Association of Vitamin C Treatment with Clinical Outcomes for COVID-19 Patients: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Coding
2.4. Risk of Bias Assessment and Publication Bias
2.5. Statistical Analysis
3. Results
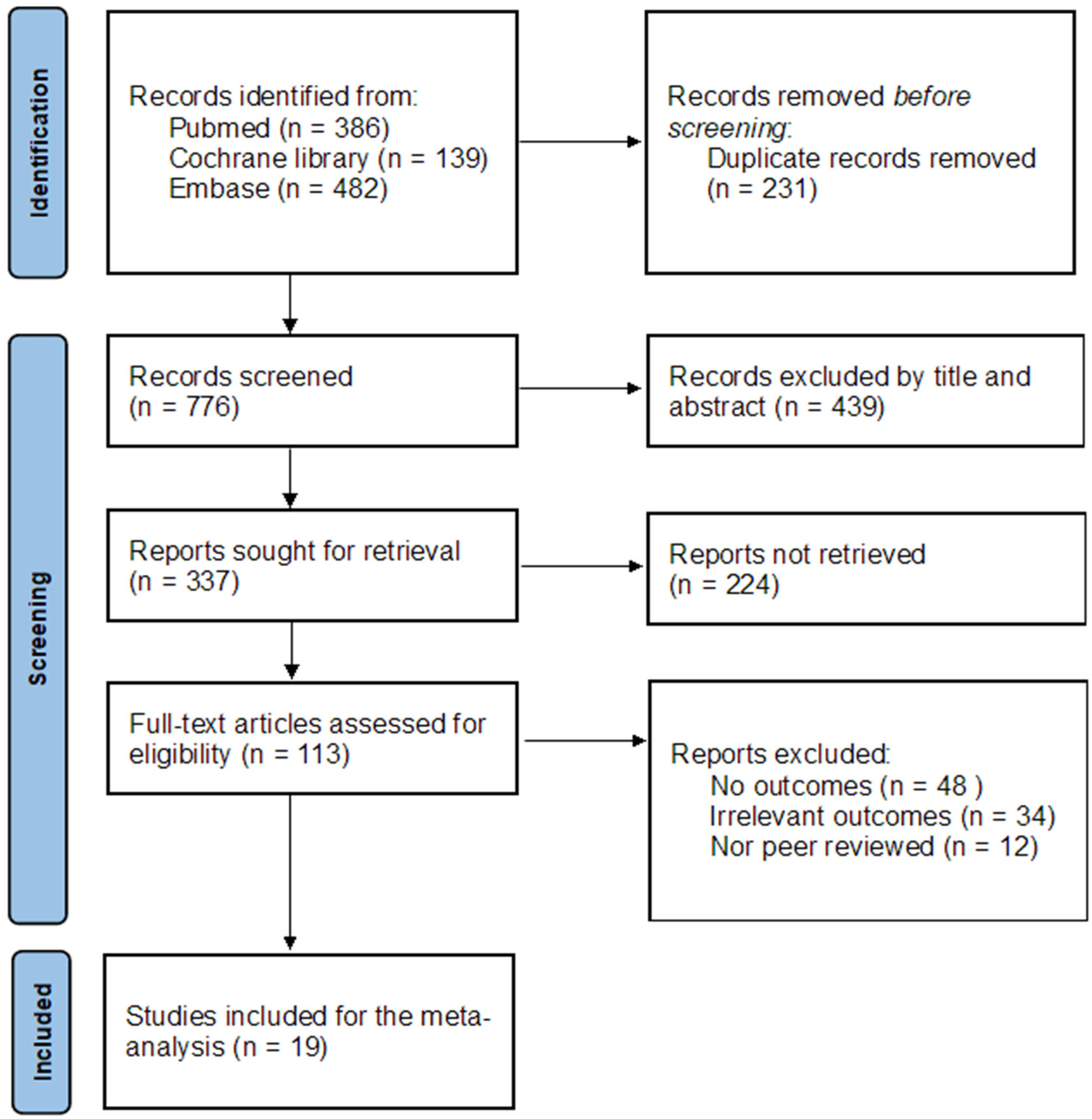
3.1. Study Selection
3.2. Study Characteristics of Included Studies
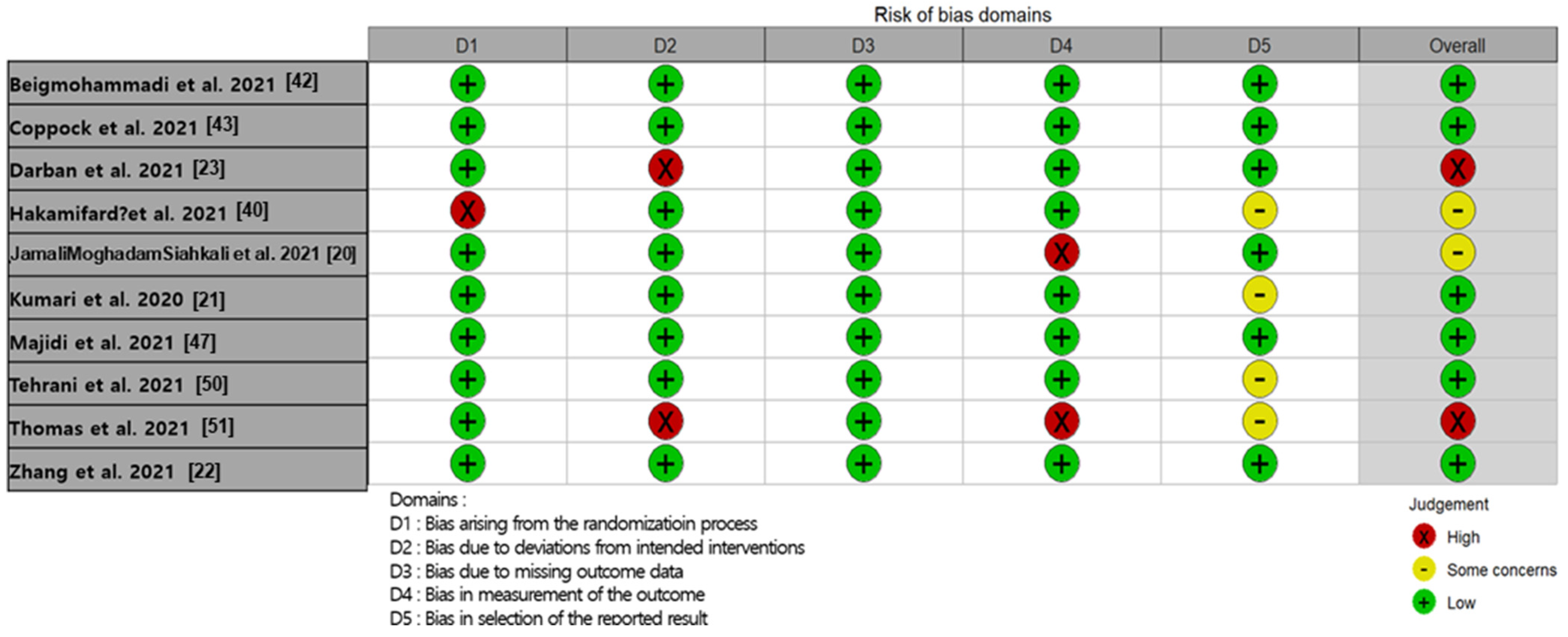
