
Interventions for Maintenance of Essential Health Service Delivery during the COVID-19 Response in Uganda, between March 2020 and April 2021
 , ,
, , {kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Description of the Health System in Uganda
2.3. Maintenance of Essential Health Service Delivery
3. Data Collection
3.1. Document Review
3.2. Qualitative Data Collection
3.3. Qualitative Data Analysis
3.4. Ethical Considerations
4. Results
4.1. Essential Health Services during the COVID-19 Pandemic
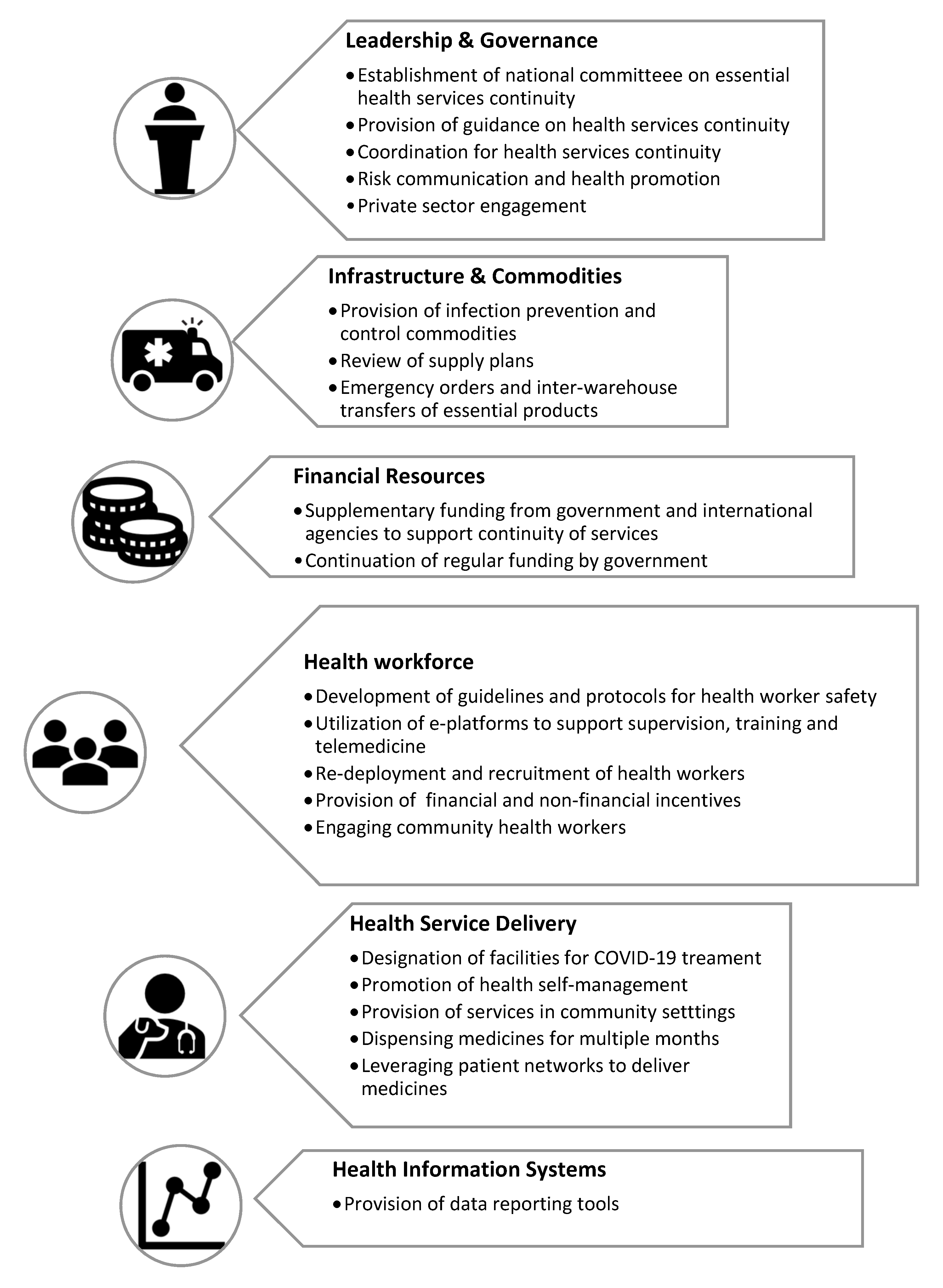
4.2. Interventions to Maintain Delivery of Essential Health Services
4.3. Leadership, Governance and Coordination
- (a)
- Establishment of national committee on continuity of essential health services. In April 2020, the Uganda MoH constituted a committee at national level to ensure the continuity of provision of essential health services [22]. Members of the committee included MoH officials, representatives from District Local Governments, national public health authorities, Health Development Partner Organizations such as UNICEF and WHO, and other Civil Society Organizations. The committee was chaired by the Director of Clinical Services who was the National Focal Point for essential health services continuity. The committee coordinated all efforts to promote maintenance of access to health services. District Health Officers were invited to present to the committee about the trends in access to care within their jurisdictions. Where disruptions were noted, interventions were proposed and implemented.
