
Public Health Literacy, Knowledge, and Awareness Regarding Antibiotic Use and Antimicrobial Resistance during the COVID-19 Pandemic: A Cross-Sectional Study

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Characteristics of Study Participants
2.2. Participants’ Health Literacy Levels
2.3. Knowledge of Antibiotic Use among Participants
2.4. Knowledge of Antibiotic Resistance among Participants
2.5. Pattern of Antibiotic Usage in Relation to Knowledge of Antibiotics and Antibiotic Resistance
2.6. Factors Associated with Participants’ Knowledge of Antibiotics and Antibiotic Resistance
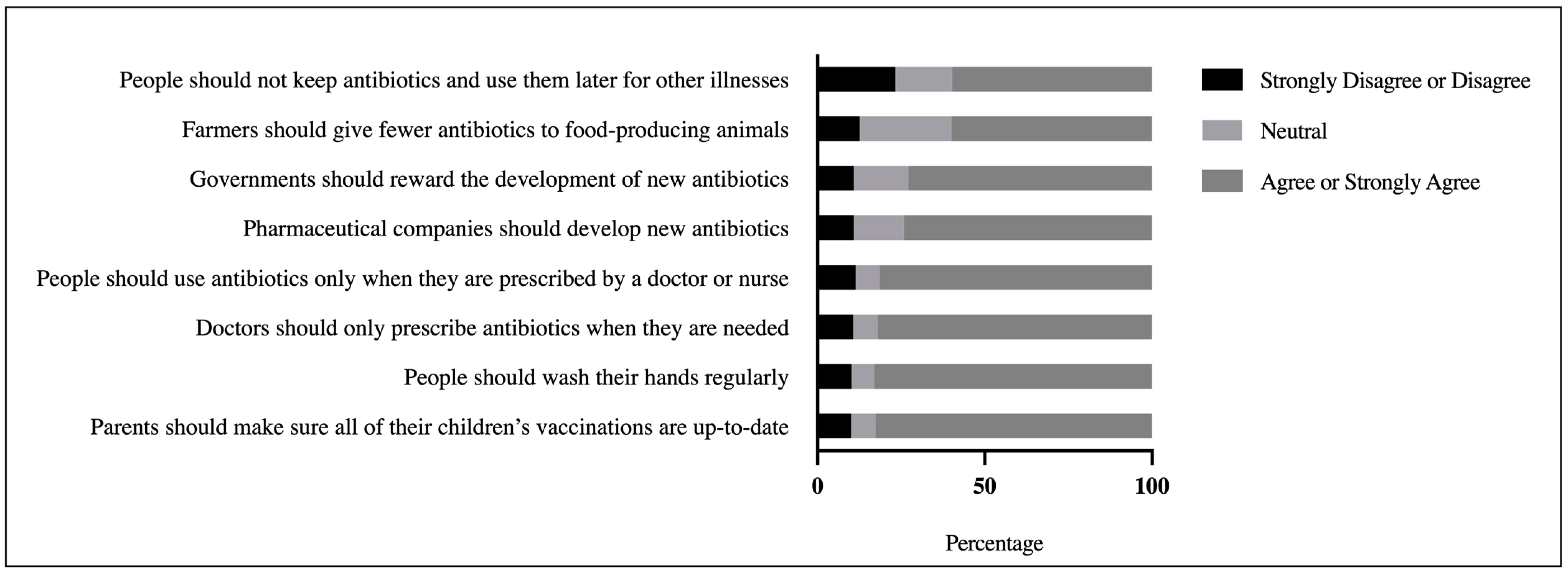
2.7. Level of Awareness of Possible Solutions to the Problem of Antibiotic Resistance
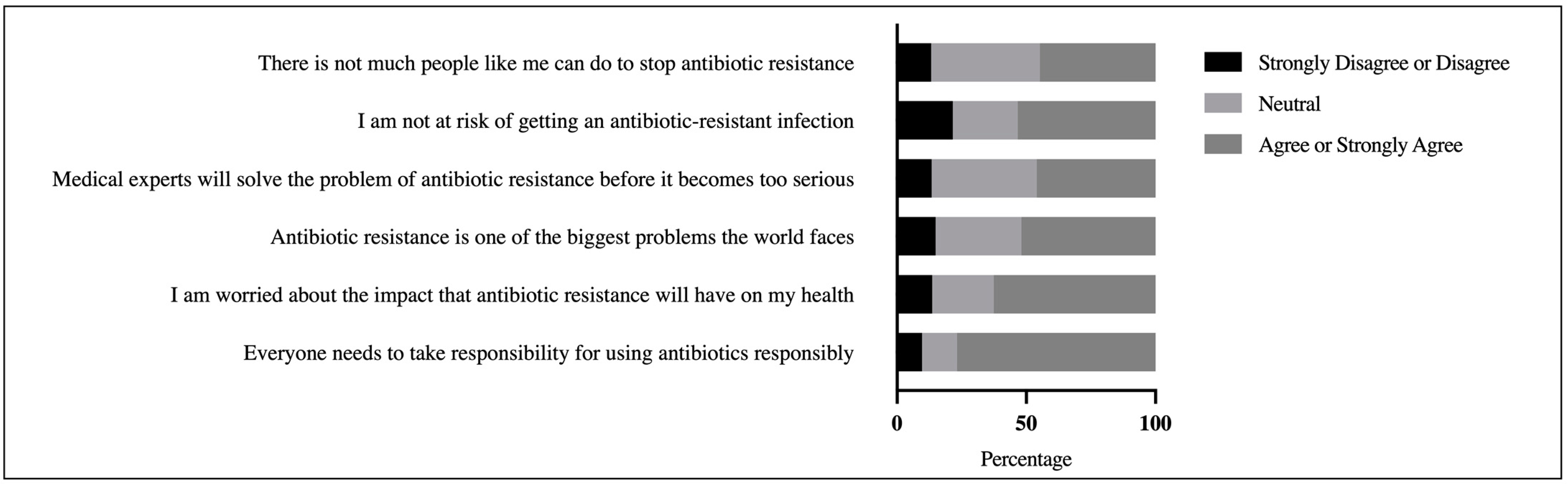
2.8. Participants’ Perspectives on the Scope of the Antibiotic Resistance Problem
3. Discussion
3.1. Health Literacy
3.2. Knowledge of Antibiotics and Antibiotic Resistance
3.2.1. Factors Associated with Participants’ Knowledge of Antibiotics and Antibiotic Resistance
3.2.2. The Use of Antibiotics
3.2.3. Implications for Education Campaigns
3.3. Participants’ Awareness of Possible Solutions to the Problem of Antibiotic Resistance
3.4. Participants’ Perspectives on the Scope of the Antibiotic Resistance Problem
3.5. Limitations and Strengths
4. Materials and Methods
4.1. Study Design and Setting
4.2. Survey Instrument
4.3. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- D’Costa, V.M.; King, C.E.; Kalan, L.; Morar, M.; Sung, W.W.L.; Schwarz, C.; Froese, D.; Zazula, G.; Calmels, F.; Debruyne, R. Antibiotic resistance is ancient. Nature 2011, 477, 457–461. [Google Scholar] [CrossRef]
- World Health Organization. Antibiotic Resistance: Multi-Country Public Awareness Survey; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Rodrigues, O.P.; Costa, T.; Branco, M.C.; Dinis, P. What’s the importance of portable tele-monitoring devices in patient therapeutic adherence? J. Int. Soc. Telemed. eHealth 2017, 5, e45. [Google Scholar]
