
Associated Factors of High Sedative Requirements within Patients with Moderate to Severe COVID-19 ARDS

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
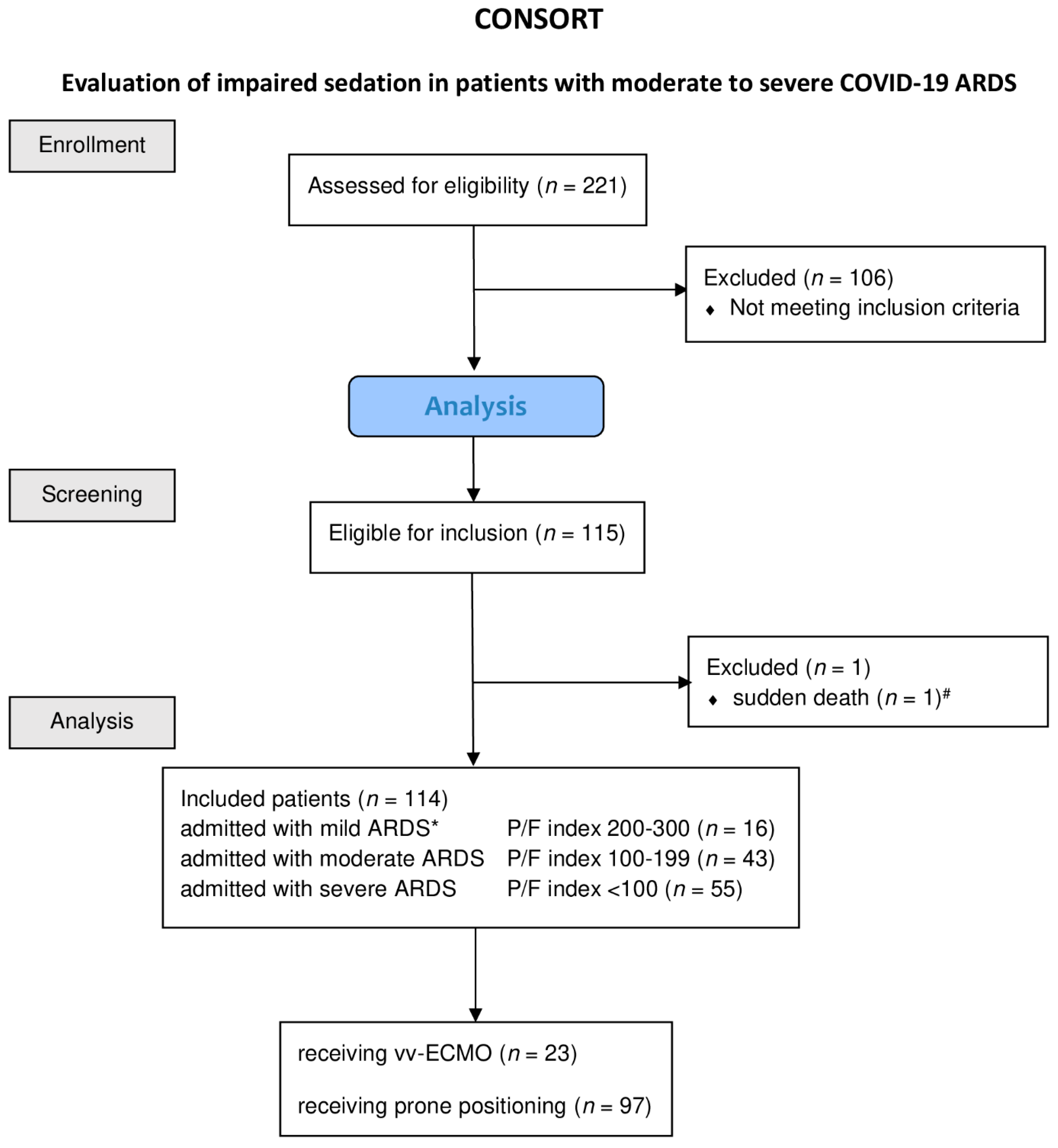
2.1. Patient Population
2.2. Data Collection
2.3. Statistical Analysis
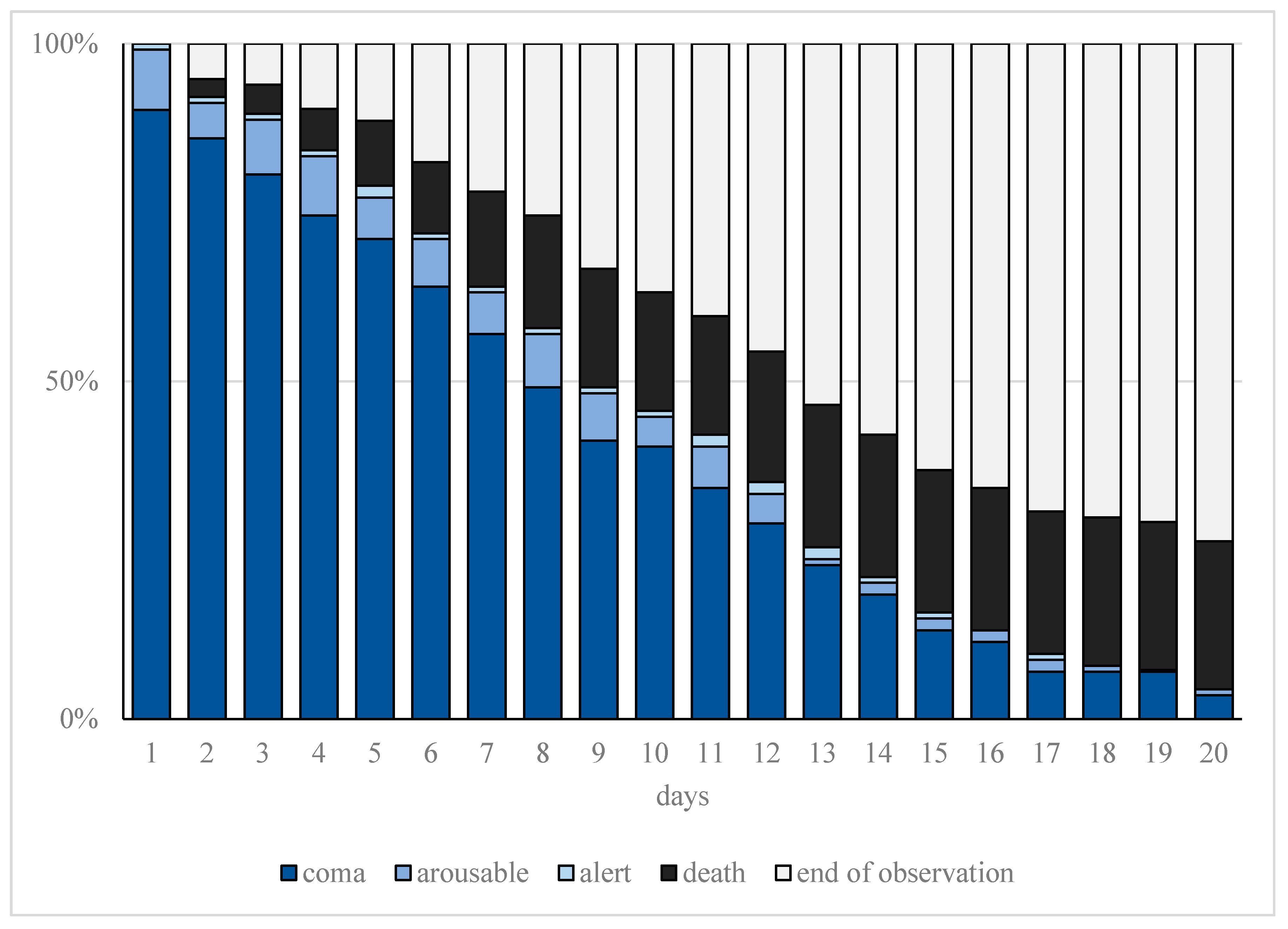
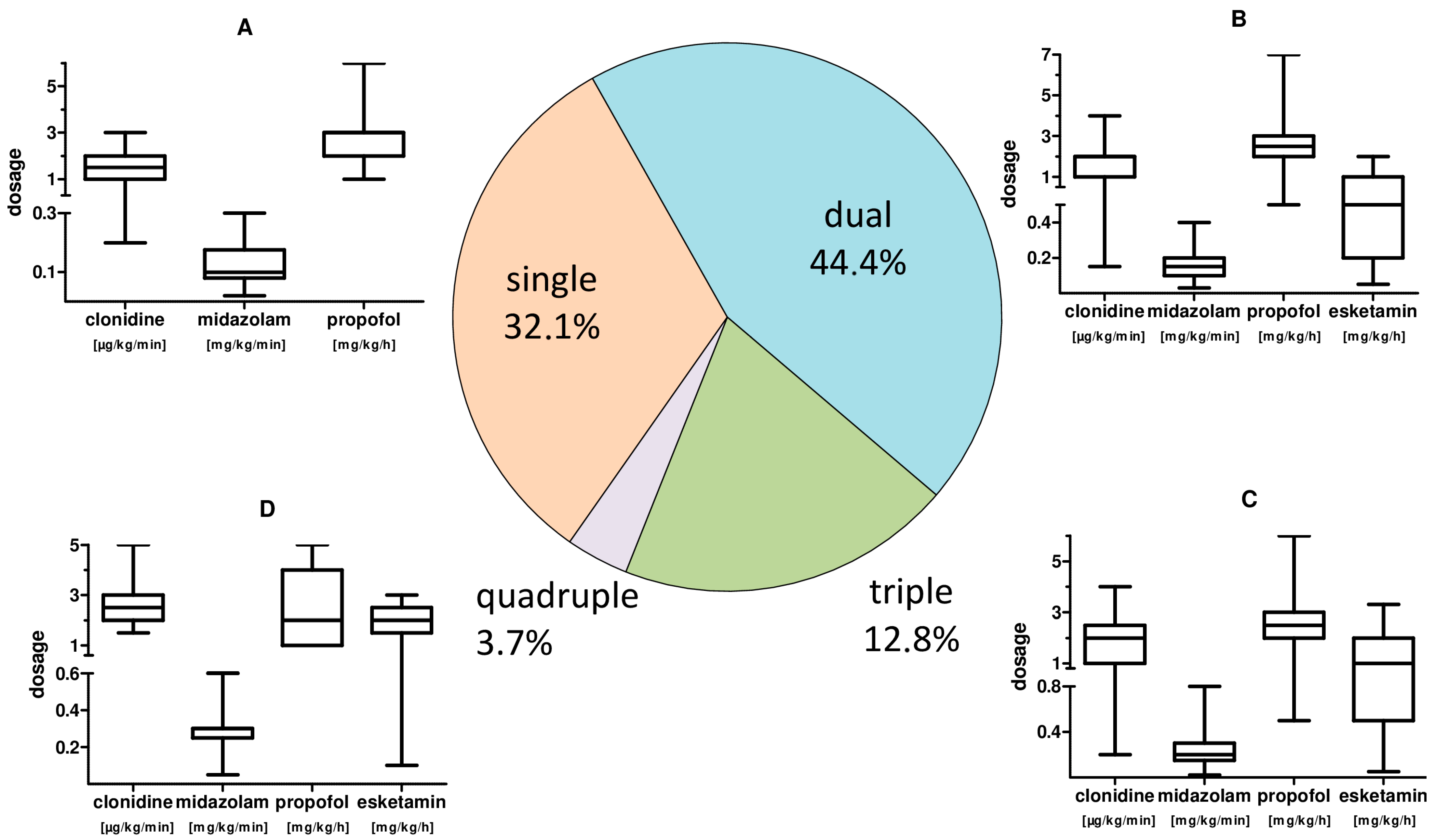
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meares, H.D.; Jones, M.P. When a system breaks: Queueing theory model of intensive care bed needs during the COVID-19 pandemic. Med. J. Aust. 2020, 212, 470. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.F.; Korevaar, D.A.; Matczak, S.; Chalumeau, M.; Allali, S.; Toubiana, J. COVID-19–Related Fatalities and Intensive-Care-Unit Admissions by Age Groups in Europe: A Meta-Analysis. Front. Med. 2020, 7, 560685. [Google Scholar] [CrossRef] [PubMed]
- Hanidziar, D.; Bittner, E.A. Sedation of Mechanically Ventilated COVID-19 Patients: Challenges and Special Considerations. Anesth. Analg. 2020, 131, e40–e41. [Google Scholar] [CrossRef] [PubMed]
- Taskforce, D.A.S.; Baron, R.; Binder, A.; Biniek, R.; Braune, S.; Buerkle, H.; Dall, P.; Demirakca, S.; Eckardt, R.; Eggers, V.; et al. Evidence and consensus based guideline for the management of delirium, analgesia, and sedation in intensive care medicine. Revision 2015 (DAS-Guideline 2015)-short version. Ger. Med. Sci. 2015, 13, Doc19. [Google Scholar] [CrossRef]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020, 48, 1–34. [Google Scholar] [CrossRef]
- Bourenne, J.; Hraiech, S.; Roch, A.; Gainnier, M.; Papazian, L.; Forel, J.M. Sedation and neuromuscular blocking agents in acute respiratory distress syndrome. Ann. Transl. Med. 2017, 5, 291. [Google Scholar] [CrossRef] [Green Version]
- Barr, J.; Fraser, G.L.; Puntillo, K.; Ely, E.W.; Gélinas, C.; Dasta, J.F.; Davidson, J.E.; Devlin, J.W.; Kress, J.P.; Joffe, A.M. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit. Care Med. 2013, 41, 263–306. [Google Scholar] [CrossRef]