- (b)
- Provision of guidance on health services continuity. In April 2020, the MoH published guidelines for the continuity of essential health services [16]. The guidelines defined the priority essential health services and provided guidance on immediate actions for the continuity of health access and monitoring service delivery. In June 2021, the MoH published a COVID-19 resurgence plan that was informed by lessons learnt in the first year of the response to the pandemic [18]. The plan strengthened the coordination of the COVID-19 response through the establishment of support teams for essential health services maintenance at regional level, occupational health and safety in health facilities and maintaining access to essential medicines and commodities.
- (c)
- Coordination for health service continuity at subnational and facility levels: At subnational level-regional, district and facility levels, the government established sub-committees to provide oversight and coordinate the maintenance of essential health services in the context of COVID-19 [16,22]. With respect to the functionality of these sub-committees a key informant noted.
“We had meetings and decided to divide ourselves in such a way that there are those on the frontline in running COVID-19 activities in the hospital and other colleagues would continue running routine medical services in the hospital and the region at large. These meetings and coordination were not just done at the hospital level, but we also had the district on board, the District Health Officer (DHO) together with his team, and the Resident District Commissioner (RDC)”KII Two Regional Referral Hospital
- (d)
- Risk communication and health promotion. The MoH also developed information, education and communication (IEC) materials and conducted media campaigns encouraging people to continue to access health services while preventing COVID-19 [15,22] and combating stigmatization of persons recovering from COVID-19. Health facilities used multi-media such as television and radio to communicate to the public about procedures for accessing emergency and other health care as noted by the key informant below:
“… (the hospital) started its first use of call and dispatch center for the ambulance during the COVID-19 time…. We disseminated these numbers on radio and … were receiving calls from the communities on those numbers to go and pick stranded patients using our ambulances….”KII Eight, Regional Referral Hospital
- (e)
- Private sector engagement. By including the private sector in the COVID-19 response effort at both national and district level, this category of stakeholders was able to contribute to the response and support continuity of services. They provided financial support, personal protective equipment and transport for both patients and health workers. For example, at the national level, at least 65 motor vehicles and 19 motorcycles were received from the private sector as in-kind donations to support both the COVID-19 response [15] and the maintenance of access to health services. Key informants acknowledged receipt of such support from the private sector.
“We received a few private donors to give us items that were used in the management of COVID-19 at that time including things like masks, face shields, we received things like money, there is an organization… which gave us seventeen million shillings (5000 USD). We were able to buy a washing machine using that money, we were able to make a few repairs before the ministry money came in…a few repairs of the place… mattresses, blankets… basins... soap.”KII 9 Regional Referral Hospital
“(private organizations) gave us means of transport. Like the vehicles I was speaking about. We had several organisations. Apart from the district vehicle, at least we had a vehicle from World Vision, we had a vehicle from Save the Children, we had a vehicle from World Harvest Mission helping in ferrying our staff and Clients to and from hospital. I’m talking about organizations bringing in physical materials to do with infection prevention. (they also) gave us gloves, they gave us chlorine powder, they gave us items really to use during the outbreak.”KII 6 District Hospital
4.4. Health Workforce
- (a)
- Development of guidelines and protocols for health worker safety. The MOH developed guidelines for managing health care workers who contracted COVID-19 while on duty. The guidance covered issues related to routine screening, limiting the entry of COVID-19 exposed caregivers at health facilities, use of personal protective equipment and promoting hand hygiene [23]. Furthermore, the MOH published a health facility screening algorithm to aid regular COVID-19 screening among health workers to avoid infection [16], promote their safety and facilitate maintenance of service delivery.
