Article Text

Abstract
Background Bedside lung ultrasound (LUS) is an affordable diagnostic tool that could contribute to identifying COVID-19 pneumonia. Different LUS protocols are currently used at the emergency department (ED) and there is a need to know their diagnostic accuracy.
Design A multicentre, prospective, observational study, to compare the diagnostic accuracy of three commonly used LUS protocols in identifying COVID-19 pneumonia at the ED.
Setting/patients Adult patients with suspected COVID-19 at the ED, in whom we prospectively performed 12-zone LUS and SARS-CoV-2 reverse transcription PCR.
Measurements We assessed diagnostic accuracy for three different ultrasound protocols using both PCR and final diagnosis as a reference standard.
Results Between 19 March 2020 and 4 May 2020, 202 patients were included. Sensitivity, specificity and negative predictive value compared with PCR for 12-zone LUS were 91.4% (95% CI 84.4 to 96.0), 83.5% (95% CI 74.6 to 90.3) and 90.0% (95% CI 82.7 to 94.4). For 8-zone and 6-zone protocols, these results were 79.7 (95% CI 69.9 to 87.6), 69.0% (95% CI 59.6 to 77.4) and 81.3% (95% CI 73.8 to 87.0) versus 89.9% (95% CI 81.7 to 95.3), 57.5% (95% CI 47.9 to 66.8) and 87.8% (95% CI 79.2 to 93.2). Negative likelihood ratios for 12, 8 and 6 zones were 0.1, 0.3 and 0.2, respectively. Compared with the final diagnosis specificity increased to 83.5% (95% CI 74.6 to 90.3), 78.4% (95% CI 68.8 to 86.1) and 65.0% (95% CI 54.6 to 74.4), respectively, while the negative likelihood ratios were 0.1, 0.2 and 0.16.
Conclusion Identifying COVID-19 pneumonia at the ED can be aided by bedside LUS. The more efficient 6-zone protocol is an excellent screening tool, while the 12-zone protocol is more specific and gives a general impression on lung involvement.
Trial registration number NL8497.
- COVID-19
- ultrasound
- thoracic medicine
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study has prospectively compared the diagnostic accuracy of three different lung ultrasound (LUS) protocols in diagnosing COVID-19 pneumonia in a multicentre setting.
All study participants received a regular medical workup (history, physical examination and routine laboratory tests) and a bedside LUS at the emergency department.
LUS findings were classified for the different protocols with prespecified criteria compatible with COVID-19 pneumonia.
Two reference standards for COVID-19 were applied: a positive reverse transcription PCR test and multidisciplinary team of experts’ decision after excluding alternative diagnoses and blinded for LUS results.
Only one physician performed the LUS per patient to minimise infection risk and to avoid unnecessary spending of scarce personal protection material.
Introduction
The COVID-19 pandemic hotspot has moved to less affluent societies with more pronounced socioeconomic disparities and limited medical resources.1 Infected individuals need to be recognised and isolated to slow down the spread. The morbidity and mortality of COVID-19 are most frequently caused by pneumonia and acute respiratory failure with need for supportive medical care.2 3
SARS-CoV-2 reverse transcription PCR is the current gold standard for diagnosing COVID-19. However, PCR has limited sensitivity in daily practice, test capacity is often insufficient, and turnaround time too long to be useful in the emergency department (ED).4 To overcome these limitations, imaging to detect lung involvement has been advocated since this is fast and widely available. Unfortunately, chest X-ray has a poor negative predictive value.5 6 Although CT of the chest does have good diagnostic accuracy, it is not always available in resource constrained areas.5–9 Moreover, an extra risk of cross contamination of healthcare personnel and patients comes along with both radiological techniques. Also, the necessary cleaning procedures are rather time consuming.10
Lung ultrasound could contribute to identification of COVID-19 pneumonia and help guide patient management.11–20 It has proven to reliably exclude COVID-19 pneumonia with equal accuracy to CT of the chest.21–24 Its advantages include: speed, affordability, ease of use, availability in low resource situations (especially handheld devices) and reducing the risk of transmission by minimising the need for patient transport. Cleaning procedures are much easier especially when handheld devices are used.19 20 25
Since the emergence of COVID-19, different lung ultrasound protocols have been used. The current protocols in COVID-19 scan 6,19 8,23 26 1217 18 24 or 1413 15 sites on the thoracic surface. It is unclear which of these protocols is best used in COVID-19.
