
Abstract
The current pandemic caused by the COVID-19 virus requires more effort, experience, and science-sharing to overcome the damage caused by the pathogen. The fast and wide human-to-human transmission of the COVID-19 virus demands a significant role of the newest technologies in the form of local and global computing and information sharing, data privacy, and accurate tests. The advancements of deep neural networks, cloud computing solutions, blockchain technology, and beyond 5G (B5G) communication have contributed to the better management of the COVID-19 impacts on society. This paper reviews recent attempts to tackle the COVID-19 situation using these technological advancements.
Similar content being viewed by others
Chapter 1: Introduction
The year 2020 will be remembered in history as the year of the spread of the Corona virus-based disease, COVID-19. Although there were several viral diseases reported in the past, technologies available today were not available then. To date (July 31, 2021), the number of confirmed cases has crossed 198 million, and more than four million people have already died in more than 188 countries and regions of the world because of this disease. Unfortunately, there is a clear gap between the rapidly increasing number of confirmed cases of COVID-19 infection and the capacity of manual pathological tests needed to mitigate and handle the pandemic [1,2,3]. This gap was developed by the human immune system being attacked by the COVID-19 viruses. As a result, the only way to halt the spread of the pathogen is to perform mass testing in the shortest possible time and isolate those who are infected with the virus and treat them with existing treatment knowledge acquired from COVID-19’s family chain (i.e., SARS-COV-2 or MERS-CoV). One of the gold standards of the current treatment process is to identify the RNA genome of COVID-19 via Reverse Transcription Polymerase Chain Reaction laboratory test (RT-PCR), which requires a minimum of 12 h to generate a report and hence hinders diagnosis on a mass scale.
Since this new virus began to spread, healthcare providers have resorted to several methods of diagnosing suspected cases on wide ranges. This has allowed timely care and isolation of confirmed COVID-19 cases. One of the testing methodologies for suspected COVID-19 cases is viral RNA sequencing by polymerase chain reaction (PCR) [4]. Another method is to conduct serological screening for antibodies, which the patients’ immune system usually starts to develop approximately 2 weeks from becoming symptomatic and lasts for several weeks at a detectable level. It is worth mentioning that these antibodies’ structure is the target for vaccinologists to mimic while developing vaccines.
Nevertheless, both testing methods suffer long-term operations that require prospecting longitudinal interventional clinical trials, as the exact nature of SARS-CoV-2, while still its cDNA/RNA sequences have not yet been completely decoded. Therefore, a third approach is to share information of viral RNA sequences isolated from confirmed cases and the antibodies developed or to experience existing drugs that have shown efficacy on a global level, all of which can accelerate the development of innovative testing techniques and cures.
This apparent failure to respond to the pandemic requires urgent technological intervention to substantially eradicate the effects of the virus and protect people at risk without further delay. Today, therefore, there is an urgent need to invest in the best technologies to mitigate the painful effects of this virus and protect the inhabitants of our planet in this race against time [5]. As we enter the third decade of the new millennium, we find the technological environment abuzz with terminologies such as 5G, the Internet of Things (IoT), blockchain, and machine learning. Like all extant technologies, these serve as tools to improve human life on planet earth. Medical science, of all sciences, is the most concerned with the physical well-being of humans. Scientists are trying to find ways to use these technologies to improve disease and health management in different ways.
The technologies mentioned above are currently being used in different areas of health science, epidemiology, and virology. The ubiquity of interconnected and Internet-connected medical devices based on IoT technology allows medical personnel to record and store large amounts of patient data in real-time. Before the invention of these devices, it was not possible to physically collect large amounts of data. However, the 5G telecommunication networks allow these IoT devices to transport data to large repositories on the Internet within milliseconds. Blockchain guarantees the secure and traceable propagation of data among these repositories using high-speed 5G networks. Data scientists then use machine-learning algorithms to analyze this data and come up with conclusions that are difficult to reach with limited human resources. The same high-speed networks also make it easy to provide medical advice to patients using telemedicine technologies in distant areas. Fortunately, since the first reported outbreak of COVID-19 in Wuhan, China, researchers around the globe have been using machine-learning algorithms to detect and diagnose COVID-19 and predict and flatten the casualty curve [6, 7]. The current efforts and solutions to fight the development of this pandemic using state-of-the-art technological advancements are summarized as follows:
-
The ability to quickly detect positive cases, which are large in number and increase daily,
-
The ability to maintain safe social distancing and dynamic immunization certificates for each person,
-
Isolation of healthy people from infected ones in a short time, and
-
Development of a vaccine by studying the behavior of viruses in their fight against the human immune system.
With the advent of the COVID-19, these technologies have become the new soldiers in humanity’s fight against the pandemic. This paper summarizes recent research on applying various computing techniques to mitigate the spread of COVID-19 viruses. To the best of our knowledge, this is the first work to summarize and review stand-alone or cross technologies used to fight against COVID-19. The rest of the paper is organized as follows: chapter two focuses on neural network technology, chapter three highlights the emergence of 5G technology, and chapter four demonstrates how blockchain can be utilized for securing transactions related to the COVID-19 process. Chapter five points out some recommendations for future researchers, and finally, we conclude our work.
Chapter 2: COVID-19 Diagnosis Through AI and Medical IoT
Preliminaries
Coronavirus is a respiratory illness and, therefore, affects breathing patterns and other vital parameters. Extant research shows that deep-learning algorithms, for example, trained to recognize cough and human respiratory sound recognition systems, can analyze a person’s voice and provide a score regarding the likelihood that an individual has coronavirus [44]. According to lung and COVID-19 specialists, one of the most distinguishing characteristics of COVID-19–positive patients is the sound of the patients’ breathing when they speak, the sound of dry cough, and their breathing patterns [45, 46]. However, there are very few large datasets of respiratory sounds available for research. Thus, to make better algorithms that can be used for early detection, researchers need as many samples from as many participants as possible. AI algorithms must be trained using many voices to understand the subtle variations in sounds that suggest someone is infected with COVID-19 [47]. The author in [48] investigated machine-learning algorithms that can recognize coughs in real-time using low-cost mobile devices. In the time of this pandemic, we can leverage the advancements in machine learning’s human voice and cough recognition algorithms to reduce the time required for the diagnosis of COVID-19 at point-of-care locations [49]. For example, AI-based automated cough sound analysis methods can be exploited to detect COVID-19 cough patterns early. This technique can be applied by processing the collected raw data observed by subjects in hospitals or subjects self-isolating worldwide.
Recently, health professionals have discovered possible associations between COVID-19 and pink eye symptoms. Researchers have used deep learning to recognize these phenomena from retinal images [50]. For example, the authors in [51] used a deep-learning algorithm to detect pink eye or conjunctivitis symptoms from optical coherence tomography (OCT) images. However, the researchers in [52] identified COVID-19 RNA from the ocular discharges of a COVID-19–positive patient. In summary, pathological tests conducted early in the diagnostic timeline, such as RT-PCR, might not show the intended results [53].
Similarly, finding an effective drug or vaccine that prevents COVID-19 requires a long time and many clinical trials. In addition, the use of pathological COVID-19 is hindered by shortages in the supply chain of chemical reagents needed for testing on a large scale. This impairs quick diagnosis and makes it challenging to filter out COVID-19–positive patients from uninfected patients. Deep neural network (DNN)-based quick diagnosis methods, such as computed tomography (CT), magnetic resonance imaging (MRI), and Positron Emission Tomography (PET), have attracted many researchers, as COVID-19 exhibits patterns different from those of other viral pneumonia conditions [54]. Therefore, clinical doctors have recently called for the development of image recognition-based early diagnostic criteria for COVID-19 as soon as possible.
Since COVID-19 attacks the epithelial cells that line our respiratory tract, doctors have resorted to the use of CT-scans to analyze the health of a patient’s lungs [55,56,57,58,59,60]. Given that nearly all hospitals have CT-scans or X-ray imaging machines, it may be possible to use CT-scans or X-ray images to test for COVID-19. However, one of the bottlenecks of CT-scan and X-ray image analysis is that they require a radiology expert [61] and take a significant amount of time, which is precious when patients need to be tested for COVID-19. Therefore, developing an automated analysis system is necessary to save valuable time and serve more patients. This study outlines point-of-care screening models to diagnose COVID-19 using DNN techniques. Moreover, these non-invasive point-of-care tests may help prioritize the limited COVID-19 resources that a country, city, or medical facility has.
The COVID-19 standard diagnosis currently relies on nasopharyngeal RT-PCR swab, although several other potential diagnosis methods exist. Several researchers suggest that a multi-modal diagnosis allows lowering the risk of false negatives [62, 63]. Deep-learning theories are imperative in recognizing health samples of various types (images, sounds, etc.) and classifying each sample according to its distinctive characteristics. Since COVID-19 results in respiratory disorders, different testing modalities can reveal the diagnosis, detection, and recognition of the viral infection. Figure 1a [42] shows different types of tests that researchers have suggested: for example, the use of DNN algorithms to determine whether CT images feature characteristics of COVID-19 infection.