- (b)
- Utilization of e-Platforms for Support Supervision, Capacity Building and Telemedicine: Support supervision and mentorship to improve health service delivery was provided via e-platforms or using telephone during the period under study [16,22]. For example, implementing partners transitioned from face-to-face to online training to build the capacity of health workers to provide family planning services during the COVID-19 pandemic. During financial year 2020/2021, health workers from 135 districts were trained in surveillance, contact tracing and provision of home-based care among others [15] via e-platforms in order to decongest health facilities. Furthermore, health workers leveraged e-platforms, tele-pharmacies and tele-laboratories to provide services such as triage, referrals and mobile medical services [24]. The challenge with the use of technology during the COVID-19 response was that the cost of internet remained prohibitively high and internet services coverage were mostly available to the urban population around the country’s capital Kampala city [24].
- (c)
- Re-deployment and recruitment. Several districts in the country recruited and/or re-deployed staff to other facilities to maintain services while a few were assigned to provide care at COVID-19 facilities. In addition, more than 500 health workers were recruited at various levels of the health system to support the COVID-19 response [15]. This contributed to the slight improvement in staffing capacity in health facilities from 73% in 2019/2020 [8] to 74% in 2020/2021 [15].
- (d)
- Provision of financial and non-financial incentives to health workers. Furthermore, the MoH adopted strategies that supported health workers to continue providing health services. These included the provision of financial [14,22] and non-financial incentives such as accommodation and transport. At the peak of movement restrictions, health workers were transported to health facilities that were understaffed to fill human resource gaps [22]. This was noted by key informants as follows:
“…we would move the doctor to do caesarean section especially if the patient was in a facility where the theatre was operational, rather than bring them to the regional referral hospital…. so we take the doctor there and bring them back when they are done.”KII One, District Health Officer
“I can also say there were a lot of efforts on psychosocial support, we had a lot of discussions talking to them, encouraging them, counselling staff and motivating them to work by staying at duty. And at some point, we informed people for instance people who worked so much had to take off time to rest”KII Ten, Senior Medical Officer
- (e)
- Engaging community health workers: Community health workers continued to support the provision of health services at community level during the COVID-19 period under review [16]. The National Malaria Control Program provided community health workers with infection prevention and control commodities and was able to ensure maintenance of community-based services such as indoor residual spraying for mosquito control and integrated community case management of childhood illnesses during the COVID-19 pandemic [8]. Furthermore, the role of community health workers was emphasized in the key informant interviews:
“We asked (the community health workers) to move within the communities where they are to help and mobilize people to come and access care in the hospital. …we would work with them to mobilize HIV+ clients in their communities so that they would meet at a central place in a particular school or church, then they would go there with their pills and then the pills would be given to the patients that they have mobilized in their region.”KII Two, Regional Referral Hospital
4.5. Provision of Financial Resources
- (a)
- Supplementary funding for COVID-19 response from government and international agencies. The parliament of Uganda approved a supplementary budget amounting to 30.7 million USD (114 billion UGX) towards the COVID-19 pandemic response [8]. This translated to about 4.1% of Uganda’s health sector budget in the financial year 2019/2020 [15]. The resources supported all aspects of the response including the payment of contact tracers, the procurement of diagnostic test kits and the strengthening the capacity of intensive care unit (ICU) in the country. In addition, international development organizations such as UNICEF, Global Fund and USAID provided resources to support health services maintenance [8,15]. According to the MoH COVID-19 resurgence plan (June 2021–July 2022) [18], 31 million USD was budgeted to finance the activities related to the maintenance of essential services during the period. The activities included supporting the national medical stores to maintain access to essential commodities, strengthen reporting and monitoring of service delivery through tracking performance using standardized indicators.
