
SARS-CoV-2 Seroprevalence in Healthcare Workers in Germany: A Follow-Up Study

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
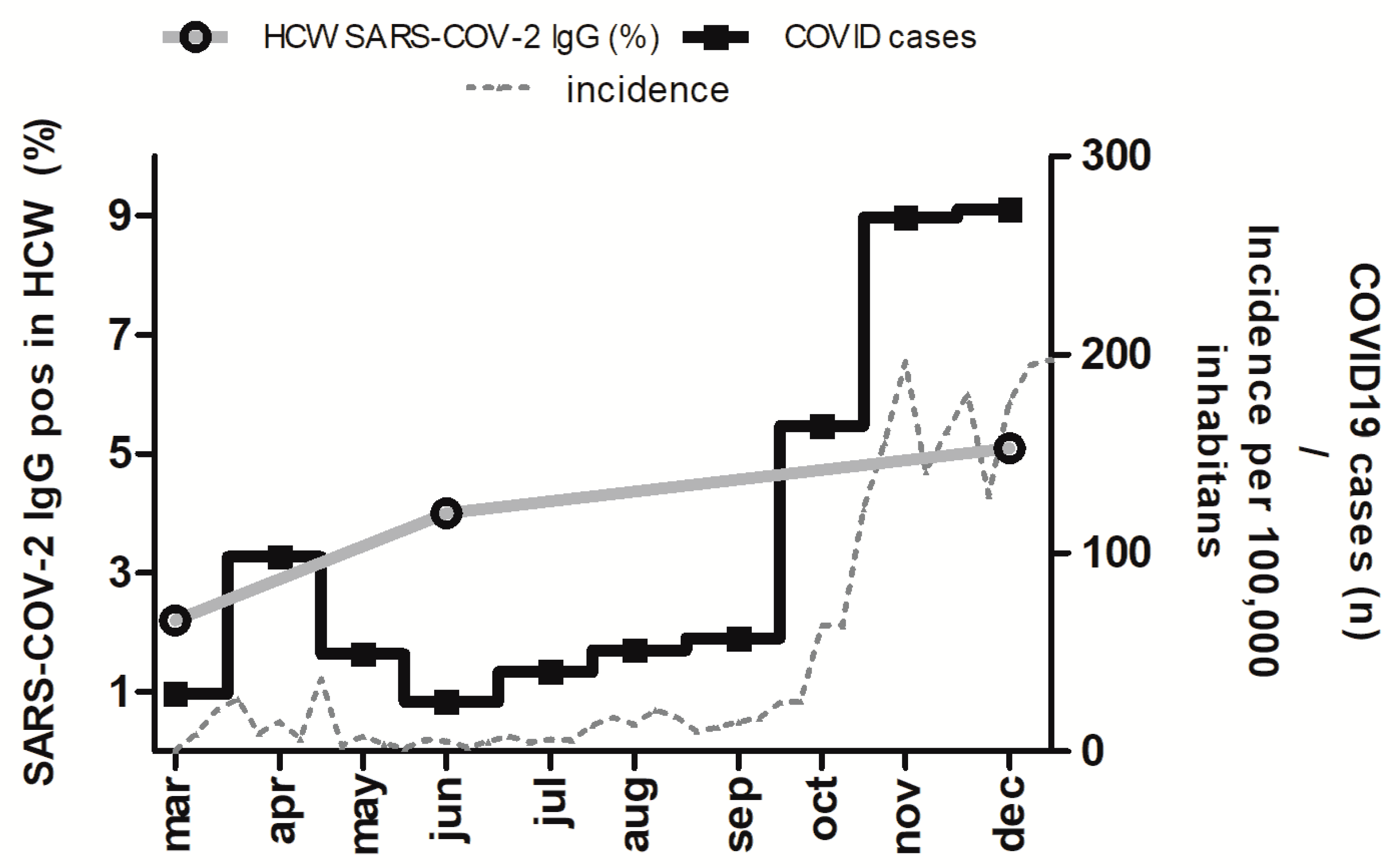
3.1. Seroprevalance
3.1.1. First Observational Period: March–May 2020
3.1.2. Second Observational Period: June–July 2020
3.1.3. Third Observational Period: October–December 2020
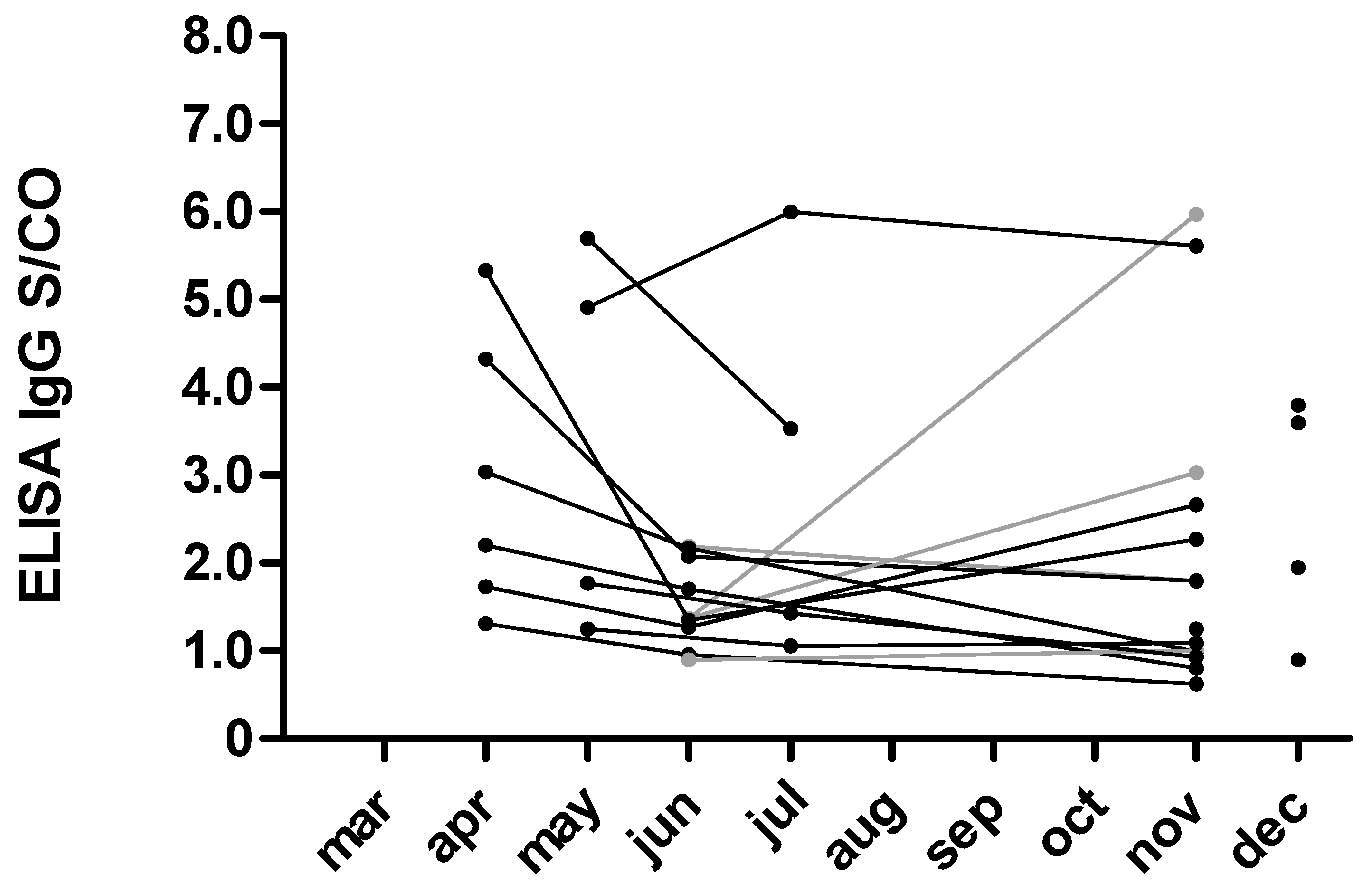
3.2. Neutralization Antibodies
3.3. Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Luo, Y.; Trevathan, E.; Qian, Z.; Li, Y.; Li, J.; Xiao, W.; Tu, N.; Zeng, Z.; Mo, P.; Xiong, Y.; et al. Asymptomatic SARS-CoV-2 Infection in Household Contacts of a Healthcare Provider, Wuhan, China. Emerg. Infect. Dis. 2020, 26. [Google Scholar] [CrossRef]
- Weissman, D.N.; de Perio, M.A.; Radonovich, L.J. COVID-19 and Risks Posed to Personnel During Endotracheal Intubation. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Hoehl, S.; Berger, A.; Kortenbusch, M.; Cinatl, J.; Bojkova, D.; Rabenau, H.; Behrens, P.; Böddinghaus, B.; Götsch, U.; Naujoks, F.; et al. Evidence of SARS-CoV-2 Infection in Returning Travelers from Wuhan, China. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Petherick, A. Developing antibody tests for SARS-CoV-2. Lancet 2020, 395, 1101–1102. [Google Scholar] [CrossRef]
- Heilingloh, C.S.; Aufderhorst, U.W.; Schipper, L.; Dittmer, U.; Witzke, O.; Yang, D.; Zheng, X.; Sutter, K.; Trilling, M.; Alt, M.; et al. Susceptibility of SARS-CoV-2 to UV irradiation. Am. J. Infect. Control 2020, 48, 1273–1275. [Google Scholar] [CrossRef]
- Herron, J.B.T.; Hay-David, A.G.C.; Gilliam, A.D.; Brennan, P.A. Personal protective equipment and Covid 19- a risk to healthcare staff? Br. J. Oral Maxillofac. Surg. 2020, 58, 500–502. [Google Scholar] [CrossRef]
- Heinz, T.K. Hygienemängel in Arztpraxis und Krankenhaus. Hessiches Ärzteblatt 2020, 5, 5–7. [Google Scholar]