Use of AI for COVID-19 diagnosis: a respiratory disorders caused by COVID-19 infections, b sample deep neural network modules that can be trained using available off-the-shelf consumer tools to recognize COVID-19 rapidly, and c DNN modules that can be trained using point-of-care on-premises tools to diagnose COVID-19 rapidly
Similarly, researchers have used DNN algorithms to recognize COVID-19 symptoms from other testing modalities. For example, authors in [64] have shown how COVID-19 symptoms such as nausea, fatigue, coughing sounds, and body temperature can be captured using modern smartphones. Then, deep-learning algorithms can be used to determine whether patients are positive or negative for COVID-19. We have studied the efforts of existing researchers and open-source initiatives and evaluated the feasibility of various potential applications for COVID-19 support at point-of-care facilities. We have also categorized our evaluated applications into two broad areas: DNN modules that can be trained, tested, and deployed via off-the-shelf consumer hardware and those that require a subject to visit a point-of-care COVID-19 test facility. Figure 1b shows the applications to which the former case applies, while Fig. 1c shows the applications that fall into the latter category. Please note that the DNN applications shown in Fig. 1b are also applicable to point-of-care facilities. The modules shown in Fig. 1c use computer vision-based DNN algorithms that utilize live camera feeds in spaces of self-isolation, public places, or point-of-care facilities. For example, modern smartphones that come with fingerprint sensors have been used by researchers to capture body temperatures [64].
In [8], the authors presented a DNN model that can be leveraged by three stakeholders (patients, doctors, and decision-maker authority). The model connects patients or suspects with various biometric sensors that help to quickly collect relevant samples and then process them locally. This process employs deep-learning algorithms to analyze observed measurements emitted from the human body and then make the appropriate decision and send it to the doctors without the need for direct contact. Figure 1 demonstrates the DNN modules for analyzing COVID-19 data. In their research, the authors validate their proposed DNN modules by developing an application that uses lung sound. The captured sounds will be evaluated using the DNN model through a mobile application. Thanks to this idea, patients can now provide valuable information and important samples from home or during isolation. In general, Table 1 shows DNN modules that can be used to deal with the COVID-19 pandemic management domains.
Diagnosis of COVID-19 Using AI
Computer science has many branches; one of them is artificial intelligence (AI), which can analyze complicated health data. The ability to fully use significant connections within a dataset, which is a feature of AI systems, can be used in the identification of a disease, treatment, and description of a possible future event [65]. Therefore, AI systems are viewed as intelligent agents that can decide what actions to take and when to take them. To quickly stop COVID-19’s real outbreaks, there is an essential need to initiate a clinical system using AI [66]. DNN is among the key components of AI that involves offering automated systems the ability to “learn” data rather than being explicitly coded.
As data is propagated through the DNN, weights and biases are updated, allowing the DNN to learn features from the provided data. However, merging deep-learning-based models [such as convolutional neural network (CNN), recurrent neural network (RNN), and Support Vector Machine (SVM)] with powerful computer vision (CV) algorithms, such as the Active Appearance Model (AAM), generates excellent precisions [67]. Many variations of DNN, such as CNN and RNN, could be utilized to classify and recognize COVID-19 cases [68].
AI has been surveyed for COVID-19 in both diagnosis and digital contact tracing [62]. The study in [69] found that Nathalie’s patients were diagnosed with the help of multi-modal AI-based clinical characteristics. As a result, chest CTs and lab test prediction of COVID-19 outcome were improved by 15% of total cases. One of the COVID-19 challenges at the Intensive Care Unit (ICU) reported by hospital authorities was the prediction of prioritizing the patients’ care as per the severity level. From two French hospitals, they collected 1003 patients’ medical information, comprising biological and clinical data where 11 clinical variables were identified in addition to three radiological reports. Deep learning (DL) models focusing on CT images were used to predict future severity, resulting in better results than radiologists’ scan reports. Finally, combining CT-scan images with the biological and clinical data results gives more accurate predictions than using only clinical and biological reports; thus, the research’s finding proves that CT-scan provides good predictions of future severity.
Scientists employed image processing methods, such as artifact removal, Firefly Algorithm (FA), and Shannon Entropy (SE), based on three-level thresholding to enhance the image. Markov-Random-Field (MRF) segmentation was used to extract the COVID-19 lesion, and a relative assessment of the extracted binary image with the Ground-Truth-Image (GTI) was also used to compute the performance measures. They initially considered the 2D CTI of the benchmark COVID-19 dataset and the clinical-grade 2D slices for the experimental investigation. The initial result attained with the benchmark dataset offered a mean segmentation accuracy of > 92% on 50 images of dimension 512 × 512 × 1 pixels. Moreover, the results achieved with the clinical grade CTI also offered better segmentation of the COVID-19 lesion, and the experimental results attained from this study confirmed the superiority of the proposed scheme. In the future, this scheme can be used to examine the clinically obtained lung CTI of COVID-19 patients. Coronavirus persists for up to nine days depending on the type of surface (Metal, Glass, Plastic, etc.) [70]. AI and CV can be used for tactile recognition [71] to resist the transmission of the SARS-COV-2 virus from various surfaces to the human body by recognizing objects already touched and objects not touched before [72].
With the help of an innovative multi-task sequential shift convolutional attention network, a researcher deployed an optical cardiopulmonary vial sign on-device video-based measurement method [73]. Furthermore, machine-learning techniques have helped in distinguishing critically ill patients suffering from pneumonia, the subgroup eligible for extracorporeal membranous oxygenation (ECMO) therapy [74]. The authors of [75] implemented machine-learning techniques for various classification tasks, such as identifying COVID-19 patients, hospitalization criteria, and critical care requirements. Visualizations of the importance of wearing masks can be a great tool to inform the public how they can do their part to flatten the curve [76].
Researchers have also worked on detecting different security issues related to finding faults within DL networks. Engagement of Universal Adversarial Perturbation (UAP) was able to produce DNN error in most categorization cases, achieving > 85% and 90% success rates [77]. Researchers have shown that DNN could also enhance the dataset by performing lung segmentation and data imputation in high opacity regions. These DL models can be used as a pipeline for automatic risk calculation [78].
Authors have used explainable AI in [79] to combat pandemics such as COVID-19. Machine learning has been used in [80] to track physical wounds. DL has also been used to diagnose COVID-19 from X-rays [21, 81], CT-scan [82, 83], and gait pattern [84]. A detailed survey on DL in the context of internet of medical things (IoMT) can be reached at [85]. Researchers have added explainability on top of the DL layers [86] to add semantic explanation and evidence. DL has been studied to detect multiple objects by a single camera feed [87, 88]. It has also been used to diagnose diabetic retinopathy in COVID-19 patients [89]. Moreover, a survey on DL algorithms that can track human daily life activities is presented in [90].
One of the most important challenges that researchers face in their fight against this pandemic is the accuracy of the examination and the speed of identification of the infected subjects. One of the most important features of the examination is distinguishing coughing for people with respiratory diseases [9]. By recognizing the coughing sound of non-COVID-19 patients and distinguishing this sound from the coughing caused by COVID-19 patients, artificial intelligence algorithms based on DL theories can produce impressive results and significantly help increase the capacity of the COVID-19 virus screening tests.
The characteristics of cough sound waves have been found unique in terms of speed, strength, and whether it is wet or dry [9, 10]. The authors in [11] developed the A14COVID-19 app, which records patients’ cough and sends it to an AI model, which detects the unique features of the repository system of COVID-19 confirmed cases, including cough sound. Because of the lack of a large dataset, they have exploited knowledge-based methods, which mitigates the need for massive samples to prove the concept of their proposed hypothesis. As a result, they succeeded in achieving 90% accuracy when recognizing COVID-19 cases from cough sounds. As of today, researchers are calling for volunteers to record their cough sounds to help them develop more tools that can help in fighting against the rapid spread of COVID-19 [12, 13]. We believe that this issue is one of the main open challenges that need to be addressed by researchers. Closely monitoring the image of the lung before and after infection with the COVID-19 virus has also become a promising method for shortening much time during screening operations [14,15,16,17]. It has been observed that radiological images related to COVID-19 confirmed cases developed unique physiological footprints over time [18]. Figure 2 shows the first COVID-19 X-ray images of a female patient observed over a 15 days’ span of infection. Researchers from China and other parts of the world have discovered the effects and symptoms of the virus, which change over the first 15 days. Hence, just testing any random RT-PCR might show false negatives, as the virus exhibits diversified types of symptoms for the first 15 days. Consequently, researchers have proposed a multi-dimensional testing mechanism that will allow multiple modalities of symptom checking, such as via cough sounds, eye color, stool, smell, lung images, and other types, in addition to PCR tests [40]. For example, researchers have observed significant developments and changes in the radiological images of the lung and found different spreading patterns of the infections.

Sample of CT images for first COVID-19 confirmed case [18]. Images a–d for day for day 10, day 13, day 17 and day 25 respectively
The authors in [14] used a database of 1065 images comprising images of positive samples for those infected with COVID-19 in addition to those with pneumonia. Using this data, they developed a machine-learning algorithm to train inputs to distinguish the distinctive properties of the lung of a COVID-19 infected person from different symptoms. They had a total accuracy of 89.5%, with a specificity of 88% and a sensitivity of 87%. As for the external data, the total accuracy reached was 79.3%, with a specificity of 83% and sensitivity of 67%. On the same approach, the authors in [15] were able to combine pneumonia and COVID-19 databases of CT-scans. They developed a method that enables them to distinguish the characteristics and features of images produced by COVID-19 patients. They succeeded in hitting 94.92% of sensibility, while the percentage for COVID-19 detection was 92.00%. In [19], a 3D model COVNET based on DNN was developed to distinguish COVID-19 cases from other possible infections, such as community-acquired pneumonia and non-pneumonia. The work presented in [20] used 4356 samples of CT images to evaluate five proposed CNN-based models (ResNet50, ResNet101, ResNet152, InceptionV3, and Inception-ResNetV2) for the detection of COVID-19 potential infection. The authors in [21] developed an automated model based on DarkNet open-source framework for COVID-19 radiological image recognition. They tested their model against a dataset comprising COVID-19 and pneumonia images and achieved 87% accuracy. Due to the lack of a large dataset related to COVID-19, the authors in [22] suggested a new model based on the Capsule Network algorithm for classifying COVID-19 X-ray images. The obtained accuracy was around 97%, while the specificity was close to 96% [23]. CoroNet is a COVID-19 diagnosis framework that has been examined using a public dataset [16, 24] and achieved 89% overall accuracy. Researchers have proposed different AI models such as transfer learning, federated learning (FL), and explainable AI for COVID-19 diagnosis and treatment [39,40,41,42,43]. Figure 3 summarizes the different AI models that can be fused to support diversified types of diagnosis. As shown in Fig. 3, different diagnosis types require different input datasets, different underlying DL algorithms, and different explainability.

AI model for COVID-19 diagnosis
Figure 4 shows details about the decentralized way of training a COVID-19 diagnosis model, called federated learning (FL), while keeping the privacy of the training dataset. In FL, the training process is distributed among several federated clients. A central trusted entity first generates a base central model based on an initial dataset available to the central entity. Then, the central entity invites several private federated entities that own their private COVID-19 dataset. Next, the central entity shares the initial DL model with the FL clients. The FL clients then train the model at their own private edge nodes without sharing the privately owned COVID-19 patients’ treatment dataset. Once all the FL clients finish training the local models, they share the local models with the central trusted authority to generate a higher accuracy global diagnosis model. This process continues until an acceptable level of accuracy is achieved, ensuring that the private COVID-19 related data is never shared with outsiders, but only the model is being shared.

Use of decentralized AI to provide privacy of the COVID-19 patient’s data
Medical IoT for the Diagnosis of COVID-19
The biomedical and health data analysis shows a vital role in self-knowledge, disease prevention, disease identification, infection, and other issues, or its root cause. With the future of data-driven applications and with other execution and apps, IoT tools such as home medical sensors, wearables, etc., enable data gathering and offer cloud storage, including centralized management. Moreover, blockchain became available with flexible storage options created on decentralized organization structures [91]. The study in [91] introduced TechO + , which allows recognition and consideration of sensors’ available data, trackers, and other IoT devices either supported by the end-user or accessible within the user’s environment (e.g., smart devices, smart home, or a smart car). Many IoT devices, like ThingSpeak, enable transferring data to the cloud [92]. Accordingly, the researcher analyzed IoT data using DL for gait analysis [93].
Researchers use blockchain to boost mHealth through storing and sharing IoT data securely and transparently. It can enhance the accessibility of a patient’s information in real-time. The IoT provides a unique identification number to every connected device, such as mobile, medical, and wearable devices. The result of using the mHealth framework with the blockchain and IoT technologies together provides quick help to the patients, allows monitoring remotely, and reduces cost and unnecessary hospitalization. The mHealth framework with blockchain and IoT technologies has been merged to increase patient involvement with the key objective of providing patients with complete information on their treatment and diagnosis [94].
The use of IoMT has been proposed for COVID-19 patient monitoring in the areas of IoT data sharing, report monitoring, patient tracking, and remote healthcare [95]. The use of IoT, drones, and robotic technologies to support a non-invasive way of caring for COVID-19 patients in hospitals has been shown in [96]. One of the IoT applications used for fighting against the COVID-19 is the use of drones for surveillance to ensure quarantine and mask-wearing. IoT can be used to trace the outbreak origin, identify patients with all contacted persons, and track the quarantine breach. IoT can also be beneficial in the remote monitoring of in-home patients [97].
Due to the long incubation period of COVID-19 and the limitation of testing capabilities, contact tracing solution comes to light, and an enormous contribution has been made to support this solution. Apple and Google collaboration comes into the picture to break the circle of the transmission of COVID-19 using Bluetooth RSSI-capture and provide COVID-19 exposure notification/logging [98]. In addition, a company called “Life Signals” has developed an IoT-enabled device [99] for remote health monitoring of COVID-19 patients staying at home due to the shortage of ICU in hospitals and who still need to be monitored remotely to reduce the risk of complications. This device can monitor patients’ vital signs, such as heart rate, electrocardiogram (ECG), blood oxygen level (SpO2), respiration rate, and skin temperature.
The authors in [28] used IoMT in physical therapy at home. IoMT has been surveyed in the context of mobile edge computing in [100]. Similarly, an overview of IoMT sensors has been studied regarding patient monitoring in [101]. A comprehensive survey of health IoT based on the Internet of Nano Things and 5G tactile Internet’s effect on healthcare quality of service have been portrayed in [102]. IoMT has been used by authors in [103] to develop an in-home diabetic management system. A review of IoMT to handle pandemics such as COVID-19 has been presented in [104]. Authors in [105] designed a wearable IoMT device that can track social distancing and generate an alert when social distancing is violated.
Researchers have proposed diversified types of medical IoT devices conducive for COVID-19 diagnosis and treatment. Figure 5 shows a summary of medical IoT devices that different researchers have proposed. Since IoT devices are generally resource-constrained to run DL applications, edge nodes with more computing and GPU processing capabilities are generally employed. Figure 5 shows several such edge nodes (e.g., PC, raspberry PI, NVIDIA Jetson Nano, smartphones, or even custom-made edge nodes). In each edge node column, a survey has been done that shows the IoT devices supported by these edge nodes. Please note that this is not an exhaustive list. These medical IoT devices can be integrated with existing treatment processes for collecting data from patients or caregiver institutions. Different AI and DL algorithms have been developed to collect symptoms from these IoT devices. A detailed list of algorithms can be found in [39,40,41,42,43].