3.3. Risk of Bias Assessment in Individual Studies
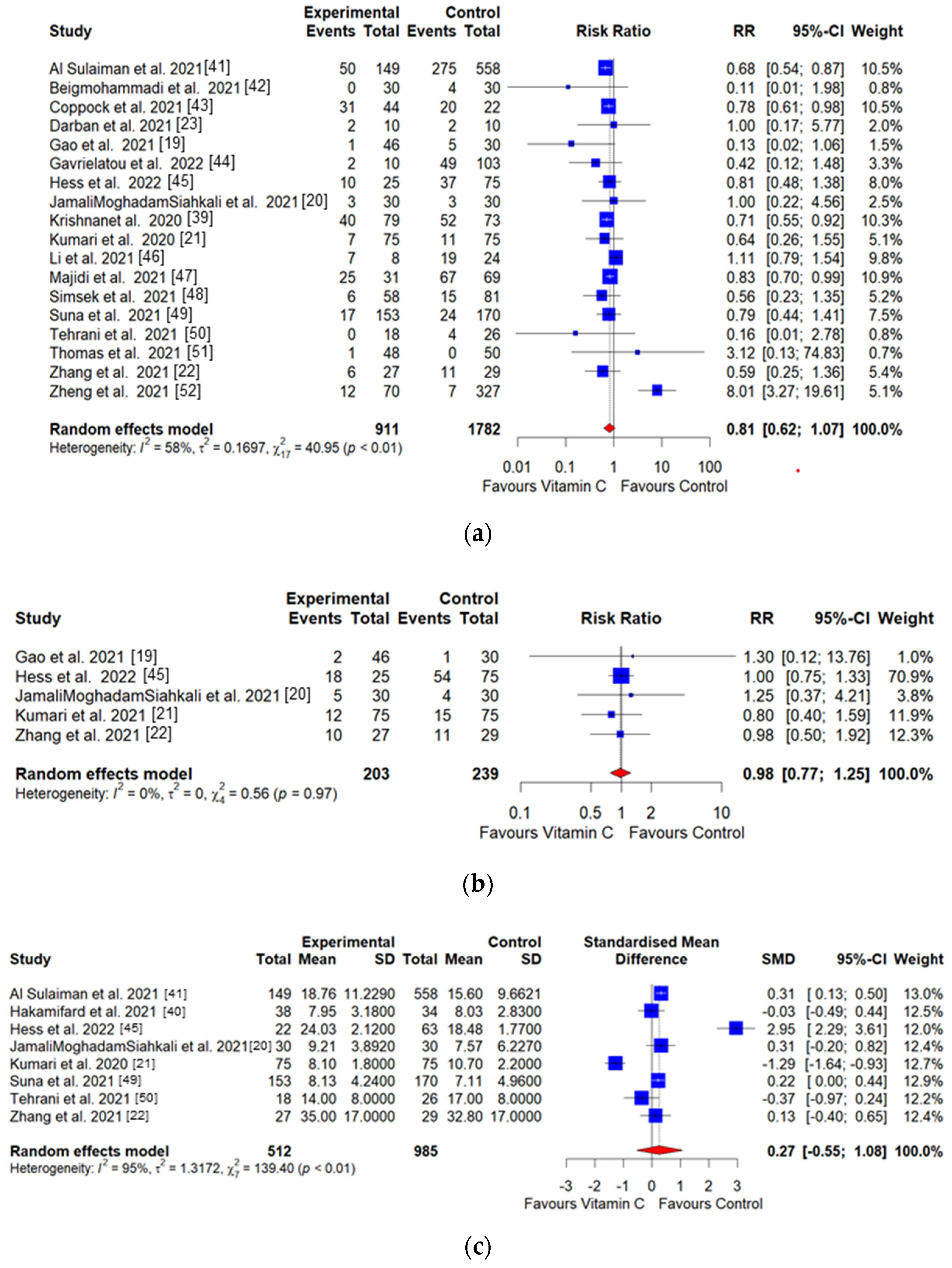
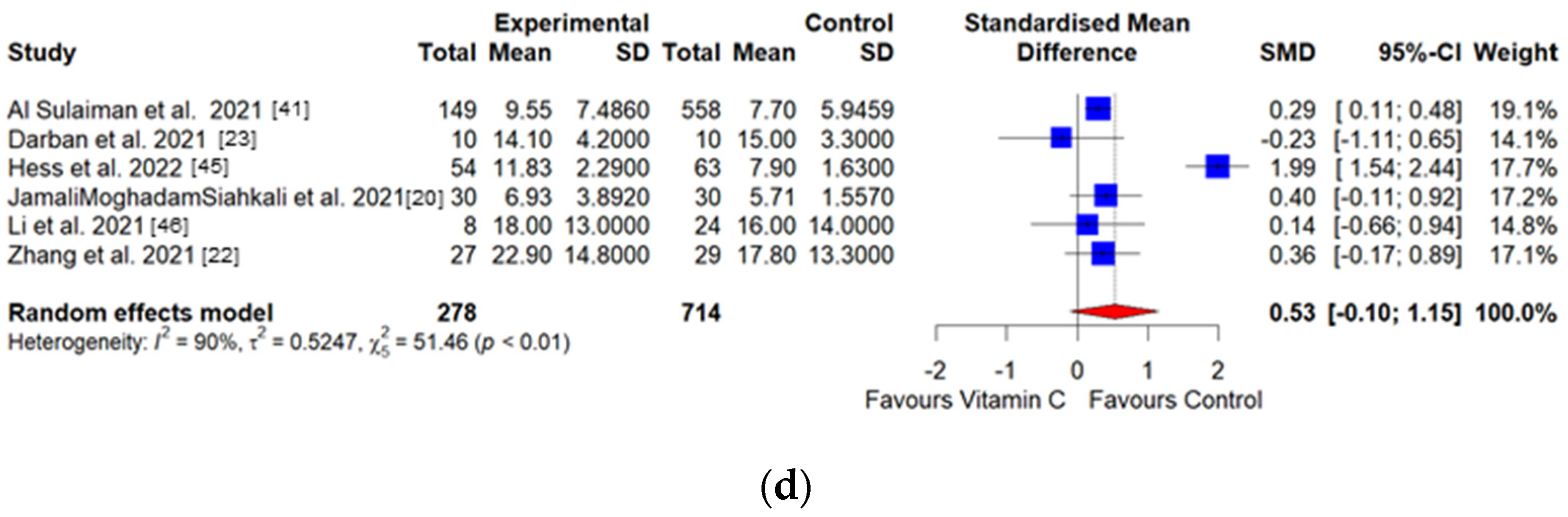
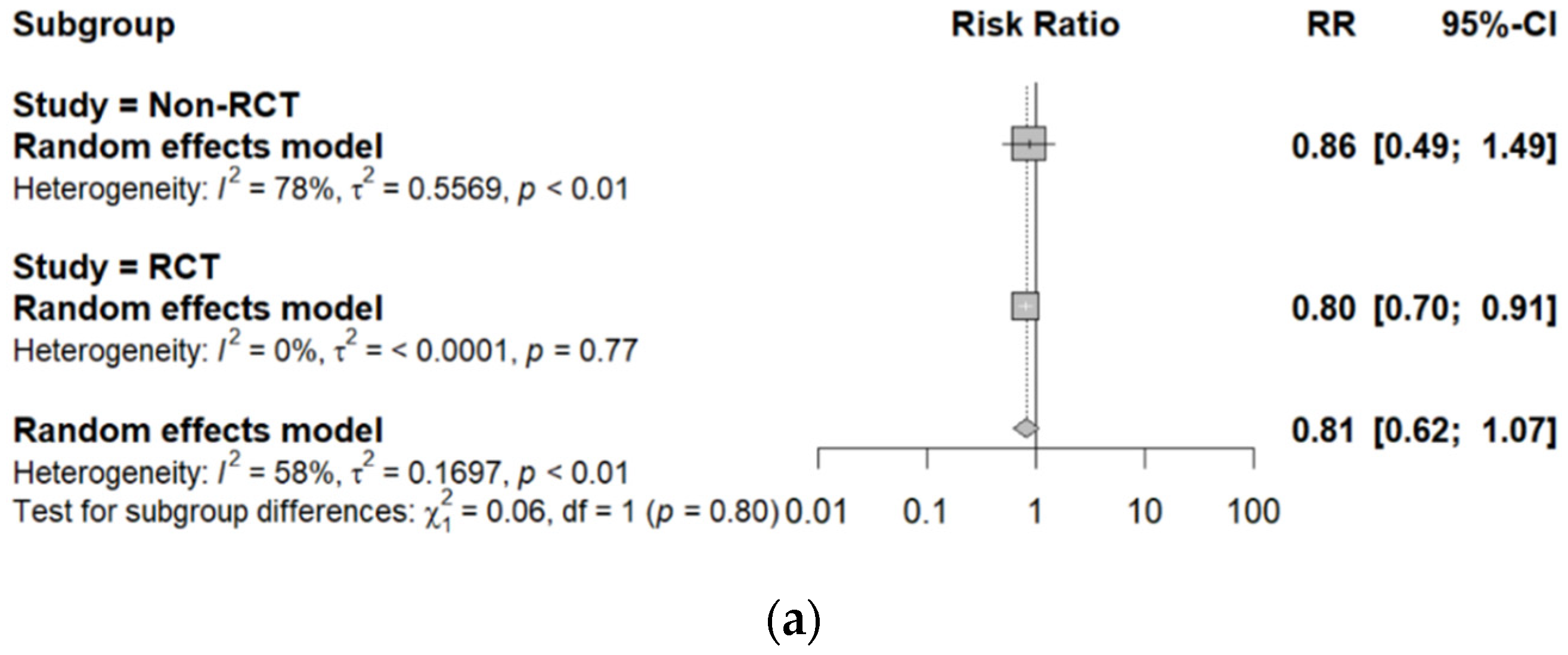
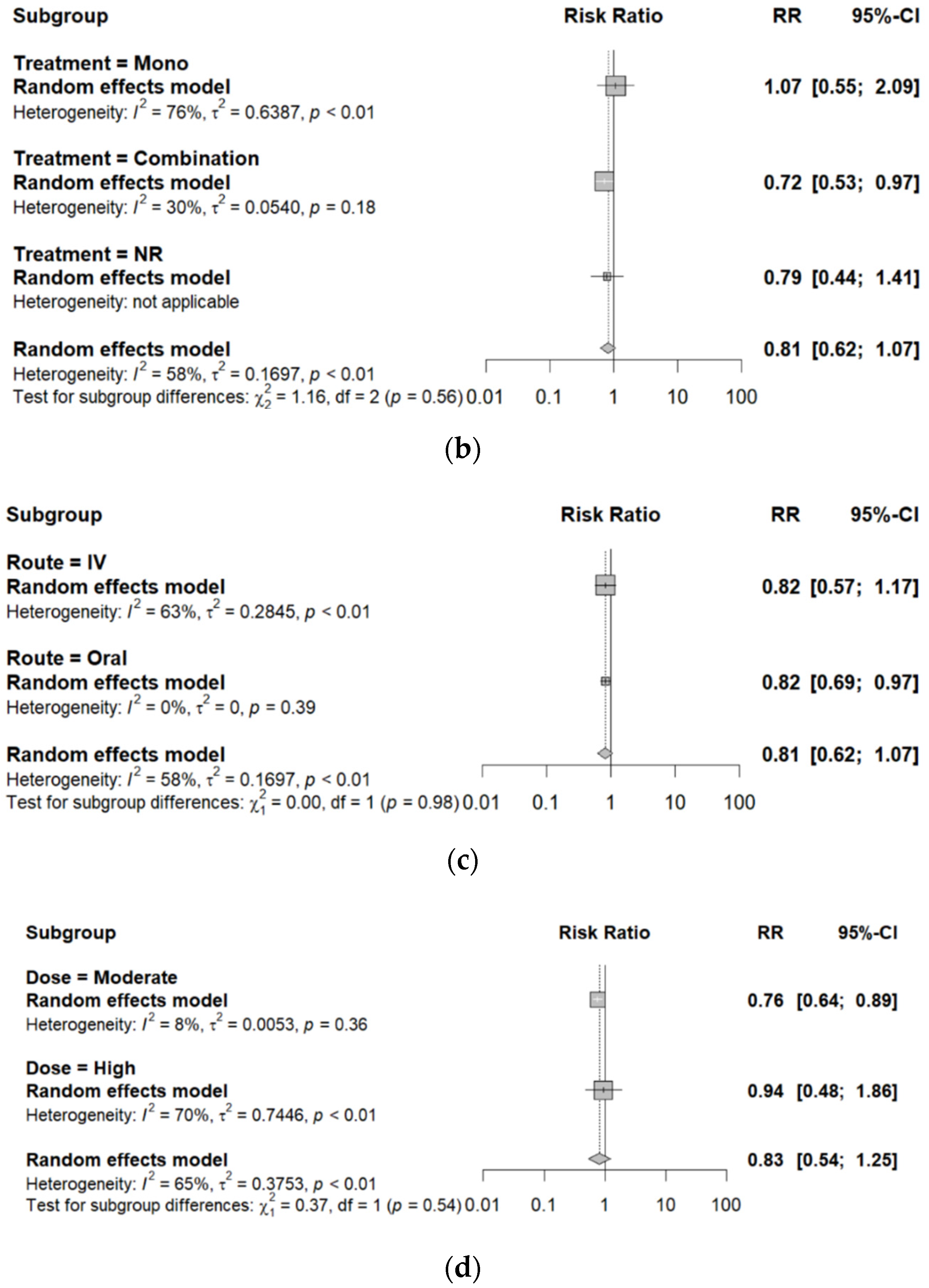
