
Patient Characteristics and Clinical Course of COVID-19 Patients Treated at a German Tertiary Center during the First and Second Waves in the Year 2020

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. RT-PCR
2.3. Clinical Data
2.4. Statistical Analyses
3. Results
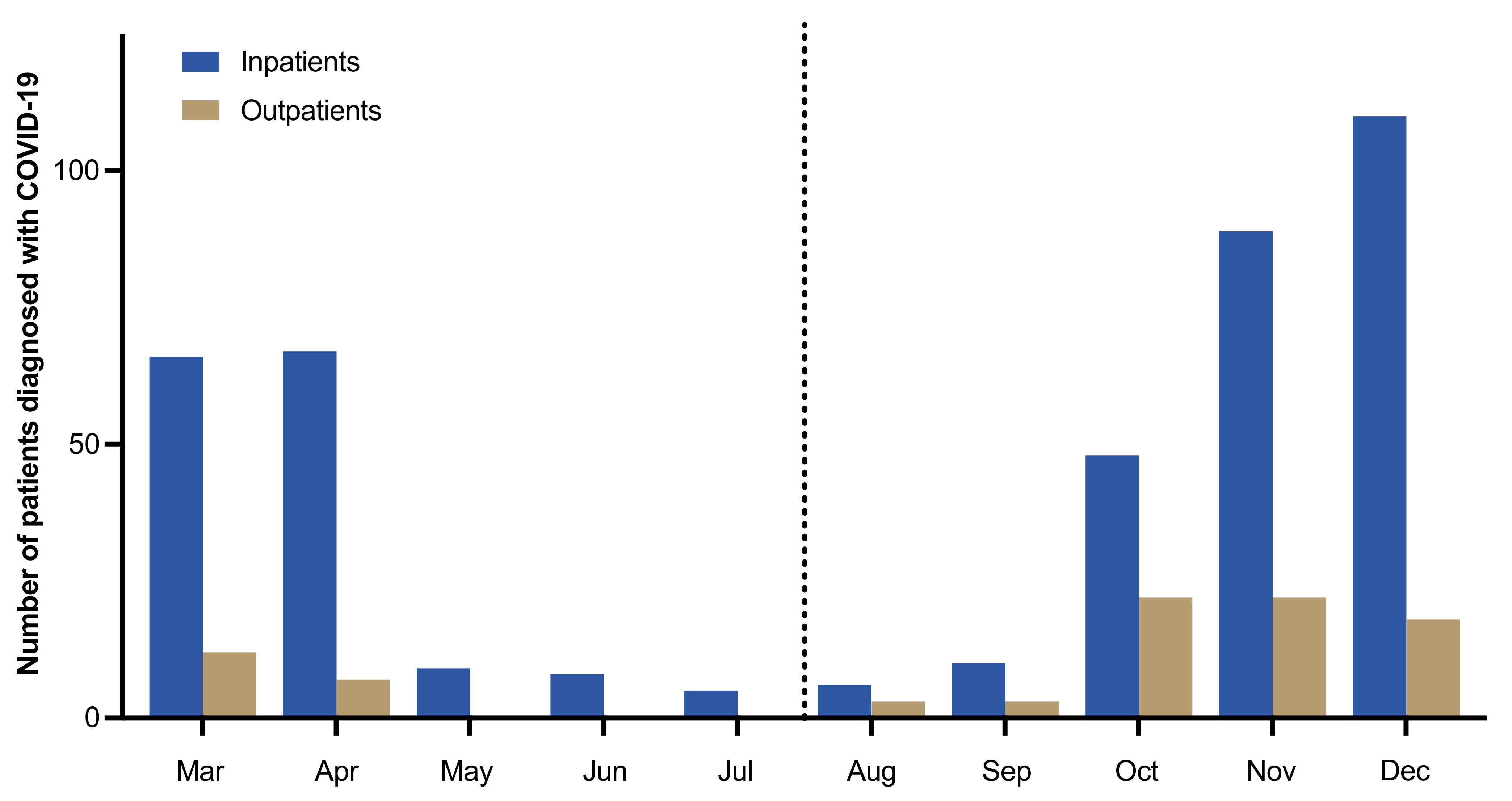
3.1. Number of Patients and Seasonal Distribution
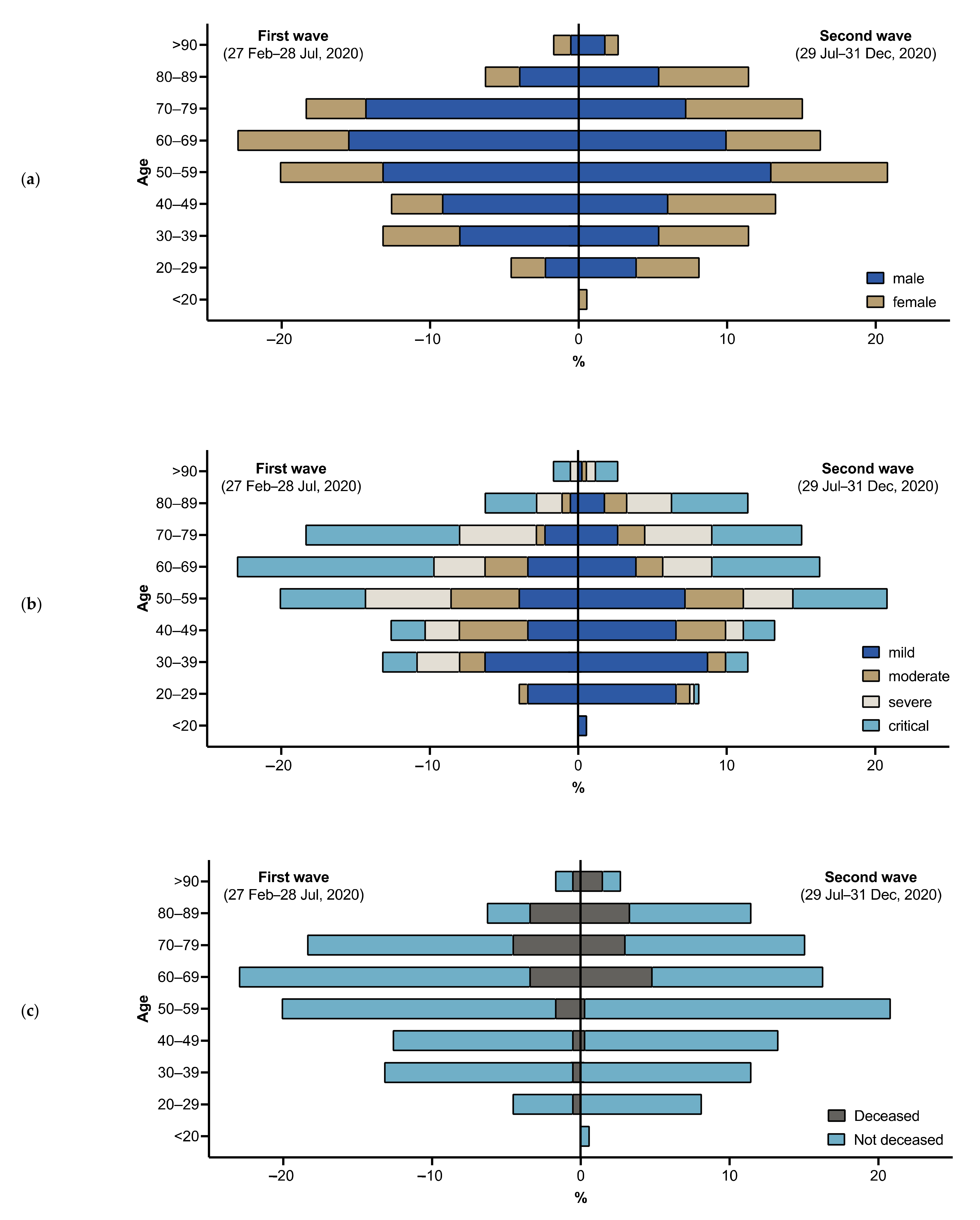