- McNulty, C.A.M.; Boyle, P.; Nichols, T.; Clappison, P.; Davey, P. Don’t wear me out—the public’s knowledge of and attitudes to antibiotic use. J. Antimicrob. Chemother. 2007, 59, 727–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. New Report Calls for Urgent Action to Avert Antimicrobial Resistance Crisis. Volume 4. Available online: https://www.who.int/news/item/29-04-2019-new-report-calls-for-urgent-action-to-avert-antimicrobial-resistance-crisis (accessed on 25 April 2020).
- Beović, B.; Doušak, M.; Ferreira-Coimbra, J.; Nadrah, K.; Rubulotta, F.; Belliato, M.; Berger-Estilita, J.; Ayoade, F.; Rello, J.; Erdem, H. Antibiotic use in patients with COVID-19: A ‘snapshot’Infectious Diseases International Research Initiative (ID-IRI) survey. J. Antimicrob. Chemother. 2020, 75, 3386–3390. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and fungal coinfection in individuals with coronavirus: A rapid review to support COVID-19 antimicrobial prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; Yu, T. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Getahun, H.; Smith, I.; Trivedi, K.; Paulin, S.; Balkhy, H.H. Tackling antimicrobial resistance in the COVID-19 pandemic. Bull. World Health Organ. 2020, 98, 442. [Google Scholar] [CrossRef] [PubMed]
- Hayajneh, W.A.; Al-Azzam, S.; Yusef, D.; Lattyak, W.J.; Lattyak, E.A.; Gould, I.; López-Lozano, J.M.; Conway, B.R.; Conlon-Bingham, G.; Aldeyab, M.A. Identification of thresholds in relationships between specific antibiotic use and carbapenem-resistant Acinetobacter baumannii (CRAb) incidence rates in hospitalized patients in Jordan. J. Antimicrob. Chemother. 2021, 76, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Jirjees, F.J.; Al-Obaidi, H.J.; Sartaj, M.; Conlon-Bingham, G.; Farren, D.; Scott, M.G.; Gould, I.M.; López-Lozano, J.M.; Aldeyab, M.A.; Jirjees, F.J.; et al. Antibiotic Use and Resistance in Hospitals: Time-Series Analysis Strategy for Determining and Prioritising Interventions. Hosp. Pharm. Eur. 2020. Available online: https://hospitalpharmacyeurope.com/news/reviews-research/antibiotic-use-and-resistance-in-hospitals-time-series-analysis-strategy-for-determining-and-prioritising-interventions/ (accessed on 27 May 2021).
