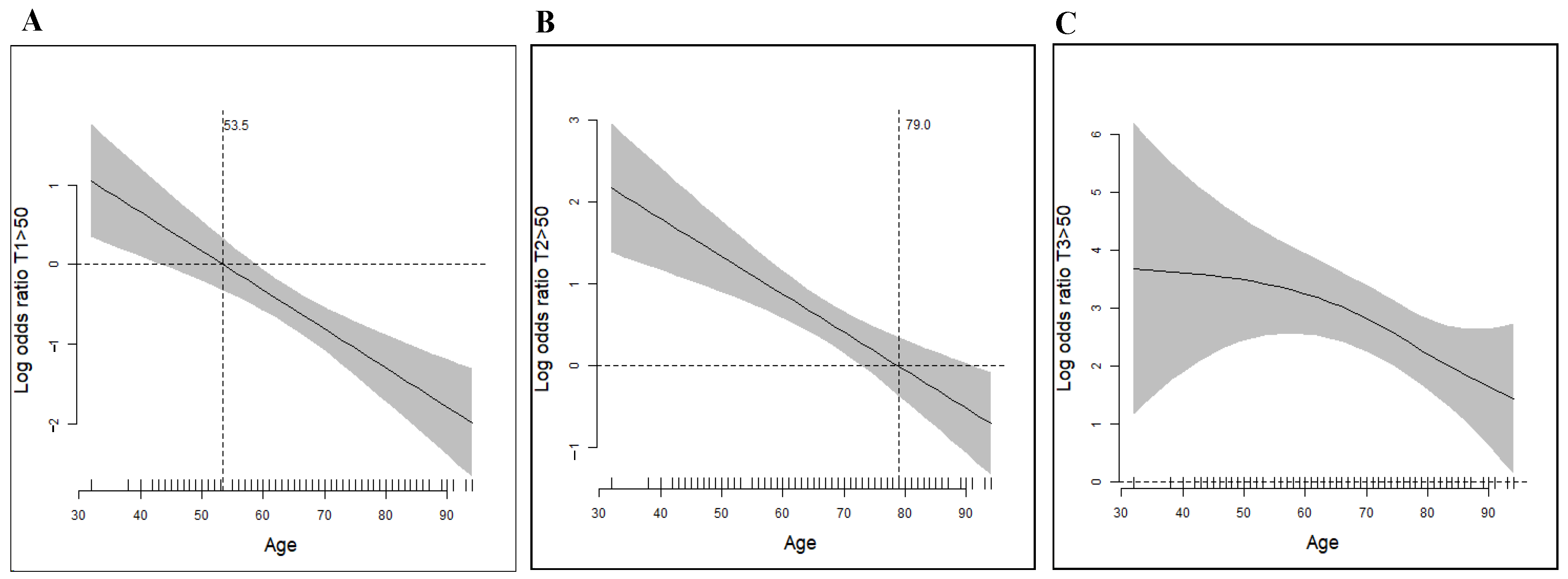
3.2.1. Age Was the Essential Factor Associated with the Vaccine Response
3.2.2. Multinominal Logistic Regression to Evaluate Clinical Factors Associated with Vaccine Response
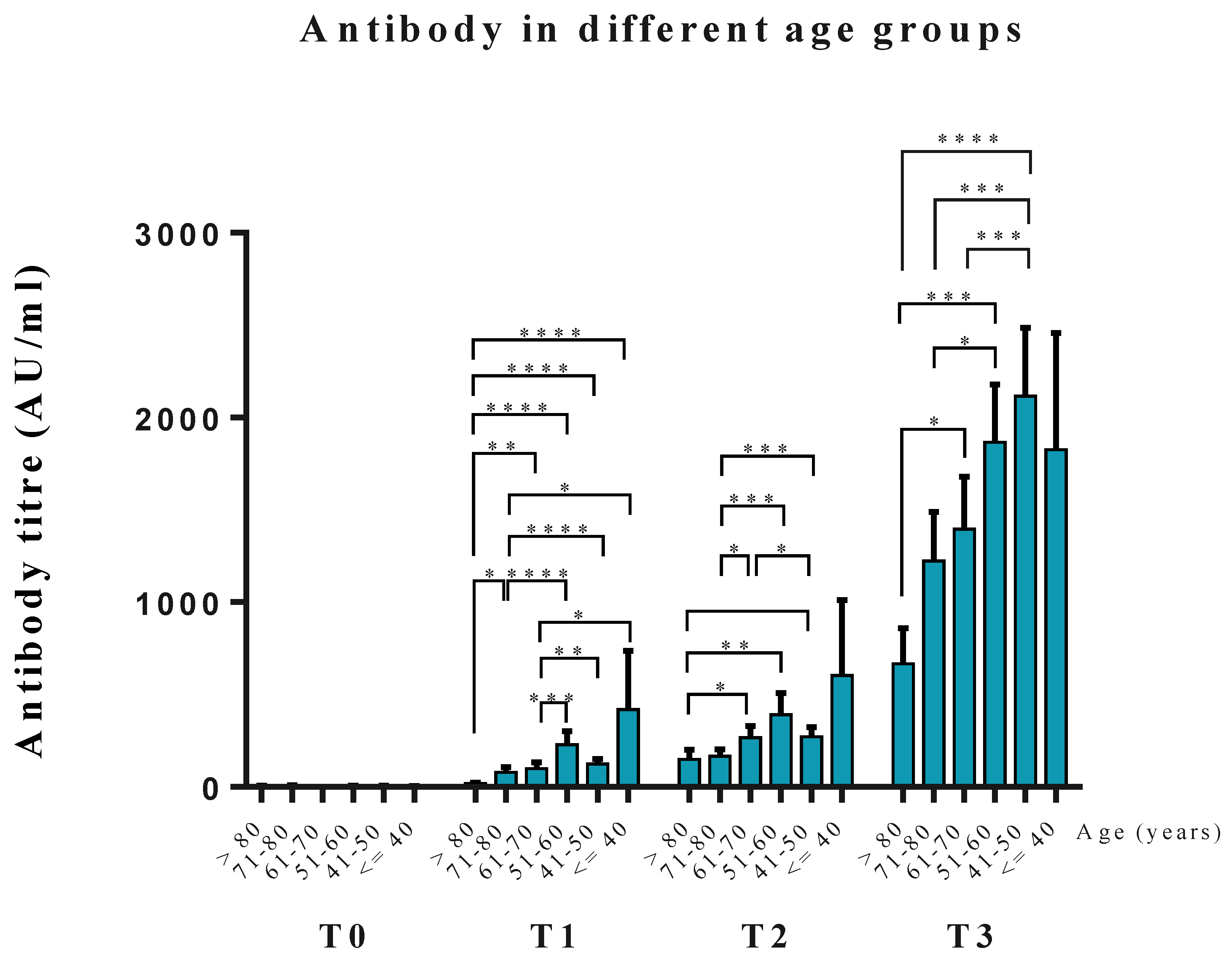
3.3. Anti-RBD Antibody Levels at the Different Age Groups
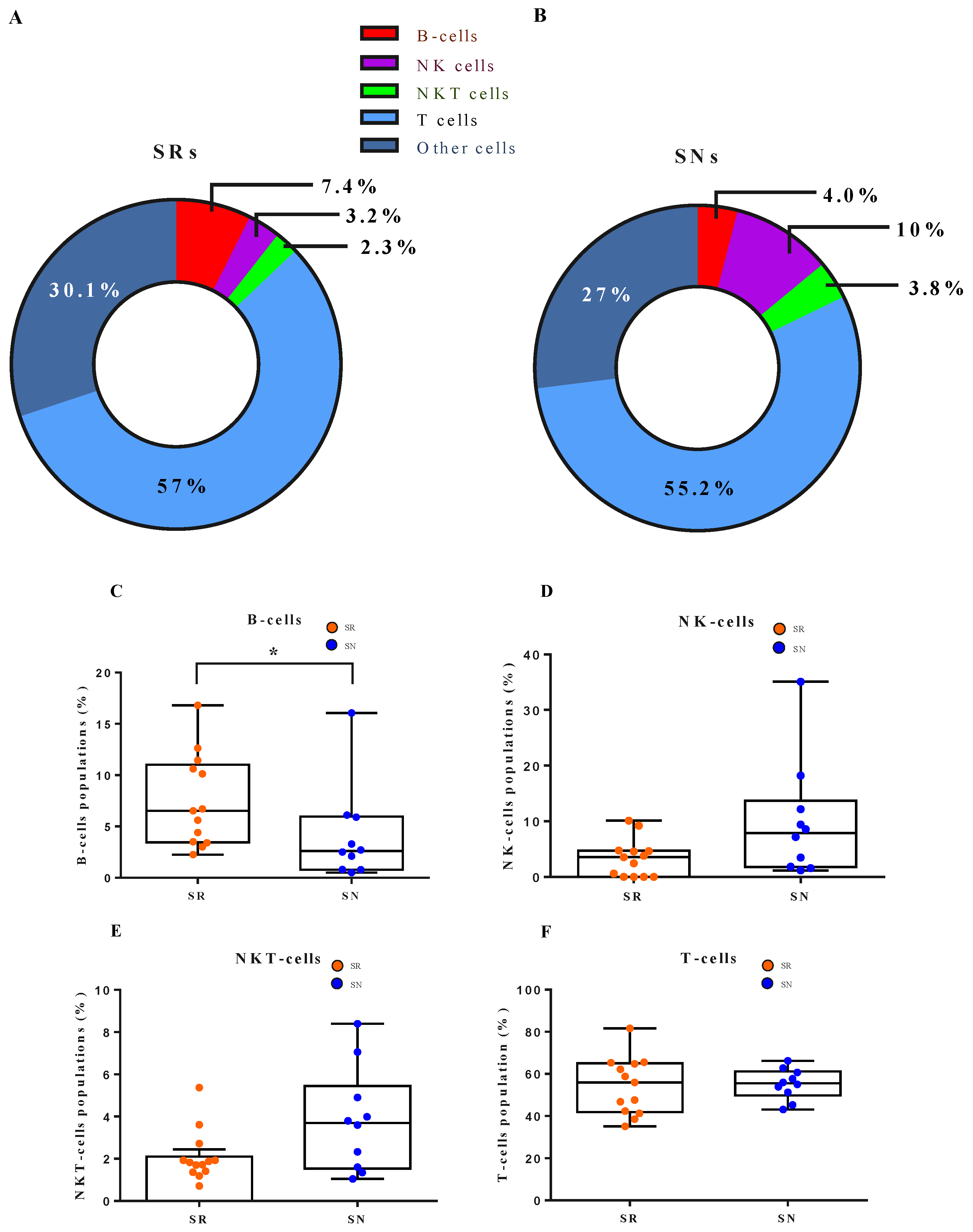
3.4. Cellular Dynamics Underlying B Cell Response to the Vaccine
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Xiong, F.; Tang, H.; Liu, L.; Tu, C.; Tian, J.B.; Lei, C.T.; Liu, J.; Dong, J.W.; Chen, W.L.; Wang, X.H.; et al. Clinical Characteristics of and Medical Interventions for COVID-19 in Hemodialysis Patients in Wuhan, China. J. Am. Soc. Nephrol. 2020, 31, 1387–1397. [Google Scholar] [CrossRef]
- Alberici, F.; Delbarba, E.; Manenti, C.; Econimo, L.; Valerio, F.; Pola, A.; Maffei, C.; Possenti, S.; Lucca, B.; Cortinovis, R.; et al. A report from the Brescia Renal COVID Task Force on the clinical characteristics and short-term outcome of hemodialysis patients with SARS-CoV-2 infection. Kidney Int. 2020, 98, 20–26. [Google Scholar] [CrossRef]
- Corbett, R.W.; Blakey, S.; Nitsch, D.; Loucaidou, M.; McLean, A.; Duncan, N.; Ashby, D.R.; West London Renal and Transplant Centre. Epidemiology of COVID-19 in an Urban Dialysis Center. J. Am. Soc. Nephrol. 2020, 31, 1815–1823. [Google Scholar] [CrossRef]
- Sim, J.J.; Huang, C.W.; Selevan, D.C.; Chung, J.; Rutkowski, M.P.; Zhou, H. COVID-19 and Survival in Maintenance Dialysis. Kidney Med. 2021, 3, 132–135. [Google Scholar] [CrossRef]
- Weiss, S.; Bhat, P.; Del Pilar Fernandez, M.; Bhat, J.G.; Coritsidis, G.N. COVID-19 Infection in ESKD: Findings from a Prospective Disease Surveillance Program at Dialysis Facilities in New York City and Long Island. J. Am. Soc. Nephrol. 2020, 31, 2517–2521. [Google Scholar] [CrossRef]