The 12 and 14 site strategies can be performed within 10 min, while the 6 and 8 site strategies take 3 min at the most. In an overcrowded ED, scanning quickly is most desirable.
To the best of our knowledge, no studies comparing the diagnostic accuracy of different lung ultrasound protocols in pneumonia of any other aetiology have been conducted. The literature on acute heart failure at the ED27 and acute respiratory distress syndrome (ARDS) in the intensive care unit28 have shown that using less scan sites can be equally accurate.
In this real-life, multicentre, observational study, we, therefore assessed and compared the diagnostic accuracy of three commonly used bedside lung ultrasound protocols in identifying COVID-19 at the ED.
Methods
Study protocol
This multicentre, observational study was conducted at the EDs of three academic hospitals in the Netherlands (Radboud University Medical Centre, Nijmegen, and both locations of the Amsterdam University Medical Centers) between 19 March 2020 and 4 May 2020. This study was registered with the Dutch Trial Registry.
Patient and public involvement
There were no patients or public involved in the study protocol.
Design
All eligible patients were 18 years and older who visited the ED with suspected COVID-19. The COVID-19 case definition of the WHO and Dutch centre for disease control (RIVM) was used. This was initially defined as having either fever, malaise, myalgia and respiratory symptoms, and subsequently included gastrointestinal symptoms, loss of smell or taste, and unexplained delirium in the elderly.
Inclusion criteria were a SARS-CoV-2 PCR and verbal informed consent. Exclusion criteria were age under 18 years, no verbal consent given.
All study participants received a regular medical workup (history, physical examination and routine laboratory tests) and a bedside lung ultrasound at the ED. If imaging of the thorax was deemed necessary by the treating physician, a CT of the chest was performed which was in accordance with local clinical guidelines.
In patients with a high clinical suspicion but negative PCR, a diagnosis of COVID-19 still could be made by a multidisciplinary team (MDT) of experts after excluding alternative diagnoses. In all three participating hospitals, it was routine care that the admitted patients were discussed daily in this MDT consisting of consultants in infectious disease, respiratory disease and microbiology. This panel reviewed all available clinical, laboratory, microbiological and CT data, and decided on the final diagnosis. The expert panel was blinded for the lung ultrasound findings during the course of the study.
Ultrasound methods
Bedside lung ultrasound was performed at the ED as an extension of the physical examination. Scans were performed or supervised by acute internal medicine physicians who were certified in point-of-care ultrasound and had entrustable professional activity (EPA) level of 4–5. See online supplemental appendix for an explanation on EPA. All patients received a 12-zone ultrasound and the findings were classified for the different lung ultrasound protocols as described in the paragraphs below. The sonographers performing the lung ultrasound were blinded for the PCR and radiological results.
Supplemental material
Handheld ultrasound systems (Iviz Sonosite and Butterfly IQ Butterfly) were mostly used with a lung pre-set (ie, settings amenable to the detection of B-line artefacts). In case handheld systems were not available a cart-based system was used (Sonosite) with an abdominal preset with tissue harmonic imaging switched off and dynamic range put at the lowest level.
Twelve-zone method
Scanning was done in a lawn mower fashion with six scanning sites on each hemithorax: two anteriorly, two laterally and two posteriorly. See figure 1 for details on the scanning zones and technique. Images of the 12 scanning zones are available in the online supplemental appendix. The ultrasound was assessed real-time as positive or negative for COVID-19. A scan was defined positive by the presence of sonographic abnormalities consistent with COVID-19 in two or more zones unilaterally, or one or more zones bilaterally (see online supplemental table 1:18 for typical sonographic findings in COVID-19 pneumonia).

Example is demonstrated by a volunteer. Scanning zones in the 12-zone method. Z1–Z6 are the six zones on each hemithorax together forming 12 zones. Anterior (A): Z1–Z2; lateral (B): Z3–Z4; posterior (C): Z5–Z6. Red-coloured lines depict the lawn mower technique. AAL, anterior axillary line; PAL, posterior axillary line.