Medical IoT devices to treat different types of COVID-19 symptoms [39]
The authors in [95] have proposed an IoMT-based framework for the proactive orthopedic treatment of COVID-19 patients for different types of diagnosis scenarios, such as in-body, in-home, in-clinic, and in-hospital. This research has considered diverse types of IoT devices, such as user health wearable devices, clinical wearable devices, mobility-related sensors, point-of-care sensors, and other types of innovative IoT devices. The work presented in [106] uses drones to collect health data non-invasively from the IoT sensors available within the COVID-19 patients’ body area network. The authors claim that this method of collecting COVID-19 patients’ health data from IoT devices is useful for those areas tagged as a high-risk zone. The authors in [28] have used Internet-connected X-ray and CT-scan machines with a COVID-19 AI diagnosis model that can diagnose the symptoms in real-time as soon as new radiometric data is fed to the machines. A detailed survey of IoT technologies, especially those developed and used for COVID-19 pandemic handling, can be found at [104]. Authors in [102] have done an extensive review of IoT devices that can support COVID-19 diagnosis and handling. Examples of IoT devices that have been reported are Arduino microcontroller with specialized onboard medical sensors, heart rate sensor and triple axis accelerometer, electrocardiogram sensor, temperature sensors, movement sensors, two thermistors, microphone, ambient humidity, smartwatch microphone, environmental sensors (passive infrared, grid-eye thermopile array), optitrack camera, wearable (ECG and breath-smart shirt), smartwatch sensors, environmental sensors, FLIR Lepton 3.5 Radiometry Long-Wave Infrared Camera, accelerometers, gyroscopes and magnetometers, EEG sensor, EMG sensor, blood pressure, respiratory rate, motion activity, glucose recognition, movement tracking sensors such as ECG sensors, accelerometers, gyroscopes magnetometers on chest, ankles and arms, and glucose level monitoring sensors. Researchers have also developed many custom COVID-19 diagnosis IoT kits. For example, an IoT kit suitable for reporting symptoms with medical authorities during one’s quarantine time has been illustrated in [107]. IoT has been used for contact tracing as well [108]. To help in social sensing, the work presented in [109] has used smart heart-rate monitors, activity trackers, and thermal scanners that are connected with a smartphone. The authors in [105] have designed a wearable IoT band to help in social distance maintenance and contact tracing.
A Sample Case Study—How AI is Used for COVID-19 Diagnosis
X-Ray Classification for COVID-19
In this section, we present a sample COVID-19 diagnosis from X-ray radiometric images. The DNN model has been trained to classify X-ray images into three classes: normal, Pneumonia, and COVID-19. The motivation for this was that COVID-19 patients usually present distinctive markings in their X-ray images. Hence, a predictive tool based on X-ray image analysis proves to be very useful. The presented X-ray classification for the COVID-19 system is a web tool that takes an X-ray image file as input and outputs the percentage score in any of the three classes: normal, pneumonia, and COVID-19. Based on the prior knowledge of the input X-ray image file, an expert medical doctor treating a patient can approve or moderate the result of the prediction.
Description of the system:
-
The homepage is shown in Fig. 6. Upon entering the website, the user sees the vast array of options available for exploring.
-
Upon selecting the X-ray Classification—Covid-19 option, the user is prompted with two-factor authentication (2FA).
-
On the X-ray classification page, the medical doctor can see the proper instructions to use the application.
-
After selecting the choose file button, the user will be prompted to a file browser, from where the user can input an X-ray image file.
-
After pressing the predict button, the doctor will be routed to the result page. On this page, the doctor can see the model’s prediction (Normal/Pneumonia/COVID-19) along with the confidence score. The higher the confidence score and closer to 100, the more the model is sure about its prediction. After seeing the results, the doctor can fill out the survey to provide feedback upon using the classification system and press the submit button to submit the survey. After pressing the submit button, the doctor is shown a pop-up to confirm the submission of the feedback (Figs. 7, 8 and 9).

X-ray classification app button

X-ray classification—input upload page

X-ray classification—image file browser

X-ray classification—inference and feedback pages
The system has been trained with the neural network in a machine equipped with a Core i7 9900 k and an Nvidia RTX 2080 TI GPU. In addition, the performance of the best trained model has been tested on an entirely new test set comprising 500 normal, 500 pneumonia, and 500 COVID-19 positive X-ray images. The training history and the test results are given in Fig. 10. The process of improving the accuracy, sensitivity, F1-Score, and recall values is continued with enough training, test, and validation datasets until medically acceptable threshold values are attained.

Sensitivity and positive predictive value: X-ray classification
Chapter 3: 5G, B5G, and 6G Technology
A 5G network has been rolled out throughout the world, which allows ultra-low latency, extreme bandwidth, and an extremely large number of medical IoT devices. These features would be convenient for the COVID-19 diagnosis ecosystem to offer applications needing end-to-end delay of less than one millisecond. As shown in Fig. 11, the round-trip time to send the COVID-19 related data originated at one location can travel to a medical caregiver at a remote location, obtain feedback from medical professionals, and get a telemetry signal back to the source within milliseconds.

Ultra-low latency in 5G to support COVID-19 treatment
Unquestionably, the faster the exchange of data between healthcare centers and patients, the more this will affect the speed of decision-making and the protection of many who are at risk. Mitigating the effect of COVID-19 requires the exchange of massive data between cities and countries around the world. Therefore, utilizing a high-speed, low-latency network is needed. 5G allows configuring the network and bandwidth that is needed to support the quality of experience of COVID-19 applications. This is done through the virtualized network functions (VNF) that leverage the “softwarized” network slices. Figure 12 shows network slices that can be initialized for different types of medical applications’ needs. The unique features of the 5G network make it possible to examine patients and give them advice without the need for direct contact resulting from their visit to the clinic. Furthermore, the high bandwidth of this network provides the ability to share information at a tremendous speed, which leads to researchers reaching more data that helps raise the accuracy of results related to algorithms used to reduce the COVID-19 pandemic [25,26,27].

