
Epidemiology, Clinical Presentation and Treatment of Non-Hepatic Hyperammonemia in ICU COVID-19 Patients

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
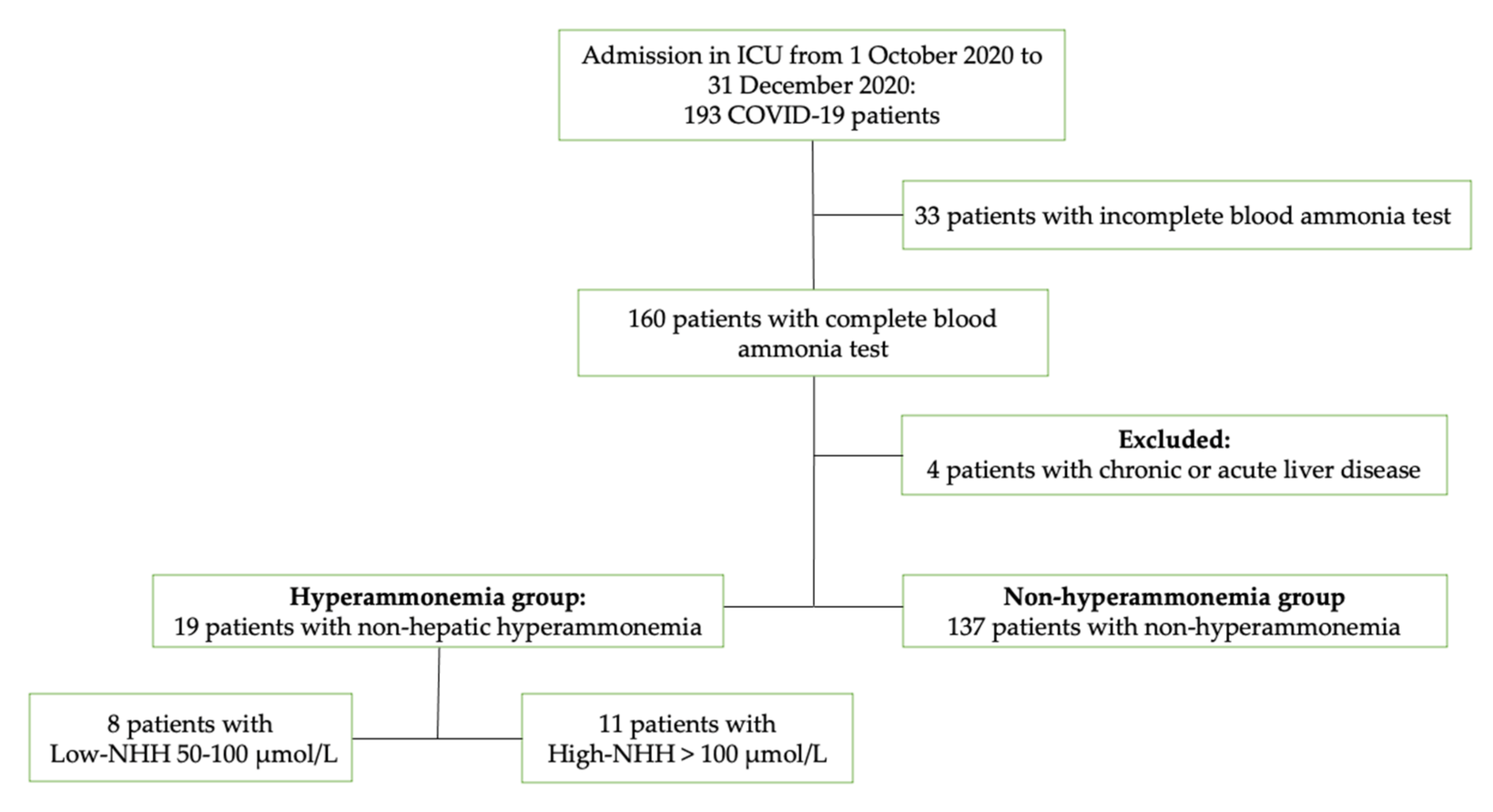
2.1. Study Design and Participants
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Risk Factors for NHH
3.2. Low-NHH vs. High-NHH
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 21 March 2021).