- Shah, F.A.; Girard, T.D.; Yende, S. Limiting sedation for patients with acute respiratory distress syndrome-time to wake up. Curr. Opin. Crit. Care 2017, 23, 45–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nasraway, S.A.; Jacobi, J.; Murray, M.J.; Lumb, P.D. Sedation, analgesia, and neuromuscular blockade of the critically ill adult: Revised clinical practice guidelines for 2002. Crit. Care Med. 2002, 30, 117–118. [Google Scholar] [CrossRef]
- Bruce, S.S.; Kahan, J.; Huq, T.; Santillan, A.; Navi, B.B.; Merkler, A.E.; Parikh, N.S.; Mir, S.; Schweitzer, A.D.; Segal, A.Z. Missed cerebrovascular events during prolonged sedation for COVID-19 pneumonia. J. Clin. Neurosci. 2021, 86, 180–183. [Google Scholar] [CrossRef]
- Ziehr, D.R.; Alladina, J.; Petri, C.R.; Maley, J.H.; Moskowitz, A.; Medoff, B.D.; Hibbert, K.A.; Thompson, B.T.; Hardin, C.C. Respiratory pathophysiology of mechanically ventilated patients with COVID-19: A cohort study. Am. J. Respir. Crit. Care Med. 2020, 12, 1560–1564. [Google Scholar] [CrossRef] [PubMed]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Kapp, C.M.; Zaeh, S.; Niedermeyer, S.; Punjabi, N.M.; Siddharthan, T.; Damarla, M. The use of analgesia and sedation in mechanically ventilated patients with COVID-19 ARDS. Anesth. Analg. 2020, 131, e198–e200. [Google Scholar] [CrossRef]
- Flinspach, A.N.; Zacharowski, K.; Ioanna, D.; Adam, E.H. Volatile Isoflurane in Critically Ill Coronavirus Disease 2019 Patients—A Case Series and Systematic Review. Crit. Care Explor. 2020, 2, e0256. [Google Scholar] [CrossRef]
- Hanidziar, D.; Baldyga, K.; Ji, C.S.; Lu, J.; Zheng, H.; Wiener-Kronish, J.; Xie, Z. Standard Sedation and Sedation with Isoflurane in Mechanically Ventilated Patients With Coronavirus Disease 2019. Crit. Care Explor. 2021, 3, e0370. [Google Scholar] [CrossRef]
- Wongtangman, K.; Santer, P.; Wachtendorf, L.J.; Azimaraghi, O.; Baedorf Kassis, E.; Teja, B.; Murugappan, K.R.; Siddiqui, S.; Eikermann, M.; Group, F.T.S.O.M.T. Association of Sedation, Coma, and In-Hospital Mortality in Mechanically Ventilated Patients with Coronavirus Disease 2019–Related Acute Respiratory Distress Syndrome: A Retrospective Cohort Study. Crit. Care Med. 2021, 49, 1524–1534. [Google Scholar] [CrossRef]
