
Mental Health of COVID-19 Patients—A Cross-Sectional Survey in Saudi Arabia

 ,
,  , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Data Analysis
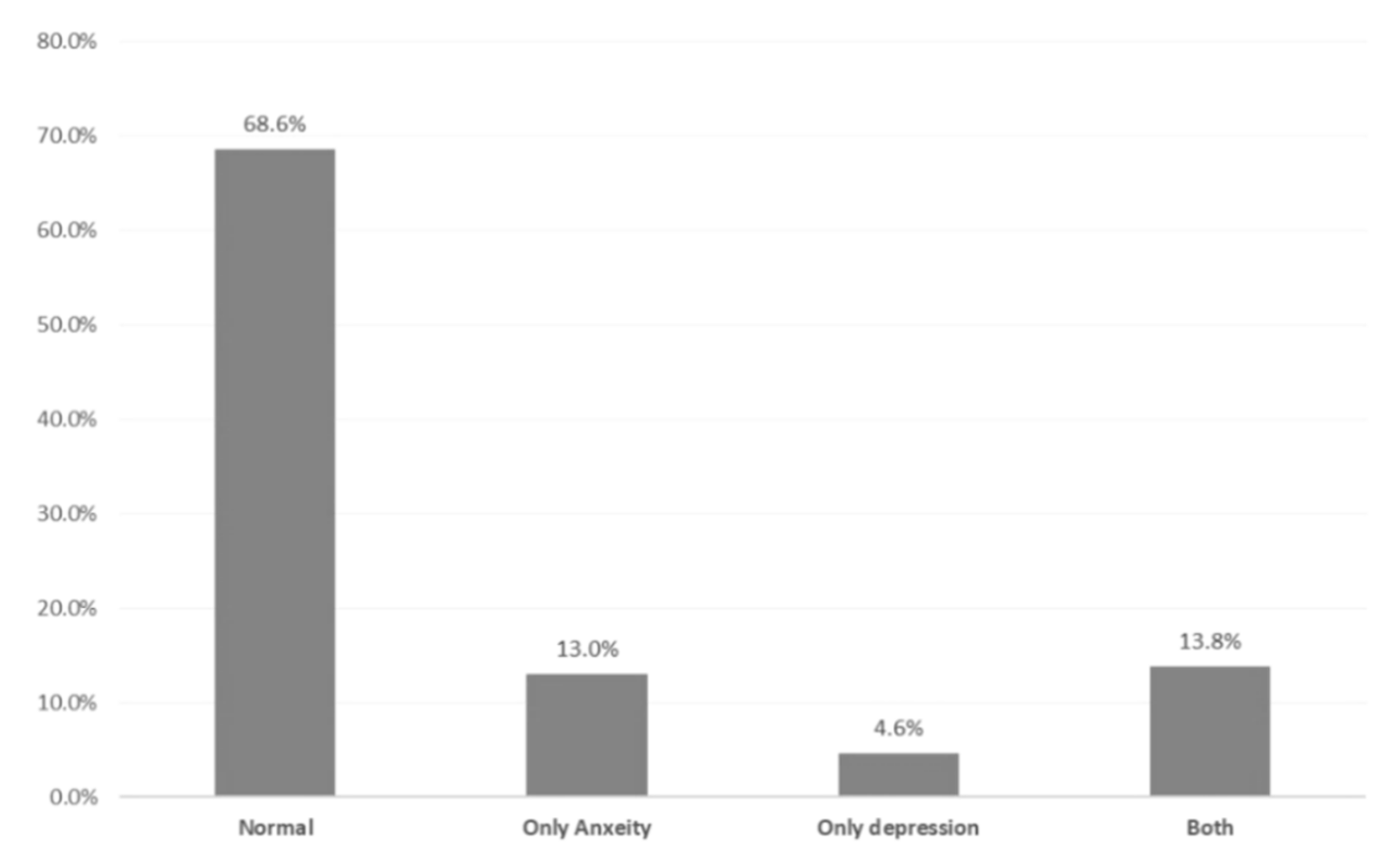
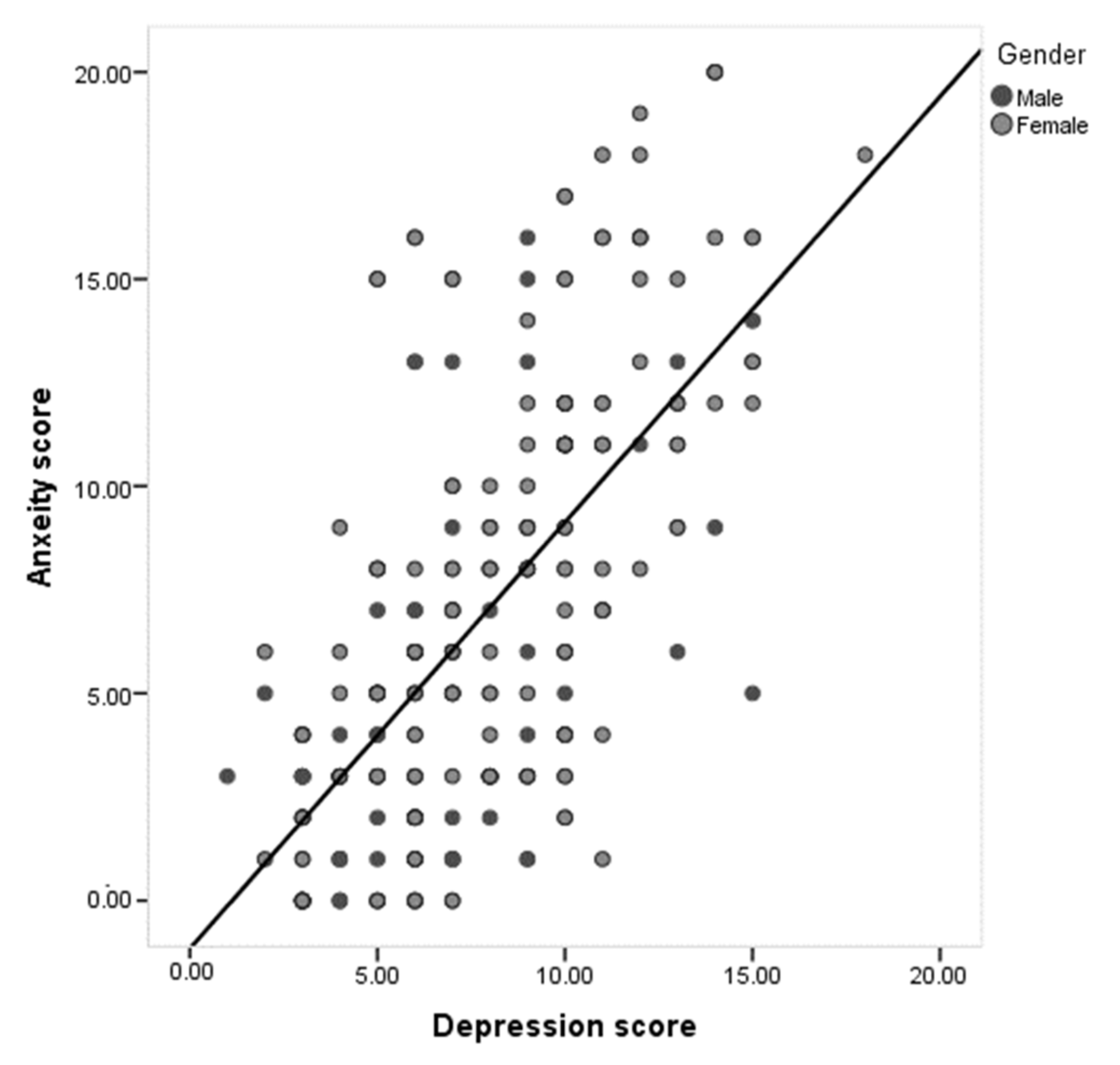
3. Results
4. Discussion
5. Conclusions
6. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heymann, D.L. Data sharing and outbreaks: Best practice exemplified. Lancet 2020, 395, 469–470. [Google Scholar] [CrossRef]
- Vara, V. Coronavirus Outbreak: The Countries Affected. 2020. Available online: https://www.pharmaceutical-technology.com/features/coronavirusoutbreak-the-countries-affected/ (accessed on 16 January 2021).
