
Parental Hesitancy towards the Established Childhood Vaccination Programmes in the COVID-19 Era: Assessing the Drivers of a Challenging Public Health Concern

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Data Collection
Socio-Demographic Characteristics, Lifestyle Factors, and General Health Status
2.2. COVID-19 Related Variables
2.3. Assessment of Childhood Vaccine Hesitancy
2.4. Statistical Analysis
3. Results
3.1. Description of Participants
3.2. Prevalence and General Determinants of Vaccine Hesitancy
3.3. COVID-19-Related Determinants of Vaccine Hesitancy
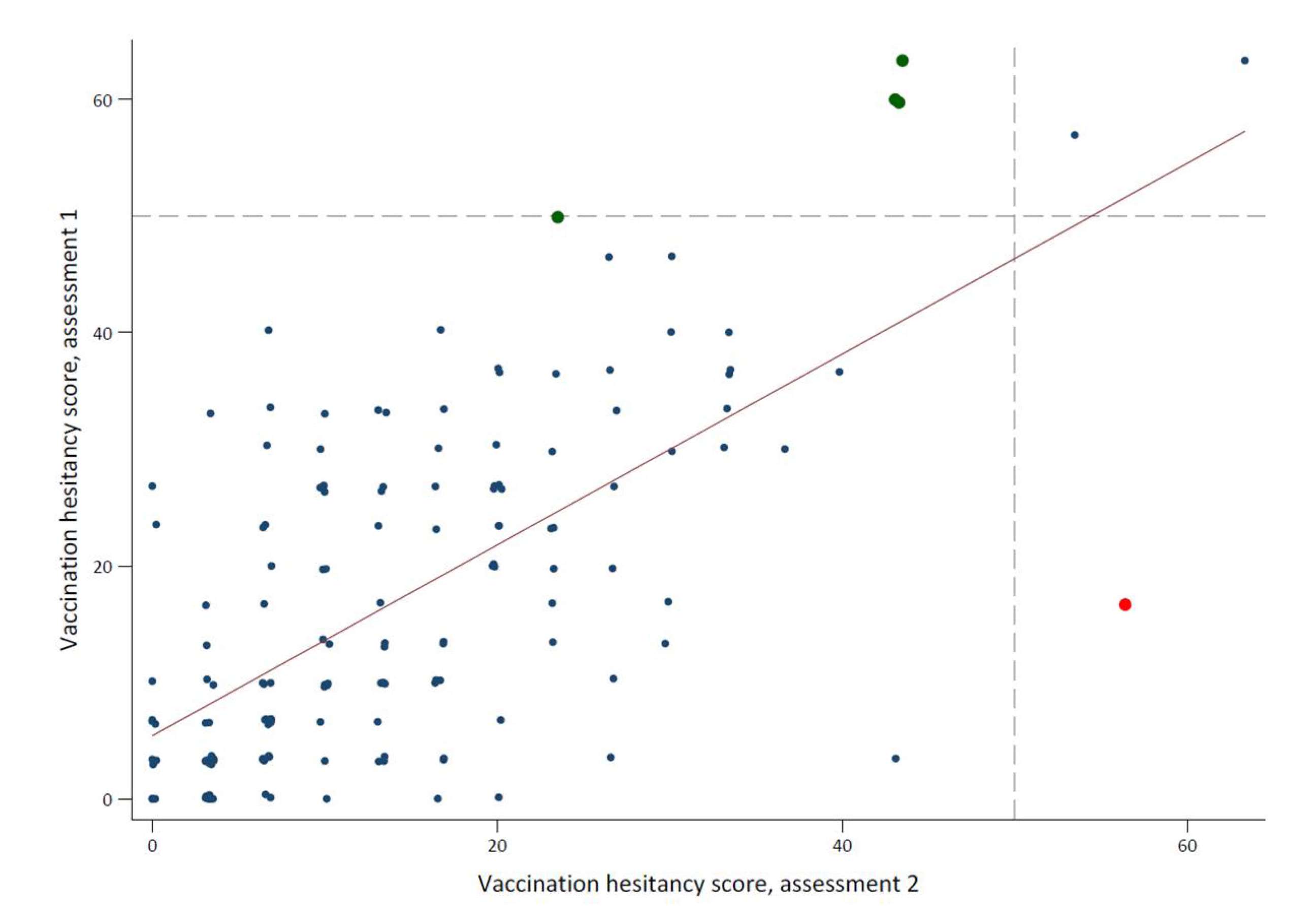
3.4. Vaccine Hesitancy in the Repeated Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Vaccines and Immunization, WHO. Available online: https://www.who.int/health-topics/vaccines-and-immunization. (accessed on 20 November 2021).