- (b)
- Continuation of recurrent funding by government. Health facilities continued to receive the quarterly disbursements of funds for the implementation of all essential health services which minimized health services disruption as noted by a key informant below:
“We normally get funds for primary health care and we continued to get it, there was no shortage of funds, the funding was as it used to be.”KII Nine, General Hospital
4.6. Infrastructure and Commodities
- (a)
- Provision of infection prevention and control commodities. The Environmental Health Department of the MoH procured and distributed commodities that promoted infection prevention and control in health care settings including hand washing facilities, hand sanitizers and handheld sprayers to 941 health care facilities in 44 districts [8,14].
- (b)
- Review of Supply plans. The pharmacy division of the MoH reviewed the supply plans for antiretroviral drugs (ARVs), commodities for voluntary medical male circumcision, drugs for treating opportunistic infections, reproductive health and laboratory commodities to avoid stockouts [8]. This enabled the maintenance of delivery of drugs and medicines for essential services as noted by a key informant:
“As for the supply of medicine and other supplies, we maintained coordination with National and Joint Medical Stores (drug distributors), we would make our order and they would deliver in time.”KII Seven, General Hospital
- (c)
“…I remember an emergency order was made to purchase some personal protective equipment (PPEs) because in our hospital we never had masks… aprons were not enough and other PPEs so emergency order was done to purchase that equipment…”KII Three, General Hospital
4.7. Health Service Delivery
- (a)
- Designation of facilities for COVID-19 treatment. Uganda’s health system is composed of the national referral hospitals, regional referral hospitals, District Hospitals, Health Center IVs, IIIs, IIs and community health workers. The system is referral based with more complex and specialized services offered at higher levels of the health system. The regional referral hospitals were designated as COVID-19 treatment units so that health service delivery at other levels of the health system could continue [14,16]. However, the designation of the regional referral hospitals for managing COVID-19 patients also affected access to other non-COVID-19 services as noted by an informant below:
…the (patients) had fear of being in hospital environments. Some of them had the fear that they could contract COVID-19 from hospitals especially they started learning that we had admitted patients. Some of them feared to come to the hospital for that reason...”KII Eight, Regional Referral Hospital
- (b)
- Promotion of self-management. The AIDS Control Program promoted HIV self-testing through development and dissemination of HIV self-testing videos and brochures in multiple local languages [8].
- (c)
- Provision of services in community settings: Health workers conducted targeted and integrated antenatal care and immunization outreaches within communities to extend services especially in hard-to-reach communities with many pregnant women [16,22]. As noted by several key informants, health facilities engaged in various activities to take services to communities to ensure maintenance of service provision:
“We continued to offer immunization outreaches, we continued to offer drug distribution especially for HIV and those ones who were having hypertension, diabetes. We would move out after announcing then we find these people in the communities and deliver the medicine to them”KII Ten, General Hospital
- (d)
“We have also learnt that for stable patients you do not need to see them weekly, monthly, we have been able to maintain the mode of giving them drugs for 3 to 6 months and that way we have been able to decongest even the HIV clinics and then we have been able to focus on those that are failing treatment and those who have challenges so that we offer them quality care”KII Eight, Regional Referral Hospital
- (e)
- Leveraging patient networks to deliver medicines. For disease conditions such as HIV where there was an existing network where patients within specific communities knew each other, service providers gave medicines to one patient who then distributed them to patients within their community network [8,15]. This was also noted by key informants:
“I think the other innovation is that of grouping the HIV clients and asking them to pick their medicines and one person comes and picks and takes it to them at given point and distributes.”District Health Officer
4.8. Health Information Systems
- (a)
- Provision of reporting tools. To address the challenge of timely reporting into the national surveillance system, the Division of Health Information engaged the District Health Officers and district biostatisticians to step in for the complete and timely submission of service statistics and reports to the relevant platforms. In addition, the MoH provided information and communication hardware including phones, tablets and computers to 135 districts to improve timely reporting [15]. Other interventions to address reporting gaps were issuance of circulars and provision of transport to reporting personnel as noted by two key informants:
“We sent circulars to the members to make sure that we continued with our reporting and surveillance, we encouraged a lot of reports, that’s at a health facility ward level for example every morning the in-charges they had to tell us.”KII Three, General Hospital
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Richards, M.; Anderson, M.; Carter, P.; Ebert, B.L.; Mossialos, E. The impact of the COVID-19 pandemic on cancer care. Nat. Cancer 2020, 1, 565–567. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R. COVID-19 disrupts vaccine delivery. Lancet Infect. Dis. 2020, 20, 546. [Google Scholar] [CrossRef]
- McQuaid, C.F.; Vassall, A.; Cohen, T.; Fiekert, K.; White, R. The impact of COVID-19 on TB: A review of the data. Int. J. Tuberc. Lung Dis. 2021, 25, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Lal, A.; Erondu, N.A.; Heymann, D.L.; Gitahi, G.; Yates, R. Fragmented health systems in COVID-19: Rectifying the misalignment between global health security and universal health coverage. Lancet 2021, 397, 61–67. [Google Scholar] [CrossRef]
- World Health Organisation. Health Security. 2022. Available online: https://www.who.int/health-topics/health-security#tab=tab_1 (accessed on 12 September 2022).