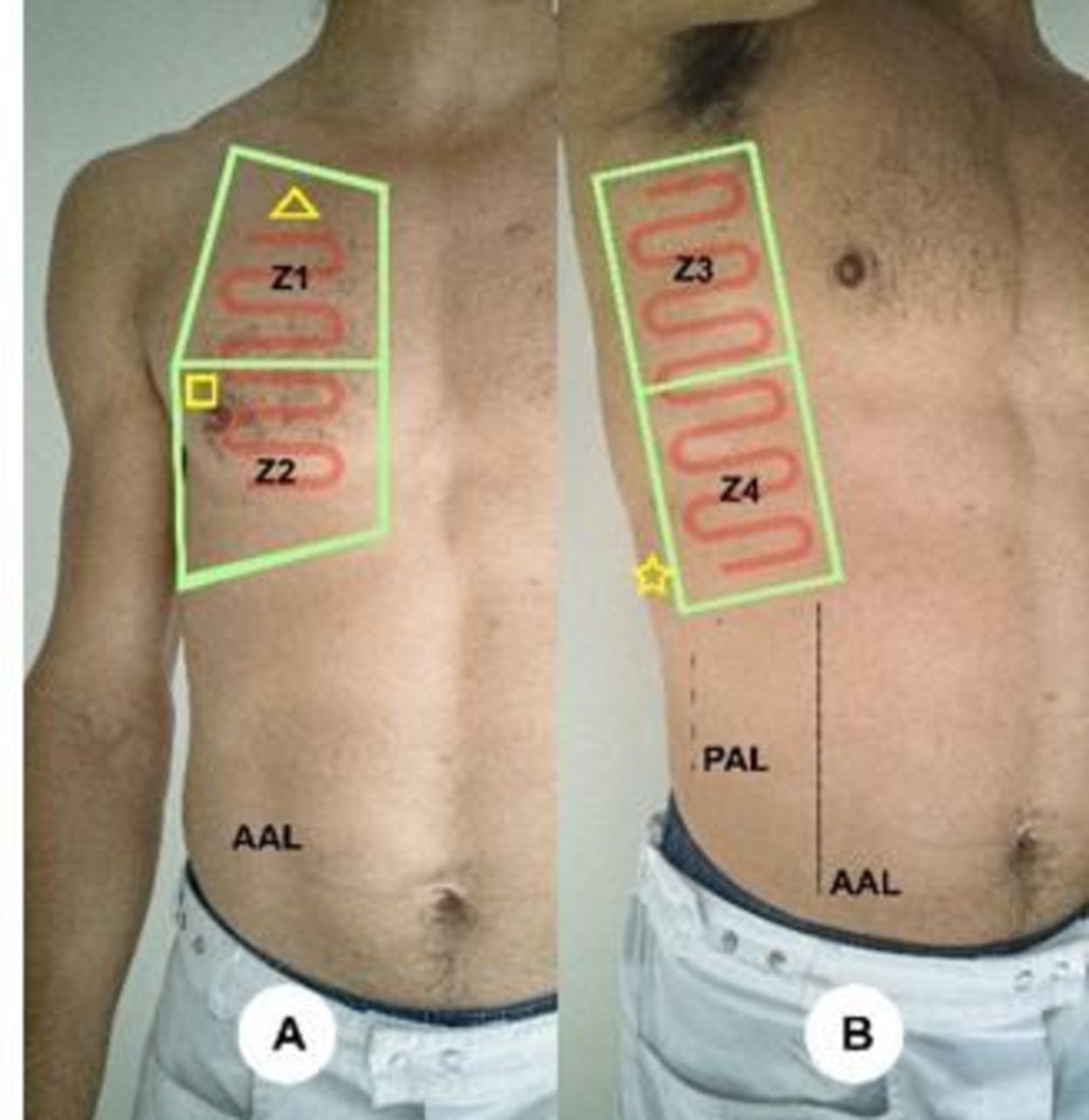
Six-points method (BLUE protocol)
This protocol is an acronym for bedside lung ultrasound in emergency (BLUE) and categorises the lung ultrasound findings into BLUE profiles.29 30 Three sites on each hemithorax are scanned: the upper BLUE point, lower BLUE point and the posterior lateral alveolar pulmonary syndrome point (PLAPS). See figure 2 for details on the scanning zones. The BLUE profile was determined real time. Based on the features and distribution of COVID-19 pneumonia, the following BLUE profiles were considered consistent with COVID-19 pneumonia:
A-profile with bilateral PLAPS without pleural effusion.