- World Health Organization. Mental Health and Psychosocial Considerations during the COVID-19 Outbreak; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- WHO. Coronavirus Disease (COVID-19) Situation Report—46, 2020b. 2019. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200306-sitrep-46-COVID-19.pdf?sfvrsn=96b04adf_2 (accessed on 16 January 2021).
- Ebrahim, S.H.; Ahmed, Q.A.; Gozzer, E.; Schlagenhauf, P.; Memish, Z.A. Covid-19 and community mitigation strategies in a pandemic. BMJ 2020, 368. [Google Scholar] [CrossRef]
- Zhou, X.; Snoswell, C.L.; Harding, L.E.; Bambling, M.; Edirippulige, S.; Bai, X.; Smith, A.C. The role of telehealth in reducing the mental health burden from COVID-19. Telemed. J. E Health 2020, 26, 377–379. [Google Scholar] [CrossRef] [PubMed]
- Li, L.Z.; Wang, S. Prevalence and predictors of general psychiatric disorders and loneliness during COVID-19 in the United Kingdom. Psychiatry Res. Sep. 2020, 291, 113267. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef]
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Ji, D.; Ji, Y.J.; Duan, X.Z.; Li, W.G.; Sun, Z.Q.; Song, X.A.; Meng, Y.-H.; Tang, H.-M.; Chu, F.; Niu, X.-X.; et al. Prevalence of psychological symptoms among Ebola survivors and healthcare workers during the 2014–2015 Ebola outbreak in Sierra Leone: A cross-sectional study. Oncotarget 2017, 8, 12784–12791. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Fang, Y.; Guan, Z.; Fan, B.; Kong, J.; Yao, Z.; Liu, X.; Fuller, C.J.; Susser, E.; Lu, J.; et al. The psychological impact of the SARS epidemic on hospital employees in China: Exposure, risk perception, and altruistic acceptance of risk. Canadian journal of psychiatry. Rev. Can. Psychiatry 2009, 54, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, D.; Rai, M. Social isolation in Covid-19: The impact of loneliness. Int. J. Soc. Psychiatry 2020, 66, 525–527. [Google Scholar] [CrossRef] [PubMed]
- Hua, Y.; Chena, Y.; Zhenga, Y.; Youa, C.; Tanb, J.; Hub, L.; Zhanga, Z.; Dinga, L. Factors related to mental health of inpatients with COVID-19 in Wuhan, China. Brain Behav. Immun. 2020, 89, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Jiawen, D.; Fangwen, Z.; Wenteng, H.; Zachary, S.; Chi, Y.W.; Oswin, C.; Emma, H.; Kang, Z.Q. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: A meta-analysis. Ann. N. Y. Acad. Sci. 2020. [Google Scholar] [CrossRef]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef]
- Kong, X.; Zheng, K.; Tang, M.; Kong, F.; Zhou, J.; Diao, L.; Wu, S.; Jiao, P.; Su, T.; Dong, Y. Prevalence and factors associated with depression and anxiety of hospitalized patients with COVID-19. MedRxiv 2020. [Google Scholar] [CrossRef]
- Polikandrioti, M.; Goudevenos, J.; Michalis, L.K.; Koutelekos, J.; Kyristi, H.; Tzialas, D.; Elisaf, M. Factors associated with depression and anxiety of hospitalized patients with heart failure. Hell. J. Cardiol. 2015, 56, 26–35. [Google Scholar] [PubMed]