- d’Aloja, E.; Finco, G.; Demontis, R.; Napoli, P.E.; Fossarello, M.; Nioi, M. COVID-19 and medical liability: Italy denies the shield to its heroes. EClinicalMedicine 2020, 25, 100470. [Google Scholar] [CrossRef] [PubMed]
- Korth, J.; Wilde, B.; Dolff, S.; Anastasiou, O.E.; Krawczyk, A.; Jahn, M.; Cordes, S.; Ross, B.; Esser, S.; Lindemann, M.; et al. SARS-CoV-2-specific antibody detection in healthcare workers in Germany with direct contact to COVID-19 patients. J. Clin. Virol. 2020, 128, 104437. [Google Scholar] [CrossRef]
- Papagiannis, D.; Malli, F.; Raptis, D.G.; Papathanasiou, I.V.; Fradelos, E.C.; Daniil, Z.; Rachiotis, G.; Gourgoulianis, K.I. Assessment of knowledge, attitudes, and practices towards new coronavirus (SARS-CoV-2) of health care professionals in greece before the outbreak period. Int. J. Environ. Res. Public Health 2020, 17, 4925. [Google Scholar] [CrossRef]
- Hesaraki, M.; Akbarizadeh, M.; Ahmadidarrehsima, S.; Moghadam, M.P.; Izadpanah, F. Knowledge, attitude, practice and clinical recommendations of health care workers towards COVID-19: A systematic review. Rev. Environ. Health 2020. [Google Scholar] [CrossRef]
- Fischer, B.; Knabbe, C.; Vollmer, T. SARS-CoV-2 IgG seroprevalence in blood donors located in three different federal states, Germany, March to June 2020. Eurosurveillance 2020, 25, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Aziz, N.A.; Corman, V.M.; Echterhoff, A.K.C.; Müller, M.A.; Richter, A.; Schmandke, A.; Schmidt, M.L.; Schmidt, T.H.; de Vries, F.M.; Drosten, C.; et al. Seroprevalence and correlates of SARS-CoV-2 neutralizing antibodies from a population-based study in Bonn, Germany. Nat. Commun. 2021, 12, 2117. [Google Scholar] [CrossRef]