- CDC. Interim Infection Prevention and Control Recommendations for Healthcare Personnel During the Coronavirus Disease 2019 (COVID-19) Pandemic. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html (accessed on 21 March 2021).
- Jacoby, K.J.; Singh, P.; Prekker, M.E.; Leatherman, J.W. Characteristics and Outcomes of Critically Ill Patients with Severe Hyperammonemia. J. Crit. Care 2020, 56, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Walker, V. Ammonia Metabolism and Hyperammonemic Disorders, 1st ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2014; Volume 67. [Google Scholar]
- Triplett, K.E.; Murray, R.; Anstey, M. Multifactorial Non-Cirrhotic Hyperammonaemic Encephalopathy. BMJ Case Rep. 2018, 2018, 2017–2019. [Google Scholar] [CrossRef] [PubMed]
- Clay, A.S.; Hainline, B.E. Hyperammonemia in the ICU. Chest 2007, 132, 1368–1378. [Google Scholar] [CrossRef] [PubMed]
- Sakusic, A.; Sabov, M.; Mccambridge, A.J.; Singh, T.D.; Mukesh, K.; Kashani, K.B.; Cook, D.; Gajic, O.; Medicine, P.; Faculty, M.; et al. Features of Adult Hyperammonemia Not Due to Liver Failure in the Intensive Care Unit. Crit. Care Med. 2019, 46, e897–e903. [Google Scholar] [CrossRef] [PubMed]
- Bobermin, L.D.; Quincozes-Santos, A. COVID-19 and Hyperammonemia: Potential Interplay between Liver and Brain Dysfunctions. Brain Behav. Immun. Health 2021, 14, 100257. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.S.; Pereira, R.; Germano, N. Liver Injury in Critically Ill Patients with COVID-19: A Case Series. Crit. Care 2020, 24, 190. [Google Scholar] [CrossRef] [PubMed]
- Gamboa, E.; Montelongo, D.; Berjaoui, H.; Varon, D.S.; Gathe, J.C.; Varon, J. COVID-19-Induced Hepatic Encephalopathy: A Case Report. Crit. Care Shock 2020, 23, 154–157. [Google Scholar]
- Zhao, L.; Walline, J.H.; Gao, Y.; Lu, X.; Yu, S.; Ge, Z.; Zhu, H.; Li, Y. Prognostic Role of Ammonia in Critical Care Patients Without Known Hepatic Disease. Front. Med. 2020, 7, 589825. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Gao, Y.; Guo, S.; Lu, X.; Yu, S.; Ge, Z.; Zhu, H.; Li, Y. Prognosis of Patients with Sepsis and Non-Hepatic Hyperammonemia: A Cohort Study. Med. Sci. Monit. 2020, 27, e928573. [Google Scholar] [CrossRef] [PubMed]
- Maher, D.; Chapman, K. Rare Case of Mortality From Non-Cirrhotic Hyperammonemia. Chest 2019, 156, A2125. [Google Scholar] [CrossRef]
- Deska Pagana, K.; Pagana, T.J.; Pagana, T.N. Ammonia. Mosby’s Diagnostic and Laboratory Test Reference, 13th ed.; Elsevier: St. Louis, MO, USA, 2017. [Google Scholar]