3.2. Demographic Information and Comorbidities
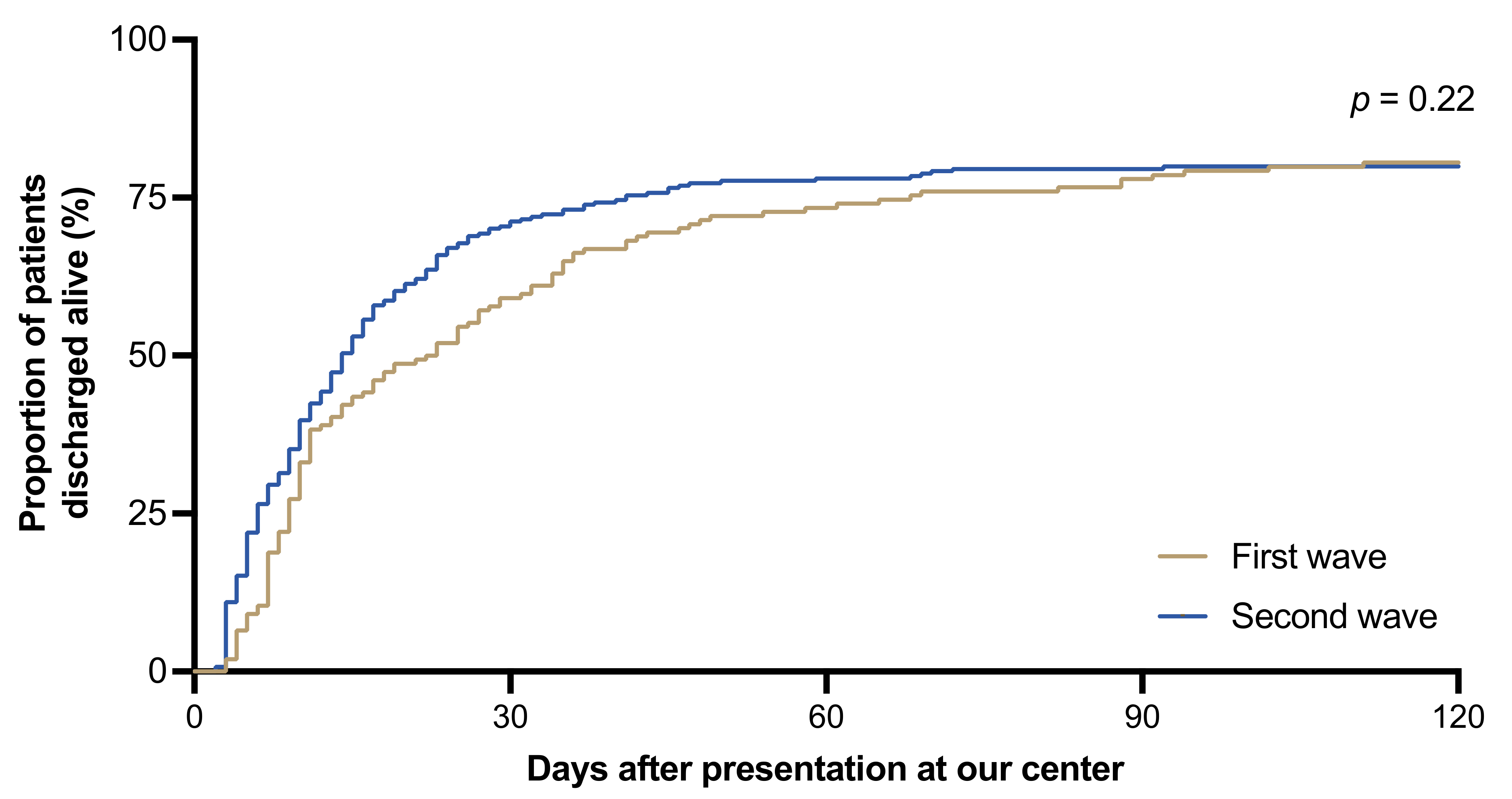
3.3. Course of Disease
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 23 April 2021).
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfefferle, S.; Günther, T.; Kobbe, R.; Czech-Sioli, M.; Nörz, D.; Santer, R.; Oh, J.; Kluge, S.; Oestereich, L.; Peldschus, K.; et al. SARS Coronavirus-2 variant tracing within the first Coronavirus Disease 19 clusters in northern Germany. Clin. Microbiol. Infect. 2021, 27, 130.e5–130.e8. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Disease 2019 (COVID-19) Daily Situation Report of the Robert Koch Institute 10/04/2020—Updated Status for Germany. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/2020-04-10-en.pdf?__blob=publicationFile (accessed on 23 April 2021).