3.4. Result of Meta-Analysis
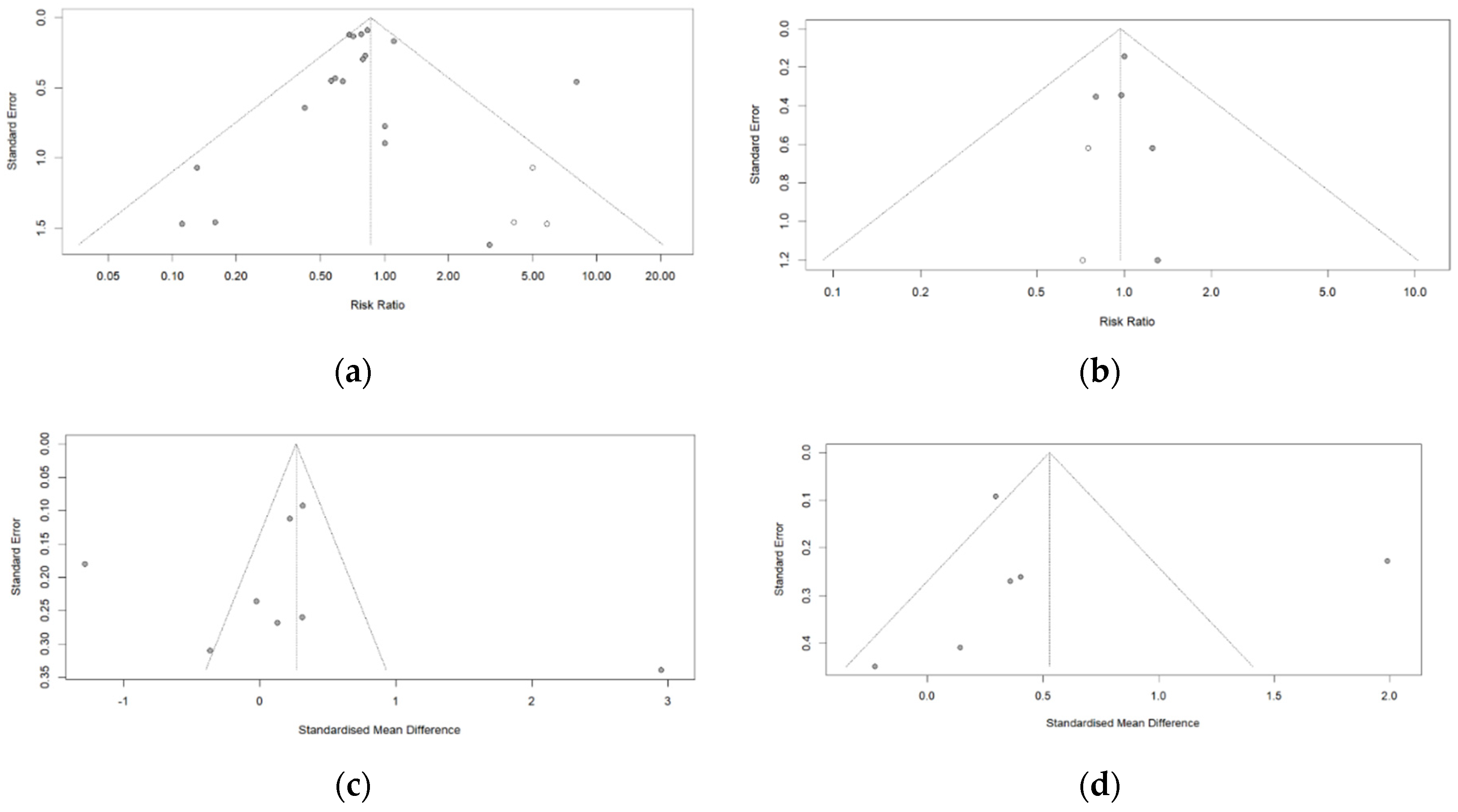
3.5. Publication Bias
4. Discussions
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 30 May 2022).