A/B-profile.
B’-profile.
C-profile.

Example is demonstrated by a volunteer. Scanning zones in the six-points method. Yellow symbols are the three points on each hemithorax together forming six points. Yellow triangle: upper BLUE point; yellow square: lower BLUE point; yellow star: PLAPS point. AAL, anterior axillary line; BLUE, bedside lung ultrasound in emergency; PAL, posterior axillary line; PLAPS, posterior lateral alveolar pleural syndrome.
Profiles that were deemed not in keeping with COVID-19 were:
A-profile without PLAPS (asthma/Chronic Obstructive Pulmonary Disease, pulmonary embolism and non-pulmonary conditions).
A-profile with unilateral PLAPS (lobar pneumonia).
A-profile with bilateral PLAPS due to pleural effusion (heart failure).
B-profile (heart failure).
Eight-points method
Scanning is done at four sites on each hemithorax: two anterior and two lateral. See figure 3 for details on the scanning zones. A positive scan was defined by the presence of at least one of the artefacts described (online supplemental table 1) in one or more zones bilaterally or two or more zones unilaterally.

{kind=link}
{kind=link}
{kind=link}
Example is demonstrated by a volunteer. Scanning zones in the eight-points method. Z1–Z4 are the four zones on each hemithorax together forming eight zones. Anterior: Z1–Z2; lateral: Z3–Z4. AAL, anterior axillary line; PAL, posterior axillary line.
Outcome
Sensitivity, specificity, diagnostic accuracy and predictive values of three different lung ultrasound protocols in COVID-19 were assessed against two reference standards: (serial) PCR (gold standard) and the final diagnosis.
Statistical analysis
No sample size calculation was performed. Normally distributed continuous variables are summarised by their mean and SD. Continuous variables that are not normally distributed are summarised by their median and IQR. Differences between patient groups were tested using the independent t-test for normally distributed outcomes and difference in means and 95% CI were calculated. The widths of the intervals have not been adjusted for multiplicity, inferences drawn may, therefore, not be reproducible. Non-parametric Mann-Whitney U test was used to compare continuous outcomes that were not normally distributed between groups. Sensitivity and specificity of the different lung ultrasound protocols were compared using the McNemar test.
Analyses were performed in SPSS V.26. Data were analysed by the first four authors: BK, FS, AL and KA.
Results
From 19 March 2020 until 4 May 2020, 202 patients with a suspicion of COVID-19 were included in our study. There were neither missing data, nor adverse events. See table 1 for patient demographics and clinical characteristics.
Patient demographics and clinical characteristics
The descriptive statistics of the lung ultrasound protocols are given in tables 2 and 3.
Descriptive statistics of the three lung ultrasound protocols vs SARS-CoV-2 PCR
Descriptive statistics of the three lung ultrasound protocols vs final diagnosis
The following diagnostic measures for the different protocols compared with PCR were found. For 12-zone ultrasound, we found a sensitivity of 91.4% (95% CI 84.4 to 96.0), specificity of 83.5% (95% CI 74.6 to 90.3), negative predictive value of 90.0% (95% CI 82.7 to 94.4) and negative likelihood ratio of 0.1 (95% CI 0.05 to 0.2). For the 6-points protocol, we found a sensitivity of 89.9% (95% CI 81.7 to 95.3), specificity of 57.5% (95% CI 47.9 to 66.8), negative predictive value of 87.8% (95% CI 79.2 to 93.2) and negative likelihood ratio of 0.2 (95% CI 0.1 to 0.3). For the 8-points method, we found a sensitivity 79.7% (95% CI 69.9 to 87.6), specificity of 69.0% (95% CI 59.6 to 77.4), negative predictive value of 81.3% (95% CI 73.8 to 87.0) and negative likelihood ratio of 0.3 (95% CI 0.2 to 0.5).
We also calculated diagnostic measures compared with the final diagnosis decided by the medical expert panel. Ninety six patients with a final diagnosis of COVID-19 had a positive 12-zone lung ultrasound. The statistical results were as follows.