- Ammar, M.A.; Sacha, G.L.; Welch, S.C.; Bass, S.N.; Kane-Gill, S.L.; Duggal, A.; Ammar, A.A. Sedation, Analgesia, and Paralysis in COVID-19 Patients in the Setting of Drug Shortages. J. Intensive Care Med. 2020, 36, 157–174. [Google Scholar] [CrossRef]
- Adams, C.D.; Altshuler, J.; Barlow, B.L.; Dixit, D.; Droege, C.A.; Effendi, M.K.; Heavner, M.S.; Johnston, J.P.; Kiskaddon, A.L.; Lemieux, D.G. Analgesia and Sedation Strategies in Mechanically Ventilated Adults with COVID-19 COVID-19. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2020, 40, 1180–1191. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D.; Group, C. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. Trials 2010, 11, 32. [Google Scholar] [CrossRef] [Green Version]
- Sethuraman, N.; Jeremiah, S.S.; Ryo, A. Interpreting Diagnostic Tests for SARS-CoV-2. JAMA 2020, 323, 2249–2251. [Google Scholar] [CrossRef] [PubMed]
- Marini, J.J.; Gattinoni, L. Management of COVID-19 Respiratory Distress. JAMA 2020, 323, 2329–2330. [Google Scholar] [CrossRef] [PubMed]
- Kluge, S.; Janssens, U.; Welte, T.; Weber-Carstens, S.; Marx, G.; Karagiannidis, C. German recommendations for critically ill patients with COVID-19. Med. Klin. Intensivmed. Und Notf. 2020, 115, 111–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhazzani, W.; Evans, L.; Alshamsi, F.; Moller, M.H.; Ostermann, M.; Prescott, H.C.; Arabi, Y.M.; Loeb, M.; Ng Gong, M.; Fan, E.; et al. Surviving Sepsis Campaign Guidelines on the Management of Adults with Coronavirus Disease 2019 (COVID-19) in the ICU: First Update. Crit. Care Med. 2021, 49, e219–e234. [Google Scholar] [CrossRef]
- Shekar, K.; Badulak, J.; Peek, G.; Boeken, U.; Dalton, H.J.; Arora, L.; Zakhary, B.; Ramanathan, K.; Starr, J.; Akkanti, B. Extracorporeal life support organization coronavirus disease 2019 interim guidelines: A consensus document from an international group of interdisciplinary extracorporeal membrane oxygenation providers. Asaio J. 2020, 66, 707–721. [Google Scholar] [CrossRef]