- Ghinai, I.; McPherson, T.D.; Hunter, J.C.; Kirking, H.L.; Christiansen, D.; Joshi, K.; Rubin, R.; Morales-Estrada, S.; Black, S.R.; Pacilli, M.; et al. First known person-to-person transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in the USA. Lancet 2020, 395, 1137–1144. [Google Scholar] [CrossRef]
- Chan, J.F.; Yuan, S.; Kok, K.H.; To, K.K.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.Y.; Poon, R.W.S.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, O.P.; Bhandari, P.; Raut, A.; Kacimi, S.E.O.; Huy, N.T. Coronavirus disease (COVID-19): Comprehensive review of clinical presentation. Front. Public Health 2021, 8, 582932. [Google Scholar] [CrossRef]
- Azkur, A.K.; Akdis, M.; Azkur, D.; Sokolowska, M.; van de Veen, W.; Brüggen, M.; O’Mahony, L.; Gao, Y.; Nadeau, K.; Akdis, C.A. Immune response to SARS-CoV-2 and mechanisms of immunopathological changes in COVID-19. Allergy 2020, 75, 1564–1581. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Huang, S.; Yin, L. The cytokine storm and COVID-19. J. Med. Virol. 2021, 93, 250–256. [Google Scholar] [CrossRef]
- Wang, L.S.; Wang, Y.R.; Ye, D.W.; Liu, Q.Q. A review of the 2019 novel coronavirus (COVID-19) based on current evidence. Int. J. Antimicrob. Agents 2020, 55, 105948. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.C.; Park, Y.K.; Kim, B.O.; Park, D. Risk factors for disease progression in COVID-19 patients. BMC Infect. Dis. 2020, 20, 445. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel Coronavirus–infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Kakodkar, P.; Kaka, N.; Baig, M.N. A comprehensive literature review on the clinical presentation, and management of the pandemic Coronavirus disease 2019 (COVID-19). Cureus 2020, 12, e7560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villlamizar-Pena, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef] [PubMed]
- Lordan, R.; Rando, H.M.; Greene, C.S. Dietary Supplements and Nutraceuticals under Investigation for COVID-19 Prevention and Treatment. Am. Soc. Microbiol. 2021, 6, e00122-21. [Google Scholar] [CrossRef] [PubMed]
- Lordan, R. Dietary supplements and nutraceuticals market growth during the coronavirus pandemic—Implications for consumers and regulatory oversight. PharmaNutrition 2021, 18, 100282. [Google Scholar] [CrossRef] [PubMed]
- Padayatty, S.J.; Katz, A.; Wang, Y.; Eck, P.; Kwon, O.; Lee, J.; Chen, S.; Corpe, C.; Dutta, A.; Dutta, S.K.; et al. Vitamin C as an antioxidant: Evaluation of its role in disease prevention. J. Am. Coll. Nutr. 2003, 22, 18–35. [Google Scholar] [CrossRef] [PubMed]
- Molina, N.; Morandi, A.C.; Bolin, A.P.; Otton, R. Comparative effect of fucoxanthin and vitamin C on oxidative and functional parameters of human lymphocytes. Int. Immunopharmacol. 2014, 22, 41–50. [Google Scholar] [CrossRef]
- Choi, W.S. The effect of vitamin C overdose on blood. KAACR 2017, 7, 117–129. [Google Scholar] [CrossRef]
- Ohno, S.; Ohno, Y.; Suzuki, N.; Soma, G.; Inoue, M. High-dose vitamin C (ascorbic acid) therapy in the treatment of patients with advanced cancer. Anticancer Res. 2009, 29, 809–815. [Google Scholar]
- LeBlanc, J.G. Implementation of nurse-driven HIV screening targeting key populations in emergency departments: A multilevel analysis from the DICI-VIH trial. Vitamin C. An Update on Current Uses and Functions: BoD–Books on Demand. Worldviews Evid.-Based Nurs. 2019, 16, 444–453. [Google Scholar] [CrossRef]
- Gao, D.; Xu, M.; Wang, G.; Lv, J.; Ma, X.; Guo, Y.; Zhang, D.; Yang, H.; Jiang, W.; Deng, F.; et al. efficiency and safety of high-dose vitamin C in patients with COVID-19: A retrospective cohort study. Aging 2021, 13, 7020–7034. [Google Scholar] [CrossRef]
- Jamali Moghadam Siahkali, S.; Zarezade, B.; Koolaji, S.; Seyed Alinaghi, S.; Zendehdel, A.; Tabarestani, M.; Sekhavati Moghadam, E.; Abbasian, L.; Dehghan Manshadi, S.A.; Salehi, M.; et al. Safety and effectiveness of high dose vitamin C in patients with COVID-19: A randomized open label clinical trial. Eur. J. Med. Res. 2021, 26, 20. [Google Scholar] [CrossRef]
- Kumari, P.; Dembra, S.; Dembra, P.; Bhawna, F.; Gul, A.; Ali, B.; Sohail, H.; Kumar, B.; Memon, M.K.; Rizwan, A. The role of vitamin C as adjuvant therapy in COVID-19. Cureus 2020, 12, e11779. [Google Scholar] [CrossRef]
- Zhang, J.; Rao, X.; Li, Y.; Zhu, Y.; Liu, F.; Guo, G.; Luo, G.; Meng, Z.; De Backer, D.; Xiang, H.; et al. Pilot trial of high-dose vitamin C in critically ill COVID-19 patients. Ann. Intensive Care 2021, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Darban, M.; Malek, F.; Memarian, M.; Gohari, A.; Kiani, A.; Emadi, A.; Lavvaf, S.; Bagheri, B. Efficacy of high dose vitamin C, melatonin and zinc in Iranian patients with acute respiratory syndrome due to Coronavirus infection: A pilot randomized trial. J. Cell. Mol. Anesth. 2021, 6, 164–167. [Google Scholar]
- Rawat, D.; Roy, A.; Maitra, S.; Gulati, A.; Khanna, P.; Baidya, D.K. Vitamin C and COVID-19 treatment: A systematic review and meta-analysis of randomized controlled trials. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102324. [Google Scholar] [CrossRef]
- Huang, L.; Wang, L.; Tan, J.; Liu, H.; Ni, Y. High-dose vitamin C intravenous infusion in the treatment of patients with COVID-19: A protocol for systematic review and meta-analysis. Medicine 2021, 100, e25876. [Google Scholar] [CrossRef]
- NCT02735707; Randomized, Embedded, Multifactorial Adaptive Platform Trial for Community—Acquired Pneumonia (REMAP-CAP). University Medical Center Utrecht: Utrecht, The Netherlands, 2016. Available online: https://clinicaltrials.gov/ct2/show/NCT02735707 (accessed on 13 April 2016).