5G custom network slicing to support COVID-19 treatment
What distinguishes their model is the replacement of a central processing unit with peripherals represented by patients’ devices in their homes. The researchers in [29] emphasized that China invested the 5G technology in reducing the impact of the COVID-19 virus by employing it in the transport system. The immense speed, high capacity, and low-latency features of 5G contribute to vehicle tracking and integration of several techniques in crowd monitoring. In [30], patients were able to respond to questionnaires and communicate with doctors without the need to visit the hospital by exchanging data via 5G technology. In [30], during the peak of the spread of the virus, the Chinese health system used 5G technology to develop a rapid response system referred to as the Emergency Telemedicine Consultation System (ETCS) to provide distance medical consultations to patients and establish live communication with more than 100 cities to track and isolate patients. Moreover, the authors in [31] highlighted the opportunity of emerging 5G technology with the IoMT and how it benefits the health system to assist patients remotely. The author in [32] explained potential features of incorporating 5G technology to combat COVID-19:
-
Patients with mild to no symptoms, undiagnosed cases, and health workers with direct exposure to the virus have a high risk of transmitting it to their families, friends, and communities. This could be monitored in real- time with the assistance of 5G technology.
-
5G technology helps to provide the required technical infrastructure to exchange information quickly about infected patients, locate their transfers, and track the people who contacted them to stop the spread of infection.
-
Exchanging high-quality images and long and short videos for COVID-19 diagnosis is vital. That can be achieved by enhancing and upgrading local, metropolitan, and wide networks to match the new requirements due to the COVID-19 pandemic.
While 5G is rolled out, researchers have started developing extensions of what is called beyond 5G (B5G), which looks at the shortcoming of 5G and tries to propose solutions to that [43]. For example, B5G network slices suitable for COVID-19 treatment can be automatically configured through AI-based system. Similarly, end-to-end delay, jitter, security of the patient data, privacy requirements, and so on can be programed through AI using B5G. However, the B5G network is not designed by AI-driven technologies from end-to-end. Hence, the 6G network is being proposed. In 6G, the industrial internet of things (IIoT) devices will have AI-enabled wireless interfaces through heterogenous frequency bands, including terahertz (THz) and millimeter wave (mmWave) and base stations such as small and tiny cells. 6G will offer high-performance networking, hyper-flexible architecture, AI-enabled intelligent architecture, and AI-enhanced security. 6G network will be able to exchange massive amounts of diversified information between the COVID-19-related distributed entities at a peak data rate of up to 1 Tbps, undetectable latency of approximately 0.1 ms, reliability on the order of nine-nines uptime, and ultra-dense IIoT networks. State-of-the-art 5G or beyond 5G deployments use DL partially (i.e., at the application layer or some parts of the network). In 6G, AI will be taking charge of the overall optimization of the complete network. For example, FL with blockchain-based provenance can be used for secure spectrum sharing within competing peers. The authors in [28] demonstrated a B5G network applicable for COVID-19, which can be deployed with various models. In their proposed work, B5G was utilized to improve data processing accuracy and throughput using DL theories.
Chapter 4: Security of COVID-19 Treatment Process
Blockchain
Blockchain is essentially a computer program that uses computational laws and cryptography to make a digitally secure record. It is usually referred to as being “immutable” because it cannot be subsequently changed [7]. Blockchain is closely related to a cryptographic process and is included in the category of a decentralized digital transaction ledger without any control from individuals, groups, or companies, where things recorded in the ledger are information whose level of accuracy and validity must be ascertained [110]. Copies of the program and the records it stores are typically distributed across several computer servers, thus creating a distributed ledger [35]. This novel technology acts as a shared repository or database, which can keep all its data copies synced and verified [38]. Recently, the healthcare and biomedical systems with other wide range of applications have shown blockchain technology’s adoptability [111]. Various industries, businesses, and even governments have been attracted by the potential and sophistication of blockchain technology, especially the healthcare industry [110].
Given the scale of the pandemic and financial impact, it makes sense that the certification of COVID-19 patients using blockchain technology would be in high demand in different areas, including the financial industry, food industry, oil & gas industry, healthcare, and IOT [37]. Many other domains include remote patient monitoring, health data analytics, drugs and pharmaceutical, and supply chain management, where the blockchain and AI are playing an excellent role [112]. Blockchain introduces different applications to the available patients’ health information management and sharing [113]. Many digital health applications, such as Health Bank, bring fundamentally new methods related to data sharing and transactions of personal health data, where users can store and manage health information in a secure manner [114]. Another example where the blockchain was used in the US is the Gem Health Network [115]. Within this framework, various healthcare clients, including specialists, are permitted to access unlocked resources that solve many operational issues using a new class of applications based on blockchain [115]. In addition, many blockchain and AI systems have been introduced to handle emerging infectious diseases [116].
A scientific research group in Egypt has set up an innovative COVID-19 blockchain framework, which has four subsystems: (1) infection verification, (2) blockchain, (3) P2P mobile application, and (4) mass surveillance. All components synergize to identify unknown infected cases and predict and give an estimation of the infection risk of COVID-19 subjects [117]. An excellent work using blockchain with a contact tracing scheme named “Beep trace” has been shown in [118].
The increasing number of people infected with the COVID-19 virus generates vast amounts of medical records that require sharing with several parties, including “other healthcare centers, decision-makers, and the World Health Organization.” This fact represents a major challenge for health communities; therefore, applying blockchain technology contributes greatly to automating health data sharing processes while maintaining the required level of data privacy [42]. In [33], the authors highlighted the possible advantages of emerging blockchain technology for the COVID-19 pandemic. The authors in [110] have used blockchain to store the COVID-19 test results and to share them with communities of interest. Moreover, blockchain has been used to store the health certificates of COVID-19 patients, which can be shared with stakeholders upon the owner’s request. Researchers have also used blockchain as a secure and trustworthy COVID-19-treatment-related data sharing platform among multiple medical institutions [37]. They specified four benefits:
-
First, blockchain will benefit the process of case reporting to make it automatically generated and transferred without the need for an intermediate party. That will make the final authority in front of the decision with more efficiency, transparency, and speed.
-
Second, with the outbreak of this pandemic, many business owners were affected, treatment cost bills increased for many patients, and the demand for isolation centers for suspected cases also increased. For these reasons, many donors have increased the desire to donate their money or items, but in a confidant method. Blockchain technology provides the confidentiality, transparency, and automation required of donors due to the privacy and speed with which they deliver the funds.
-
Third, as can be observed, many false claims and misleading figures hindered the efforts to combat the pandemic and caused considerable losses for health authorities. Exchanging records related to COVID-19 cases through blockchain will certainly provide integrity of the treatment data and the specimens used.
-
Fourth, the digitization of transactions’ papers and documents between patients, clinics, and insurance companies prevents the potential infection caused by touching. Nevertheless, direct contact can also increase the percentage of infectious diseases. Blockchain is an excellent alternative to non-invasive and paperless processes, and it enhances security significantly.
-
Fifth, researchers have shown that DL algorithms can be attacked using adversarial examples [41]. Hence, the DL models need to be secured from such attacks so that the COVID-19 data is trustworthy. Hence, a blockchain-based provenance system has been proposed.
The authors in [34] developed a model based on AI and blockchain. The model was built based on four elements: COVID-19 data sources, blockchain properties, AI properties, and stakeholders. In [35], the author highlighted the contribution of blockchain technology to secure donations of donors who want to contribute to minimizing the effects of the COVID-19 virus. In [36], the authors proposed a framework based on blockchain technology to mitigate the impact of COVID-19 and provide secure and private data in the healthcare sector. In their proposed model, the test procedure for COVID-19 has been demonstrated, which is named COVID Test Certification (CTC). The main objective is to provide infected people with the ability to share their history with other parties and related authorities in a private and secure manner. In [37], blockchain technology was utilized to propose a secure healthcare system and break down massive and complicated health processes. The authors in [38] elaborate on blockchain technology and how it leads to mitigating the virus by discussing several advantages. First, all medical records related to COVID-19 should be securely saved and processed through blockchain technology for performing medical studies. By using blockchain, researchers worldwide can exchange information, findings, and recommendations in a secure and decentralized process.
Blockchain has gained trust in providing provenance, data integrity, authentication, and immutability for the Internet of Health Things (IoHT) [119]. A detailed survey on IoT application security through blockchain can be found in [120]. The authors in [121] designed a multi-tenant blockchain application that guaranteed scalability, data integrity, and data privacy within a permissioned blockchain. BlockDeepNet is an architecture that allows secure sharing of private data among collaborative IoT nodes to make enough IoT data available as the training data required for the DL application. Blockchain was used to provide the collaborative IoT nodes’ confidentiality, authentication, and integrity [122]. Blockchain and an InterPlanetary File System (IPFS)-based off-chain solution was used in [123] to provide secure mobile cloud access and secure EHR data sharing between patients and medical service providers while keeping the personal data on the mobile device private. The probabilistic method has also been combined with blockchain to provide authentication and authorization for IoT data transactions [124]. Blockchain has been used to provide data assurance and resilience in an IoT network [125]. A high-throughput and scalable blockchain data structure based on DAG, designed for industrial IoT, was proposed in [126].
Blockchain and DL have been used for provenance [127]. The authors in [128] showed that the trust of IoHT data by different parties could be ensured through smart contracts containing trusted IoT zones. The work presented in [129] used blockchain smart contracts and physically unclonable functions (PUFs) to resist IoT data tampering and data provenance and impersonation attack. Blockchain-based data provenance and a lightweight hash-based security algorithm were proposed in [130] to detect data tampering. A software-defined network offering blockchain-as-a-service was presented in [131], where two different secure DL model training scenarios were presented. The blockchain-empowered training data are first uploaded to a decentralized IPFS file system for data provenance. Then, either a partially decentralized or a fully decentralized co-operative model training takes place. Researchers have proposed blockchain to thwart data poisoning and membership inferencing attacks by not allowing malicious or unreliable FL participants [132]. Blockchain has been used for failure detection in IoHT devices using FL [133]. Secure and privacy-maintained data and model sharing with the help of a permissioned blockchain was illustrated in [134].
Figure 13 shows a framework in which blockchain has been used in combination with medical IoT related to COVID-19 treatment. Different edge entities treating COVID-19 subjects can collaboratively train the DL algorithms using FL, as detailed in Fig. 4. Each edge node can retain its own private health data, while the global model is only shared among the clients. Blockchain is then used to provide provenance and trust among the collaborative clients. Figure 14 shows a detailed explanation of the system shown in Fig. 13 in a different dimension. Figure 14 shows how blockchain can support medical IoT devices within the COVID-19 treatment ecosystem to share data securely among multiple clients distributed around the globe. In Fig. 4, we explained the FL process in which the coordination of choosing FL clients, sharing the central model, and aggregating the FL client-provided models was assumed by a trusted central authority. However, this trusted central authority poses two challenges. First, the central authority might be compromised; hence, there should be a mechanism to trust each other. Second, the system must ensure that the FL clients are also trustworthy and that there is no malicious client. Hence, blockchain has been recommended to add provenance, trustworthiness, and decentralization to the process. Figure 14 shows the timeline of events that take place during the similar process discussed in Fig. 4 but in a decentralized way, handled by blockchain.

Blockchain, distributed DL, and medical IoT to support COVID-19 treatment

Distributed blockchain and off-chain for the provenance of COVID-19-related health data
Differential Privacy to Provide Privacy of COVID-19 Patients’ Data
Blockchain has been used in the context of differential privacy (DP). Because artificial noise is being added to prevent a privacy leak through a data query, the authors in [135] proposed a blockchain to track the total and individual privacy budgets, how much additional noise was added to unique queries, and how much more noise could be allowed before degrading the quality of the dataset and privacy cost. In another effort [136], researchers proposed collaborative game-based training data sharing and made the updated model available on the blockchain. An appropriate incentive for a genuine training data provider is embedded into the framework. To prevent a malicious attack and reduce the amount of consensus computing on the blockchain network, the authors in [137] designed a blockchain-based FL network to store the global model and the incremental updates. DP was combined with FL and the blockchain for IoT data used in smart home health monitoring [138].
Researchers have used FL to provide DP. Interesting work in [139] benchmarked the usage of FL in IoHT edge nodes. For example, the work presented in [140] uses a one-shot FL that tries to find a privacy balance between two extreme phenomena, in which fully private nodes suffer from a very low amount of data. Concurrently, the fully central aggregation of data models is done on a central node. The privacy of IoT data was studied in the context of FL in [141]. FL suitable for IoHT-based edge computing was illustrated in [142]. The security and privacy aspects of IoHT data through distributed FL in the context of a 6G network were studied in [143]. In a similar study, the security and privacy of AI training or inferencing data and models within 6G networks were surveyed in [144, 145]. The authors in [146] proposed a self-healing FL network, which could collaboratively train and detect anomalous nodes. To address privacy, poisoning attacks, and latency issues, the work presented in [147] used a blockchain where miners approved the uploaded models from federated edge nodes through a consensus mechanism. To avoid data privacy leaks within 5G ultra-dense mobile edge networks, the authors in [148] proposed FL administered by blockchain. To provide auditing and accountability in terms of the contribution of collaborative FL processes, the authors in [149] designed BlockFlow, which incentivizes genuine contributors while isolating malicious contributors. To ensure the anonymity and privacy of IoT data in edge devices, the authors of [150] proposed a blockchain based on a decentralized FL architecture. The security and privacy of IoHT data used within the data aggregation cycle of FL have been studied by the authors of [151] in a smart home context.
Security of the AI Model
The security and privacy of DL applications over 5G edge networks were surveyed in [152]. To protect the sensitive data available to network functions or network slices of a 5G network and protect the confidentiality of local DL model updates, the authors in [153] proposed a Multi-Party Computation (MPC) protocol on top of FL within 5G networks. IoT-based traffic data was subjected to FL by the authors in [154], where private data was trained using an SVM RBF kernel function, and the global training module was administered by a secure blockchain smart contract. Blockchain is gaining popularity for verifying the integrity and authenticity of on-device FL models [155]. Because 5G allows a huge number of federated clients to join in model creation, the authors in [156] proposed a byzantine-resilient distributed learning suitable for 5G networks. Although applied in the vehicular IoT domain, the work shown in [157] uses a permissioned blockchain and a local directed acyclic graph to secure the DL model parameters. The blockchain ensures the reliability of the shared data that are used for the deep reinforced learning process within the FL network. Researchers have proposed a consortium blockchain for finding the reputation of each federated node so that the IoT nodes or mobile federated nodes that have either malicious data or poor-quality data can be filtered [158]. A secure DL model called secureSVM was developed by the authors in [159] that did not require a trusted third party. The IoHT data was first encrypted using the Paillier homomorphic cryptosystem, and then the encrypted IoHT data was stored in the blockchain for immutability and provenance. Data poisoning and inferencing attacks on FL algorithms were surveyed in [160]. The survey also proposes the design factors of a resilient FL model.
End-to-End Encrypted DL Application
DL applications using IoHT require confidentiality and security. The authors in [161] proposed an encrypted facial recognition algorithm called Wasserstein generative adversarial network encryption to encrypt facial features. A demonstration of using fully homomorphic encryption (FHE) called MORE (matrix operation for randomization or encryption) shows [162] that the training can take place on an encrypted dataset. Finally, the inferencing algorithm can classify the encrypted X-ray images. The proposed end-to-end encryption algorithm was applied to the MNIST dataset, and the performance was satisfactory compared with plain text DL. To support crowdsourcing in blockchain-enabled FL with high security, the authors in [163] proposed the ElGamal public-key cryptographic scheme to protect the communication among federated blockchain worker and requester nodes. Researchers have used blockchain to monitor and control global model updates and aggregation from local federated models [164]. The authors in [165] proposed an FHE that could encrypt a batch of local model update gradients to lower communication and computational costs. To protect IoT data privacy, the authors in [166] proposed a secure parameter aggregation technique called a gated recurrent unit, which supports FL without disclosing private IoT data.
Secure Internet of the Health Things (IoHT)
Previously, researchers proposed lightweight security protocols for the IoHT [130, 167]. For example, XOR, addition, subtraction, and a hash-based authentication protocol were proposed for bringing trust to IoHT device-device authentication [168]. A lightweight, secure key exchange algorithm was designed for IoHT-based EHR data exchange scenarios in which a three-way handshake takes place between an IoT device, a gateway, and the IoT cloud [169]. IoHT data privacy and the secure aggregation of FL models were presented in [170], where hardware-based security protection and a Diffie–Hellman key exchange protocol were used to make an Ethereum native encryption toolkit. Bringing trust to IoHT data was the central focus of the research presented in [171]. A privacy protected IoHT framework was designed in [172], where IoHT data with provenance and audit trails were delivered to authorized subscribers. The authors in [173] designed a cryptosystem that can secure IoHT data during transmission between two endpoints. The cryptosystem was successfully tested with medical image transmission. Federated transfer learning of IoHT data was proposed in [174]. There was a recent initiative of the Internet Engineering Task Force to manage DDoS or man-in-the-middle attacks on the IoHT suggested using a manufacturer usage description (MUD) as a unique signature [175]. An FL architecture can use the MUD signature with the IoHT to provide security for DL applications at the edge.
Chapter 5: Discussion, Conclusion, and Recommendations for Future Work
Discussion
To avoid the shutdown of businesses, education, economies, traveling, and industries and minimize the loss of humans, every country in the world has invested in technologies to overcome the effects of COVID-19. For example, technologies such as DL have been invented to develop vaccines and drugs. Social distancing and facial mask detection techniques have been implemented using AI. Diagnosis of COVID-19 using DL from automated and non-invasive body temperature measurements, cough sounds, CT scans, and X-ray images has been done in many hospitals. Spreading patterns and monitoring of COVID-19 cases are done using machine learning. Blockchain and machine learning have been used to manage health passports. DL has been used to forecast hospital ICU or treatment-related supply chain management. Governments are also using AI for lockdown enforcement through camera-based social gathering, facial recognition, and car plate number recognition.
In summary, technologies have made their footprint in containing the effects of COVID-19. Figure 15 shows a scenario on how an AI hospital can employ diversified types of diagnosis modules to treat COVID-19 patients in a hospital. The figure shows that a patient entering the hospital can be checked with DL modules responsible for initial screening with non-invasive fever detection. His/her face recognition for electronic health records (EHRs) and electronic medical records (EMRs) can also be checked, and data can be pulled to look at his/her past travel history. If any positive result comes out, the patient is directed to a COVID-19 dedicated area equipped with more deep-learning modules and diagnosis facilities. This will allow less human exposure to the pathogen.