- Fichtner, F.; Mörer, O.; Laudi, S.; Weber-Carstens, S.; Kaisers, U. S3-Leitlinie “Invasive Beatmung und Einsatz extrakorporaler Verfahren bei akuter respiratorischer Insuffizienz”. DIVI 2017, 4, 154–163. [Google Scholar]
- López Sanchez, M. Mechanical ventilation in patients subjected to extracorporeal membrane oxygenation (ECMO). Med. Intensiva 2017, 41, 491–496. [Google Scholar] [CrossRef]
- Flinspach, A.N.; Booke, H.; Zacharowski, K.; Balaban, Ü.; Herrmann, E.; Adam, E.H. High sedation needs of critically ill COVID-19 ARDS patients—A monocentric observational study. PLoS ONE 2021, 16, e0253778. [Google Scholar] [CrossRef]
- Murias, G.; Villagra, A.; Blanch, L. Patient-ventilator dyssynchrony during assisted invasive mechanical ventilation. Minerva Anestesiol. 2013, 79, 434–444. [Google Scholar]
- Chanques, G.; Constantin, J.-M.; Devlin, J.W.; Ely, E.W.; Fraser, G.L.; Gélinas, C.; Girard, T.D.; Guérin, C.; Jabaudon, M.; Jaber, S. Analgesia and sedation in patients with ARDS. Intensive Care Med. 2020, 46, 2342–2356. [Google Scholar] [CrossRef]
- Parker, E.M.; Bittner, E.A.; Berra, L.; Pino, R.M. Efficiency of Prolonged Prone Positioning for Mechanically Ventilated Patients Infected with COVID-19. J. Clin. Med. 2021, 10, 2969. [Google Scholar] [CrossRef] [PubMed]
- Khullar, R.; Shah, S.; Singh, G.; Bae, J.; Gattu, R.; Jain, S.; Green, J.; Anandarangam, T.; Cohen, M.; Madan, N.; et al. Effects of Prone Ventilation on Oxygenation, Inflammation, and Lung Infiltrates in COVID-19 Related Acute Respiratory Distress Syndrome: A Retrospective Cohort Study. J. Clin. Med. 2020, 9, 4129. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, J.; Bates, D.; DebRoy, S.; Sarkar, D.; R Core Team. Linear and Nonlinear Mixed Effects Models; R Foundation for Statistical Computing: Vienna, Austria, 2007; Volume 3, pp. 1–89. [Google Scholar]
- Venables, W.N.R.; Brian, D. Modern Applied Statistics with S; Springer: Berlin/Heidelberg, Germany, 2002. [Google Scholar]