- Coronavirus Disease 2019 (COVID-19) Daily Situation Report of the Robert Koch Institute. 31/12/2020—Updated Status for Germany. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Dez_2020/2020-12-31-en.pdf?__blob=publicationFile (accessed on 23 April 2021).
- Coronavirus Disease 2019 (COVID-19) Daily Situation Report of the Robert Koch Institute, 15/04/2020—Updated Status for Germany. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Apr_2021/2021-04-15-en.pdf?__blob=publicationFile (accessed on 23 April 2021).
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Mellan, T.A.; Coupland, H.; Whittaker, C.; Zhu, H.; Berah, T.; Eaton, J.W.; et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature 2020, 584, 257–261. [Google Scholar] [CrossRef] [PubMed]
- S3-Leitlinie—Empfehlungen zur Stationären Therapie von Patienten mit COVID-19. Available online: https://www.awmf.org/uploads/tx_szleitlinien/113-001l_S3_Empfehlungen-zur-stationaeren-Therapie-von-Patienten-mit-COVID-19__2021-04.pdf (accessed on 23 April 2021).
- Brehm, T.T.; van der Meirschen, M.; Hennigs, A.; Roedl, K.; Jarczak, D.; Wichmann, D.; Frings, D.; Nierhaus, A.; Oqueka, T.; Fiedler, W.; et al. Comparison of clinical characteristics and disease outcome of COVID-19 and seasonal influenza. Sci. Rep. 2021, 11, 5803. [Google Scholar] [CrossRef]
- Robert Koch-Institut: COVID-19-Dashboard. Available online: https://experience.arcgis.com/experience/478220a4c454480e823b17327b2bf1d4/page/page_1/ (accessed on 23 April 2021).
- Nörz, D.; Fischer, N.; Schultze, A.; Kluge, S.; Mayer-Runge, U.; Aepfelbacher, M.; Pfefferle, S.; Lütgehetmann, M. Clinical evaluation of a SARS-CoV-2 RT-PCR assay on a fully automated system for rapid on-demand testing in the hospital setting. J. Clin. Virol. 2020, 128, 104390. [Google Scholar] [CrossRef]
- Pfefferle, S.; Reucher, S.; Nörz, D.; Lütgehetmann, M. Evaluation of a quantitative RT-PCR assay for the detection of the emerging coronavirus SARS-CoV-2 using a high throughput system. Euro Surveill. 2020, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Gutiérrez-González, E.; Cantero-Escribano, J.M.; Redondo-Bravo, L.; San Juan-Sanz, I.; Robustillo-Rodela, A.; Cendejas-Bueno, E.; Influenza Working Group. Effect of vaccination, comorbidities and age on mortality and severe disease associated with influenza during the season 2016–2017 in a Spanish tertiary hospital. J. Infect. Public Health 2019, 12, 486–491. [Google Scholar] [CrossRef] [PubMed]
- WHO COVID-19 Clinical Management: Living Guidance. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1 (accessed on 23 April 2021).
- Navaratnam, A.V.; Gray, W.K.; Day, J.; Wendon, J.; Briggs, T.W.R. Patient factors and temporal trends associated with COVID-19 in-hospital mortality in England: An observational study using administrative data. Lancet Respir. Med. 2021, 9, 397–406. [Google Scholar] [CrossRef]
- Salama, C.; Han, J.; Yau, L.; Reiss, W.G.; Kramer, B.; Neidhart, J.D.; Criner, G.J.; Kaplan-Lewis, E.; Baden, R.; Pandit, L.; et al. Tocilizumab in patients hospitalized with Covid-19 pneumonia. N. Engl. J. Med. 2021, 384, 20–30. [Google Scholar] [CrossRef]
- Karakas, M.; Jarczak, D.; Becker, M.; Roedl, K.; Addo, M.M.; Hein, F.; Bergmann, A.; Zimmermann, J.; Simon, T.P.; Marx, G.; et al. Targeting endothelial dysfunction in eight extreme-critically ill patients with COVID-19 using the anti-adrenomedullin antibody adrecizumab (HAM8101). Biomolecules 2020, 10, 1171. [Google Scholar] [CrossRef] [PubMed]
- Recovery Collaborative Group. Lopinavir-Ritonavir in patients admitted to hospital with COVID-19 (Recovery): A randomised, controlled, open-label, platform trial. Lancet 2020, 396, 1345–1352. [Google Scholar] [CrossRef]