- Nioi, M.; Napoli, P.E.; Lobina, J.; Fossarello, M.; d’Aloja, E. COVID-19 and Italian Healthcare Workers From the Initial Sacrifice to the mRNA Vaccine: Pandemic Chrono-History, Epidemiological Data, Ethical Dilemmas, and Future Challenges. Front. Public Health 2021, 8, 1–7. [Google Scholar] [CrossRef]
- Chen, X.; Chen, Z.; Azman, A.S.; Deng, X.; Chen, X.; Lu, W.; Zhao, Z.; Yang, J.; Viboud, C.; Ajelli, M.; et al. Serological evidence of human infection with SARS-CoV-2: A systematic review and meta-analysis. Lancet Glob. Health 2020. [Google Scholar] [CrossRef]
- Streeck, H.; Schulte, B.; Kümmerer, B.M.; Richter, E.; Höller, T.; Fuhrmann, C.; Bartok, E.; Dolscheid-Pommerich, R.; Berger, M.; Wessendorf, L.; et al. Infection fatality rate of SARS-CoV2 in a super-spreading event in Germany. Nat. Commun. 2020, 11, 1–12. [Google Scholar] [CrossRef]
- Finkenzeller, T.; Faltlhauser, A.; Dietl, K.H.; Paetzel, C.; Szczypien, N.; Klawonn, F.; Bodmann, K.-F.; von Meyer, A. SARS-CoV-2 antibodies in ICU and clinic staff: From Germany’s region with the highest infection rate. Med. Klin. Intensivmed. Notf. 2020, 115, 139–145. [Google Scholar] [CrossRef]
- Rudberg, A.S.; Havervall, S.; Månberg, A.; Jernbom Falk, A.; Aguilera, K.; Ng, H.; Gabrielsson, L.; Salomonsson, A.C.; Hanke, L.; Murrell, B.; et al. SARS-CoV-2 exposure, symptoms and seroprevalence in healthcare workers in Sweden. Nat. Commun. 2020, 11, 1–8. [Google Scholar] [CrossRef]
- Brehm, T.T.; Schwinge, D.; Lampalzer, S.; Schlicker, V.; Küchen, J.; Thompson, M.; Ullrich, F.; Huber, S.; Schmiedel, S.; Addo, M.M.; et al. Seroprevalence of SARS-CoV-2 antibodies among hospital workers in a German tertiary care center: A sequential follow-up study. Int. J. Hyg. Environ. Health 2021, 232, 113671. [Google Scholar] [CrossRef]