- DiMatteo, M.R.; Lepper, H.S.; Croghan, T.W. Depression is a risk factor for noncompliance with medical treatment: Meta-analysis of the effects of anxiety and depression on patient adherence. Arch. Intern. Med. 2000, 160, 2101–2107. [Google Scholar] [CrossRef]
- Shoar, S.; Naderan, M.; Aghajani, M.; Sahimi-Izadian, E.; Hosseini-Araghi, N.; Khorgami, Z. Prevalence and Determinants of Depression and Anxiety Symptoms in Surgical Patients. Oman Med. J. 2016, 31, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Galea, S.; Merchant, R.M.; Lurie, N. The Mental Health Consequences of COVID-19 and Physical Distancing: The Need for Prevention and Early Intervention. JAMA Intern. Med. 2020, 180, 817. [Google Scholar] [CrossRef] [PubMed]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547. [Google Scholar] [CrossRef]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611. [Google Scholar] [CrossRef]
- Sommer, I.E.; Bakker, P.R. What can psychiatrists learn from SARS and MERS outbreaks? Lancet Psychiatry 2020, 7, 565. [Google Scholar] [CrossRef]
- Malasi, T.H.; Mirza, I.A.; El-Islam, M.F. Validation of the Hospital Anxiety and Depression Scale in Arab patients. Acta Psychiatr. Scand. 1991, 84, 323–326. [Google Scholar] [CrossRef] [PubMed]
- El Rufaie, O.E.; Absood, G.H.; Abou-Saleh, M.T. Retesting the validity of the Arabic version of the hospital anxiety and depression (HAD) scale in primary health care. Soc. Psychiatry Psychiatr. Epidemiol. 1995, 30, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China Summary of a Report of 72,314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.Y.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.Y.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemicamong the general population in China. Brain Behav. Immun. 2020, 17, 1729. [Google Scholar] [CrossRef]
- Aghagoli, G.; Marin, B.G.; Katchur, N.J.; Chaves-Sell, F.; Asaad, W.F.; Murphy, S.A. Neurological Involvement in COVID-19 and Potential Mechanisms: A Review. Neurocrit. Care 2020. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Personal Data | No | % | |
|---|---|---|---|
| Gender | Male | 100 | 38.3% |
| Female | 161 | 61.7% | |
| Age in years | <25 years | 45 | 17.2% |
| 25–34 | 85 | 32.6% | |
| 35–44 | 79 | 30.3% | |
| 45–54 | 42 | 16.1% | |
| 55+ | 10 | 3.8% | |
| Nationality | Saudi | 220 | 84.3% |
| Non-Saudi | 41 | 15.7% | |
| Educational level | Below secondary | 37 | 14.2% |
| Secondary | 59 | 22.6% | |
| University/more | 165 | 63.2% | |
| Work | Not working | 98 | 37.5% |
| Governmental sector | 82 | 31.4% | |
| Private sector | 66 | 25.3% | |
| Military sector | 15 | 5.7% | |
| Monthly income | <5000 SR | 120 | 46.0% |
| 5000–10,000 | 54 | 20.7% | |
| 10,000–20,000 | 71 | 27.2% | |
| >20,000 SR | 16 | 6.1% | |
| Marital status | Single | 82 | 31.4% |
| Married | 167 | 64.0% | |
| Divorced/widow | 12 | 4.6% | |
| Children | No children | 110 | 42.1% |
| 1–2 | 44 | 16.9% | |
| 3–5 | 75 | 28.7% | |
| 6+ | 32 | 12.3% | |
| Risk Factors with COVID-19 | No | % | |
|---|---|---|---|
| Pregnant | Yes | 8 | 7.4% |
| No | 100 | 92.6% | |
| Smoking | Nonsmoker | 189 | 72.4% |
| Ex-smoker | 34 | 13.0% | |
| Current smoker | 38 | 14.6% | |
