


Myocarditis after receiving an mRNA vaccine against SARS-CoV-2 is a rare but recognized complication.
Myocarditis after SARS-CoV vaccination tends to be mild and occurs predominantly in young people.
We present a case of severe myocarditis in a middle-aged woman that required extracorporeal membrane oxygenation support and that appeared to respond to steroid treatment.
Despite the possibility of this severe adverse reaction, the benefits of vaccination against SARS-CoV-2 far outweigh the risks.
A 49-year-old woman with a history of hypothyroidism and drug allergies (to penicillin, meperidine and sulfonamides) causing rash presented to an emergency department with chest discomfort and worsening dyspnea 6 days after a SARS-CoV-2 mRNA-BNT162b2 (Pfizer–BioNTech) vaccine. She had received her first dose with the adenoviral vector AZD1222 ChAdOx1 nCOV-19 (AstraZeneca) vaccine 8 weeks previously. She had not had any allergic reactions to previous vaccines, did not use recreational drugs and had no history of SARS-CoV-2 infection.
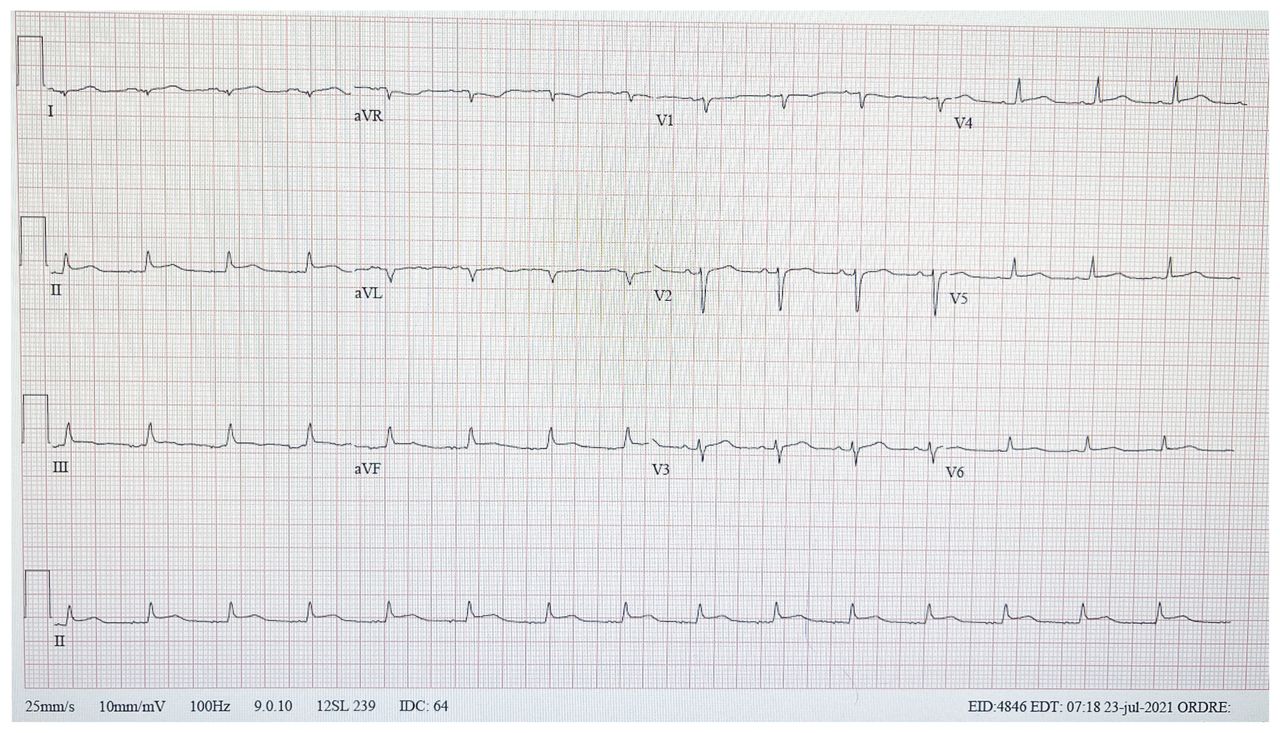
In the emergency department, the patient initially appeared to be in no acute distress, with a normal physical examination. The results of her blood work are shown in Table 1. A nasopharyngeal polymerase chain reaction (PCR) test for SARS-CoV-2 was negative. Electrocardiography showed diffuse ST-T wave elevation with incomplete left bundle branch block (Figure 1); the left ventricular ejection fraction (LVEF) was normal on echocardiography. Coronary angiography was performed about 30 hours after presentation and showed normal coronary arteries.