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Ten Threats to Global Health in 2019, WHO. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019. (accessed on 20 November 2021).
- Larson, H.J.; De Figueiredo, A.; Xiahong, Z.; Schulz, W.S.; Verger, P.; Johnston, I.G.; Cook, A.R.; Jones, N.S. The State of Vaccine Confidence 2016: Global Insights Through a 67-Country Survey. EBioMedicine 2016, 12, 295–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef]
- Larson, H.J.; Cooper, L.Z.; Eskola, J.; Katz, S.L.; Ratzan, S. Addressing the vaccine confidence gap. Lancet 2011, 378, 526–535. [Google Scholar] [CrossRef]
- Global Preparedness Monitoring Board. A World at Risk: Annual Report on Global Preparedness for Health Emergencies; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- COVID-19 Dashboard by the Center for Systems Science and Engineering at Johns Hopkins University. Available online: https://gisanddata.maps.arcgis.com/apps/dashboards/bda7594740fd40299423467b48e9ecf6. (accessed on 14 March 2022).
- Hellenic Statistical Authority. Available online: https://www.statistics.gr/en/home/ (accessed on 30 October 2021).
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348, Correction in Nat. Hum. Behav. 2021, 5, 960. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Muhoza, P.; Danovaro-Holliday, M.C.; Diallo, M.S.; Murphy, P.; Sodha, S.V.; Requejo, J.H.; Wallace, A.S. Routine Vaccination Coverage—Worldwide, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 1495–1500. [Google Scholar] [CrossRef]
- Temsah, M.-H.; Alhuzaimi, A.N.; Aljamaan, F.; Bahkali, F.; Al-Eyadhy, A.; Alrabiaah, A.; Alhaboob, A.; Bashiri, F.A.; Alshaer, A.; Temsah, O.; et al. Parental Attitudes and Hesitancy About COVID-19 vs. Routine Childhood Vaccinations: A National Survey. Front. Public Health 2021, 9, 2323. [Google Scholar] [CrossRef]
- Olusanya, O.A.; Bednarczyk, R.A.; Davis, R.L.; Shaban-Nejad, A. Addressing Parental Vaccine Hesitancy and Other Barriers to Childhood/Adolescent Vaccination Uptake During the Coronavirus (COVID-19) Pandemic. Front. Immunol. 2021, 12, 663074. [Google Scholar] [CrossRef]
- He, K.; Mack, W.J.; Neely, M.; Lewis, L.; Anand, V. Parental Perspectives on Immunizations: Impact of the COVID-19 Pandemic on Childhood Vaccine Hesitancy. J. Community Health 2021, 47, 39–52. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Bull. World Health Organ. 2007, 85, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Kanellopoulou, A.; Giannakopoulos, I.; Fouzas, S.; Papachatzi, E.; Nasikas, S.; Papakonstantinopoulou, A.; Dimitriou, G.; Gkentzi, D. Vaccination coverage among school children in Western Greece from 2016 to 2019. Hum. Vaccines Immunother. 2021, 17, 4535–4541. [Google Scholar] [CrossRef] [PubMed]