Use of DL for automated COVID-19 diagnosis
Figure 16 shows a scenario where a patient visits an AI-enabled hospital, which leverages automated usage of diversified types of technologies, as discussed above [176]. In every visit, certain types of tasks are performed. Such tasks include patient recognition and appointment validation, storing doctor’s handwritten medical notes in patients’ profiles, adding medical diagnosis results and further recommendations to patients’ profiles, maintaining and updating treatment plans for patients, orchestrating a follow-up mechanism, generating and storing prescriptions, and finally updating EHRs and medical records. These are usually performed through manual human interventions, which renders the whole process prone to errors and long delays in patients’ next visit. However, recent AI and DL applications have shown excellent human-level accuracy in maintaining and accomplishing the tasks mentioned above and can perform them automatically [177]. Researchers have proposed different families of AI algorithms to perform these tasks through an automated process while consuming negligible time with higher accuracy [178]. For example, handwritten medical notes, prescriptions, and other types of content can be automatically read by an OCR algorithm and made a digital copy. All the symptoms reported by each patient during each hospital visit are added to the profile through the speech-enabled AI algorithm [179]. In this way, each visit will result in a rich set of data points, which will allow the doctor to have greater insight and make a better treatment plan, plan the next visit, and so on. Finally, human resources at the hospital will be able to interact with the AI to approve or moderate the results. Since a patient might have to visit multiple hospitals for different types of treatment and share the health records, a recent innovation in blockchain shows promising results in securely sharing and updating the health records within multiple institutions. Being the owner of his/her EHRs, a patient can share certain or all parts of EHR with a community of interest, with diagnosis results, prior doctor’s notes, and so on [123]. This interoperability and interaction with digital records will allow better healthcare and lower unnecessary costs.

AI-enabled hospital
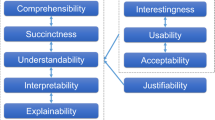
Another vital aspect that needs to be addressed by AI researchers to help medical professionals is the incorporation of several areas of AI within the medical diagnosis workflow. Figure 17 shows the advanced need for AI. Medical doctors in particular and humans in general have to use a solid ethical background to give the needed trust in case of medical treatment. Hence, the AI or DL algorithms must show human-level ethics within their algorithms to assure medical doctors about its ethics. DL algorithms can show bias if the algorithms are trained with insufficient or unbalanced datasets. Once a model has been trained and deployed in a real-life diagnosis environment, medical doctors have no way of identifying such biasness. This will lead to incorrect diagnosis results. Hence, the AI algorithm must show fairness in the treatment. Another aspect of AI is the explainability of the algorithm. The existing blackbox nature of DL algorithms does not explain how the input was processed and how the conclusion was drawn regarding the diagnosis. The way one doctor explains the evidence to another doctor and convinces him/her with reasoning is a fundamental requirement of semantic human-AI teaming. If a doctor makes any mistake in a treatment plan, he/she is held responsible. However, a big concern is what happens to an AI algorithm that is used for diagnosis. If the AI algorithm makes any mistake, will the AI algorithm be held responsible? If an AI algorithm makes any mistake in diagnosis, it should be auditable by the respective authority. Finally, the patient data’s security, safety, and privacy must be ensured, as the DL algorithms are exposed to a large amount of patient data during training and inferencing. Figure 17 shows a scenario in which an AI with the above features interacts with a human doctor: a cancer patient with COVID-19 symptoms. It is expected that the technologies described in this chapter will converge and fuse together to support COVID-19 pandemic management.