| Chronic health conditions | None | 201 | 77.0% |
| D.M. | 19 | 7.3% | |
| HTN | 23 | 8.8% | |
| Allergic/autoimmune diseases | 27 | 10.3% | |
| Chronic cardiac conditions | 6 | 2.3% | |
| Psychological conditions | 6 | 2.3% | |
| Renal conditions | 4 | 1.5% | |
| Hypothyroidism | 3 | 1.1% | |
| Was abroad within the last three months | Yes | 8 | 3.1% |
| No | 253 | 96.9% | |
| Contact with a confirmed COVID-19 case | Yes | 121 | 46.4% |
| No | 140 | 53.6% | |
| Days in Hospital | 1–7 | 17 | 8.9% |
| 8–14 | 63 | 33.0% | |
| 15–21 | 33 | 17.3% | |
| 22+ | 78 | 40.8% | |
| Anxiety Items | No | % | |
|---|---|---|---|
| I feel tense or wound up. | Not at all | 102 | 39.1% |
| From time to time, occasionally | 83 | 31.8% | |
| A lot of the time | 41 | 15.7% | |
| Most of the time | 35 | 13.4% | |
| I get a sort of frightened feeling as if something awful is about to happen | Not at all | 126 | 48.8% |
| A little, but it does not worry me | 84 | 32.6% | |
| Yes, but not too badly | 32 | 12.4% | |
| Very definitely and quite badly | 16 | 6.2% | |
| Worrying thoughts go through my mind | Only occasionally | 137 | 52.5% |
| From time to time, but not too often | 55 | 21.1% | |
| A lot of the time | 39 | 14.9% | |
| A great deal of the time | 30 | 11.5% | |
| I can sit at ease and feel relaxed | Definitely | 90 | 34.5% |
| Usually | 71 | 27.2% | |
| Not Often | 79 | 30.3% | |
| Not at all | 21 | 8.0% | |
| I get a sort of frightened feeling like butterflies in the stomach | Not at all | 126 | 48.3% |
| Occasionally | 89 | 34.1% | |
| Quite Often | 16 | 6.1% | |
| Very Often | 30 | 11.5% | |
| I feel restless if I have to be on the move | Not at all | 46 | 17.6% |
| Not very much | 114 | 43.7% | |
| Quite a lot | 45 | 17.2% | |
| Very much indeed | 56 | 21.5% | |
| I get sudden feelings of panic | Not at all | 136 | 52.1% |
| Not very often | 64 | 24.5% | |
| Quite often | 43 | 16.5% | |
| Very often indeed | 18 | 6.9% | |
| Anxiety level | Normal (0–7) | 157 | 60.2% |
| Borderline (8–10) | 34 | 13.0% | |
| Abnormal (11–21) | 70 | 26.8% | |
| Depression Items | |||
| I still enjoy the things I used to enjoy | Definitely as much | 18 | 6.9% |
| Not quite so much | 93 | 35.6% | |
| Only a little | 34 | 13.0% | |
| Hardly at all | 116 | 44.4% | |
| I can laugh and see the funny side of things | As much as I always could | 186 | 71.3% |
| Not quite so much now | 53 | 20.3% | |
| Definitely not so much now | 16 | 6.1% | |
| Not at all | 6 | 2.3% | |
| I feel cheerful | Most of the time | 69 | 26.4% |
| Sometimes | 100 | 38.3% | |
| Not often | 68 | 26.1% | |
| Not at all | 24 | 9.2% | |
| I feel as if I am slowed down | Not at all | 125 | 47.9% |
| Sometimes | 80 | 30.7% | |
| Very often | 25 | 9.6% | |
| Nearly all the time | 31 | 11.9% | |
| I have lost interest in my appearance | I take just as much care as ever | 110 | 42.1% |
| I may not take quite as much care | 51 | 19.5% | |
| I don’t take as much care as I should | 88 | 33.7% | |
| Definitely | 12 | 4.6% | |
| I look forward with enjoyment to things | As much as I ever did | 114 | 43.7% |