- Zaim, S.; Chong, J.H.; Sankaranarayanan, V.; Harky, A. COVID-19 and Multiorgan Response. Curr. Probl. Cardiol. 2020, 45, 100618. [Google Scholar] [CrossRef] [PubMed]
- Force, T.A.D.T. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Nielsen, S.; Degenhardt, L.; Hoban, B.; Gisev, N. Comparing Opioids: A Guide to Estimating Oral Morphine Equivalents (OME) in Research; National Drug and Alcohol Research Centre Sydney: Sydney, NSW, Australia, 2014. [Google Scholar]
- Wilson, W.C.; Smedira, N.G.; Fink, C.; McDowell, J.A.; Luce, J.M. Ordering and Administration of Sedatives and Analgesics during the Withholding and Withdrawal of Life Support from Critically III Patients. JAMA 1992, 267, 949–953. [Google Scholar] [CrossRef] [PubMed]
- Purivatra, E.; Guenette, M.; Coleman, B.; Cheung, A.; Burry, L. High-versus low-dose clonidine for sedation and analgesia in critically ill adults: A retrospective cohort study. J. Clin. Pharm. Ther. 2021, 46, 1706–1713. [Google Scholar] [CrossRef] [PubMed]
- Lim, Z.J.; Subramaniam, A.; Ponnapa Reddy, M.; Blecher, G.; Kadam, U.; Afroz, A.; Billah, B.; Ashwin, S.; Kubicki, M.; Bilotta, F.; et al. Case Fatality Rates for Patients with COVID-19 Requiring Invasive Mechanical Ventilation. A Meta-analysis. Am. J. Respir. Crit. Care Med. 2021, 203, 54–66. [Google Scholar] [CrossRef]
- Shekar, K.; Fraser, J.F.; Smith, M.T.; Roberts, J.A. Pharmacokinetic changes in patients receiving extracorporeal membrane oxygenation. J. Crit. Care 2012, 27, 741.e9–741.e18. [Google Scholar] [CrossRef]
- Nigoghossian, C.D.; Dzierba, A.L.; Etheridge, J.; Roberts, R.; Muir, J.; Brodie, D.; Schumaker, G.; Bacchetta, M.; Ruthazer, R.; Devlin, J.W. Effect of Extracorporeal Membrane Oxygenation Use on Sedative Requirements in Patients with Severe Acute Respiratory Distress Syndrome. Pharmacotherapy 2016, 36, 607–616. [Google Scholar] [CrossRef]
- Cheng, V.; Abdul-Aziz, M.-H.; Roberts, J.A.; Shekar, K. Optimising drug dosing in patients receiving extracorporeal membrane oxygenation. J. Thorac. Dis. 2017, 10, S629–S641. [Google Scholar] [CrossRef]