- Patel, A.; Emerick, M.; Cabunoc, M.K.; Williams, M.H.; Preas, M.A.; Schrank, G.; Rabinowitz, R.; Luethy, P.; Johnson, J.K.; Leekha, S. Rapid Spread and Control of Multidrug-Resistant Gram-Negative Bacteria in COVID-19 Patient Care Units. Emerg. Infect. Dis. 2021, 27, 1234. [Google Scholar] [CrossRef]
- Pavydė, E.; Veikutis, V.; Mačiulienė, A.; Mačiulis, V.; Petrikonis, K.; Stankevičius, E. Public knowledge, beliefs and behavior on antibiotic use and self-medication in Lithuania. Int. J. Environ. Res. Public Health 2015, 12, 7002–7016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallin, M.; Polyzoi, M.; Marrone, G.; Rosales-Klintz, S.; Tegmark Wisell, K.; Stålsby Lundborg, C. Knowledge and attitudes towards antibiotic use and resistance-a latent class analysis of a Swedish population-based sample. PLoS ONE 2016, 11, e0152160. [Google Scholar] [CrossRef] [Green Version]
- Anderson, A. Online health information and public knowledge, attitudes, and behaviours regarding antibiotics in the UK: Multiple regression analysis of Wellcome Monitor and Eurobarometer Data. PLoS ONE 2018, 13, e0204878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salm, F.; Ernsting, C.; Kuhlmey, A.; Kanzler, M.; Gastmeier, P.; Gellert, P. Antibiotic use, knowledge and health literacy among the general population in Berlin, Germany and its surrounding rural areas. PLoS ONE 2018, 13, e0193336. [Google Scholar] [CrossRef] [Green Version]
- Kickbusch, I.; Pelikan, J.M.; Apfel, F.; Tsouros, A. Health Literacy; WHO Regional Office for Europe: Copenhagen, Denmark, 2013; ISBN 9289000155. [Google Scholar]
- Wang, M.P.; Viswanath, K.; Lam, T.H.; Wang, X.; Chan, S.S. Social determinants of health information seeking among Chinese adults in Hong Kong. PLoS ONE 2013, 8, e73049. [Google Scholar] [CrossRef] [Green Version]
- El Sherbiny, N.A.; Ibrahim, E.H.; Masoud, M. Assessment of knowledge, attitude and behavior towards antibiotic use in primary health care patients in Fayoum Governorate, Egypt. Alex. J. Med. 2018, 54, 535–540. [Google Scholar] [CrossRef] [Green Version]
- Mostafa, A.; Abdelzaher, A.; Rashed, S.; AlKhawaga, S.I.; Afifi, S.K.; AbdelAlim, S.; Mostafa, S.A.; Zidan, T.A. Is health literacy associated with antibiotic use, knowledge and awareness of antimicrobial resistance among non-medical university students in Egypt? A cross-sectional study. BMJ Open 2021, 11, e046453. [Google Scholar] [CrossRef]
- Sawair, F.A.; Baqain, Z.H.; Abu Karaky, A.; Abu Eid, R. Assessment of self-medication of antibiotics in a Jordanian population. Med. Princ. Pract. 2008, 18, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Nusair, M.B.; Al-azzam, S.; Alhamad, H.; Momani, M.Y. The prevalence and patterns of self-medication with antibiotics in Jordan: A community-based study. Int. J. Clin. Pract. 2021, 75, e13665. [Google Scholar] [CrossRef]
- Al-Azzam, S.I.; Al-Husein, B.A.; Alzoubi, F.; Masadeh, M.M.; Al-Horani, M.A.S. Self-medication with antibiotics in Jordanian population. Int. J. Occup. Med. Environ. Health 2007, 20, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Alshogran, O.Y.; Alzoubi, K.H.; Khabour, O.F.; Farah, S. Patterns of self-medication among medical and nonmedical university students in Jordan. Risk Manag. Healthc. Policy 2018, 11, 169. [Google Scholar] [CrossRef] [Green Version]
- Muflih, S.M.; Bashir, H.N.; Khader, Y.S.; Karasneh, R.A. The impact of health literacy on self-medication: A cross-sectional outpatient study. J. Public Health 2020. [Google Scholar] [CrossRef] [PubMed]