- Chandir, S.; Siddiqi, D.A.; Setayesh, H.; Khan, A.J. Impact of COVID-19 lockdown on routine immunisation in Karachi, Pakistan. Lancet Glob. Health 2020, 8, e1118–e1120. [Google Scholar] [CrossRef]
- Ahmed, S.A.K.S.; Ajisola, M.; Azeem, K.; Bakibinga, P.; Chen, Y.-F.; Choudhury, N.N.; Fayehun, O.; Griffiths, F.; Harris, B.; Kibe, P.; et al. Impact of the societal response to COVID-19 on access to healthcare for non-COVID-19 health issues in slum communities of Bangladesh, Kenya, Nigeria and Pakistan: Results of pre-COVID and COVID-19 lockdown stakeholder engagements. BMJ Glob. Health 2020, 5, e003042. [Google Scholar] [CrossRef]
- Ministry of Health. Annual Health Sector Performance Report 2019/2020; Ministry of Health: Kampala, Uganda, 2020. [Google Scholar]
- Kruk, M.E.; Myers, M.; Varpilah, S.T.; Dahn, B.T. What is a resilient health system? Lessons from Ebola. Lancet 2015, 385, 1910–1912. [Google Scholar] [CrossRef]
- World Health Organization. Monitoring the Building Blocks of Health Systems: A Handbook of Indicators and Their Measurement Strategies; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- World Health Organization. Maintaining Essential Services: Operational Guidance for the COVID-19 Context; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Wang, Z.; Grundy, Q.; Parker, L.; Bero, L. Variations in processes for guideline adaptation: A qualitative study of World Health Organization staff experiences in implementing guidelines. BMC Pub. Health 2020, 20, 1758. [Google Scholar] [CrossRef]
- World Health Organisation. COVID-19: Operational Guidance for Maintaining Essential Health Services During an Outbreak; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Ministry of Finance Planning and Economic Development. Budget Monitoring and Accountability Unit. COVID-19 Interventions Report Financial Year 2019/2020; Ministry of Finance Planning and Economic Development: Kampala, Uganda, 2020. [Google Scholar]
- Ministry of Health. Annual Health Sector Performance Report 2020/2021; Ministry of Health: Kampala, Uganda, 2021. [Google Scholar]
- Ministry of Health (MOH) Uganda. Guidance on Continuity of Essential Health Services during the COVID-19 Outbreak; Ministry of Health: Kampala, Uganda, 2020. [Google Scholar]
- Ministry of Health Uganda. Corona Virus Disease-2019 (COVID-19) Preparedness and Response Plan March 2020–June 2021; Ministry of Health Uganda: Kampala, Uganda, 2020. [Google Scholar]
- Ministry of Health Uganda. COVID-19 Resurgence Plan (June 2021–June 2022); Ministry of Health Uganda: Kampala, Uganda, 2021. [Google Scholar]
- Van Olmen, J.; Criel, B.; Bhojani, U.; Marchal, B.; Van Belle, S.; Chenge, F.; Hoeree, T.; Pirard, M.; Van Damme, W.; Kegels, G. The health system dynamics framework: The introduction of an analytical model for health system analysis and its application to two case-studies. Health Cult. Soc. 2012, 2, 1–21. [Google Scholar] [CrossRef]
- Anderson, R. Thematic Content Analysis (TCA). Descriptive Presentation of Qualitative Data. Ph.D. Thesis, Institute of Transpersonal Psychology, Palo Alto, CA, USA, 2007; pp. 1–4. [Google Scholar]
- Kabwama, S.N.; Kiwanuka, S.N.; Mapatano, M.A.; Fawole, O.I.; Seck, I.; Namale, A.; Ndejjo, R.; Kizito, S.; Monje, F.; Bosonkie, M.; et al. Private Sector Engagement in the COVID-19 Response Experiences and Lessons from the Democratic Republic of Congo, Nigeria, Senegal and Uganda. BMC Glob Health 2022, 18, 60. [Google Scholar] [CrossRef]