- Bauer, T.M.; Ritz, R.; Haberthür, C.; Haefeli, W.; Scollo-Lavizzari, G.; Ha, H.; Hunkeler, W.; Sleight, A. Prolonged sedation due to accumulation of conjugated metabolites of midazolam. Lancet 1995, 346, 145–147. [Google Scholar] [CrossRef]
- Diep, U.; Chudow, M.; Sunjic, K.M. Pharmacokinetic Changes in Liver Failure and Impact on Drug Therapy. AACN Adv. Crit. Care 2017, 28, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Driessen, J.J.; Vree, T.B.; Guelen, P.J. The effects of acute changes in renal function on the pharmacokinetics of midazolam during long-term infusion in ICU patients. Acta Anaesthesiol. Belg. 1991, 42, 149–155. [Google Scholar] [PubMed]
- Krassioukov, A.V.; Gelb, A.W.; Weaver, L.C. Action of propofol on central sympathetic mechanisms controlling blood pressure. Can. J. Anaesth. 1993, 40, 761–769. [Google Scholar] [CrossRef] [Green Version]
- De Backer, D.; Foulon, P. Minimizing catecholamines and optimizing perfusion. Crit. Care 2019, 23, 149. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, T.; Fujino, Y.; Amato, M.B.; Kavanagh, B.P. Fifty years of research in ARDS. Spontaneous breathing during mechanical ventilation. Risks, mechanisms, and management. Am. J. Respir. Crit. Care Med. 2017, 195, 985–992. [Google Scholar] [CrossRef]
- Putensen, C.; Zech, S.; Wrigge, H.; Zinserling, J.; Stuber, F.; von Spiegel, T.; Mutz, N. Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury. Am. J. Respir. Crit. Care Med. 2001, 164, 43–49. [Google Scholar] [CrossRef]
- Hraiech, S.; Forel, J.-M.; Papazian, L. The role of neuromuscular blockers in ARDS: Benefits and risks. Curr. Opin. Crit. Care 2012, 18, 495–502. [Google Scholar] [CrossRef]
- Gattinoni, L.; Marini, J.J. Prone positioning and neuromuscular blocking agents are part of standard care in severe ARDS patients: We are not sure. Intensive Care Med. 2015, 41, 2201–2203. [Google Scholar] [CrossRef] [Green Version]