- Milazzo, L.; Lai, A.; Pezzati, L.; Oreni, L.; Bergna, A.; Conti, F.; Meroni, C.; Minisci, D.; Galli, M.; Corbellino, M.; et al. Dynamics of the seroprevalence of SARS-CoV-2 antibodies among healthcare workers at a COVID-19 referral hospital in Milan, Italy. Occup. Environ. Med. 2021, 1–7. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Seroprevalence of SARS-CoV-2 antibodies and associated factors in healthcare workers: A systematic review and meta-analysis. J. Hosp. Infect. 2021, 108, 120–134. [Google Scholar] [CrossRef] [PubMed]
- Bar-On, Y.M.; Flamholz, A.; Phillips, R.; Milo, R. Sars-cov-2 (covid-19) by the numbers. eLife 2020, 9, e57309. [Google Scholar] [CrossRef] [PubMed]
- Bourouiba, L. Turbulent Gas Clouds and Respiratory Pathogen Emissions: Potential Implications for Reducing Transmission of COVID-19. JAMA J. Am. Med. Assoc. 2020, 323, 1837–1838. [Google Scholar] [CrossRef] [PubMed]
- Bartoszko, J.J.; Farooqi, M.A.M.; Alhazzani, W.; Loeb, M. Medical masks vs N95 respirators for preventing COVID-19 in healthcare workers: A systematic review and meta-analysis of randomized trials. Influenza Other Respir. Viruses 2020, 14, 365–373. [Google Scholar] [CrossRef] [Green Version]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, 1–23. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates. N. Engl. J. Med. 2020, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Schwarzkopf, S.; Krawczyk, A.; Knop, D.; Klump, H.; Heinold, A.; Heinemann, F.M.; Thümmler, L.; Temme, C.; Breyer, M.; Witzke, O.; et al. Cellular Immunity in COVID-19 Convalescents with PCR-Confirmed Infection but with Undetectable SARS-CoV-2–Specific IgG. Emerg. Infect. Dis. 2021, 27, 122–129. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| High-Risk | Intermediate-Risk | Low-Risk | Overall | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| HCW | 338 | 75% | 78 | 17% | 34 | 8% | 450 | 100% |
| female | 220 | 65% | 49 | 63% | 25 | 74% | 294 | 65% |
| age (±SD) | 36.6 ± 10.7 | 42.6 ± 11.4 | 42.2 ± 13.0 | 38.1 ± 11.3 | ||||
| profession | ||||||||
| nurse | 246 | 73% | 50 | 64% | 0 | 0% | 296 | 66% |