Laboratory investigations

Electrocardiogram of a 49-year-old woman with myocarditis, showing diffuse ST-T elevation with incomplete left bundle branch block.
A presumptive diagnosis of myopericarditis was made based on evidence of myocardial injury on the electrocardiogram, mildly elevated troponin levels, leukocytosis, the increased C-reactive protein level and the normal coronary angiogram. Less than 24 hours after presentation, the patient had a ventricular fibrillation cardiac arrest, was resuscitated and urgently transferred to our hospital.
The patient appeared ill upon arrival, with signs of low cardiac output and pulmonary congestion despite being supported by norepinephrine and milrinone perfusion. Her temperature was 36.8°C, her heart rate was 75 beats/min, her blood pressure was 100/60 mm Hg, her oxygen saturation was 95% on room air and her respiratory rate was 28 breaths/min. We heard a third heart sound but no murmur. Jugular venous pressure was elevated and urine output was reduced (10 mL/h). A repeat echocardiogram showed severe biventricular dysfunction, markedly increased cardiac wall thickness (suggestive of edema) and a small pericardial effusion (Appendix 1, Video 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.211687/tab-related-content). Despite escalation of inotropic support, the patient’s clinical condition worsened, with arrhythmic instability and recurrent ventricular fibrillation cardiac arrest. We intubated her and administered intravenous methylprednisolone (1000 mg/d for 3 d) for possible giant cell or autoimmune myocarditis, given her fulminant course. We started peripheral venoarterial extracorporeal membrane oxygenation (VA-ECMO) about 48 hours after initial presentation. We performed a right ventricle endomyocardial biopsy under ECMO support, which showed cardiomyocyte damage with moderate inflammatory infiltrates composed of small lymphocytes, macrophages and eosinophils, consistent with a diagnosis of eosinophil-rich lymphocytic myocarditis (Figure 2). We did not observe any large areas of myocyte necrosis, granulomas or giant cells.
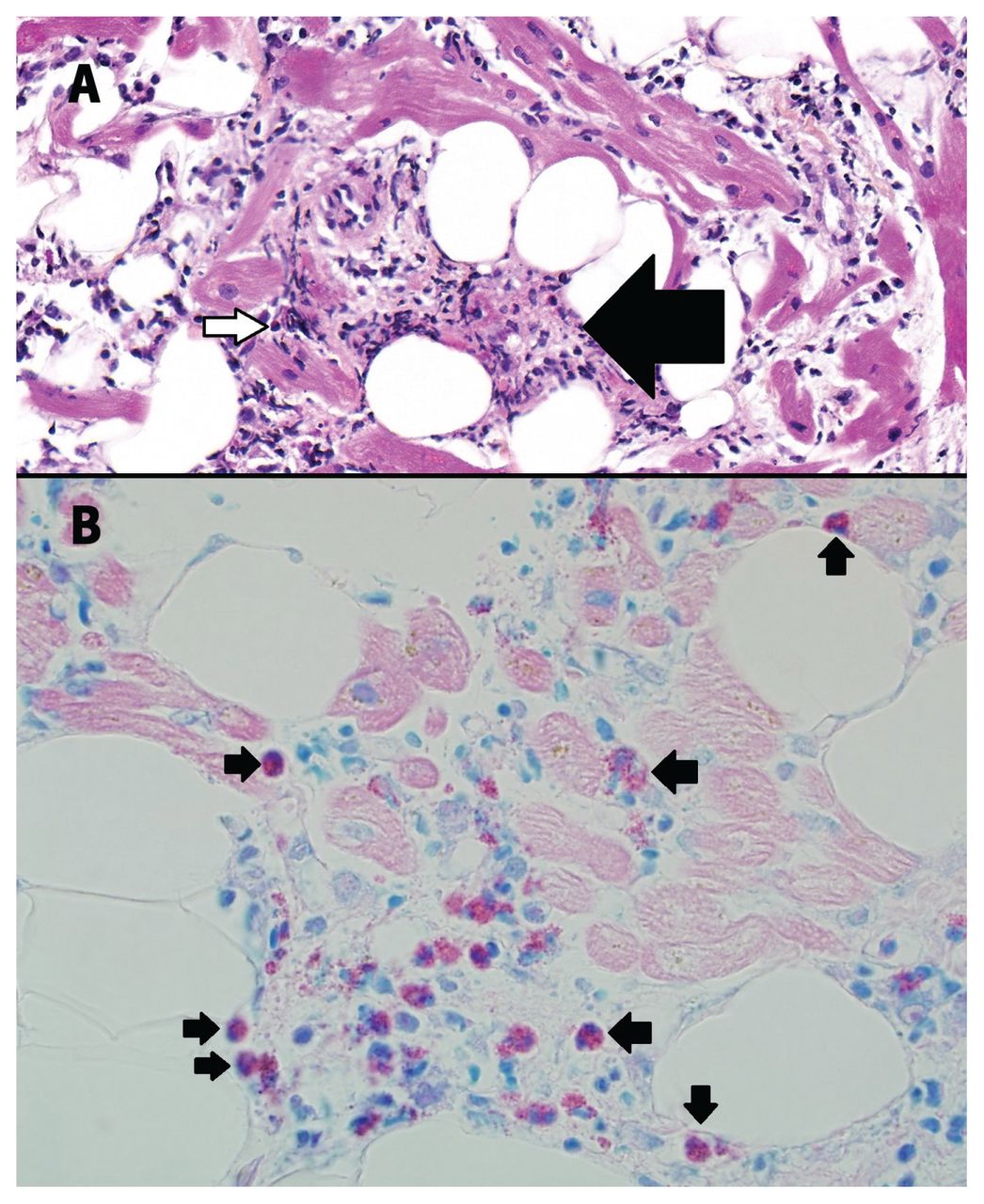
Histopathological findings from an endomyocardial biopsy from our patient’s right ventricle, showing eosinophil-rich lymphocytic myocarditis. Samples were stained with CD3, CD20, CD138, CD68, Giemsa, Iron stain, Congo red and sulfated Alcian blue. The sample stained in CD3 was positive for T-cell lymphocytes, whereas CD68 staining highlighted macrophages. CD20 and CD138 staining did not show B-cell lymphocytes or plasma cells. Giemsa stain showed red intracytoplasmic granules in eosinophils. Iron stain, Congo red and sulfated Alcian blue were negative for amyloid and iron overload. (A) Cardiomyocyte damage with moderate inflammatory infiltrate, composed of small lymphocytes, macrophages (arrow) and eosinophils (white arrow) (hematoxylin and eosin stain with 400 × magnification). (B) Red intracytoplasmic granules, indicating numerous eosinophils (arrows; Giemsa stain with 400 × original magnification).