The 12-zone lung ultrasound protocol had a sensitivity of 91.4% (95% CI 84.4 to 96.0), specificity of 83.5% (95% CI 74.6 to 90.3), negative predictive value of 90.0% (95% CI 82.7 to 94.4) and negative likelihood ratio of 0.1 (95% CI 0.05 to 0.2). The 6-points protocol had a sensitivity of 89.5 (95% CI 82.0 to 94.7), specificity of 65.0% (95% CI 54.6 to 74.4), negative predictive value of 85.1% (95% CI 76.3 to 91.1) and negative likelihood ratio of 0.16 (95% CI 0.09 to 0.3). The 8-points method had a sensitivity of 81.0% (95% CI 72.1 to 88.0), specificity of 78.4% (95% CI 68.8 to 86.1), negative predictive value of 79.2% (95% CI 71.7 to 85.1) and negative likelihood ratio of 0.2 (95% CI 0.2 to 0.4). Comprehensive results are shown in table 2.
The inter-observer reliability of 12-zone lung ultrasound was excellent, with an intraclass correlation coefficient of 0.88 (95% CI 0.77 to 0.95).
Six patients had false negative results in the 12-zone scan and thus also in the 6-points and 8-points protocols. In four of these patients, ultrasound abnormalities were seen in one zone only. Therefore, the results were not compatible with the prespecified criteria for a positive ultrasound scan. In the remaining two patients, no abnormalities were seen at all.
Three patients had false negative results in the six-points protocol. One of these was falsely negative in the eight-points protocol too. All three false negative ultrasounds had abnormalities visualised in one zone only (eg, BLUE profile A with unilateral PLAPS or only one site in the eight-points protocol). As such, they were not in keeping with COVID-19 pneumonia. However, if the 12-zone protocol was applied, all three ultrasounds were positive.
Eleven patients had a false negative ultrasound in the 8-points protocol but not in the 6-points or 12-zone protocol.
Twenty nine patients had a false positive ultrasound in the 12-zone protocol. Further analysis of these 29 scans showed that 22 ultrasounds were falsely positive in all three protocols, 6 recordings in the 12-zone protocol and 1 other protocol (5/6 also in the 6-points protocol and 1/6 also in the 8-points protocol) and 1 false positive scan in the 12-zone protocol only.
Twenty three patients had a false positive ultrasound in one or both of the six-points and eight-points protocols but not in the 12-zone approach. Twelve scans were solely false positive in the six-points method and two scans were false positive in the eight-points method only. The remaining nine false positive ultrasounds were considered as such in both the six-points and eight-points protocols.
Discussion
Screening
The findings in our study show that the 6-points protocol and the 12-zone approach can reliably and safely rule out COVID-19 pneumonia. Our study also shows that one must convert to a complete 12-zone ultrasound in case any abnormalities are seen in the six-points method. Application of this approach will minimise the chance of a false negative ultrasound in the six-points protocol.
In our study, the three false negatives in the six-points protocol had the BLUE-profile A with unilateral PLAPS, which is suggestive of lobar pneumonia.29 30 If the ultrasound examination was extended to a 12-zone scanning, all three scans would have been ruled in. On the contrary, the absence of any abnormality in the six-points protocol safely rules out COVID-19 pneumonia. In our study, this was shown by the excellent negative predictive values of the 12-zone and 6-points protocols. Importantly, patients who were COVID-19 positive with false negative results in the six-points protocol had no need for admission due to COVID-19-related symptoms.
Conversely, in our study, the eight-points scanning method resulted in missing patients in whom supportive care was necessary. The lower sensitivity of this approach could be explained by the fact that scanning of the posterior chest is omitted. In COVID-19 pneumonia, abnormalities tend to originate inferior posterior. Our results indicate that zone six (named PLAPS in the BLUE protocol) should be examined to have a high negative predictive value.
Although scanning this zone can sometimes be challenging in immobile, obese and bedridden patients, a supine patient can still be examined by adduction of the arm across the midline and thereby exposing the back of the chest.
Diagnosing
The specificities of the lung ultrasound protocols in our study are substantially lower than found in the literature on pneumonia.29–34 For example, findings which we considered suggestive of COVID-19 pneumonia in the six-points and eight-points protocols were in fact compatible with lobar pneumonia, heart failure with pleural effusion, compression atelectasis or progression of intrapulmonary malignancy.