- NCT03680274; Lessening Organ Dysfunction with VITamin C. University of Sherbrooke: Sherbrooke, QC, Canada, 2022.
- NCT04344184; Early Infusion of Vitamin C for Treatment of Novel COVID-19 Acute Lung Injury (EVICT-CORONA-ALI). Virginia Commonwealth University: Richmond, VA, USA, 2020.
- NCT04342728; Coronavirus 2019 (COVID-19)—Using Ascorbic Acid and Zinc Supplementation (COVIDAtoZ). U.S. National Library of Medicine: Bethesda, MD, USA, 2020.
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Luo, D.; Weng, H.; Zeng, X.; Lin, L.; Chu, H.; Tong, T. Optimally estimating the sample standard deviation from the five-number summary. Res. Synth. Methods 2020, 25, 1429. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Br. Med. J. 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Sutton, A.J.; Duval, S.J.; Tweedie, R.L.; Abrams, K.R.; Jones, D.R. Empirical assessment of effect of publication bias on meta analyses. BMJ 2000, 320, 1574–1577. [Google Scholar] [CrossRef]
- Melsen, W.G.; Bootsma, M.C.; Rovers, M.M.; Bonten, M.J. The effects of clinical and statistical heterogeneity on the predictive values of results from meta-analyses. Clin. Microbiol. Infect. 2014, 20, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, S.; Patel, K.; Desai, R.; Sule, A.; Paik, P.; Miller, A.; Barclay, A.; Cassella, A.; Lucaj, J.; Royster, Y.; et al. Clinical comorbidities, characteristics, and outcomes of mechanically ventilated patients in the State of Michigan with SARS-CoV-2 pneumonia. J. Clin. Anesth. 2020, 67, 110005. [Google Scholar] [CrossRef]
- Hakamifard, A.; Soltani, R.; Maghsoudi, A.; Rismanbaf, A.; Aalinezhad, M.; Tarrahi, M.J.; Mashayekhbakhsh, S.; Dolatshahi, K. The effect of vitamin E and vitamin C in patients with COVID-19 pneumonia; A randomized controlled clinical trial. Immunopathol. Persa 2021, 8, e08. [Google Scholar]
- Al Sulaiman, K.; Aljuhani, O.; Saleh, K.B.; Badreldin, H.A.; Al Harthi, A.; Alenazi, M.; Alharbi, A.; Algarni, R.; Al Harbi, S.; Alhammad, A.M.; et al. Ascorbic acid as an adjunctive therapy in critically ill patients with COVID-19: A propensity score matched study. Sci. Rep. 2021, 11, 17648. [Google Scholar] [CrossRef]
- Beigmohammadi, M.T.; Bitarafan, S.; Hoseindokht, A.; Abdollahi, A.; Amoozadeh, L.; Soltani, D. The effect of supplementation with vitamins A, B, C, D, and E on disease severity and inflammatory responses in patients with COVID-19: A randomized clinical trial. Trials 2021, 22, 802. [Google Scholar] [CrossRef]
- Coppock, D.; Violet, P.C.; Vasquez, G.; Belden, K.; Foster, M.; Mullin, B.; Magee, D.; Mikell, I.; Shah, L.; Powers, V.; et al. Pharmacologic Ascorbic Acid as Early Therapy for Hospitalized Patients with COVID-19: A Randomized Clinical Trial. Life 2022, 12, 453. [Google Scholar] [CrossRef]
- Gavrielatou, E.; Xourgia, E.; Xixi, N.A.; Mantelou, A.G.; Ischaki, E.; Kanavou, A.; Zervakis, D.; Routsi, C.; Kotanidou, A.; Siempos, I.I. Effect of Vitamin C on Clinical Outcomes of Critically Ill Patients with COVID-19: An Observational Study and Subsequent Meta-Analysis. Front. Med. 2022, 9, 814587. [Google Scholar] [CrossRef]
- Hess, A.L.; Halalau, A.; Dokter, J.J.; Paydawy, T.S.; Karabon, P.; Bastani, A.; Baker, R.E.; Balla, A.K.; Galens, S.A. High-doseintravenous vitamin C decreases rates of mechanical ventilation and cardiac arrest in severe COVID-19. Intern. Emerg. Med. 2022, 17, 1759–1768. [Google Scholar] [CrossRef]
- Li, M.; Ching, T.H.; Hipple, C.; Lopez, R.; Sahibzada, A.; Rahman, H. Use of intravenous vitamin c in critically ill patients with COVID-19 infection. J. Pharm. Pract. 2021, 8, 8971900211015052. [Google Scholar] [CrossRef]
- Majidi, N.; Rabbani, F.; Gholami, S.; Gholamalizadeh, M.; BourBour, F.; Rastgoo, S.; Hajipour, A.; Shadnoosh, M.; Akbari, M.E.; Bahar, B.; et al. The Effect of Vitamin C on Pathological Parameters and Survival Duration of Critically Ill Coronavirus Disease 2019 Patients: A Randomized Clinical Trial. Front. Immunol. 2021, 12, 717816. [Google Scholar] [CrossRef] [PubMed]
- Simsek, F.; Senkal, S.; Yazici, E.; Yonca, H.; Tahmaz, I.; Kara, U.; Sir, E.; Eksert, S.; Ince, M.E.; Ozdemirkan, I.; et al. Effects of high dose vitamin C administration in COVID-19 patients. Ann. Med. Res. 2021, 28, 1699–1703. [Google Scholar] [CrossRef]
- Suna, K.; Melahat, U.Ş.; Murat, Y.; Figen, Ö.E.; Ayperi, Ö. Effect of high-dose intravenous vitamin C on prognosis in patients with SARS-CoV-2 pneumonia. Med. Clin. 2021, 5, 356–360. [Google Scholar]
- Tehrani, S.; Yadegarynia, D.; Abrishami, A.; Moradi, H.; Gharaei, B.; Rauofi, M.; Nejad, F.M.; Sali, S.; Khabiri, N.; Abolghasemi, S. An investigation into the effects of intravenous vitamin C on pulmonary CT findings and clinical outcomes of patients with COVID-19 pneumonia a randomized clinical trial. Urol. J. 2021, 11, 6863. [Google Scholar]