- Kalra, A.; Norvell, J.P. Cause for Confusion: Noncirrhotic Hyperammonemic Encephalopathy. Clin. Liver Dis. 2020, 15, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Honore, P.M.; Barreto Gutierrez, L.; Kugener, L.; Redant, S.; Attou, R.; Gallerani, A.; de Bels, D. Liver Injury without Liver Failure in COVID-19 Patients: How to Explain, in Some Cases, Elevated Ammonia without Hepatic Decompensation. Crit. Care 2020, 24, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Falasca, L.; Nardacci, R.; Colombo, D.; Lalle, E.; di Caro, A.; Nicastri, E.; Antinori, A.; Petrosillo, N.; Marchioni, L.; Biava, G.; et al. Postmortem Findings in Italian Patients with COVID-19: A Descriptive Full Autopsy Study of Cases with and without Comorbidities. J. Infect. Dis. 2020, 222, 1807–1815. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Lkhagva, E.; Chung, H.J.; Kim, H.J.; Hong, S.T. The Pharmabiotic Approach to Treat Hyperammonemia. Nutrients 2018, 10, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| ICU COVID-19 Patients | NHH Group | Non-NHH Group | |
|---|---|---|---|
| Characteristics | 156 | 19 | 137 |
| Age, median (IQR) | 68 (58–76) | 68 (60–76.5) | 68 (58–76) |
| Male, n (%) | 115 (73.7) | 15 (79) | 100 (73) |
| Female, n (%) | 41 (26.3) | 4 (21) | 37 (27) |
| BMI, median (IQR) | 27.7 (25.4–31) | 27.3 (24.3–29) | 27.8 (25.7–31) |
| SOFA score, median (IQR) | 4 (3–7) | 5 (3–6.5) | 4 (3–7) |
| APACHE II score, median (IQR) | 12 (8–18) | 11 (8.5–15) | 12 (8–18.2) |
| ICU Patients | NHH Group | Univariate | Multivariate | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | aOR (95% CI) | p | |||
| 156 | 19 (12.2) | |||||
| Age > 70 years old | 67 | 8 (11.9) | 0.96 (0.36–2.54) | 0.937 | ||
| Male (vs. female), n (%) | 115 | 15 (13) | 1.39 (0.43–4.45) | 0.581 | ||
| SOFA score ≥ 4 | 86 | 13 (19) | 1.9 (0.68–5.29) | 0.214 | ||
| APACHE II score ≥ 10 | 97 | 12 (12.4) | 1.05 (0.39–2.83) | 0.925 | ||
| Comorbidities, n (%) | ||||||
| Arterial hypertension | 77 | 12 (15.6) | 1.89 (0.7–5.1) | 0.199 | ||
| Cardiovascular diseases | 37 | 7 (18.9) | 2.08 (0.75–5.75) | 0.151 | ||
| Diabetes | 24 | 4 (16.7) | 1.56 (0.47–5.18) | 0.465 | ||
| Obesity a | 57 | 5 (8.8) | 0.58 (0.19–1.71) | 0.323 | ||
| Chronic renal disease b | 6 | 1 (16.7) | 1.47 (0.16–13.3) | 0.732 | ||
| Hemodialysis | 5 | 1 (20.0) | 1.85 (0.19–17.4) | 0.587 | ||
| Chronic lung disease | 23 | 6 (26.1) | 2.51 (1.09–9.71) | 0.103 | ||
| Previous neoplasm c | 13 | 2 (15.4) | 1.35 (0.27–6.60) | 0.712 | ||
| Chronic neurological disorders | 11 | 2 (18.2) | 1.67 (0.33–8.4) | 0.528 | ||
| Autoimmune diseases | 13 | 2 (15.4) | 1.35 (0.27–6.6) | 0.712 | ||
| Other chronical diseases | 22 | 3 (13.6) | 1.16 (0.31–4.38) | 0.822 | ||
| Clinical characteristics | ||||||
| Pre-ICU hospitalization ≥ 7 days | 44 | 4 (9.1) | 0.65 (0.20–2.07) | 0.460 | ||
| PaO2/FiO2 ≤ 100 mmHg | 16 | 4 (25) | 2.78 (0.79–9.71) | 0.098 | ||
| Invasive mechanical ventilation | 118 | 18 (15.3) | 6.66 (0.86–51.6) | 0.039 | 7.1 (0.90–56.4) | 0.062 |
| ICU length of stay > 28 days | 55 | 8 (14.5) | 1.39 (0.52–3.69) | 0.505 | ||
| 28-day ICU mortality | 49 | 5 (10.2) | 0.75 (0.25–2.23) | 0.610 | ||