- Koutsonida, M.; Kanellopoulou, A.; Markozannes, G.; Gousia, S.; Doumas, M.T.; Sigounas, D.E.; Tzovaras, V.T.; Vakalis, K.; Tzoulaki, I.; Evangelou, E.; et al. Adherence to Mediterranean Diet and Cognitive Abilities in the Greek Cohort of Epirus Health Study. Nutrients 2021, 13, 3363. [Google Scholar] [CrossRef] [PubMed]
- Rontogianni, M.O.; Kanellopoulou, A.; Markozannes, G.; Bouras, E.; Derdemezis, C.; Doumas, M.T.; Sigounas, D.E.; Tzovaras, V.T.; Vakalis, K.; Panagiotakos, D.B.; et al. Prevalence and Determinants of Sex-Specific Dietary Supplement Use in a Greek Cohort. Nutrients 2021, 13, 2857. [Google Scholar] [CrossRef] [PubMed]
- Opel, D.J.; Taylor, J.A.; Zhou, C.; Catz, S.; Myaing, M.; Mangione-Smith, R. The relationship between parent attitudes about childhood vaccines survey scores and future child immunization status: A validation study. JAMA Pediatrics 2013, 167, 1065–1071. [Google Scholar] [CrossRef] [Green Version]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; et al. Strategies for Addressing Vaccine Hesitancy-A Systematic Review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [Green Version]
- WHO/UNICEF Electronic Joint Reporting Form. Available online: https://immunizationdata.who.int/ (accessed on 20 November 2021).
- Benecke, O.; Deyoung, S.E. Anti-Vaccine Decision-Making and Measles Resurgence in the United States. Glob. Pediatr. Health 2019, 6, 2333794X19862949. [Google Scholar] [CrossRef] [Green Version]
- Salmon, D.A.; Dudley, M.Z.; Glanz, J.M.; Omer, S.B. Vaccine Hesitancy: Causes, Consequences, and a Call to Action. Am. J. Prev. Med. 2015, 49 (Suppl. 4), S391–S398. [Google Scholar] [CrossRef]
- Opel, D.J.; Mangione-Smith, R.; Taylor, J.A.; Korfiatis, C.; Wiese, C.; Catz, S.; Martin, D.P. Development of a survey to identify vaccine-hesitant parents: The parent attitudes about childhood vaccines survey. Hum Vaccin. 2011, 7, 419–425. [Google Scholar] [CrossRef] [Green Version]
- Opel, D.J.; Taylor, J.A.; Mangione-Smith, R.; Solomon, C.; Zhao, C.; Catz, S.; Martin, D. Validity and reliability of a survey to identify vaccine-hesitant parents. Vaccine 2011, 29, 6598–6605. [Google Scholar] [CrossRef]
- Bianco, A.; Mascaro, V.; Zucco, R.; Pavia, M. Parent perspectives on childhood vaccination: How to deal with vaccine hesitancy and refusal? Vaccine 2019, 37, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Hamadah, R.E.; Hussain, A.N.; Alsoghayer, N.A.; Alkhenizan, Z.A.; Alajlan, H.A.; Alkhenizan, A.H. Attitude of parents towards seasonal influenza vaccination for children in Saudi Arabia. J. Fam. Med. Prim. Care 2021, 10, 904–909. [Google Scholar]
- Yufika, A.; Wagner, A.L.; Nawawi, Y.; Wahyuniati, N.; Anwar, S.; Yusri, F.; Haryanti, N.; Wijayanti, N.P.; Rizal, R.; Fitriani, D.; et al. Parents’ hesitancy towards vaccination in Indonesia: A cross-sectional study in Indonesia. Vaccine 2020, 38, 2592–2599. [Google Scholar] [CrossRef] [PubMed]