- Guérin, C.; Mancebo, J. Prone positioning and neuromuscular blocking agents are part of standard care in severe ARDS patients: Yes. Intensive Care Med. 2015, 41, 2195–2197. [Google Scholar] [CrossRef]
- Boldrini, M.; Canoll, P.D.; Klein, R.S. How COVID-19 Affects the Brain. JAMA Psychiatry 2021, 78, 682–683. [Google Scholar] [CrossRef] [PubMed]
- Nouchi, A.; Chastang, J.; Miyara, M.; Lejeune, J.; Soares, A.; Ibanez, G.; Saadoun, D.; Morelot-Panzini, C.; Similowski, T.; Amoura, Z.; et al. Prevalence of hyposmia and hypogeusia in 390 COVID-19 hospitalized patients and outpatients: A cross-sectional study. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Gamberini, L.; Mazzoli, C.A.; Sintonen, H.; Colombo, D.; Scaramuzzo, G.; Allegri, D.; Tonetti, T.; Zani, G.; Capozzi, C.; Giampalma, E.; et al. Quality of life of COVID-19 critically ill survivors after ICU discharge: 90 days follow-up. Qual. Life Res. 2021, 30, 2805–2817. [Google Scholar] [CrossRef] [PubMed]
- Banno, A.; Hifumi, T.; Takahashi, Y.; Soh, M.; Sakaguchi, A.; Shimano, S.; Miyahara, Y.; Isokawa, S.; Ishii, K.; Aoki, K. One-Year Outcomes of Postintensive Care Syndrome in Critically Ill Coronavirus Disease 2019 Patients: A Single Institutional Study. Crit. Care Explor. 2021, 3, e0595. [Google Scholar] [CrossRef]
- Poston, J.T.; Patel, B.K.; Davis, A.M. Management of Critically Ill Adults with COVID-19. JAMA 2020, 323, 1839–1841. [Google Scholar] [CrossRef] [PubMed]
- Hemphill, S.; McMenamin, L.; Bellamy, M.C.; Hopkins, P.M. Propofol infusion syndrome: A structured literature review and analysis of published case reports. Br. J. Anaesth. 2019, 122, 448–459. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients Included n = 114 | |
|---|---|---|
| age, y | 66 | (±13.7) |
| sex, male | 88 | (77.2%) |
| bodyweight, kg * | 93.9 | (±20.7) |
| BMI * | 30.84 | (±6.7) |
| SAPS II * | 43.88 | (±10.84) |
| paO2 × FiO2−1 * | 123.7 | (±69.0) |
| median observation period, h | 242.6 | (±170.8) |
| vv-ECMO treatment | 23 | (20.2%) |
| vv-ECMO treatment time, h | 277.9 | (±254.2) |