| physician | 84 | 25% | 22 | 28% | 9 | 26% | 115 | 26% |
| lab assistant | 0 | 0% | 0 | 0% | 20 | 59% | 20 | 4% |
| other | 8 | 2% | 6 | 8% | 5 | 15% | 19 | 4% |
| Symptoms | Healthcare Workes | |||||
|---|---|---|---|---|---|---|
| Positive (n, %) | Negative (n, %) | Unknown (n, %) | ||||
| headache | 9 | (47%) | 8 | (42%) | 2 | (11%) |
| general malaise | 8 | (42%) | 9 | (47%) | 2 | (11%) |
| anosmia | 7 | (37%) | 10 | (53%) | 2 | (11%) |
| rhinitis | 7 | (37%) | 10 | (53%) | 2 | (11%) |
| cough | 6 | (32%) | 11 | (58%) | 2 | (11%) |
| fever | 5 | (26%) | 12 | (63%) | 2 | (11%) |
| sore throat | 5 | (26%) | 12 | (63%) | 2 | (11%) |
| dyspnoea | 3 | (16%) | 14 | (74%) | 2 | (11%) |
| asymptomatic | 4 | (21%) | 13 | (68%) | 2 | (11%) |
| hospitalization | 0 | (0%) | 17 | (89%) | 2 | (11%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korth, J.; Wilde, B.; Dolff, S.; Frisch, J.; Jahn, M.; Krawczyk, A.; Trilling, M.; Schipper, L.; Cordes, S.; Ross, B.; et al. SARS-CoV-2 Seroprevalence in Healthcare Workers in Germany: A Follow-Up Study. Int. J. Environ. Res. Public Health 2021, 18, 4540. https://doi.org/10.3390/ijerph18094540
Korth J, Wilde B, Dolff S, Frisch J, Jahn M, Krawczyk A, Trilling M, Schipper L, Cordes S, Ross B, et al. SARS-CoV-2 Seroprevalence in Healthcare Workers in Germany: A Follow-Up Study. International Journal of Environmental Research and Public Health. 2021; 18(9):4540. https://doi.org/10.3390/ijerph18094540
Chicago/Turabian StyleKorth, Johannes, Benjamin Wilde, Sebastian Dolff, Jasmin Frisch, Michael Jahn, Adalbert Krawczyk, Mirko Trilling, Leonie Schipper, Sebastian Cordes, Birgit Ross, and et al. 2021. "SARS-CoV-2 Seroprevalence in Healthcare Workers in Germany: A Follow-Up Study" International Journal of Environmental Research and Public Health 18, no. 9: 4540. https://doi.org/10.3390/ijerph18094540