Doctor-AI semantic interaction scenario for diagnosing COVID-19 patients
Conclusion
In this article, we highlighted some current and published research discussing the latest ways to use the latest technologies to help fight the COVID-19 virus. We emphasized DL techniques, blockchain, and the 5G network. From what has been explained previously, we conclude that an urgent need remains to intensify efforts in developing algorithms that contribute to integrating DL technology for automatic detection of COVID-19 patients through chest X-rays to obtain the results of accurate tests to be dispensed by those that use PCR technology. Moreover, the advantage of distinguishing cough for those with respiratory diseases, especially COVID-19, still needs more data to improve the results of the algorithms. Finally, research has efficiently demonstrated that blockchain is one of the most promising technologies in securing and selective sharing of medical records, which directly contributes to improving COVID-19’s decision-making results.
Recommendations
As shown in Table 1, the COVID-19 has opened the doors of many technological areas that can help in pandemic management. However, there are several joint initiatives that need to be taken by different relevant entities. For example, medical doctors treating COVID-19 patients need to be trained and updated with the new AI-based diagnosis tools. Medical institutions and healthcare organizations treating COVID-19 patients should allow novel research ideas with clinical trials. Collaboration between academia with a research background, funding, and hands-on experience and medical professionals should be established so that both entities can share their living-lab experiences. One of the shortcomings of DL AI models is that the models need to be trained with real-life patient datasets. The collaboration between AI and blockchain researchers and the medical professional will allow such datasets to be available for clinical trials. Furthermore, the privacy and security of the COVID-19 treatment-related data need to be ensured. Collaboration between the two entities and the use of technologies will also make the EHR and EMR data safe and secure.
References
World Health Organization. Situation report-73. World Health Organization; 2020. https://doi.org/10.3201/eid2606.200239
Shereen MA, Khan S, Kazmi A, Bashir N, Siddique R. COVID-19 infection: origin, transmission, and characteristics of human coronaviruses. J Adv Res. 2020;24:91–8. https://doi.org/10.1016/j.jare.2020.03.005.
Amira F, et al. CoronaTracker: World-wide COVID-19 outbreak data analysis and prediction CoronaTracker Community Research Group Correspondence to Fairoza. https://doi.org/10.2471/BLT.20.251561.
Shen M, et al. Recent advances and perspectives of nucleic acid detection for coronavirus. J Pharm Anal. 2020;10(2):97–101. https://doi.org/10.1016/j.jpha.2020.02.010.
Phan T. Novel coronavirus: from discovery to clinical diagnostics. Infect Genet Evol. 2020. https://doi.org/10.1016/j.meegid.2020.104211.
Mavragani A. Tracking COVID-19 in Europe: infodemiology approach. JMIR Public Health Surveill. 2020;6(2):e18941. https://doi.org/10.2196/18941.
Schüttler J, Schlickeiser R, Schlickeiser F, Kröger M. COVID-19 predictions using a gauss model, based on data from April 2. Physics. 2020;2(2):197–212. https://doi.org/10.3390/physics2020013.
Abdur Rahman MD, Shamim Hossain M, Alrajeh NA, Gupta BB. A Multimodal, multimedia point-of-care deep learning framework for COVID-19 diagnosis. ACM Trans. Multimedia Comput. Commun. Appl. 2021;17(1):24. https://doi.org/10.1145/3421725
Pop G, Cucu H, Burileanu D. Cough sound recognition in respiratory disease epidemics. Rom J Inf Sci Technol. 2020;23(S):S77-88.
Rudraraju G, et al. Cough sound analysis and objective correlation with spirometry and clinical diagnosis. Inform Med Unlocked. 2020;19: 100319. https://doi.org/10.1016/j.imu.2020.100319.
Imran A, et al. AI4COVID-19: AI enabled preliminary diagnosis for COVID-19 from cough samples via an App. 2020. http://arxiv.org/abs/2004.01275.
CIADA center launches a scientific experiment to test for coronavirus via the person’s cough. https://uqu.edu.sa/en/App/News/79347. Accessed 21 June 2020.
Jeremy H, Samantha R. Scientists developing app based on sound of COVID-19 cough. 2020. https://www.wbur.org/hereandnow/2020/04/15/COVID-19-cough-sound-app. Accessed 20 June 2020.
Wang S, et al. A deep learning algorithm using CT images to screen for Corona Virus Disease (COVID-19). 2020. https://doi.org/10.1101/2020.02.14.20023028.
Saiz F, Barandiaran I. COVID-19 detection in chest X-ray images using a deep learning approach. Int J Interact Multimed Artif Intell. 2020. https://doi.org/10.9781/ijimai.2020.04.003.
Wang L, Wong A. COVID-Net: a tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. 2020. arxiv:2003.09871.
Hemdan EE-D, Shouman MA, Karar ME. COVIDX-Net: a framework of deep learning classifiers to diagnose COVID-19 in X-ray images. 2020. arxiv:2003.11055.
Cheng SC, et al. First case of Coronavirus Disease 2019 (COVID-19) pneumonia in Taiwan. J Formos Med Assoc. 2020;119(3):747–51. https://doi.org/10.1016/j.jfma.2020.02.007.
Li L, et al. Artificial intelligence distinguishes COVID-19 from community acquired pneumonia on chest CT. Radiology. 2020. https://doi.org/10.1148/radiol.2020200905.
Narin A, Kaya C, Pamuk Z. Automatic detection of coronavirus disease (COVID-19) using X-ray images and deep convolutional neural networks. 2020. arxiv:2003.10849.
Ozturk T, Talo M, Yildirim EA, Baloglu UB, Yildirim O, Acharya UR. Automated detection of COVID-19 cases using deep neural networks with X-ray images. Comput Biol Med. 2020;121: 103792. https://doi.org/10.1016/j.compbiomed.2020.103792.
Afshar P, Heidarian S, Naderkhani F, Oikonomou A, Plataniotis KN, Mohammadi A. COVID-CAPS: a capsule network-based framework for identification of COVID-19 cases from X-ray Images. 2020. arxiv:2004.02696.
Khan AI, Shah JL, Bhat M. CoroNet: a deep neural network for detection and diagnosis of COVID-19 from chest X-ray images. 2020. arxiv:2004.04931.
Cohen JP, Morrison P, Dao L. COVID-19 image data collection. 2020. arxiv:2003.11597.
Rahman MS, Peeri NC, Shrestha N, Zaki R, Haque U, Hamid SHA. Defending against the Novel Coronavirus (COVID-19) outbreak: how can the Internet of Things (IoT) help to save the world? Health Policy Technol. 2020;9(2):136. https://doi.org/10.1016/j.hlpt.2020.04.005.
Vaishya R, Haleem A, Vaish A, Javaid M. Emerging technologies to combat the COVID-19 pandemic. J Clin Exp Hepatol. 2020. https://doi.org/10.1016/j.jceh.2020.04.019.
Zhai Y, et al. From isolation to coordination: how can telemedicine help combat the COVID-19 outbreak? medRxiv. 2020. https://doi.org/10.1101/2020.02.20.20025957.
Rahman MA, Hossain MS, Alrajeh NA, Guizani N. B5G and explainable deep learning assisted healthcare vertical at the edge: COVID-I9 perspective. IEEE Netw 34(4):98-105. https://doi.org/10.1109/MNET.011.2000353
Shaw R, Kim Y, Hua J. Governance, technology and citizen behavior in pandemic: lessons from COVID-19 in East Asia. Prog Disaster Sci. 2020;6: 100090. https://doi.org/10.1016/j.pdisas.2020.100090.
Sun Y, Mao Y. Editorial. Response to COVID-19 in Chinese neurosurgery and beyond. J Neurosurg. 2020. https://doi.org/10.3171/2020.3.jns20929.
Keshvardoost S, Bahaadinbeigy K, Fatehi F. Role of telehealth in the management of COVID-19: lessons learned from previous SARS, MERS, and ebola outbreaks. Telemed e-Health. 2020. https://doi.org/10.1089/tmj.2020.0105.
Fighting COVID-19 with 5G enabled technologies—Huawei Australia Hub. https://huaweihub.com.au/fighting-COVID-19-with-5g-enabled-technologies/. Accessed 16 June 2020.
Chang MC, Park D. How can blockchain help people in the event of pandemics such as the COVID-19? J Med Syst. 2020. https://doi.org/10.1007/s10916-020-01577-8.
Nguyen DC, Dinh M, Pathirana PN, Seneviratne A. Blockchain and AI-based solutions to combat coronavirus (COVID-19)-like epidemics: a survey. 2020. https://doi.org/10.20944/PREPRINTS202004.0325.V1.
Johnstone S. A viral warning for change. The Wuhan coronavirus versus the red cross: better solutions via blockchain and artificial intelligence. SSRN Electron J. 2020. https://doi.org/10.2139/ssrn.3530756.
Rahardja U, Bist AS, Hardini M, Aini Q, Harahap EP. Authentication of COVID-19 patient certification with blockchain protocol. Int J Adv Sci Technol. 2020;29(8s):4015–24.
Khatoon A. Use of blockchain technology to curb novel coronavirus disease (COVID-19) transmission. SSRN Electron J. 2020. https://doi.org/10.2139/ssrn.3584226.
Azim A, Islam MN, Spranger PE. Blockchain and novel coronavirus: towards preventing COVID-19 and future pandemics. 2020. Iberoam J Med. https://doi.org/10.5281/zenodo.3779244.
Rahman MA, Hossain MS. An internet of medical things-enabled edge computing framework for tackling COVID-19. EEE Internet Things J. 2021. https://doi.org/10.1109/JIOT.2021.3051080t.
Rahman MA, Hossain MS, Alrajeh NA, Gupta B. A multi-modal multimedia point-of-care deep learning framework for COVID-19 diagnosis. ACM Trans Multimed Comput Commun Appl. 2021;17:24. https://doi.org/10.1145/3421725.
Rahman MA, Hossain MS, Alrajeh NA, Alsolami F. Adversarial examples—security threats to COVID-19 deep learning systems in medical IoT devices. EEE Internet Things J. 2021;8(12):9603–10. https://doi.org/10.1109/JIOT.2020.3013710.
Rahman MA, Hossain MS, Islam MS, Alrajeh NA, Muhammad G. Secure and provenance supported internet of health things and edge learning-based COVID-19 management framework. IEEE Access. 2020;8:205071–87. https://doi.org/10.1109/ACCESS.2020.3037474.
Rahman MA, Hossain MS, Alrajeh NA, Guizani N. B5G and explainable deep learning assisted healthcare vertical at the edge—COVID-19 perspective. IEEE Netw. 2020;34(4):98–105. https://doi.org/10.1109/MNET.011.2000353.
Lane ND, Georgiev P, Qendro L. DeepEar: robust smartphone audio sensing in unconstrained acoustic environments using deep learning. In: UbiComp 2015—proceedings on 2015 ACM international joint conference on pervasive ubiquitous Computing, 2015, pp. 283–94. https://doi.org/10.1145/2750858.2804262.
Hande RS, Deshpande PS. An integrated computerized cough analysis by using wavelet for pneumonia diagnosis. Int J Innov Sci Res Technol. 2017;2(9):283–7.
Alonso DP. ANÁLISIS DE SEÑALES DE TOS PARA DETECCIÓN TEMPRANA DE ENFERMEDADES RESPIRATORIAS. Universidad de Valladolid; 2019.
Kvapilova L, et al. Continuous sound collection using smartphones and machine learning to measure cough. Digit Biomark. 2019;3(3):166–75. https://doi.org/10.1159/000504666.
Pham C. MobiCough: real-time cough detection and monitoring using low-cost mobile devices. In: Intelligent information and database systems, 8th Asian conference, ACIIDS 2016, 2016, pp. 300–9.
Porter P, et al. A prospective multicentre study testing the diagnostic accuracy of an automated cough sound centred analytic system for the identification of common respiratory disorders in children. Respir Res. 2019;20(1):1–10. https://doi.org/10.1186/s12931-019-1046-6.
Guo F, et al. Yanbao: a mobile app using the measurement of clinical parameters for glaucoma screening. IEEE Access. 2018;6:77414–28. https://doi.org/10.1109/ACCESS.2018.2882946.
Sundararajan SK. Detection of conjunctivitis with deep learning algorithm in medical image processing. In: 2019 Third international conference on I-SMAC (IoT in Social, Mobile, Analytics and Cloud), 2020, pp. 714–7. https://doi.org/10.1109/i-smac47947.2019.9032705.
Sun X, et al. The infection evidence of SARS-COV-2 in ocular surface: a single-center cross-sectional study. medRxiv. 2020. https://doi.org/10.1101/2020.02.26.20027938.