The patient’s hospital course was complicated by acute kidney injury requiring renal replacement therapy, and ventilator-associated pneumonia. An enzyme-linked immunosorbent assay was positive for immunoglobulin (Ig) G antibodies against SARS-CoV-2 but negative for IgM, indicating previous vaccination and no acute infection. Several nasal PCR tests were negative for SARS-CoV-2. An autoimmune screening panel was negative. We stopped the ECMO on day 5; the patient’s cardiac wall thickness had normalized and her LVEF improved to 40% (Appendix 2, Video 2, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.211687/tab-related-content). We successfully extubated her and tapered the corticosteroids. However, she developed a generalized multiform erythematous rash and high eosinophil count (5.68 [normal 0.02–0.50] × 109/L). We restarted corticosteroids and the rash resolved within 24 hours.
We transferred the patient to a rehabilitation centre 35 days after her initial presentation. At transfer, she was taking oral prednisone (15 mg/d) and her eosinophil count had normalized.
Discussion
Our patient presented with features typical of hypersensitivity myocarditis after receiving an mRNA vaccine as her second dose against SARS-CoV-2.1 Unlike previous reports of myocarditis, mostly among young men,2 our patient was a middle-aged woman who had received a mixed vaccine regimen and developed cardiogenic shock requiring ECMO support.
Although myocarditis typically occurs within a week after mRNA-COVID-19 vaccination,3–10 delayed localized skin hypersensitivity reactions have been described a median of 7 days after vaccination. Few histopathological reports of patients with myocarditis after mRNA-SARS-CoV-2 vaccination have been published. In mild cases, nonspecific changes without infiltrates suggestive of active inflammation have been found at endomyocardial biopsy, raising the possibility of a sampling error owing to patchy infiltration.3,9 In 2 patients with cardiogenic shock, histopathology showed multifocal cardiomyocyte damage, with mixed infiltration of macrophages, T cells, eosinophils and B cells, suggesting an antibody-mediated mechanism.11 Like our patient, and in contrast to milder cases, these patients were middle-aged (a 45-year-old woman and a 42-year-old man), developed symptoms later (10 d after her first dose and 14 d after his second dose, respectively) and received only mRNA vaccines. One patient recovered completely after 2 weeks of inotropic support and treatment with corticosteroids, but the other died within 3 days of clinical presentation.11
Given the temporal relation between our patient’s symptoms and the administration of the SARS-CoV-2 vaccine, and the pathology findings, it is probable that her condition was etiologically related to the vaccine.12 Her score on the Naranjo Adverse Drug Reaction Probability Scale was 7 (https://www.evidencio.com/models/show/661; Appendix 3, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.211687/tab-related-content), suggesting a probable adverse drug reaction (score 5–8).