- Francis, A.; Baigent, C.; Ikizler, T.A.; Cockwell, P.; Jha, V. The urgent need to vaccinate dialysis patients against severe acute respiratory syndrome coronavirus 2: A call to action. Kidney Int. 2021, 99, 791–793. [Google Scholar] [CrossRef]
- Udomkarnjananun, S.; Takkavatakarn, K.; Praditpornsilpa, K.; Nader, C.; Eiam-Ong, S.; Jaber, B.L.; Susantitaphong, P. Hepatitis B virus vaccine immune response and mortality in dialysis patients: A meta-analysis. J. Nephrol. 2020, 33, 343–354. [Google Scholar] [CrossRef]
- Betjes, M.G. Immune cell dysfunction and inflammation in end-stage renal disease. Nat. Rev. Nephrol. 2013, 9, 255–265. [Google Scholar] [CrossRef]
- Windpessl, M.; Bruchfeld, A.; Anders, H.J.; Kramer, H.; Waldman, M.; Renia, L.; Ng, L.F.P.; Xing, Z.; Kronbichler, A. COVID-19 vaccines and kidney disease. Nat. Rev. Nephrol. 2021, 17, 291–293. [Google Scholar] [CrossRef]
- Jahn, M.; Korth, J.; Dorsch, O.; Anastasiou, O.E.; Sorge-Hadicke, B.; Tyczynski, B.; Gäckler, A.; Witzke, O.; Dittmer, U.; Dolff, S.; et al. Humoral Response to SARS-CoV-2-Vaccination with BNT162b2 (Pfizer-BioNTech) in Patients on Hemodialysis. Vaccines 2021, 9, 360. [Google Scholar] [CrossRef]
- Frantzen, L.; Cavaille, G.; Thibeaut, S.; El-Haik, Y. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in a haemodialysis cohort. Nephrol. Dial. Transplant. 2021, 36, 1756–1757. [Google Scholar] [CrossRef]
- Billany, R.E.; Selvaskandan, H.; Adenwalla, S.F.; Hull, K.L.; March, D.S.; Burton, J.O.; Bishop, N.C.; Carr, E.J.; Beale, R.; Tang, J.W.; et al. Seroprevalence of antibody to S1 spike protein following vaccination against COVID-19 in patients receiving hemodialysis: A call to arms. Kidney Int. 2021, 99, 1492–1494. [Google Scholar] [CrossRef]