Butt C, Gill J, Chun D, Babu BA. RETRACTED ARTICLE: Deep learning system to screen coronavirus disease 2019 pneumonia. Applied Intelligence, 1. Advance online publication. 2020. https://doi.org/10.1007/s10489-020-01714-3
Zhang H, et al. Corona virus international public health emergencies: implications for radiology management. Acad Radiol. 2020. https://doi.org/10.1016/j.acra.2020.02.003.
Li L, Qin L, Xu Z, Yin Y, Wang X, Kong B, Bai J, Lu Y, Fang Z, Song Q, Cao K, Liu D, Wang G, Xu Q, Fang X, Zhang S, Xia J, Xia J. Using Artificial Intelligence to Detect COVID-19 and Community-acquired Pneumonia Based on Pulmonary CT: Evaluation of the Diagnostic Accuracy. Radiology. 2020;296(2):E65–E71. https://doi.org/10.1148/radiol.2020200905
Song Y, et al. Deep learning enables accurate diagnosis of novel coronavirus (COVID-19) with CT images. medRxiv. 2020. https://doi.org/10.1101/2020.02.23.20026930.
Xu Y-H, et al. Clinical and computed tomographic imaging features of novel coronavirus pneumonia caused by SARS-CoV-2. J Infect. 2020. https://doi.org/10.1016/j.jinf.2020.02.017.
Al-tawfiq JA, Memish ZA. Diagnosis of SARS-CoV-2 Infection based on CT scan vs RT-PCR: reflecting on experience from MERS-CoV. J Hosp Infect. 2020. https://doi.org/10.1016/j.jhin.2020.03.001.
Wang L, Lin ZQ, Wong A. COVID-Net: a tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. Sci Rep. 2020;10:19549. https://doi.org/10.1038/s41598-020-76550-z
Lin C, et al. Asymptomatic novel coronavirus pneumonia patient outside WuHan: the value of CT images in the course of the disease. Clin Imaging. 2020. https://doi.org/10.1016/j.clinimag.2020.02.008.
Kooraki S, Hosseiny M, Myers L, Gholamrezanezhad A. Coronavirus outbreak: what the department of radiology should know. J Am Coll Radiol. 2020. https://doi.org/10.1016/j.jacr.2020.02.008.
Feng H, Liu Y, Lv M, Zhong J. A case report of COVID-19 with false negative RT-PCR test: necessity of chest CT. Jpn J Radiol. 2020;38(5):409–10. https://doi.org/10.1007/s11604-020-00967-9.
Wang Y, Hou H, Wang W, Wang W. Combination of CT and RT-PCR in the screening or diagnosis of COVID-19. J Glob Health. 2020;10(1):010347. https://doi.org/10.7189/jogh.10.010347.
Maghdid HS, Ghafoor KZ, Sadiq AS, Curran K, Rabie K. A novel AI-enabled framework to diagnose coronavirus COVID 19 using smartphone embedded sensors: design study. arXiv, 2020, pp. 1–5.
Ramesh AN, Kambhampati C, Monson JRT, Drew PJ. Artificial intelligence in medicine. Ann R Coll Surg Engl. 2004;86(5):334–8. https://doi.org/10.1308/147870804290.
Siddiqui MK, et al. Correlation between temperature and COVID-19 (suspected, confirmed and death) cases based on machine learning analysis. J Pure Appl Microbiol. 2020;14(suppl 1):1017–24. https://doi.org/10.22207/jpam.14.spl1.40.
Wang L, Lin ZQ, Wong A. COVID-Net: a tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. Sci Rep. 2020;10:19549. https://doi.org/10.1038/s41598-020-76550-z
Maghded HS, Ghafoor KZ, Sadiq AS, Curran K, Rawat DB, Rabie K. A novel AI-enabled framework to diagnose coronavirus COVID-19 using smartphone embedded sensors: design study. In: 2020 IEEE 21st International Conference on Information Reuse and Integration for Data Science (IRI), 2020, pp. 180–7. https://doi.org/10.1109/IRI49571.2020.00033
Lassau N, et al. AI-based multi-modal integration of clinical characteristics, lab tests and chest CTs improves COVID-19 outcome prediction of hospitalized patients. medRxiv. 2020. https://doi.org/10.1101/2020.05.14.20101972.
Kampf G, Todt D, Pfaender S, Steinmann E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J Hosp Infect. 2020;104(3):246–51. https://doi.org/10.1016/j.jhin.2020.01.022.
Abderrahmane Z, Ganesh G, Crosnier A, Cherubini A. A deep learning framework for tactile recognition of known as well as novel objects. IEEE Trans Ind Inform. 2020;16(1):423–32. https://doi.org/10.1109/TII.2019.2898264.
Chen Y, et al. The presence of SARS-CoV-2 RNA in the feces of COVID-19 patients. J Med Virol. 2020;92:833–40. https://doi.org/10.1002/jmv.25825.
Liu X, Fromm J, Patel SN, McDuff D. Multi-task temporal shift attention networks for on-device contactless vitals measurement. 2020. arxiv:2006.03790
Zhou H, Cheng C, Lipton ZC, Chen GH, Weiss JC. Predicting mortality risk in viral and unspecified pneumonia to assist clinicians with COVID-19 ECMO planning. 2020. arxiv:2006.01898
Schwab P, DuMont Schütte A, Dietz B, Bauer S. Clinical Predictive Models for COVID-19: Systematic Study. J Med Internet Res. 2020 Oct 6;22(10):e21439. https://doi.org/10.2196/21439. PMID: 32976111; PMCID: PMC7541040.
Kai D, Goldstein G-P, Morgunov A, Nangalia V, Rotkirch A. Universal masking is urgent in the COVID-19 pandemic: SEIR and agent based models, empirical validation, policy recommendations. arXiv. 2020.
Hirano H, Koga K, Takemoto K. Vulnerability of deep neural networks for detecting COVID-19 cases from chest X-ray images to universal adversarial attacks. arXiv. 2020.
Selvan R, Dam EB, Rischel S, Sheng K, Nielsen M, Pai A. Lung segmentation from chest X-rays using variational data imputation. arXiv. 2020.
Hossain MS, Muhammad G, Guizani N. Explainable AI and mass surveillance system-based healthcare framework to combat COVID-I9 like pandemics. IEEE Netw. 2020;34(4):126–32.
Sattar H, et al. An IoT-based intelligent wound monitoring system. IEEE Access. 2019;7:144500–15. https://doi.org/10.1109/ACCESS.2019.2940622.
El Asnaoui K, Chawki Y. Using X-ray images and deep learning for automated detection of coronavirus disease. J Biomol Struct Dyn. 2020. https://doi.org/10.1080/07391102.2020.1767212.
Li X, Deng Z, Deng Q, Zhang L, Niu T, Kuang YU. A novel deep learning framework for internal gross target volume definition from 4D computed tomography of lung cancer patients. IEEE Access. 2018;6:37775–83. https://doi.org/10.1109/ACCESS.2018.2851027.
Han Z, et al. Accurate screening of COVID-19 using attention based deep 3D multiple instance learning. IEEE Trans Med Imaging. 2020. https://doi.org/10.1109/tmi.2020.2996256.
Zou Q, Wang Y, Wang Q, Zhao Y, Li Q. Deep learning-based gait recognition using smartphones in the wild. IEEE Trans Inf Forensics Secur. 2020. https://doi.org/10.1109/tifs.2020.2985628.
Alom MZ, et al. A state-of-the-art survey on deep learning theory and architectures. Electronics. 2019. https://doi.org/10.3390/electronics8030292.
Selvaraju RR, Cogswell M, Das A, Vedantam R, Parikh D, Batra D. Grad-CAM: visual explanations from deep networks via gradient-based localization. Int J Comput Vis. 2020;128(2):336–59. https://doi.org/10.1007/s11263-019-01228-7.
Ciaparrone G, Sánchez FL, Tabik S, Troiano L, Tagliaferri R, Herrera F. Deep learning in video multi-object tracking: a survey. Neurocomputing. 2020;381:61–88. https://doi.org/10.1016/j.neucom.2019.11.023.
Jiao L, et al. A survey of deep learning-based object detection. IEEE Access. 2019;7:128837–68. https://doi.org/10.1109/ACCESS.2019.2939201.
Asiri N, Hussain M, Al-Adel F, Alzaidi N. Deep learning based computer-aided diagnosis systems for diabetic retinopathy: a survey. Artif Intell Med. 2019;99: 101701. https://doi.org/10.1016/j.artmed.2019.07.009.
Li X, He Y, Jing X. A survey of deep learning-based human activity recognition in radar. Remote Sens. 2019. https://doi.org/10.3390/rs11091068.
Estrada-Galinanes V, Wac K. Visions and challenges in managing and preserving data to measure quality of life. In: Proceedings of 2018 IEEE 3rd international workshop foundations and applications on Self* Systems FAS*W 2018, 2019, pp. 92–9. https://doi.org/10.1109/FAS-W.2018.00031.
Zhang Z, Zhu Z, Bazor B, Lee SB, Ding Z, Pan T. FeetBeat: a flexible iontronic sensing wearable detects pedal pulses and muscular activities. IEEE Trans Biomed Eng. 2019;66(11):3072–9. https://doi.org/10.1109/TBME.2019.2900224.
Mehendale ND, Shah N, Kamdar L, Gokalgandhi D. Walking pattern analysis using deep learning for energy harvesting smart shoes with IoT. bioRxiv. 2020. https://doi.org/10.1101/2020.05.10.087197.
Alam T. mHealth Communication framework using blockchain and IoT technologies. Int J Sci Res Technol. 2020. https://doi.org/10.2094/preprints202006.0180.v1.
Pratap R, Javaid M, Haleem A, Vaishya R, Ali S. Internet of medical things (IoMT) for orthopaedic in COVID-19 pandemic: roles, challenges, and applications. J Clin Orthop Trauma. 2020;11:1–6.
Madurai R, Pugazhendhi R. Restructured society and environment: a review on potential technological strategies to control the COVID-19 pandemic. Sci Total Environ. 2020;725(138858):1–19.
Javaid M, Haleem A, Vaishya R, Bahl S, Suman R. Industry 4.0 technologies and their applications in fighting COVID-19 pandemic. 2020.
Privacy-Preserving contact tracing - Apple and Google. (n.d.). Retrieved May 06, 2020, from https://covid19.apple.com/contacttracing.
L. (2020, May 05). LifeSignals receives CE Mark Approval for LifeSignals ECG Remote Monitoring Patch Platform (LX1250E). Retrieved June 06, 2020, from https://lifesignals.com/2020/05/05/lifesignals-receives-ce-mark-approval-for-lifesignals-ecg-remote-monitoring-patch-platform-lx1250e/.
Porambage P, Okwuibe J, Liyanage M, Ylianttila M, Taleb T. Survey on multi-access edge computing for internet of things realization. IEEE Commun Surv Tutor. 2018;20(4):2961–91. https://doi.org/10.1109/COMST.2018.2849509.
Vishnu S, Ramson SRJ, Jegan R. Internet of medical things (IoMT)-an overview. In: ICDCS 2020—2020 5th international conference on devices, circuits systems, 2020, pp. 101–4. https://doi.org/10.1109/ICDCS48716.2020.243558.
Greco L, Percannella G, Ritrovato P, Tortorella F, Vento M. Trends in IoT based solutions for health care: moving AI to the Edge. Pattern Recognit Lett. 2020;135:346–53. https://doi.org/10.1016/j.patrec.2020.05.016.
Basatneh R, Najafi B, Armstrong DG. Health sensors, smart home devices, and the internet of medical things: an opportunity for dramatic improvement in care for the lower extremity complications of diabetes. J Diabetes Sci Technol. 2018;12(3):577–86. https://doi.org/10.1177/1932296818768618.
Chamola V, Hassija V, Gupta V, Guizani M. A comprehensive review of the COVID-19 pandemic and the role of IoT, drones, AI, blockchain, and 5G in managing its impact. IEEE Access. 2020;8:90225–65. https://doi.org/10.1109/ACCESS.2020.2992341.
Tripathy AK, Mohapatra AG, Mohanty SP, Kougianos E, Joshi AM, Das G. EasyBand: a wearable for safety-aware mobility during pandemic outbreak. IEEE Consum Electron Mag. 2020;2248:10–4. https://doi.org/10.1109/MCE.2020.2992034.
Kumar A, Sharma K, Singh H, Naugriya SG, Gill SS, Buyya R. A drone-based networked system and methods for combating coronavirus disease (COVID-19) pandemic. arXiv Preprint, 2020, pp. 1–25.
Yang T, Gentile M, Shen CF, Cheng CM. Combining point-of-care diagnostics and internet of medical things (IOMT) to combat the COVID-19 pandemic. Diagnostics. 2020;10(4):4–6. https://doi.org/10.3390/diagnostics10040224.
Tedeschi P, Bakiras S, Di Pietro R. IoTrace: a flexible, efficient, and privacy-preserving IoT-enabled architecture for contact tracing. IEEE Commun Mag. 2020;59(6):82–8.
Rashid MT, Wang D. CovidSens: a vision on reliable social sensing for COVID-19. Artif Intell Rev. 2020. https://doi.org/10.1007/s10462-020-09852-3.
Rahardja U, Bist AS, Hardini M, Aini Q, Harahap EP. Authentication of COVID-19 patient certification with blockchain protocol. IJAST. 2020;29(8):4015–24.
Mettler M, Hsg MA. In: 2016 IEEE 18th international conference on e-health networking, applications and services, Healthcom 2016, 2016, pp. 16–8.
Agbo C, Mahmoud Q, Eklund J. Blockchain technology in healthcare: a systematic review. Healthcare. 2019;7(2):56. https://doi.org/10.3390/healthcare7020056.
Swan M. Bitcoin: blueprint for a new economy. 2015.