The patient’s endomyocardial biopsy findings were consistent with a diagnosis of hypersensitivity myocarditis, despite little necrosis, as may have been expected in such a fulminant presentation. Potential explanations for the lack of necrosis include the short time between cardiogenic shock and biopsy (< 12 h), such that myocardial necrosis had not yet occurred; sampling error, as patchy myocardial damage was seen on the cardiac magnetic resonance imaging that was performed later; or, less likely, extremely rapid response to high-dose corticosteroid treatment.13 Hypersensitivity myocarditis with a fulminant course may be a rapidly fatal manifestation of drug rash with eosinophilia and systemic symptoms (DRESS) syndrome, which can occur after any drug administration, including vaccines.13 Peripheral eosinophilia and cutaneous rash at presentation are typical, but cardiac involvement is uncommon; when it occurs, myocyte necrosis and eosinophilic infiltrates are found on endomyocardial biopsy, and treatment requires aggressive immunosuppression. 13 Although our patient did not initially exhibit all features typical of DRESS (Box 1), the temporal association between her symptom onset, mRNA SARS-CoV-2 vaccination and eosinophil-rich lymphocytic myocarditis suggests an autoreactive T-cell mechanism against the myocardium, perhaps by increased expression of cardiac autoantibodies specific to human leukocyte antigen after immunization in genetically predisposed patients.13
Criteria for diagnosis of drug rash with eosinophilia and systemic symptoms (DRESS)
Diagnosis is confirmed by the presence of 7 of the following criteria:
Maculopapular rash developing > 3 weeks after starting with the suspected drug
Prolonged clinical symptoms 2 weeks after discontinuation of the suspected drug
Fever > 38°C
Liver abnormalities (alanine transferase > 100 U/L)
Leukocytosis > 11 × 109/L
Atypical lymphocytosis > 5%
Eosinophilia > 1.5 × 109/L
Lymphadenopathy
Human herpesvirus 6 reactivation
Adapted from Shiohara and Mizukawa14 using the Creative Commons Attribution (CC BY-NC-ND 4.0) licence.
Although the role of corticosteroid treatment in acute myocarditis is controversial, it might be considered in patients with a fulminant presentation or when autoimmune myocarditis is suspected. 13 Corticosteroids seemed beneficial in our patient, as well as for another patient in a recent report;11 a prolonged taper of corticosteroids may be considered in some cases.
Previous reports did not describe their patients’ detailed vaccination regimen, but most cases occurred a few days after a second dose of an mRNA vaccine against SARS-CoV-2. Whether the use of an adenovirus-based vaccine for the patient’s first dose, followed by a second dose using an mRNA vaccine, played a role in our patient’s fulminant presentation by triggering a stronger immunologic response is unknown, but warrants surveillance as many countries have adopted such a regimen, including the United Kingdom and United States (for the Johnson & Johnson adenoviral vaccine). Observational data suggest that this regimen provides a good safety profile, with a more robust humoural and cellular immunity than the homologous mRNA vaccine schedule,15 but also a higher rate of common adverse effects, possibly by a synergistic mechanism. Finally, it is possible that our patient had a systemic overreaction, resulting from the interplay between activation of proinflammatory cascades and immunological pathways (type IV hypersensitivity reaction) induced by the heterologous vaccination treatment and genetic predisposition.16
A fulminant presentation of myocarditis after SARS-CoV-2 vaccination is very rare and the remarkable efficacy of vaccines at preventing severe COVID-19 means that their benefits clearly outweigh their risks.
Videos of perioperative transesophageal echography of a 49-year-old woman with myocarditis are available in Appendix 1 and Appendix 2, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.211687/tab-related-content.
The section Cases presents brief case reports that convey clear, practical lessons. Preference is given to common presentations of important rare conditions, and important unusual presentations of common problems. Articles start with a case presentation (500 words maximum), and a discussion of the underlying condition follows (1000 words maximum). Visual elements (e.g., tables of the differential diagnosis, clinical features or diagnostic approach) are encouraged. Consent from patients for publication of their story is a necessity. See information for authors at www.cmaj.ca.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
Contributors: All of the authors contributed to the conception and design of the work, drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
{kind=link}
Article extras
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