- World Health Organization. Maintaining the Provision and Use of Services for Maternal, Newborn, Child and Adolescent Health and Older People During the COVID-19 Pandemic: Lessons Learned From 19 Countries; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Uganda Ministry of Health. National Guidelines for Management of COVID-19; Uganda Ministry of Health: Kampala, Uganda, 2020. [Google Scholar]
- Kamulegeya, L.H.; Bwanika, J.M.; Musinguzi, D.; Bakibinga, P. Continuity of health service delivery during the COVID-19 pandemic: The role of digital health technologies in Uganda. Pan. Afr. Med. J. 2020, 35, 43. [Google Scholar] [CrossRef] [PubMed]
- Living Goods. Ensuring Communities Continue to Access Critical Health Services During the COVID-19 Pandemic. 2020. Available online: https://livinggoods.org/media/ensuring-communities-continue-to-access-critical-health-services-during-the-covid-19-pandemic/ (accessed on 1 February 2021).
- Zakumumpa, H.; Tumwine, C.; Milliam, K.; Spicer, N. Dispensing antiretrovirals during Covid-19 lockdown: Re-discovering community-based ART delivery models in Uganda. BMC Health Serv. Res. 2021, 21, 692. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Strategic Preparedness and Response Plan. 2019 Novel Corona Virus; Contract No.: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Magassouba, A.S.; Diallo, B.D.; Camara, L.M.; Sow, K.; Camara, S.; Bah, B.; Barry, A.O.; Diallo, T.H.; Camara, A.; Bangoura, A.M.; et al. Impact of the Ebola virus disease outbreak (2014–2016) on tuberculosis surveillance activities by Guinea’s National Tuberculosis Control Program: A time series analysis. BMC Pub. Health. 2020, 20, 1200. [Google Scholar] [CrossRef]
- Gomez, H.M.; Mejia Arbelaez, C.; Ocampo Cañas, J.A. A qualitative study of the experiences of pregnant women in accessing healthcare services during the Zika virus epidemic in Villavicencio, Colombia, 2015. Int. J. Gyn. Obs. 2020, 148, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Delamou, A.; El Ayadi, A.M.; Sidibe, S.; Delvaux, T.; Camara, B.S.; Sandouno, S.D.; Beavogui, A.H.; Rutherford, G.W.; Okumura, J.; Zhang, W.H.; et al. Effect of Ebola virus disease on maternal and child health services in Guinea: A retrospective observational cohort study. Lancet Glob. Health 2017, 5, e448–e457. [Google Scholar] [CrossRef]
- World Health Organisation. The Standard Operating Procedures for Coordinating Public Health Event Preparedness and Response in the WHO African Region (“the SOPs”); WHO Regional Office for Africa: Brazzaville, Congo, 2014. [Google Scholar]
- Oppenheim, B.; Gallivan, M.; Madhav, N.K.; Brown, N.; Serhiyenko, V.; Wolfe, N.D.; Ayscue, P. Assessing global preparedness for the next pandemic: Development and application of an epidemic preparedness index. BMJ Glob. Health 2019, 4, e001157. [Google Scholar] [CrossRef]
- Kruk, M.E.; Ling, E.J.; Bitton, A.; Cammett, M.; Cavanaugh, K.; Chopra, M.; El-Jardali, F.; Macauley, R.J.; Muraguri, M.K.; Konuma, S.; et al. Building resilient health systems: A proposal for a resilience index. BMJ 2017, 357, j2323. [Google Scholar] [CrossRef]