- Horby, P.; Mafham, M.; Linsell, L.; Bell, J.L.; Staplin, N.; Emberson, J.R.; Wiselka, M.; Ustianowski, A.; Elmahi, E.; Prudon, B.; et al. Effect of hydroxychloroquine in hospitalized patients with Covid-19. N. Engl. J. Med. 2020, 383, 2030–2040. [Google Scholar] [CrossRef]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in hospitalized patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Kluge, S.; Janssens, U.; Welte, T.; Weber-Carstens, S.; Schälte, G.; Salzberger, B.; Gastmeier, P.; Langer, F.; Wepler, M.; Westhoff, M.; et al. German recommendations for treatment of critically ill patients with COVID-19—Version 3: S1-Guideline. Anaesthesist 2020, 69, 653–664. [Google Scholar] [CrossRef] [PubMed]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of Covid-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Pan, H.; Peto, R.; Henao-Restrepo, A.M.; Preziosi, M.P.; Sathiyamoorthy, V.; Abdool Karim, Q.; Alejandria, M.M.; Hernández García, C.; Kieny, M.P.; Malekzadeh, R.; et al. Repurposed antiviral drugs for Covid-19—Interim WHO solidarity trial results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, C.; Hentschker, C.; Westhoff, M.; Weber-Carstens, S.; Janssens, U.; Kluge, S.; Pfeifer, M.; Spies, C.; Welte, T.; Rossaint, R.; et al. Changes in utilization and outcomes of mechanical ventilation of COVID-19 during the course of the pandemic in Germany in 2020: An observational study of 7490 patients. medRxiv 2021. [Google Scholar] [CrossRef]
- Epidemiologisches Bulletin 18/2021 des Robert Koch-Institutes. Available online: https://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2021/Ausgaben/18_21.pdf?__blob=publicationFile (accessed on 23 April 2021).
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk stratification of patients admitted to hospital with Covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Development and validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef]
- Brehm, T.T.; Schwinge, D.; Lampalzer, S.; Schlicker, V.; Küchen, J.; Thompson, M.; Ullrich, F.; Huber, S.; Schmiedel, S.; Addo, M.M.; et al. Seroprevalence of SARS-CoV-2 antibodies among hospital workers in a German tertiary care center: A sequential follow-up study. Int. J. Hyg. Environ. Health 2021, 232, 113671. [Google Scholar] [CrossRef]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Black, J.R.M.; Bailey, C.; Przewrocka, J.; Dijkstra, K.K.; Swanton, C. COVID-19: The case for health-care worker screening to prevent hospital transmission. Lancet 2020, 395, 1418–1420. [Google Scholar] [CrossRef]
- Rieg, S.; von Cube, M.; Kalbhenn, J.; Utzolino, S.; Pernice, K.; Bechet, L.; Baur, J.; Lang, C.N.; Wagner, D.; Wolkewitz, M.; et al. COVID-19 in-hospital mortality and mode of death in a dynamic and non-restricted tertiary care model in Germany. PLoS ONE 2020, 15, e0242127. [Google Scholar] [CrossRef] [PubMed]
- Nachtigall, I.; Lenga, P.; Jóźwiak, K.; Thürmann, P.; Meier-Hellmann, A.; Kuhlen, R.; Brederlau, J.; Bauer, T.; Tebbenjohanns, J.; Schwegmann, K.; et al. Clinical course and factors associated with outcomes among 1904 patients hospitalized with COVID-19 in Germany: An observational study. Clin. Microbiol. Infect. 2020, 26, 1663–1669. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Mostert, C.; Hentschker, C.; Voshaar, T.; Malzahn, J.; Schillinger, G.; Klauber, J.; Janssens, U.; Marx, G.; Weber-Carstens, S.; et al. Case characteristics, resource use, and outcomes of 10,021 patients with COVID-19 admitted to 920 German hospitals: An observational study. Lancet Respir. Med. 2020, 8, 853–862. [Google Scholar] [CrossRef]