CIO.com—tech news, analysis, blogs, video.
The blockchain for healthcare: gem launches gem health network with philips blockchain lab.
Mashamba-Thompson TP, Crayton ED. Blockchain and artificial intelligence technology for novel coronavirus disease-19 self-testing. Diagnostics. 2020;10(4):8–11. https://doi.org/10.3390/diagnostics10040198.
Torky, M., & Hassanien, A. (2020). COVID-19 Blockchain Framework: Innovative Approach. arxiv:2004.06081.
Xu H, Zhang L, Onireti O, Fang Y, Buchanan WB, Imran MA. BeepTrace: blockchain-enabled privacy-preserving contact tracing for COVID-19 pandemic and beyond. arXiv. 2020. https://doi.org/10.13140/RG.2.2.25101.15849/1.
Salman T, Zolanvari M, Erbad A, Jain R, Samaka M. Security services using blockchains: a state of the art survey. IEEE Commun Surv Tutor. 2019;21(1):858–80. https://doi.org/10.1109/COMST.2018.2863956.
Dai H, Member S, Zheng Z, Member S, Zhang Y, Member S. Blockchain for internet of things: a survey. 2020;1(1):1–19. arxiv:1906.00245v5.
Weber I, Lu Q, Tran AB. A platform architecture for multi-tenant blockchain-based systems. 2019;1(1):1–10. arxiv:1901.11219v1.
Rathore S, Pan Y, Park JH. BlockDeepNet: a blockchain-based secure deep learning for IoT network. Sustain. 2019;1(1):1–15.
Nguyen DC, Pathirana PN, Member S. Blockchain for secure EHRs sharing of mobile cloud based e-health systems. IEEE Access. 2019;7:66792–806. https://doi.org/10.1109/ACCESS.2019.2917555.
Tahir M, Sardaraz M, Muhammad S, Khan MS. A lightweight authentication and authorization framework for blockchain-enabled IoT network in health-informatics. Sustain. 2020;12(6960):1–22.
Liang X, Zhao J, Shetty S, Li D. Towards data assurance and resilience in IoT using blockchain. In: Milcom cyber security and trusted computing, 2017, pp. 261–6.
Cui L, Yang S, Chen Z, Pan Y, Xu M, Xu K. An efficient and compacted DAG-based blockchain protocol for industrial internet of things. IEEE Trans Ind Inform. 2019;3203:1–12. https://doi.org/10.1109/TII.2019.2931157.
Khan PW, Byun Y-C, Park N. IoT-Blockchain enabled optimized provenance system for food industry 4.0 using advanced deep learning. Sensors (MDPI). 2020;20(2990):1–24. https://doi.org/10.3390/s20102990.
Abou-nassar EM, Iliyasu AM, El-kafrawy PM, Song O, Bashir ALIK, El-latif AAA. DITrust Chain: towards blockchain-based trust models for sustainable healthcare IoT systems. IEEE Access. 2020;8:111223–38. https://doi.org/10.1109/ACCESS.2020.2999468.
Javaid U, Aman MN, Sikdar B. BlockPro: block chain based data pro venance and integrity for secure IoT environments. In: 1st Workshop on blockchain-enabled networked sensor systems (BlockSys’18), 2018, pp. 1–6.
Kamal M, Tariq M. Light-weight security and blockchain based provenance for advanced metering infrastructure. IEEE Access. 2019;7:87345–56. https://doi.org/10.1109/ACCESS.2019.2925787.
Mendis GJ, Wu Y, Wei J, Sabounchi M, Roche R. Blockchain as a service: a decentralized and secure computing paradigm. 2019;1(1):1–14. arxiv:1807.02515v3.
Liu Y, Peng J, Kang J, Iliyasu AM, Niyato D, El-Latif AAA. A secure federated learning framework for 5G networks. IEEE Wirel Commun. 2020;27(4):24–31.
Zhang W et al. Blockchain-based federated learning for failure detection in industrial IoT. 2020;1(1):1–11. arxiv:2009.02643v1.
Lu Y, Huang X, Dai Y, Maharjan S, Zhang Y. Blockchain and federated learning for privacy-preserved data sharing in industrial IoT. IEEE Trans Ind Inform. 2020;16(6):4177–86.
Zhao Y, Zhao J, Kang J, Zhang Z, Niyato D, Shi S. A blockchain-based approach for saving and tracking differential-privacy cost. 2020;1(1):1–14. arxiv:2001.09259v1.
Harris JD, Waggoner B. Decentralized and collaborative AI on blockchain. In: 2019 IEEE international conference on blockchain (Blockchain), 2019, pp. 1–9. https://doi.org/10.1109/Blockchain.2019.00057.
Li Y, Chen C, Liu N, Huang H, Zheng Z, Yan Q. A blockchain-based decentralized federated learning framework with committee consensus. 2020;1(1):1–7. arxiv:2004.00773v1.
Zhao Y, et al. Privacy-preserving blockchain-based federated learning for IoT devices. IEEE Internet Things J. 2020;1906(1):1–12.
Gao Y et al. End-to-end evaluation of federated learning and split learning for internet of things. 200;1(1):1–10. arxiv:2003.13376v2.
Guha N, Talwalkar A, Smith V. One-shot federated learning. 2019;1(1):1–5. arxiv:1902.11175v2.
Xiao Y, Ye Y, Huang S, Hao L, Ma Z. Fully decentralized federated learning based beamforming design for UAV communications. 2020;1(1):1–6. arxiv:2007.13614v1.
Chen M, Poor HV, Saad W, Cui S. Wireless communications for collaborative federated learning. 2020;1(1):1–17. arxiv:2006.02499v2.
Xiao Y, Shi G, Krunz M. Towards ubiquitous AI in 6G with federated learning. 2020;1(1):1–7. arxiv:2004.13563v1.
Liu Y, Yuan X, Xiong Z, Kang J, Wang X, Niyato D. Federated learning for 6G communications: challenges, methods, and future directions. China Commun. 2020;17(9):105–18.
Pokhrel SR. Federated learning meets blockchain at 6G edge : a drone-assisted networking for disaster response. In: ACM MobiCom workshop on drone assisted wireless communications for 5G and beyond (DroneCom 20), 2020, pp. 49–54.
Liu Y, et al. Deep anomaly detection for time-series data in industrial IoT: a communication-efficient on-device federated learning approach. IEEE Internet Things J. 2020;1(1):1–11.
Qu Y, et al. Decentralized privacy using blockchain-enabled federated learning in fog computing. IEEE Internet Things J. 2020;7(6):5171–83.
Yu S, Chen X, Zhou Z, Gong X, Wu D. When deep reinforcement learning meets federated learning: intelligent multi-timescale resource management for multi-access edge computing in 5G ultra dense network. 2020;1(1):1–14. arxiv:2009.10601v1.
Mugunthan V, Rahman R, Kagal L. BlockFLow: an accountable and privacy-preserving solution for federated learning. 2020;1(1):1–12. arxiv:2007.03856v1.
Habib M, Salah K, Damiani E, Svetinovic D. Towards blockchain-based reputation-aware federated learning. In: IEEE INFOCOM 2020—IEEE conference on computer communications workshops (INFOCOM WKSHPS), 2020, pp. 183–188.
Aïvodji UM, Gambs S, Martin A. IOTFLA: a secured and privacy-preserving smart home architecture implementing federated learning. In: 2019 IEEE security and privacy workshops (SPW), 2019, pp. 175–180. https://doi.org/10.1109/SPW.2019.00041.
Mcclellan M, Cervelló-pastor C, Sallent S. Deep learning at the mobile edge: opportunities for 5G networks. Appl Sci. 2020;20(4735):1–27. https://doi.org/10.3390/app10144735.
Isaksson M, Norrman K. Secure federated learning in 5G mobile networks. 2020;1(1):1–7. arxiv:2004.06700v2.
Hua G, Zhu LI, Wu J, Shen C, Zhou L, Lin Q. Blockchain-based federal learning for intelligent control in heavy haul railway. IEEE Access. 2020;8:176830–9. https://doi.org/10.1109/ACCESS.2020.3021253.
Kim H, Park J, Bennis M, Kim S. Blockchained on-device federated learning. IEEE Commun Lett. 2019;24(6):1279–83. https://doi.org/10.1109/LCOMM.2019.2921755.
Zhou S, Huang H, Chen W, Zheng Z, Guo S. PIRATE: a blockchain-based secure framework of distributed machine learning in 5G networks. 2019;1(1):1–8. arxiv:1912.07860v1.
Lu Y, Huang X, Zhang K, Maharjan S, Zhang Y. Blockchain empowered asynchronous federated learning for secure data sharing in internet of vehicles. IEEE Trans Veh Technol. 2020;69(4):4298–311.
Kang J, Xiong Z, Niyato D, Zou Y, Zhang Y, Guizani M. Reliable federated learning for mobile networks. 2019;1(1):1–8. arxiv:1910.06837v1.
Shen M, Tang X, Zhu L, Du X, Guizani M. Privacy-preserving support vector machine training over blockchain-based encrypted IoT data in smart cities. IEEE Internet Things J. 2019;6(5):7702–12.
Lyu L, Yu H, Yang Q. Threats to federated learning: a survey. 2020;1(1):1–7. arxiv:2003.02133v1.
Wu C, Ju B, Wu Y, Xiong NN, Zhang S. WGAN-E: a generative adversarial networks for facial feature security. Electron. 2020;9(486):1–20.
Vizitiu A, Niţ CI, Puiu A, Suciu C, Itu LM. Applying deep neural networks over homomorphic encrypted medical data. Comput Math Methods Med. 2020;2020(3910250):1–26.
Li Z, Liu J, Hao J, Wang H, Xian M. CrowdSFL: a secure crowd computing framework based on blockchain and federated learning. Electron. 2020;9(773):1–21. https://doi.org/10.3390/electronics9050773.
Majeed U, Hong CS. FLchain: federated learning via MEC-enabled blockchain network. In: 20th Asia-Pacific Network Operations and Management Symposium (APNOMS) 2019, 2019, pp. 1–4.
Zhang C, Li S, Xia J, Wang W, Kong H. BatchCrypt: efficient homomorphic encryption for cross-silo federated learning. In: 2020 USENIX annual technical conference, 2020, pp. 493–506.
Liu Y, Member S, Yu JJQ, Kang J, Niyato D, Zhang S. Privacy-preserving traffic flow prediction: a federated learning approach. IEEE Internet Things J. 2020;1(1):1–12.
Kamal M, Srivastava G, Tariq M. Blockchain-based lightweight and secured V2V communication in the internet of vehicles. IEEE Trans Intell Transp Syst. 2020;1(1):1–8.
Lara E, Aguilar L, Sanchez MA, García JA. Lightweight authentication protocol for M2M communications of resource-constrained devices in industrial internet of things. Sens MDPI. 2020;20(501):1–22. https://doi.org/10.3390/s20020501.
More S, et al. Security assured CNN-based model for reconstruction of medical images on the internet of healthcare things. IEEE Access. 2020;8:126333–46.
Passerat-palmbach J, Farnan T, Miller R, Flannery HL, Gross MS, Gleim B. A blockchain-orchestrated federated learning architecture for healthcare consortia. 2019;1(1):1–6. arxiv:1910.12603v1.
Jaigirdar FT, Rudolph C, Bain C. Can i trust the data i see? In: ACSW’19, 2019, pp. 1–10.
Lomotey RK, Sofranko K, Orji R. Enhancing privacy in wearable Iot through a provenance architecture. Multimodal Technol Interact. 2018;2(18):1–13. https://doi.org/10.3390/mti2020018.
Tsafack N, et al. A new chaotic map with dynamic analysis and encryption application in internet of health things. IEEE Access. 2020;8(1):137731–44. https://doi.org/10.1109/ACCESS.2020.3010794.
Chen Y, Wang J, Yu C, Gao W, Qin X. FedHealth: a federated transfer learning framework for wearable healthcare. 2019;1(1):1–8. arxiv:1907.09173v1.
Feraudo A, Popescu DA, Bellavista P, Crowcroft J. CoLearn: enabling federated learning in MUD-compliant IoT edge networks. In: EdgeSys’20, 2020, pp. 1–6.
Zhao Y, Yin Y, Gui G. Lightweight deep learning based intelligent edge surveillance techniques. IEEE Trans Cogn Commun Netw. 2020;6(4):1146–54. https://doi.org/10.1109/TCCN.2020.2999479.
She C, et al. A tutorial on ultrareliable and low-latency communications in 6G: integrating domain knowledge into deep learning. Proc IEEE. 2021;109(3):204–46. https://doi.org/10.1109/JPROC.2021.3053601.
Zhang Z, et al. Deep learning in omics: a survey and guideline. Brief Funct Genom. 2019;18(1):41–57. https://doi.org/10.1093/bfgp/ely030.
Wang W, Liu F, Zhi X, Zhang T, Huang C. An integrated deep learning algorithm for detecting lung nodules with low-dose CT and its application in 6G-enabled internet of medical things. IEEE Internet Things J. 2020;8(7):1–1. https://doi.org/10.1109/jiot.2020.3023436.
Funding
This research is funded by King Abdulaziz City for Science and Technology through its grant#5-20-01-127-0001.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the topical collection “Computer Aided Methods to Combat COVID-19 Pandemic” guest edited by David Clifton, Matthew Brown, Yuan-Ting Zhang and Tapabrata Chakraborty.
Rights and permissions
About this article

Cite this article
Alharbi, A., Abdur Rahman, M. Review of Recent Technologies for Tackling COVID-19. SN COMPUT. SCI. 2, 460 (2021). https://doi.org/10.1007/s42979-021-00841-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s42979-021-00841-z