- Ben Avraham, B.; Crespo-Leiro, M.G.; Filippatos, G.; Gotsman, I.; Seferovic, P.; Hasin, T.; Potena, L.; Milicic, D.; Coats, A.J.S.; Rosano, G.; et al. HFA of the ESC Position paper on the management of LVAD supported patients for the non LVAD specialist healthcare provider Part 1: Introduction and at the non-hospital settings in the community. ESC Heart Fail. 2021, 8, 4394–4408. [Google Scholar] [CrossRef]
- Ducloux, D.; Colladant, M.; Chabannes, M.; Yannaraki, M.; Courivaud, C. Humoral response after three doses of BNT162b2 mRNA COVID-19 vaccine in patients on hemodialysis. Kidney Int. 2021, 100, 702–704. [Google Scholar] [CrossRef]
- Voysey, M.; Costa Clemens, S.A.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Single-dose administration and the influence of the timing of the booster dose on immunogenicity and efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine: A pooled analysis of four randomised trials. Lancet 2021, 397, 881–891. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W.; Jr Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Hin, L.Y.; Lau, T.K.; Rogers, M.S.; Chang, A.M. Dichotomization of continuous measurements using generalized additive modelling--application in predicting intrapartum caesarean delivery. Stat. Med. 1999, 18, 1101–1110. [Google Scholar] [CrossRef]
- Bachelet, T.; Bourdenx, J.P.; Martinez, C.; Mucha, S.; Martin-Dupont, P.; Perier, V.; Pommereau, A. Humoral response after SARS-CoV-2 mRNA vaccines in dialysis patients: Integrating anti-SARS-CoV-2 Spike-Protein-RBD antibody monitoring to manage dialysis centers in pandemic times. PLoS ONE 2021, 16, e0257646. [Google Scholar] [CrossRef]