- Haque, M.; Rahman, N.A.A.; McKimm, J.; Kibria, G.M.; Majumder, M.A.A.; Haque, S.Z.; Islam, M.Z.; Abdullah, S.L.B.; Daher, A.M.; Zulkifli, Z. Self-medication of antibiotics: Investigating practice among university students at the Malaysian National Defence University. Infect. Drug Resist. 2019, 12, 1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz, M.E. Risks of self-medication practices. Curr. Drug Saf. 2010, 5, 315–323. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines for the Regulatory Assessment of Medicinal Products for Use in Self-Medication; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Schroeck, J.L.; Ruh, C.A.; Sellick, J.A.; Ott, M.C.; Mattappallil, A.; Mergenhagen, K.A. Factors associated with antibiotic misuse in outpatient treatment for upper respiratory tract infections. Antimicrob. Agents Chemother. 2015, 59, 3848–3852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.M.; Wertheim, H.F.L.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H. Antibiotic resistance—the need for global solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef] [Green Version]
- Pereko, D.D.; Lubbe, M.S.; Essack, S.Y. Public knowledge, attitudes and behaviour towards antibiotic usage in Windhoek, Namibia. S. Afr. J. Infect. Dis. 2015, 30, 27–29. [Google Scholar] [CrossRef] [Green Version]
- Gowri, S.; Mehta, D.; Kannan, S. Antibiotic use in dentistry: A cross-sectional survey from a developing country. J. Orofac. Sci. 2015, 7, 90. [Google Scholar]
- Nathan, C.; Cars, O. Antibiotic resistance—problems, progress, and prospects. N. Engl. J. Med. 2014, 371, 1761–1763. [Google Scholar] [CrossRef]
- Knight, G.M.; Glover, R.E.; McQuaid, C.F.; Olaru, I.D.; Gallandat, K.; Leclerc, Q.J.; Fuller, N.M.; Willcocks, S.J.; Hasan, R.; van Kleef, E. Antimicrobial resistance and COVID-19: Intersections and implications. eLife 2021, 10, e64139. [Google Scholar] [CrossRef]
- Effah, C.Y.; Amoah, A.N.; Liu, H.; Agboyibor, C.; Miao, L.; Wang, J.; Wu, Y. A population-base survey on knowledge, attitude and awareness of the general public on antibiotic use and resistance. Antimicrob. Resist. Infect. Control 2020, 9, 105. [Google Scholar] [CrossRef]
- Brookes-Howell, L.; Elwyn, G.; Hood, K.; Wood, F.; Cooper, L.; Goossens, H.; Ieven, M.; Butler, C.C. “The body gets used to them”: Patients’ interpretations of antibiotic resistance and the implications for containment strategies. J. Gen. Intern. Med. 2012, 27, 766–772. [Google Scholar] [CrossRef] [Green Version]
- Kong, L.S.; Islahudin, F.; Muthupalaniappen, L.; Chong, W.W. Knowledge and expectations on antibiotic use among older adults in Malaysia: A cross-sectional survey. Geriatrics 2019, 4, 61. [Google Scholar] [CrossRef] [Green Version]
- Lim, K.K.; Teh, C.C. A cross sectional study of public knowledge and attitude towards antibiotics in Putrajaya, Malaysia. South. Med. Rev. 2012, 5, 26. [Google Scholar]
- Kim, S.S.; Moon, S.; Kim, E.J. Public knowledge and attitudes regarding antibiotic use in South Korea. J. Korean Acad. Nurs. 2011, 41, 742–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, D.R.M.; Dolk, F.C.K.; Smieszek, T.; Robotham, J.V.; Pouwels, K.B. Understanding the gender gap in antibiotic prescribing: A cross-sectional analysis of English primary care. BMJ Open 2018, 8, e020203. [Google Scholar] [CrossRef] [Green Version]
- Waaseth, M.; Adan, A.; Røen, I.L.; Eriksen, K.; Stanojevic, T.; Halvorsen, K.H.; Garcia, B.H.; Holst, L.; Ulshagen, K.M.; Blix, H.S.; et al. Knowledge of antibiotics and antibiotic resistance among Norwegian pharmacy customers—A cross-sectional study. BMC Public Health 2019, 19, 66. [Google Scholar] [CrossRef]
- Abdel-Qader, D.H.; Albassam, A.; Ismael, N.S.; El-Shara’, A.; Shehri, A.; Almutairi, F.S.; Al-Harbi, D.M.; Al Zahrani, M.M.; Chen, L.-C.; Al Mazrouei, N. Awareness of antibiotic use and resistance in Jordanian Community. J. Prim. Care Community Health 2020, 11, 2150132720961255. [Google Scholar] [CrossRef] [PubMed]