- Ludwig, M.; Jacob, J.; Basedow, F.; Andersohn, F.; Walker, J. Clinical outcomes and characteristics of patients hospitalized for Influenza or COVID-19 in Germany. Int. J. Infect. Dis. 2021, 103, 316–322. [Google Scholar] [CrossRef]
- Budweiser, S.; Baş, Ş.; Jörres, R.A.; Engelhardt, S.; Thilo, C.; von Delius, S.; Eckel, F.; Biller, U.; Lenherr, K.; Deerberg-Wittram, J.; et al. Comparison of the first and second waves of hospitalized patients with SARS-CoV-2. Dtsch. Arztebl. Int. 2021, 118, 326–327. [Google Scholar] [CrossRef]
- Roedl, K.; Jarczak, D.; Thasler, L.; Bachmann, M.; Schulte, F.; Bein, B.; Weber, C.F.; Schäfer, U.; Veit, C.; Hauber, H.P.; et al. Mechanical ventilation and mortality among 223 critically ill patients with coronavirus disease 2019: A multicentric study in Germany. Aust. Crit. Care 2021, 34, 167–175. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Windisch, W.; McAuley, D.F.; Welte, T.; Busse, R. Major differences in ICU admissions during the first and second COVID-19 wave in Germany. Lancet Respir. Med. 2021, 9, e47–e48. [Google Scholar] [CrossRef]
- Sorci, G.; Faivre, B.; Morand, S. Explaining among-country variation in COVID-19 case fatality rate. Sci. Rep. 2020, 10, 18909. [Google Scholar] [CrossRef]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef] [PubMed]
- In-Hospital Mortality Among Hospital Confirmed COVID-19 Encounters by Week From Selected Hospitals. Available online: https://www.cdc.gov/nchs/covid19/nhcs/hospital-mortality-by-week.htm (accessed on 23 April 2021).
- Ranzani, O.T.; Bastos, L.S.L.; Gelli, J.G.M.; Marchesi, J.F.; Baião, F.; Hamacher, S.; Bozza, F.A. Characterisation of the first 250,000 hospital admissions for COVID-19 in Brazil: A retrospective analysis of nationwide data. Lancet Respir. Med. 2021, 9, 407–418. [Google Scholar] [CrossRef]
- Ticinesi, A.; Nouvenne, A.; Cerundolo, N.; Parise, A.; Prati, B.; Guerra, A.; Meschi, T. Trends of COVID-19 admissions in an Italian hub during the pandemic peak: Large retrospective study focused on older subjects. J. Clin. Med. 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Emmons-Bell, S.; Alger, H.M.; Bradley, S.M.; Das, S.R.; de Lemos, J.A.; Gakidou, E.; Elkind, M.S.V.; Hay, S.; Hall, J.L.; et al. Trends in patient characteristics and COVID-19 in-hospital mortality in the United States during the COVID-19 pandemic. JAMA Netw. Open 2021, 4, e218828. [Google Scholar] [CrossRef]
- Coronavirus Disease 2019 (COVID-19) Daily Situation Report of the Robert Koch Institute. 5 January 2021—Updated Status for Germany. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Jan_2021/2021-01-05-en.pdf?__blob=publicationFile (accessed on 23 April 2021).
- Iftimie, S.; López-Azcona, A.F.; Vallverdú, I.; Hernández-Flix, S.; de Febrer, G.; Parra, S.; Hernández-Aguilera, A.; Riu, F.; Joven, J.; Andreychuk, N.; et al. First and second waves of coronavirus disease-19: A comparative study in hospitalized patients in Reus, Spain. PLoS ONE 2021, 16, e0248029. [Google Scholar] [CrossRef] [PubMed]
- Seong, H.; Hyun, H.J.; Yun, J.G.; Noh, J.Y.; Cheong, H.J.; Kim, W.J.; Song, J.Y. Comparison of the second and third waves of the COVID-19 pandemic in South Korea: Importance of early public health intervention. Int. J. Infect. Dis. 2021, 104, 742–745. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A.; Axfors, C.; Contopoulos-Ioannidis, D.G. Second versus first wave of COVID-19 deaths: Shifts in age distribution and in nursing home fatalities. Environ. Res. 2021, 195, 110856. [Google Scholar] [CrossRef]
- Bericht zu Virusvarianten von SARS-CoV-2 in Deutschland, Insbesondere zur Variant of Concern (VOC) B.1.1.7. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/DESH/Bericht_VOC_05022021.pdf?__blob=publicationFile (accessed on 23 April 2021).