- Grupper, A.; Sharon, N.; Finn, T.; Cohen, R.; Israel, M.; Agbaria, A.; Rechavi, Y.; Schwartz, I.F.; Schwartz, D.; Lellouch, Y.; et al. Humoral Response to the Pfizer BNT162b2 Vaccine in Patients Undergoing Maintenance Hemodialysis. Clin. J. Am. Soc. Nephrol. 2021, 16, 1037–1042. [Google Scholar] [CrossRef]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Hassan, K.; Shternberg, L.; Alhaj, M.; Giron, R.; Reshef, R.; Barak, M.; Kristal, B. The effect of erythropoietin therapy and hemoglobin levels on the immune response to Engerix-B vaccination in chronic kidney disease. Ren. Fail. 2003, 25, 471–478. [Google Scholar] [CrossRef]
- Moon, S.J.; Lee, S.H.; Byun, Y.H.; Yun, G.Y.; Kim, S.K.; Seong, B.L.; Kim, A.R.; Park, E.S.; Kim, H.J.; Lee, J.E.; et al. Risk factors affecting seroconversion after influenza A/H1N1 vaccination in hemodialysis patients. BMC Nephrol. 2012, 13, 165. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.T.; Guo, C.Y.; Tsai, M.S.; Cheng, Y.Y.; Lin, M.T.; Chen, C.H.; Shen, D.; Wang, J.R.; Sung, J.M. Poor immune response to a standard single dose non-adjuvanted vaccination against 2009 pandemic H1N1 influenza virus A in the adult and elder hemodialysis patients. Vaccine 2012, 30, 5009–5018. [Google Scholar] [CrossRef]
- Calder, P.C. Nutrition, immunity and COVID-19. BMJ Nutr. Prev. Health 2020, 3, 74–92. [Google Scholar] [CrossRef]
- Nurko, S. Anemia in chronic kidney disease: Causes, diagnosis, treatment. Clevel. Clin. J. Med. 2006, 73, 289–297. [Google Scholar] [CrossRef]
- Alavian, S.M.; Tabatabaei, S.V. The effect of diabetes mellitus on immunological response to hepatitis B virus vaccine in individuals with chronic kidney disease: A meta-analysis of current literature. Vaccine 2010, 28, 3773–3777. [Google Scholar] [CrossRef]