- Baum, A.; Kaboli, P.J.; Schwartz, M.D. Reduced in-person and increased telehealth outpatient visits during the COVID-19 pandemic. Ann. Intern. Med. 2021, 174, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Araia, Z.Z.; Gebregziabher, N.K.; Mesfun, A.B. Self medication practice and associated factors among students of Asmara College of Health Sciences, Eritrea: A cross sectional study. J. Pharm. Policy Pract. 2019, 12, 3. [Google Scholar] [CrossRef] [Green Version]
- Hoxha, I.; Malaj, A.; Kraja, B.; Bino, S.; Oluka, M.; Marković-Peković, V.; Godman, B. Are pharmacists’ good knowledge and awareness on antibiotics taken for granted? The situation in Albania and future implications across countries. J. Glob. Antimicrob. Resist. 2018, 13, 240–245. [Google Scholar] [CrossRef] [Green Version]
- Jafari, F.; Khatony, A.; Rahmani, E. Prevalence of self-medication among the elderly in Kermanshah-Iran. Glob. J. Health Sci. 2015, 7, 360. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, A.; Naqvi, R.; Grewal, A.; Diachun, L.; Gutmanis, I. Antibiotic resistance knowledge in the elderly. UWO Med. J. 2009, 78, 69–72. [Google Scholar]
- Davis, M.E.; Liu, T.-L.; Taylor, Y.J.; Davidson, L.; Schmid, M.; Yates, T.; Scotton, J.; Spencer, M.D. Exploring patient awareness and perceptions of the appropriate use of antibiotics: A mixed-methods study. Antibiotics 2017, 6, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoelzer, K.; Bielke, L.; Blake, D.P.; Cox, E.; Cutting, S.M.; Devriendt, B.; Erlacher-Vindel, E.; Goossens, E.; Karaca, K.; Lemiere, S. Vaccines as alternatives to antibiotics for food producing animals. Part 1: Challenges and needs. Vet. Res. 2018, 49, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smulski, S.; Turlewicz-Podbielska, H.; Wylandowska, A.; Włodarek, J. Non-antibiotic possibilities in prevention and treatment of calf diarrhoea. J. Vet. Res. 2020, 64, 119. [Google Scholar] [CrossRef] [PubMed]
- Higuita-Gutiérrez, L.F.; Villamil, G.E.R.; Quiceno, J.N.J. Knowledge, attitude, and practice regarding antibiotic use and resistance among medical students in Colombia: A cross-sectional descriptive study. BMC Public Health 2020, 20, 1861. [Google Scholar] [CrossRef]
- Dixit, A.; Kumar, N.; Kumar, S.; Trigun, V. Antimicrobial resistance: Progress in the decade since emergence of New Delhi metallo-β-lactamase in India. Indian J. Community Med. 2019, 44, 4. [Google Scholar]
- Aldeyab, M.; López-Lozano, J.M.; Gould, I.M. Global antibiotics use and resistance. In Global Pharmaceutical Policy; Palgrave Macmillan: London, UK, 2020; pp. 331–344. ISBN 9789811527241. [Google Scholar]
- Shebehe, J.; Ottertun, E.; Carlén, K.; Gustafson, D. Knowledge about infections is associated with antibiotic use: Cross-sectional evidence from the health survey Northern Ireland. BMC Public Health 2021, 21, 1041. [Google Scholar] [CrossRef]
- van Dijk, J.A.G.M. The Deepening Divide: Inequality in the Information Society; Sage Publications: London, UK, 2005. [Google Scholar]
- Hargittai, E. Second-Level Digital Divide: Mapping Differences in People’s Online Skills. arXiv 2001, arXiv:cs/0109068. [Google Scholar] [CrossRef]
- Department of Statistics. Available online: http://dosweb.dos.gov.jo/ (accessed on 22 August 2021).
- Lehdonvirta, V.; Oksanen, A.; Räsänen, P.; Blank, G. Social Media, Web, and Panel Surveys: Using Non-Probability Samples in Social and Policy Research. Policy Internet 2021, 13, 134–155. [Google Scholar] [CrossRef]
- Evangelista, L.S.; Rasmusson, K.D.; Laramee, A.S.; Barr, J.; Ammon, S.E.; Dunbar, S.; Ziesche, S.; Patterson, J.H.; Yancy, C.W. Health literacy and the patient with heart failure—implications for patient care and research: A consensus statement of the Heart Failure Society of America. J. Card. Fail. 2010, 16, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Sample Size Calculator by Raosoft, Inc. Available online: http://www.raosoft.com/samplesize.html (accessed on 22 April 2021).