- Esper, F.P.; Cheng, Y.W.; Adhikari, T.M.; Tu, Z.J.; Li, D.; Li, E.A.; Farkas, D.H.; Procop, G.W.; Ko, J.S.; Chan, T.A.; et al. Genomic epidemiology of SARS-CoV-2 infection during the initial pandemic wave and association with disease severity. JAMA Netw. Open 2021, 4, e217746. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Patients | First Wave (27 February–28 July) | Second Wave (29 July–31 December) | p | |
|---|---|---|---|---|
| Total | 505 | 174 | 331 | |
| Male, n (%) | 292 (58) | 117 (67) | 175 (53) | 0.002 |
| Age, median (IQR) | 58 (43, 72) | 59 (46, 71) | 58 (42, 73) | 0.82 |
| Age < 60, n (%) | 268 (53) | 88 (51) | 180 (54) | 0.03 |
| Age 60–79, n (%) | 176 (35) | 72 (41) | 104 (31) | |
| Age ≥ 80, n (%) | 61 (12) | 14 (8) | 47 (14) | |
| ACCI, median (IQR) | 2 (2, 4) | 2 (1, 4) | 2 (0, 4) | 0.50 |
| All Patients | First Wave (27 February–28 July) | Second Wave (29 July–31 December) | p | |
|---|---|---|---|---|
| Disease severity, n (%) | ||||
| Mild | 169 (33) | 41 (24) | 128 (39) | 0.005 |
| Moderate | 76 (15) | 27 (16) | 49 (15) | |
| Severe | 92 (18) | 38 (22) | 54 (16) | |
| Critical | 168 (33) | 68 (39) | 100 (30) | |
| Location of treatment, n (%) | ||||
| Outpatient treatment | 87 (17) | 20 (11) | 67 (20) | 0.002 |
| Regular ward | 247 (49) | 79 (45) | 168 (51) | |
| ICU | 171 (34) | 75 (43) | 96 (29) | |
| Duration of hospitalization, median (IQR) | 11 (6–23) | 14 (8–34) | 11 (5–19) | <0.001 |
| Hospital course, n (%) | ||||
| Nosocomial infection | 28 (6) | 24 (14) | 4 (1) | <0.001 |
| Transferred to our center | 76 (15) | 29 (17) | 47 (14) | 0.51 |
| HFNC | 65 (13) | 28 (16) | 37 (11) | 0.13 |
| NIV | 47 (9) | 8 (5) | 39 (12) | 0.009 |
| Mechanical ventilation | 123 (24) | 56 (32) | 67 (20) | 0.004 |
| Vasopressor treatment | 136 (27) | 60 (34) | 76 (23) | 0.006 |
| Antibiotic treatment | 262 (52) | 114 (66) | 148 (45) | <0.001 |
| RRT | 84 (17) | 37 (21) | 47 (14) | 0.045 |
| ECMO | 50 (10) | 13 (7) | 37 (11) | 0.21 |
| Death | 81 (16) | 27 (16) | 54 (16) | 0.89 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brehm, T.T.; Heyer, A.; Roedl, K.; Jarczak, D.; Nierhaus, A.; Nentwich, M.F.; van der Meirschen, M.; Schultze, A.; Christner, M.; Fiedler, W.; et al. Patient Characteristics and Clinical Course of COVID-19 Patients Treated at a German Tertiary Center during the First and Second Waves in the Year 2020. J. Clin. Med. 2021, 10, 2274. https://doi.org/10.3390/jcm10112274
Brehm TT, Heyer A, Roedl K, Jarczak D, Nierhaus A, Nentwich MF, van der Meirschen M, Schultze A, Christner M, Fiedler W, et al. Patient Characteristics and Clinical Course of COVID-19 Patients Treated at a German Tertiary Center during the First and Second Waves in the Year 2020. Journal of Clinical Medicine. 2021; 10(11):2274. https://doi.org/10.3390/jcm10112274
Chicago/Turabian StyleBrehm, Thomas Theo, Andreas Heyer, Kevin Roedl, Dominik Jarczak, Axel Nierhaus, Michael F Nentwich, Marc van der Meirschen, Alexander Schultze, Martin Christner, Walter Fiedler, and et al. 2021. "Patient Characteristics and Clinical Course of COVID-19 Patients Treated at a German Tertiary Center during the First and Second Waves in the Year 2020" Journal of Clinical Medicine 10, no. 11: 2274. https://doi.org/10.3390/jcm10112274