- Khan, A.N.; Bernardini, J.; Rault, R.M.; Piraino, B. Low seroconversion with hepatitis B vaccination in peritoneal dialysis patients. Perit. Dial. Int. 1996, 16, 370–373. [Google Scholar] [CrossRef]
- Fabrizi, F.; Dixit, V.; Bunnapradist, S.; Martin, P. Meta-analysis: The dialysis mode and immunological response to hepatitis B virus vaccine in dialysis population. Aliment. Pharmacol. Ther. 2006, 23, 1105–1112. [Google Scholar] [CrossRef]
- Cyster, J.G.; Allen, C.D.C. B Cell Responses: Cell Interaction Dynamics and Decisions. Cell 2019, 177, 524–540. [Google Scholar] [CrossRef] [Green Version]
- Rincon-Arevalo, H.; Choi, M.; Stefanski, A.L.; Halleck, F.; Weber, U.; Szelinski, F.; Jahrsdörfer, B.; Schrezenmeier, H.; Ludwig, C.; Sattler, A.; et al. Impaired humoral immunity to SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients and dialysis patients. Sci. Immunol. 2021, 6, eabj1031. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Minn, D.; Chang, S.-H.; Suh, J.-S. Comparing SARS-CoV-2 Antibody Responses after Various COVID-19 Vaccinations in Healthcare Workers. Vaccines 2022, 10, 193. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 308) | |
|---|---|
| Age ± SD (years) | 65.5 ± 12.38 |
| HD/PD patient numbers | 269/39 |
| Sex (Male/Female) | 189/119 |
| Body weight (kg) | 63.9 ± 13.49 |
| BMI (kg/m2) | 24.16 ± 4.11 |
| Kt/V (HD/PD) | 1.53 ± 0.23/2.06 ± 0.24 |
| URR/WCC (HD/PD) | 72.90 ± 5.32/61.32 ± 16.39 |
| Albumin (g/dL) | 3.84 ± 0.38 |
| Dialysis vintage (Months) | 74.13 ± 69.04 |
| Ferritin (ng/mL) | 437.85 ± 348.88 |
| WBC (×103/μL) | 4.31 ± 3.46 |
| Hemoglobin (g/dL) | 10.34 ± 1.21 |
| Platelet (103/μL) | 178.86 ± 68.11 |
| Sodium (mmol/L) | 136.65 ± 8.33 |
| Potassium (mmol/L) | 4.54 ± 0.75 |
| Calcium (mg/dL) | 9.1 ± 0.81 |
| Phosphate (mg/dL) | 5.02 ± 1.45 |
| Intact PTH (pg/mL) | 409.52 ± 400.71 |