- Morris, N.S.; MacLean, C.D.; Chew, L.D.; Littenberg, B. The Single Item Literacy Screener: Evaluation of a brief instrument to identify limited reading ability. BMC Fam. Pract. 2006, 7, 21. [Google Scholar] [CrossRef] [PubMed]
- Kerlinger, F. Foundations of Behavioral Research, 3rd ed.; Holt, Rinehart and Winston: New York, NY, USA, 1986. [Google Scholar]
- Sperandei, S. Understanding logistic regression analysis. Biochem. Med. 2014, 24, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Templeton, G.F. A two-step approach for transforming continuous variables to normal: Implications and recommendations for IS research. Commun. Assoc. Inf. Syst. 2011, 28, 4. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | n (%) |
|---|---|
| Age (years) | |
| 18–24 | 279 (23) |
| 25–34 | 429 (35.4) |
| 35–44 | 334 (27.5) |
| >45 | 171 (14.1) |
| Gender | |
| Male | 357 (29.4) |
| Female | 856 (70.6) |
| Area of Living | |
| Urban | 741 (61.1) |
| Suburban | 242 (20) |
| Rural | 230 (19) |
| Family Structure | |
| Nuclear family | 607 (50) |
| Joint family | 306 (25.2) |
| Extended family | 300 (24.7) |
| Education Level | |
| Up to High School | 256 (21.1) |
| Bachelor’s degree | 666 (54.9) |
| Postgraduate degree (e.g., MSc, PhD) | 291 (24) |
| Employment Status | |
| Unemployed | 481 (39.7) |
| Employed in nonmedical field | 389 (32.1) |
| Employed in medical field | 343 (28.3) |
| Family Monthly Income | |
| Less than JOD 500 (USD 700) | 399 (32.9) |
| JOD 501 (USD 700)–JOD 1000 (USD 1400) | 549 (45.3) |
| JOD 1001 (USD 1400)–JOD 1500 (USD 2100) | 147 (12.1) |
| Above JOD 1500 (USD 2100) | 118 (9.7) |
| Do you have health insurance? | |
| Yes | 931 (76.8) |
| No | 282 (23.2) |
| Have you ever been infected with COVID-19? | |
| Yes | 486 (40.1) |
| No | 727 (59.9) |
| Statements | n (%) |
|---|---|
| When do you think you should stop taking antibiotics once you’ve begun treatment? | |
| When you feel better | 208 (17.1) |
| When you’ve taken all of the antibiotics as directed | 989 (81.5) |
| Don’t know | 16 (1.3) |
| Do you think this statement is “true” or “false”? “It’s okay to use antibiotics that were given to a friend or family member, as long as they were used to treat the same illness.” | |
| True | 165 (13.6) |
| False | 997 (82.2) |
| Don’t know | 51 (4.2) |
| Do you think this statement is “true” or “false”? “It’s okay to buy the same antibiotics, or request these from a doctor, if you’re sick and they helped you get better when you had the same symptoms before.” | |
| True | 414 (34.1) |
| False | 716 (59) |
| Don’t know | 83 (6.8) |
| Do you think these conditions can be treated with antibiotics? | n of “Yes” Answers (%) |
| HIV/AIDS | 57 (4.7) |
| Gonorrhea | 173 (14.3) |
| Bladder infection or urinary tract infection | 914 (75.4) |
| Diarrhea | 202 (16.7) |
| Cold and flu | 524 (43.2) |
| Fever | 299 (24.6) |
| Malaria | 158 (13) |
| Measles | 85 (7) |
| Skin or wound infection | 805 (66.4) |
| Sore throat | 1021 (84.2) |
| Body aches | 163 (13.4) |
| Headaches | 169 (13.9) |
| COVID-19 | 319 (26.3) |
| Statement | Correct Answer | n (%) | ||
|---|---|---|---|---|
| False | I Don’t Know | True | ||
| False | 172 (14.2) | 192 (15.8) | 849 (70.0) |
| True | 149 (12.3) | 222 (18.3) | 842 (69.4) |
| True | 363 (29.9) | 299 (24.6) | 550 (45.3) |
| True | 187 (15.4) | 275 (22.7) | 750 (61.8) |
| False | 568 (46.8) | 394 (32.5) | 250 (20.6) |
| False | 519 (42.8) | 281 (23.2) | 412 (34.0) |
| True | 361 (29.8) | 402 (33.2) | 449 (37.0) |
| True | 76 (6.3) | 304 (25.1) | 832 (68.6) |
| Have you heard of any of the following terms before this survey? | n of “Yes” (%) | |||