- World Health Organization. Joint External Evaluation Tool: International Health Regulations (2005); World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Cameron, E.; Nuzzo, J.; Bell, J.; Nalabandian, M.; O’Brien, J.; League, A.; Ravi, S.; Meyer, D.; Snyder, M.; Mullen, L.; et al. Global Health Security Index; Nuclear Threat Initiative: Washington, DC, USA, 2019. [Google Scholar]
- Ballard, M.; Olsen, H.E.; Millear, A.; Yang, J.; Whidden, C.; Yembrick, A.; Thakura, D.; Nuwasiima, A.; Christiansen, M.; Ressler, D.J.; et al. Continuity of community-based healthcare provision during COVID-19: A multicountry interrupted time series analysis. BMJ Open 2022, 12, e052407. [Google Scholar] [CrossRef]
- Cambiano, V.; Johnson, C.C.; Hatzold, K.; Terris-Prestholt, F.; Maheswaran, H.; Thirumurthy, H.; Figueroa, C.; Cowan, F.M.; Sibanda, E.L.; Ncube, G.; et al. The impact and cost-effectiveness of community-based HIV self-testing in sub-Saharan Africa: A health economic and modelling analysis. J. Int. AIDS Soc. 2019, 22, e25243. [Google Scholar] [CrossRef]
- Bailey, L.E.; Siberry, G.K.; Agaba, P.; Douglas, M.; Clinkscales, J.R.; Godfrey, C. The impact of COVID-19 on multi-month dispensing (MMD) policies for antiretroviral therapy (ART) and MMD uptake in 21 PEPFAR-supported countries: A multi-country analysis. J. Int. AIDS Soc. 2021, 24, e25794. [Google Scholar] [CrossRef]
- Hoffman, R.M.; Moyo, C.; Balakasi, K.T.; Siwale, Z.; Hubbard, J.; Bardon, A.; Fox, M.P.; Kakwesa, G.; Kalua, T.; Nyasa-Haambokoma, M.; et al. Multimonth dispensing of up to 6 months of antiretroviral therapy in Malawi and Zambia (INTERVAL): A cluster-randomised, non-blinded, non-inferiority trial. Lancet Glob. Health 2021, 9, e628–e638. [Google Scholar] [CrossRef]
- Bemelmans, M.; Baert, S.; Goemaere, E.; Wilkinson, L.; Vandendyck, M.; van Cutsem, G.; Silva, C.; Perry, S.; Szumilin, E.; Gerstenhaber, R.; et al. Community-supported models of care for people on HIV treatment in sub-S aharan Africa. Trop. Med. Int Health 2014, 19, 968–977. [Google Scholar] [CrossRef] [PubMed]
- Hoffer-Hawlik, M.A.; Moran, A.E.; Burka, D.; Kaur, P.; Cai, J.; Frieden, T.R.; Gupta, R. Leveraging Telemedicine for Chronic Disease Management in Low- and Middle-Income Countries During COVID. Glob. Heart 2020, 15, 63. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kabwama, S.N.; Wanyenze, R.K.; Kiwanuka, S.N.; Namale, A.; Ndejjo, R.; Monje, F.; Wang, W.; Lazenby, S.; Kizito, S.; Troeger, C.; et al. Interventions for Maintenance of Essential Health Service Delivery during the COVID-19 Response in Uganda, between March 2020 and April 2021. Int. J. Environ. Res. Public Health 2022, 19, 12522. https://doi.org/10.3390/ijerph191912522
Kabwama SN, Wanyenze RK, Kiwanuka SN, Namale A, Ndejjo R, Monje F, Wang W, Lazenby S, Kizito S, Troeger C, et al. Interventions for Maintenance of Essential Health Service Delivery during the COVID-19 Response in Uganda, between March 2020 and April 2021. International Journal of Environmental Research and Public Health. 2022; 19(19):12522. https://doi.org/10.3390/ijerph191912522
Chicago/Turabian StyleKabwama, Steven Ndugwa, Rhoda K. Wanyenze, Suzanne N. Kiwanuka, Alice Namale, Rawlance Ndejjo, Fred Monje, William Wang, Siobhan Lazenby, Susan Kizito, Christopher Troeger, and et al. 2022. "Interventions for Maintenance of Essential Health Service Delivery during the COVID-19 Response in Uganda, between March 2020 and April 2021" International Journal of Environmental Research and Public Health 19, no. 19: 12522. https://doi.org/10.3390/ijerph191912522