- Mohd Azizi, F.S.; Kew, Y.; Moy, F.M. Vaccine hesitancy among parents in a multi-ethnic country, Malaysia. Vaccine 2017, 35, 2955–2961. [Google Scholar] [CrossRef] [PubMed]
- Henrikson, N.B.; Anderson, M.L.; Opel, D.J.; Dunn, J.; Marcuse, E.K.; Grossman, D.C. Longitudinal Trends in Vaccine Hesitancy in a Cohort of Mothers Surveyed in Washington State, 2013–2015. Public Health Rep. 2017, 132, 451–454. [Google Scholar] [CrossRef] [Green Version]
- Marshall, S.; Moore, A.C.; Sahm, L.J.; Fleming, A. Parent Attitudes about Childhood Vaccines: Point Prevalence Survey of Vaccine Hesitancy in an Irish Population. Pharmacy 2021, 9, 188. [Google Scholar] [CrossRef]
- Strelitz, B.; Gritton, J.; Klein, E.J.; Bradford, M.C.; Follmer, K.; Zerr, D.M.; Englund, J.A.; Opel, D.J. Parental vaccine hesitancy and acceptance of seasonal influenza vaccine in the pediatric emergency department. Vaccine 2015, 33, 1802–1807. [Google Scholar] [CrossRef]
- Napolitano, F.; D'Alessandro, A.; Angelillo, I.F. Investigating Italian parents' vaccine hesitancy: A cross-sectional survey. Hum. Vaccines Immunother. 2018, 14, 1558–1565. [Google Scholar] [CrossRef] [Green Version]
- Danis, K.; Georgakopoulou, T.; Stavrou, T.; Laggas, D.; Panagiotopoulos, T. Socioeconomic factors play a more important role in childhood vaccination coverage than parental perceptions: A cross-sectional study in Greece. Vaccine 2010, 28, 1861–1869. [Google Scholar] [CrossRef]
- Aldakhil, H.; Albedah, N.; Alturaiki, N.; Alajlan, R.; Abusalih, H. Vaccine hesitancy towards childhood immunizations as a predictor of mothers' intention to vaccinate their children against COVID-19 in Saudi Arabia. J. Infect. Public Health 2021, 14, 1497–1504. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Leon, A.S.; Jacobs, D.R.; Montoye, H.J.; Sallis, J.F.; Paffenbarger, R.S. Compendium of physical activities: Classification of energy costs of human physical activities. Med. Sci. Sports Exerc. 1993, 25, 71–80. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total N = 1095 | Non-Hesitant N = 997 (91.1%) | Hesitant N = 98 (8.9%) | p-Value | |
|---|---|---|---|---|
| Women, N (%) | 715 (65.3) | 651 (65.3) | 64 (65.3) | >0.99 |
| Age (years), mean (SD) | 50.25 (9.37) | 50.33 (9.32) | 49.43 (9.90) | 0.364 |
| BMI (kg/m2), mean (SD) * | 26.25 (4.66) | 26.26 (4.67) | 26.22 (4.55) | 0.948 |
| Total METs [kcal/(kg × h)], mean (SD) ** | 21.31 (29.67) | 19.97 (26.17) | 35.64 (52.56) | 5.7 × 10−6 |
| Marital status, N (%) | ||||
| Unmarried/divorced/widowed | 155 (14.3) | 131 (13.2) | 24 (25.5) | |
| Married/in cohabitation agreement | 928 (85.7) | 858 (86.8) | 70 (74.5) | 0.001 |
| Education, N (%) | ||||
| Up to high school | 278 (25.5) | 243 (24.4) | 35 (36.8) | |