| Antibiotic resistance | 907 (74.8) | |||
| Superbugs | 761 (62.7) | |||
| Antimicrobial resistance | 583 (48.1) | |||
| Drug resistance | 782 (64.5) | |||
| Antibiotic-resistant bacteria | 830 (68.4) | |||
| Never heard of any of these terms | 139 (11.5) | |||
| Statements | n (%) | Knowledge of Antibiotics (Adequate vs. Inadequate) | Knowledge of Antibiotic Resistance (Adequate vs. Inadequate) | ||
|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | ||
| When did you last take antibiotics? | |||||
| More than a year ago | 188 (15.5) | 3.63 (2.44–5.41) | 0.000 | 2.08 (1.45–2.99) | 0.000 |
| Last year | 119 (9.8) | 2.19 (1.42–3.39) | 0.000 | 2.13 (1.39–3.26) | 0.001 |
| Six months ago | 365 (30.1) | 1.74 (1.29–2.35) | 0.000 | 1.42 (1.06–1.91) | 0.02 |
| One month ago | 344 (28.4) | 1 | 1 | ||
| On that occasion, did you get the antibiotics by a prescription from a doctor or nurse? (Appropriate self-medication of antibiotics) | |||||
| Yes | 851 (70.2) | 2.01 (1.57–2.58) | 0.000 | 1.31 (1.03–1.68) | 0.03 |
| No or can’t remember | 362 (29.8) | 1 | 1 | ||
| On that occasion, did you get advice from a doctor, nurse, or pharmacist on how to take them? | |||||
| Yes | 889 (73.3) | 1.98 (1.53–2.56) | 0.000 | 1.18 (0.91–1.52) | 0.215 |
| No or can’t remember | 324 (26.7) | 1 | 1 | ||
| Main sources of self-medication antibiotics (n = 362) | |||||
| Pharmacy | 185 (51.1) | ||||
| Healthcare centers | 45 (12.4) | ||||
| Friends or family | 88 (24.3) | ||||
| Using leftover antibiotics | 44 (12.2) | ||||
| Variables | Knowledge of Antibiotics (Adequate vs. Inadequate) | Knowledge of Antibiotic Resistance (Adequate vs. Inadequate) | ||||
|---|---|---|---|---|---|---|
| Standardized β (S.E.) | Adjusted OR (95% CI) | p-Value * | Standardized β (S.E.) | Adjusted OR (95% CI) | p-Value * | |
| Age | ||||||
| 18–24 | 0.9 (0.23) | 2.46 (1.55–3.9) | 0.000 | 0.29 (0.22) | 1.34 (0.87–2.08) | 0.179 |
| 25–34 | 0.48 (0.22) | 1.61 (1.05–2.49) | 0.029 | 0.29 (0.2) | 1.34 (0.9–1.99) | 0.148 |
| 35–44 | 0.18 (0.22) | 1.2 (0.77–1.86) | 0.401 | 0.38 (0.2) | 1.46 (0.98–2.18) | 0.062 |
| >45 | Reference | Reference | ||||
| Gender | ||||||
| Male | −0.39 (0.14) | 0.67 (0.5-0.89) | 0.007 | −0.11 (0.17) | 0.89 (0.69–1.14) | 0.364 |
| Female (Ref.) | Reference | Reference | ||||
| Area of Living | ||||||
| Urban | 0.4 (0.17) | 1.5 (1.07–2.10) | 0.018 | 0.98 (0.67–1.41) | 0.928 | 0.269 |
| Suburban | −0.04 (0.2) | 0.96 (0.64–1.43) | 0.847 | 1.15 (0.85–01.54) | 0.361 | |
| Rural | Reference | Reference | ||||
| Employment Status | ||||||
| Employed in medical field | 1.12 (0.18) | 3.08 (2.13–4.44) | 0.000 | 1.02 (0.16) | 2.78 (2.00–3.87) | 0.000 |
| Employed in nonmedical field | −0.03 (0.16) | 0.96 (0.69–1.33) | 0.822 | −0.03 (0.15) | 0.97 (0.71–1.30) | 0.849 |
| Unemployed | Reference | Reference | ||||
| Do you have health insurance? | ||||||
| Yes | 0.15 (0.15) | 1.16 (0.85–1.57) | 0.332 | 0.32 (0.14) | 1.38 (1.03–1.85) | 0.026 |
| No (Ref.) | Reference | Reference | ||||
| How do you protect yourself and others from COVID-19? | ||||||
| Received antibiotics? | ||||||
| Yes (n = 250, 20.6%) | −1.11 (0.18) | 0.31 (0.22–0.45) | 0.000 | −0.29 (0.17) | 0.74 (0.53–1.05) | 0.093 |
| No | Reference | Reference | ||||
| Received COVID-19 vaccine? | ||||||
| Yes (n = 377, 31.1%) | 0.48 (0.15) | 1.62 (1.20–2.18) | 0.002 | 0.22 (0.14) | 1.24 (10.94–1.64) | 0.130 |
| No | Reference | Reference | ||||
| Health Literacy | ||||||
| Adequate (n = 759, 62.6%) | 0.31 (0.13) | 1.37 (1.05–1.77) | 0.017 | 0.38 (0.12) | 1.46 (1.14–1.89) | 0.003 |
| Inadequate | Reference | Reference | ||||