| cRRT treatment due to AKI | 43 | (37.7%) |
| cRRT treatment time, h | 189.5 | (±135.2) |
| mortality | 65 | (57.0%) |
| coronary artery disease * | 37 | (32.5%) |
| pulmonary disease * | 35 | (30.7%) |
| diabetes * | 48 | (42.1%) |
| arterial hypertonus * | 78 | (68.4%) |
| chronic kidney disease * | 24 | (21.1%) |
| cerebrovascular events * | 15 | (13.2%) |
| Condition | Value | Standard Error | p-Value |
|---|---|---|---|
| CARDS-associated | |||
| vv-ECMO therapy | 0.050 | 0.005 | <0.001 |
| catecholamine dose | 0.013 | 0.003 | <0.001 |
| liver failure | −0.006 | 0.002 | 0.001 |
| renal failure | −0.008 | 0.003 | 0.001 |
| SAPS II on admission | 0.001 | 0.000 | 0.089 |
| Preconditions | |||
| age (years) | −0.001 | 0.000 | 0.003 |
| body mass index (kg/m2) | 0.000 | 0.001 | 0.982 |
| coronary artery disease | −0.022 | 0.011 | 0.059 |
| pulmonary disease | 0.016 | 0.010 | 0.110 |
| cerebrovascular disease | 0.022 | 0.014 | 0.130 |
| chronic kidney disease | −0.016 | 0.012 | 0.185 |
| cancer | −0.025 | 0.023 | 0.275 |
| arterial hypertonus | 0.010 | 0.012 | 0.379 |
| diabetes mellitus | −0.004 | 0.010 | 0.686 |
| peripheral artery disease | −0.006 | 0.016 | 0.712 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flinspach, A.N.; Booke, H.; Zacharowski, K.; Balaban, Ü.; Herrmann, E.; Adam, E.H. Associated Factors of High Sedative Requirements within Patients with Moderate to Severe COVID-19 ARDS. J. Clin. Med. 2022, 11, 588. https://doi.org/10.3390/jcm11030588
Flinspach AN, Booke H, Zacharowski K, Balaban Ü, Herrmann E, Adam EH. Associated Factors of High Sedative Requirements within Patients with Moderate to Severe COVID-19 ARDS. Journal of Clinical Medicine. 2022; 11(3):588. https://doi.org/10.3390/jcm11030588
Chicago/Turabian StyleFlinspach, Armin N., Hendrik Booke, Kai Zacharowski, Ümniye Balaban, Eva Herrmann, and Elisabeth H. Adam. 2022. "Associated Factors of High Sedative Requirements within Patients with Moderate to Severe COVID-19 ARDS" Journal of Clinical Medicine 11, no. 3: 588. https://doi.org/10.3390/jcm11030588