The suboptimal specificity of the six-points and eight-points protocol are inherent to their limited scanning area. COVID-19 pneumonia has a patchy and irregular distribution. In the six-points protocol, too few zones are scanned to have a good overview, which improves the specificity of lung ultrasound. Also, COVID-19 pneumonia tends to begin inferior posterior, but this holds also true for pleural effusion and compression atelectasis. In the eight-points protocol, there is no visualisation of this area and thus valuable information which increases specificity is missed. In summary, our study has shown that a 12-zone lung ultrasound yields the highest specificity to diagnose COVID-19 pneumonia compared with the six-points and eight-points protocols.
Nevertheless, the limited specificity of lung ultrasound is inherent to COVID-19 pneumonia, which does not cause a pathognomonic picture, but rather one similar to other viral pneumonias, inflammatory pneumonitis and ARDS.
Perspectives
Bedside ultrasound could contribute in identifying COVID-19 pneumonia and guide on patient management. Screening for signs of COVID-19 pneumonia will only take 3 min with an excellent negative predictive value, and when a 12-zone ultrasound is necessary, this will take 10 min after which useful information to guide on patient management is obtained. Also, this technique comes along with less exposure of healthcare personnel and other patients to a patient with COVID-19 because of its use directly at the bedside. Most importantly, bedside lung ultrasound can be available in resource constrained areas even off the grid when handheld ultrasound devices are used.
Limitations
This multicentre study has numerous limitations. As all patients were scanned using the 12-zone protocol, the diagnostic measures calculated in the six-points and eight-points protocols can be overrated. Because we applied a lawn mower technique, more positive findings were seen in the six-points protocol when compared with a strict adherence to the anatomical points described in this protocol. In our opinion, a too rigid adherence to exact anatomical points is a false interpretation and will result in a decrease in diagnostic accuracy, especially in a disease with a patchy and irregular pattern like COVID-19 pneumonia. Only one physician performed the lung ultrasound per patient. Hospital protocol did not allow the same patient to be scanned by three separate physicians, to minimise infection risk and to avoid unnecessary spending of scarce personal protection material. Since all the scanning was performed and recorded systematically in 12 separate images, we consider the influence on the classification of the six-points and eight-points protocols as minimal. Moreover, the same methodology was used in research to compare different ultrasound protocols in heart failure and deep vein thrombosis.27 35 36
The diagnostic accuracy measures found in this study are subject to a possible attention bias due to the high prevalence setting in which we performed our study. Lung ultrasound has an excellent negative predictive value and sensitivity to screen for possible COVID-19. However, we advocate future research on this subject in low prevalence setting.
In this study, we applied two reference standards for COVID-19: (serial) PCR (gold standard) and the final diagnosis. The latter was a positive decision made by an MDT expert based on clinical information, microbiological, RT-PCR SARS-COV-2 and CT of the chest data. This approach reflects daily practice and has the advantages of detecting patients with COVID-19 with false negative RT-PCR results, and being applicable in circumstances where RT-PCR data are not readily available. This approach is advocated by the WHO. From a methodological viewpoint, the comparison between a molecular diagnosis of COVID-19 (RT-PCR) and imaging to detect COVID-19 pneumonia is an incongruence. Still, pneumonia and its sequalae are the majority of COVID-19’s morbidity and mortality and thus we feel the combination suits better in day to day care. For clarity reasons, we reported the comparison between lung ultrasound and RT-PCR, and the comparison between lung ultrasound and MDT decision separately. The results of both comparisons are, respectively, listed in tables 2 and 3.
Importantly, regardless of the reference chosen, the findings in our study remain the same.
We have used various ultrasound systems (mostly handheld). Although this causes heterogeneity, it does reflect daily clinical practice and thus adds to the generalisability of our findings.
Conclusion
Identifying COVID-19 at the ED can be aided by bedside lung ultrasound. A 3-minute scan of the six lung zones can safely rule out COVID-19 pneumonia. The 12-zone scanning protocol is the only protocol that is specific enough to diagnose COVID-19 pneumonia at the ED in a high prevalence setting. We recommend further research be conducted in other settings to validate our findings.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Medical Ethical Committee (CMO region Arnhem-Nijmegen) with reference number 2020-6372.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
BK, FS and AL contributed equally.
Contributors BK, FS, AL, PWBN and FB were involved in developing the research plan and study design. BK, FS and AL collected the data and entered the data in the database an drafted the paper. BK, FS, AL and KA analysed the data. All authors critically appraised the paper, revised where appropriate and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.