| Variables | Awareness of Possible Solutions to the Problem of Antibiotic Resistance | Perspectives on the Scope of the Antibiotic Resistance Problem | ||
|---|---|---|---|---|
| Mean (SD) | p-Value * | Mean (SD) | p-Value * | |
| Age | ||||
| 18–24 | 3.89 (0.97) | 0.004 | 3.42 (0.76) | 0.066 |
| 25–34 | 3.99 (0.89) | 3.51 (0.70) | ||
| 35–44 | 3.88 (0.95) | 3.57 (0.70) | ||
| >45 | 3.68 (0.94) | 3.49 (0.71) | ||
| Gender | ||||
| Male | 3.85 (0.99) | 0.271 | 3.45 (0.72) | 0.071 |
| Female | 3.92 (0.91) | 3.53 (0.72) | ||
| Area of Living | ||||
| Urban | 3.95 (0.93) | 0.061 | 3.53 (0.71) | 0.181 |
| Suburban | 3.81 (0.95) | 3.46 (0.72) | ||
| Rural | 3.82 (0.92) | 3.45 (0.73) | ||
| Family Structure | ||||
| Nuclear family | 3.89 (0.95) | 0.846 | 3.54 (0.76) | 0.162 |
| Joint family | 3.92 (0.95) | 3.48 (0.71) | ||
| Extended family | 3.89 (0.9) | 3.45 (0.63) | ||
| Education Level | ||||
| Up to high school | 3.77 (0.92) | 0.002 | 3.49 (0.77) | 0.489 |
| Bachelor’s degree | 3.88 (0.94) | 3.52 (0.73) | ||
| Postgraduate degree | 4.05 (0.93) | 3.46 (0.65) | ||
| Employment Status | ||||
| Employed in medical field | 3.92 (0.96) | 0.156 | 3.57 (0.74) | 0.828 |
| Employed in nonmedical field | 3.89 (0.95) | 3.47 (0.7) | ||
| Unemployed | 3.88 (0.9) | 3.48 (0.72) | ||
| Family Monthly Income | ||||
| Less than JOD 500 | 3.89 (0.93) | 0.742 | 3.47 (0.72) | 0.650 |
| JOD 501–JOD 1000 | 3.87 (0.96) | 3.52 (0.73) | ||
| JOD 1001–JOD 1500 | 3.96 (0.96) | 3.54 (0.73) | ||
| Above JOD 1500 | 3.94 (0.81) | 3.5 (0.65) | ||
| Do you have health insurance? | ||||
| Yes | 3.89 (0.94) | 0.822 | 3.52 (0.72) | 0.157 |
| No | 3.91 (0.92) | 3.45 (0.71) | ||
| Have you ever been infected with COVID-19? | ||||
| Yes | 3.91 (0.91) | 0.614 | 3.50 (0.69) | 0.896 |
| No | 3.89 (0.95) | 3.51 (0.74) | ||
| Health Literacy | ||||
| Adequate | 3.95 (0.93) | 0.011 | 3.54 (0.72) | 0.016 |
| Inadequate | 3.81 (0.94) | 3.44 (0.71) | ||
| Knowledge of Antibiotics | ||||
| Adequate | 3.93 (0.94) | 0.003 | 3.53 (0.71) | 0.001 |
| Inadequate | 3.71 (0.91) | 3.34 (0.73) | ||
| Knowledge of Antibiotic Resistance | ||||
| Adequate | 4.01 (0.99) | 0.000 | 3.63 (0.74) | 0.000 |
| Inadequate | 3.78 (0.86) | 3.36 (0.67) | ||
| Subscales | No. of Items | Mean ± SD | Cronbach’s α |
|---|---|---|---|
| Knowledge of antibiotics | 15 | 9.76 ± 2.06 | 0.67 |
| Knowledge of antibiotic resistance | 8 | 4.42 ± 2.03 | 0.65 |
| Awareness of possible solutions to the problem of antibiotic resistance | 8 | 3.90 ± 0.97 | 0.94 |
| Perspectives on the scope of the antibiotic resistance problem | 6 | 3.51 ± 0.73 | 0.82 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muflih, S.M.; Al-Azzam, S.; Karasneh, R.A.; Conway, B.R.; Aldeyab, M.A. Public Health Literacy, Knowledge, and Awareness Regarding Antibiotic Use and Antimicrobial Resistance during the COVID-19 Pandemic: A Cross-Sectional Study. Antibiotics 2021, 10, 1107. https://doi.org/10.3390/antibiotics10091107
Muflih SM, Al-Azzam S, Karasneh RA, Conway BR, Aldeyab MA. Public Health Literacy, Knowledge, and Awareness Regarding Antibiotic Use and Antimicrobial Resistance during the COVID-19 Pandemic: A Cross-Sectional Study. Antibiotics. 2021; 10(9):1107. https://doi.org/10.3390/antibiotics10091107
Chicago/Turabian StyleMuflih, Suhaib M., Sayer Al-Azzam, Reema A. Karasneh, Barbara R. Conway, and Mamoon A. Aldeyab. 2021. "Public Health Literacy, Knowledge, and Awareness Regarding Antibiotic Use and Antimicrobial Resistance during the COVID-19 Pandemic: A Cross-Sectional Study" Antibiotics 10, no. 9: 1107. https://doi.org/10.3390/antibiotics10091107