| Rather less than I used to | 52 | 19.9% | |
| Definitely less than I used to | 78 | 29.9% | |
| Hardly at all | 17 | 6.5% | |
| I can enjoy a good book or radio or T.V. program | Often | 92 | 35.2% |
| Sometimes | 37 | 14.2% | |
| Not often | 85 | 32.6% | |
| Very seldom | 47 | 18.0% | |
| Depression | Normal | 135 | 51.7% |
| Borderline | 78 | 29.9% | |
| Abnormal | 48 | 18.4% | |
| Factors | Anxiety | p-Value | Depression | p-Value | |||
|---|---|---|---|---|---|---|---|
| No | % | No | % | ||||
| Gender | Male | 14 | 14.0% | 0.001 * | 9 | 9.0% | 0.002 * |
| Female | 56 | 34.8% | 39 | 24.2% | |||
| Age in years | <25 years | 12 | 26.7% | 0.027 * | 7 | 15.6% | 0.374 |
| 25–34 | 33 | 38.8% | 19 | 22.4% | |||
| 35–44 | 17 | 21.5% | 15 | 19.0% | |||
| 45–54 | 6 | 14.3% | 4 | 9.5% | |||
| 55+ | 2 | 20.0% | 3 | 30.0% | |||
| Nationality | Saudi | 66 | 30.0% | 0.007 * | 43 | 19.5% | 0.265 |
| Non-Saudi | 4 | 9.8% | 5 | 12.2% | |||
| Educational level | Below secondary | 8 | 21.6% | 0.071 | 9 | 24.3% | 0.003 * |
| Secondary | 10 | 16.9% | 2 | 3.4% | |||
| University/more | 52 | 31.5% | 37 | 22.4% | |||
| Health care worker | Yes | 19 | 42.2% | 0.010 * | 12 | 26.7% | 0.115 |
| No | 51 | 23.6% | 36 | 16.7% | |||
| Marital status | Single | 28 | 34.1% | 0.193 | 16 | 19.5% | 0.342 |
| Married | 39 | 23.4% | 28 | 16.8% | |||
| Divorced/widow | 3 | 25.0% | 4 | 33.3% | |||
| Children | No children | 39 | 35.5% | 0.048 * | 23 | 20.9% | 0.288 |
| 1–2 | 7 | 15.9% | 11 | 25.0% | |||
| 3–5 | 17 | 22.7% | 10 | 13.3% | |||
| 6+ | 7 | 21.9% | 4 | 12.5% | |||
| Pregnant | Yes | 4 | 50.0% | 0.190 | 2 | 25.0% | 0.879 |
| No | 28 | 28.0% | 23 | 23.0% | |||
| Smoking | Nonsmoker | 53 | 28.0% | 0.430 | 35 | 18.5% | 0.426 |
| Ex-smoker | 6 | 17.6% | 4 | 11.8% | |||
| Current smoker | 11 | 28.9% | 9 | 23.7% | |||
| Chronic health conditions | No | 56 | 27.9% | 0.487 | 35 | 17.4% | 0.455 |
| Yes | 14 | 23.3% | 13 | 21.7% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alamri, H.S.; Mousa, W.F.; Algarni, A.; Megahid, S.F.; Al Bshabshe, A.; Alshehri, N.N.; Bashah, D.M.; Alosaimi, R.; Alshehri, A.; Alsamghan, A.; et al. Mental Health of COVID-19 Patients—A Cross-Sectional Survey in Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 4758. https://doi.org/10.3390/ijerph18094758
Alamri HS, Mousa WF, Algarni A, Megahid SF, Al Bshabshe A, Alshehri NN, Bashah DM, Alosaimi R, Alshehri A, Alsamghan A, et al. Mental Health of COVID-19 Patients—A Cross-Sectional Survey in Saudi Arabia. International Journal of Environmental Research and Public Health. 2021; 18(9):4758. https://doi.org/10.3390/ijerph18094758
Chicago/Turabian StyleAlamri, Hasan Saeed, Wesam F. Mousa, Abdullah Algarni, Shehata F. Megahid, Ali Al Bshabshe, Nada N. Alshehri, Dalal M. Bashah, Roaa Alosaimi, Ahlam Alshehri, Awad Alsamghan, and et al. 2021. "Mental Health of COVID-19 Patients—A Cross-Sectional Survey in Saudi Arabia" International Journal of Environmental Research and Public Health 18, no. 9: 4758. https://doi.org/10.3390/ijerph18094758