| Triglyceride (mg/dL) | 175.68 ± 131.72 |
| Cholesterol (mg/dL) | 151.32 ± 41.01 |
| GOT (U/L) | 15.78 ± 8.97 |
| GPT (U/L) | 14.29 ± 9.68 |
| Total Bilirubin (mg/dL) | 0.45 ± 0.19 |
| Direct bilirubin (mg/dL) | 0.11 ± 0.10 |
| DM (%) | 152 (49.35%) |
| Hypertension (%) | 247 (80.19%) |
| Variables | Non-Responders vs. Responders | |||
|---|---|---|---|---|
| Univariable | Multivariable | |||
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Age (Years) | 0.948 (0.907–0.990) | 0.015 * | 0.921(0.874, 0.972) | 0.003 * |
| Sex | 2.124 (0.676–6.673) | 0.197 | ||
| BMI (kg/m2) | 0.982 (0.880–1.096) | 0.744 | ||
| BW (kg) | 0.990 (0.958–1.024) | 0.567 | ||
| Dialysis modality (HD/PD) | 2.127 (0.336–13.448) | 0.423 | ||
| GPT (U/L) | 0.974 (0.939–1.010) | 0.153 | ||
| K (mmol/L) | 1.075 (0.556–2.081) | 0.830 | ||
| TG (mg/dL) | 1.002 (0.997–1.007) | 0.351 | ||
| Hb | 1.453 (0.979, 2.158) | 0.064 | 1.756 (1.137, 2.713) | 0.011 * |
| WBC (×103/μL) | 0.982 (0.958–1.007) | 0.159 | ||
| DM | 0.542 (0.195–1.504) | 0.239 | 0.291 (0.089, 0.949) | 0.041 * |
| Kt/V | 4.322 (0.647, 28.897) | 0.131 | ||
| URR | 1.006 (0.952, 1.064) | 0.822 | ||
| Dialysis vintage (months) | 1.001 (0.994–1.008) | 0.793 | ||
| 1st Quartile (<212.5 AU/mL) | 2nd Quartile (212.5–657.0 AU/mL) | 3rd Quartile (657.1–1788 AU/mL) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age (yrs) | 1.11 | 1.06–1.15 | 0.0001 *** | 1.06 | 1.02–1.10 | 0.001 ** | 1.04 | 1.01–1.08 | 0.013 ** |
| Sex | 0.86 | 0.30–2.49 | 0.784 | 1.16 | 0.43–3.16 | 0.766 | 0.60 | 0.22–1.68 | 0.335 |
| BW (kg) | 1.08 | 1.00–1.17 | 0.038 * | 1.01 | 0.95–1.09 | 0.71 | 1.06 | 0.99–1.14 | 0.111 |
| Alb (g/dL) | 1.17 | 0.38–3.61 | 0.791 | 1.12 | 0.37–3.33 | 0.843 | 0.99 | 0.34–2.95 | 0.990 |
| K (mmol/L) | 1.24 | 0.74–2.05 | 0.414 | 1.10 | 0.68–1.79 | 0.689 | 0.96 | 0.59–1.58 | 0.877 |