- Thomas, S.; Patel, D.; Bittel, B.; Wolski, K.; Wang, Q.; Kumar, A.; Il’Giovine, Z.J.; Mehra, R.; McWilliams, C.; Nissen, S.E.; et al. Effect of high-dose zinc and ascorbic acid supplementation vs. usual care on symptom length and reduction among ambulatory patients with SARS-CoV-2 infection: The COVID A to Z randomized clinical trial. JAMA Netw. Open 2021, 4, e210369. [Google Scholar] [CrossRef]
- Zheng, S.; Chen, Q.; Jiang, H.; Guo, C.; Luo, J.; Li, S.; Wang, H.; Li, H.; Zheng, X.; Weng, Z. No significant benefit of moderate-dose vitamin C on severe COVID-19 cases. Open Med. 2021, 16, 1403–1414. [Google Scholar] [CrossRef]
- Wang, Y.; Lin, H.; Lin, B.W.; Lin, J.D. Effects of different ascorbic acid doses on the mortality of critically ill patients: A meta-analysis. Ann. Intensive Care 2019, 9, 58. [Google Scholar] [CrossRef] [Green Version]
- Gavriilaki, E.; Anyfanti, P.; Gavriilaki, M.; Lazaridis, A.; Douma, S.; Gkaliagkousi, E. Endothelial dysfunction in COVID-19: Lessons learned from coronaviruses. Curr. Hypertens. Rep. 2020, 22, 63. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Carr, A.C.; Maggini, S. Vitamin C and immune function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- May, C.N.; Bellomo, R.; Lankadeva, Y.R. Therapeutic potential of megadose vitamin C to reverse organ dysfunction in sepsis and COVID-19. Br. J. Pharmacol. 2021, 178, 3864–3868. [Google Scholar] [CrossRef]
- Abobaker, A.; Alzwi, A.; Alraied, A.H.A. Overview of the possible role of vitamin C in management of COVID-19. Pharmacol. Rep. 2020, 72, 1517–1528. [Google Scholar] [CrossRef]
- Sato, R.; Hasegawa, D.; Prasitlumkum, N.; Miki, U.; Kazuki, N.; Kunihiko, T.; Nasu, M.; Dugar, S. Effect of IV high-dose vitamin C on mortality in patients sepsis: A systematic review and meta-analysis of randomized controlled trials. Crit. Care Med. 2021, 49, 2121–2130. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Li, H.; Wen, Y.; Zhang, M. Adjuvant administration of vitamin C improves mortality of patients with sepsis and septic shock: A systems review and meta-analysis. Open J. Intern. Med. 2018, 8, 146–159. [Google Scholar] [CrossRef]
- Zhang, M.; Jativa, D.F. Vitamin C supplementation in the critically ill: A systematic review and meta-analysis. SAGE Open Med. 2018, 6, 2050312118807615. [Google Scholar] [CrossRef] [Green Version]
- Langlois, P.L.; Manzanares, W.; Adhikari, N.K.; Lamontagne, F.; Stoppe, C.; Hill, A.; Heyland, D.K. Vitamin C administration to the critically ill: A systematic review and meta-analysis. J. Parenter. Enter. Nutr. 2019, 43, 335–346. [Google Scholar] [CrossRef]
- Putzu, A.; Daems, A.M.; Lopez-Delgado, J.C.; Giordano, V.F.; Landoni, G. The effect of vitamin C on clinical outcome in critically ill patients: A systematic review with meta-analysis of randomized controlled trials. Crit. Care Med. 2019, 47, 774–783. [Google Scholar] [CrossRef]
- Tang, Y.; Liu, J.; Zhang, D.; Xu, Z.; Ji, J.; Wen, C. Cytokine storm in COVID-19: The current evidence and treatment strategies. Front. Immunol. 2020, 11, 1708. [Google Scholar] [CrossRef]
- Costela-Ruiz, V.J.; Illescas-Montes, R.; Puerta-Puerta, J.M.; Ruiz, C.; Melguizo-Rodríguez, L. SARS-CoV-2 infection: The role of cytokines in COVID-19 disease. Cytokine Growth Factor Rev. 2020, 54, 62–75. [Google Scholar] [CrossRef]
- Xia, G.; Fan, D.; He, Y.; Zhu, Y.; Zheng, Q. High-dose intravenous vitamin C attenuates hyper inflammation in severe coronavirus disease 2019. Nutrition 2021, 91, 111405. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Update on Omicron. 2021. Available online: https://www.who.int/news/item/28-11-2021-update-on-omicron (accessed on 29 December 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | First Author (Year) | Study Design | Sample Size I/C | Dosage of Vitamin C | Treatment Duration | Treatment Method (Route) | Outcomes Measurement |
|---|---|---|---|---|---|---|---|
| 1 | Al Sulaiman (2021) [41] | Retro | 149/558 | 1 g/day | NR | Mono therapy (IV) | All-cause mortality, Hospitalization duration, ICU stay |
| 2 | Beigmohammadi (2021) [42] | RCT | 30/30 | 2 g/day | 7 days | Combination with vitamin A, D, B1, B2, nicotinamide, pyridoxine, sodium pantothenate (IV) | All-cause mortality |
| 3 | Coppock (2021) [43] | RCT | 44/22 | 0.3–0.9 g/kg | 5 days | Mono therapy (IV) | All-cause mortality |
| 4 | Darban (2021) [23] | RCT | 10/ 10 | 8 g/day | 10 days | Combination with melatonin and zinc (IV) | All-cause mortality, ICU stay |