| Overall ICU mortality | 57 | 6 (10.5) | 0.778 (0.28–2.2) | 0.632 | ||
| NHH Group (19) | L-NHH | H-NHH | p | |
|---|---|---|---|---|
| No. | 19 | 8 | 11 | |
| Age, median (IQR) | 68 (60–76.5) | 71 (58.5–76.5) | 66 (61.5–73.5) | 0.868 |
| Male, n (%) | 15 (79%) | 6 (75) | 9 (81.8) | 0.737 |
| Female, n (%) | 4 (21%) | 2 (25) | 2 (18.2) | 0.737 |
| BMI, median (IQR) | 27.3 (24.3–29) | 27.7 (26.8–27.7) | 26.8 (23.1–28.2) | 0.078 |
| SOFA score, median (IQR) | 5 (3–6.5) | 5 (3–6) | 5 (3.5–6.5) | 0.883 |
| APACHE II score, median (IQR) | 11 (8.5–15) | 12 (8.7–17.2) | 11 (8.5–14) | 0.579 |
| Comorbidities, n (%) | ||||
| Arterial hypertension | 12 (63.1%) | 6 (75) | 6 (45.5) | 0.390 |
| Cardiovascular diseases | 7 (36.8%) | 4 (50) | 3 (27.7) | 0.338 |
| Diabetes | 4 (21.0%) | 2 (25) | 2 (18.2) | 0.737 |
| Obesity a | 5 (26.3%) | 3 (37.5) | 2 (18.2) | 0.373 |
| Kidney disease b | 1 (5.3%) | 1 (12.5) | 0 (0) | N.A. |
| Hemodialysis | 1 (5.3) | 1 (12.5) | 0 (0) | N.A. |
| Chronic lung disease | 6 (31.6%) | 2 (25) | 4 (36.4) | 0.623 |
| Previous neoplasm c | 3 (15.7%) | 1 (12.5) | 2 (18.2) | 0.824 |
| Chronic neurological disorders | 2 (10.5%) | 0 (0) | 2 (18.2) | N.A. |
| Autoimmune diseases | 2 (10.5%) | 1 (12.5) | 1 (9.1) | 0.824 |
| Other chronical diseases | 3 (29.0%) | 2 (25) | 1 (9.1) | 0.376 |
| Clinical characteristics, no. (%) | ||||
| Pre-ICU hospitalization ≥ 7 days | 4 (21) | 0 (0) | 4 (36.4) | N.A. |
| PaO2/FiO2 ≤ 100 mmHg | 4 (21) | 3 (37.5) | 1 (9.1) | 0.149 |
| Invasive mechanical ventilation | 18 (94.7) | 7 (87.5) | 11 (100) | N.A. |
| ICU length of stay > 28 days | 8 (42) | 3 (37.5) | 5 (45.5) | 0.746 |
| ICU mortality, no (%) | ||||
| 28-day ICU mortality | 5 (26.3) | 3 (37.5) | 2 (18.2) | 0.373 |
| Overall ICU mortality | 6 (31.6) | 3 (37.5) | 3 (27.3) | 0.658 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tetaj, N.; Stazi, G.V.; Marini, M.C.; Garotto, G.; Busso, D.; Scarcia, S.; Caravella, I.; Macchione, M.; De Angelis, G.; Di Lorenzo, R.; et al. Epidemiology, Clinical Presentation and Treatment of Non-Hepatic Hyperammonemia in ICU COVID-19 Patients. J. Clin. Med. 2022, 11, 2592. https://doi.org/10.3390/jcm11092592
Tetaj N, Stazi GV, Marini MC, Garotto G, Busso D, Scarcia S, Caravella I, Macchione M, De Angelis G, Di Lorenzo R, et al. Epidemiology, Clinical Presentation and Treatment of Non-Hepatic Hyperammonemia in ICU COVID-19 Patients. Journal of Clinical Medicine. 2022; 11(9):2592. https://doi.org/10.3390/jcm11092592
Chicago/Turabian StyleTetaj, Nardi, Giulia Valeria Stazi, Maria Cristina Marini, Gabriele Garotto, Donatella Busso, Silvana Scarcia, Ilaria Caravella, Manuela Macchione, Giada De Angelis, Rachele Di Lorenzo, and et al. 2022. "Epidemiology, Clinical Presentation and Treatment of Non-Hepatic Hyperammonemia in ICU COVID-19 Patients" Journal of Clinical Medicine 11, no. 9: 2592. https://doi.org/10.3390/jcm11092592