| TG (mg/dL) | 0.99 | 0.99–1.01 | 0.129 | 0.99 | 0.99–1.01 | 0.206 | 1.01 | 0.99–1.01 | 0.735 |
| GPT (U/L) | 0.98 | 0.95–1.02 | 0.343 | 0.97 | 0.93–1.01 | 0.076 | 0.97 | 0.93–1.01 | 0.108 |
| WBC (×103/μL) | 1.08 | 0.97–1.21 | 0.155 | 1.05 | 0.93–1.18 | 0.458 | 1.08 | 0.96–1.20 | 0.189 |
| Hb (g/dL) | 0.62 | 0.45–0.87 | 0.005 * | 0.81 | 0.60–1.10 | 0.176 | 0.82 | 0.60–1.12 | 0.217 |
| DM | 0.88 | 0.42–1.87 | 0.743 | 1.75 | 0.80–3.47 | 0.170 | 0.88 | 0.43–1.83 | 0.741 |
| Dialysis vintage (months) | 0.99 | 0.99–1.01 | 0.198 | 1.01 | 0.99–1.01 | 0.420 | 0.99 | 0.99–1.01 | 0.229 |
| Kt/V | 1.48 | 0.36–6.08 | 0.589 | 1.14 | 0.30–4.38 | 0.846 | 0.37 | 0.09–1.61 | 0.185 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, C.-Y.; Fang, T.-C.; Liao, H.-W.; Chen, T.-H.; Chang, J.-H.; Lin, Y.-C.; Kao, C.-C.; Liu, M.-C.; Chang, H.-W.; Hung, C.-S.; et al. The Humoral Immune Response of the ChAdOx1 nCoV-19 Vaccine in Maintenance Dialysis Patients without Prior COVID-19 Infection. Vaccines 2022, 10, 338. https://doi.org/10.3390/vaccines10020338
Cheng C-Y, Fang T-C, Liao H-W, Chen T-H, Chang J-H, Lin Y-C, Kao C-C, Liu M-C, Chang H-W, Hung C-S, et al. The Humoral Immune Response of the ChAdOx1 nCoV-19 Vaccine in Maintenance Dialysis Patients without Prior COVID-19 Infection. Vaccines. 2022; 10(2):338. https://doi.org/10.3390/vaccines10020338
Chicago/Turabian StyleCheng, Chung-Yi, Te-Chao Fang, Hung-Wei Liao, Tso-Hsiao Chen, Jer-Hwa Chang, Yen-Chung Lin, Chih-Chin Kao, Ming-Che Liu, Hui-Wen Chang, Ching-Sheng Hung, and et al. 2022. "The Humoral Immune Response of the ChAdOx1 nCoV-19 Vaccine in Maintenance Dialysis Patients without Prior COVID-19 Infection" Vaccines 10, no. 2: 338. https://doi.org/10.3390/vaccines10020338