| 5 | Gao (2021) [19] | Retro | 46/30 | 12 g/day (1st day), 6 g/day (2nd–5th day) | 5 days | Combination with antibiotics, corticosteroids, and other antivirals (IV) | All-cause mortality, Ventilation incidence |
| 6 | Gavrielatou (2022) [44] | Retro | 10/103 | –1.5 g/day | 7 days | Combination with thiamine (IV) | All-cause mortality |
| 7 | Hakamifard (2021) [40] | RCT | 38/34 | 1 g/day | NR | Combination with vitamin E (Oral) | Hospitalization day |
| 8 | Hess (2022) [45] | Retro | 25/75 | 18 g/day | 7 days | Mono therapy (IV) | All-cause mortality, ICU stay, Ventilation incidence |
| 9 | JamaliMoghadamSiahkali (2021) [20] | RCT | 30/30 | 6 g/day | 5 days | Combination with lopinavir and ritonavir (IV) | All-cause mortality, Hospitalization duration, ICU stay, Ventilation incidence |
| 10 | Krishnan (2020) [39] | Retro | 79/73 | NR | NR | Combination with steroids (NR) | All-cause mortality |
| 11 | Kumari (2020) [21] | RCT | 75/75 | 50 mg/kg/day | NR | Combination with dexamethasone and prophylactic antibiotics (IV) | All-cause mortality, Hospitalization duration, Ventilation incidence |
| 12 | Li (2021) [46] | Retro | 8/24 | 9 g/day | 4 days | Combination with hydrocortisone and thiamine (IV) | All-cause mortality, ICU stay |
| 13 | Majidi (2021) [47] | RCT | 31/69 | 500 mg/day | 14 days | Mono therapy (Oral) | All-cause mortality |
| 14 | Simsek (2021) [48] | Retro | 58/81 | 25 g/day | 7 days | Combination with hydroxychloroquine, azithromycin, favipiravir (Oral) | All-cause mortality |
| 15 | Suna (2021) [49] | Retro | 153/170 | 2 g/day | NR | NR (IV) | All-cause mortality, Hospitalization duration |
| 16 | Tehrani (2021) [50] | RCT | 18/26 | 8 g/day | 5 days | Mono therapy (IV) | All-cause mortality, Hospitalization duration |
| 17 | Thomas (2021) [51] | RCT | 48/50 | 8 g/day | 10 days | Mono therapy (IV) | All-cause mortality |
| 18 | Zhang et al. (2021) [22] | RCT | 27/29 | 24 g/day | 7 days | Combination with antiviral(glucocorticoid) (IV) | All-cause mortality, Hospitalization duration, ICU stay, Ventilation incidence |
| 19 | Zheng (2021) [52] | Retro | 70/327 | 4 g/ day | NR | Mono therapy (IV) | All-cause mortality |
| Quality Criteria | Selection | Comparability | Exposure | Total | |||||
|---|---|---|---|---|---|---|---|---|---|
| Is Case Definition Adequate? | Representativeness of the Cases | Selection of controls | Definition of controls | Comparability on Basis of Design or Analysis | Ascertainment of Exposure | Same Method of Ascertainment for Cases and Controls | Nonresponse Rate | ||
| Al Sulaiman (2021) [41] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 7 | |
| Gao (2021) [19] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 8 |
| Gavrielato (2022) [44] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 7 | |
| Hess (2022) [45] | ★ | ★ | ★ | ★ | ★ | 5 | |||
| Krishnan (2020) [39] | ★ | ★ | ★ | ★ | ★ | 5 | |||
| Li (2021) [46] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 8 |
| Simsek (2021) [48] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 7 | |
| Suna (2021) [49] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 8 |
| Zheng (2021) [52] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 8 |
| Outcomes | Bias | Se. 1 Bias | Intercept | Se. Intercept | t | df 2 | p-Value |
|---|---|---|---|---|---|---|---|
| All-cause mortality | −0.10 | 0.56 | −0.21 | 0.12 | −0.17 | 16 | 0.87 |
| Ventilation incidence | 0.09 | 0.34 | −0.04 | 0.09 | 0.28 | 3 | 0.80 |
| Hospitalization duration | 0.65 | 3.80 | 0.05 | 0.63 | 0.17 | 6 | 0.87 |
| Length of ICU stay | 0.94 | 2.70 | 0.33 | 0.50 | 0.35 | 4 | 0.74 |
| Items | Added Studies | Adjusted Effect Size | 95% CI | I2 (%) | p-Value |
|---|---|---|---|---|---|
| All-cause mortality | 3 | 0.86 | 0.65–1.14 | 57.4 | 0.29 |
| Ventilation incidence | 2 | 0.97 | 0.77–1.22 | 0.0 | 0.99 |
| Hospitalization duration | 0 | 0.27 | −0.55–1.08 | 95.0 | 0.52 |
| Length of ICU stay | 0 | 0.53 | −0.10–1.15 | 90.3 | 0.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, W.Y.; Hong, J.; Ahn, S.-I.; Han, B.K.; Kim, Y.J. Association of Vitamin C Treatment with Clinical Outcomes for COVID-19 Patients: A Systematic Review and Meta-Analysis. Healthcare 2022, 10, 2456. https://doi.org/10.3390/healthcare10122456
Huang WY, Hong J, Ahn S-I, Han BK, Kim YJ. Association of Vitamin C Treatment with Clinical Outcomes for COVID-19 Patients: A Systematic Review and Meta-Analysis. Healthcare. 2022; 10(12):2456. https://doi.org/10.3390/healthcare10122456
Chicago/Turabian StyleHuang, Wen Yan, Jiyoun Hong, Sung-Il Ahn, Bok Kyung Han, and Young Jun Kim. 2022. "Association of Vitamin C Treatment with Clinical Outcomes for COVID-19 Patients: A Systematic Review and Meta-Analysis" Healthcare 10, no. 12: 2456. https://doi.org/10.3390/healthcare10122456