| University degree | 458 (42.0) | 409 (41.1) | 49 (51.6) | |
| Master's degree or higher | 354 (32.5) | 343 (34.5) | 11 (11.6) | 2.1 × 10−5 |
| Profession, N (%) | ||||
| Executive/scientist/artist/office | 769 (76.1) | 722 (78.1) | 47 (54.7) | |
| Providing services/seller | 99 (9.8) | 88 (9.5) | 11 (12.8) | |
| Manual labor | 142 (14.1) | 114 (12.3) | 28 (32.6) | 4.1 × 10−7 |
| Income (Euros/month), N (%) | ||||
| ≤900 | 270 (27.3) | 226 (25.0) | 44 (51.8) | |
| 901–1100 | 177 (17.9) | 167 (18.5) | 10 (11.8) | |
| 1101–1400 | 293 (29.6) | 277 (30.6) | 16 (18.8) | |
| >1400 | 249 (25.2) | 234 (25.9) | 15 (17.6) | 3.5 × 10−6 |
| Smoking status, N (%) | ||||
| Non-smokers | 414 (37.9) | 384 (38.6) | 30 (30.9) | |
| Former smokers | 256 (23.5) | 240 (24.1) | 16 (16.5) | |
| Current smokers | 421 (38.6) | 370 (37.2) | 51 (52.6) | 0.010 |
| Alcohol consumption, N (%) | ||||
| Never | 172 (15.8) | 158 (15.9) | 14 (14.3) | |
| Less than once/month | 318 (29.1) | 289 (29.1) | 29 (29.6) | |
| 1–3 times/month | 253 (23.2) | 226 (22.7) | 27 (27.6) | |
| 1–2 times/week | 234 (21.4) | 218 (21.9) | 16 (16.3) | |
| 3 or more times/week | 115 (10.5) | 103 (10.4) | 12 (12.2) | 0.617 |
| Weight change during last 6 months, N (%) | ||||
| No change | 574 (52.8) | 518 (52.3) | 56 (57.1) | |
| Lost weight | 196 (18.0) | 182 (18.4) | 14 (14.3) | |
| Gained weight | 318 (29.2) | 290 (29.3) | 28 (28.6) | 0.538 |
| Self-perceived health status, N (%) | ||||
| Moderate/bad/very bad | 152 (13.9) | 138 (13.9) | 14 (14.4) | |
| Good | 573 (52.5) | 536 (53.9) | 37 (38.1) | |
| Very good | 366 (33.5) | 320 (32.2) | 46 (47.4) | 0.006 |
| Restriction of activities during last year due to health issue, N (%) | ||||
| None | 622 (57.5) | 552 (56.1) | 70 (71.4) | |
| A little/moderately | 291 (26.9) | 274 (27.8) | 17 (17.3) | |
| Much/very much | 169 (15.6) | 158 (16.1) | 11 (11.2) | 0.013 |
| Stress symptoms during last 2 weeks, N (%) | ||||
| No days | 192 (17.5) | 173 (17.4) | 19 (19.4) | |
| Some days | 607 (55.4) | 566 (56.8) | 41 (41.8) | |
| More than half days | 144 (13.2) | 131 (13.1) | 13 (13.3) | |
| Almost every day | 152 (13.9) | 127 (12.7) | 25 (25.5) | 0.003 |
| Depressive symptoms during last 2 weeks, N (%) | ||||
| No days | 374 (34.2) | 347 (34.8) | 27 (27.6) | |
| Some days | 516 (47.1) | 479 (48.0) | 37 (37.8) | |
| More than half days | 122 (11.1) | 104 (10.4) | 18 (18.4) | |
| Almost every day | 83 (7.6) | 67 (6.7) | 16 (16.3) | 2.4 × 10−4 |
| Self-reported presence of chronic disease, N (%) | 392 (36.5) | 365 (37.2) | 27 (28.7) | 0.101 |
| Physician diagnosis of diabetes, N (%) | 79 (7.2) | 75 (7.5) | 4 (4.1) | 0.208 |
| Physician diagnosis of high cholesterol, N (%) | 417 (38.3) | 398 (40.1) | 19 (19.4) | 5.6 × 10−5 |
| Physician diagnosis of high blood pressure, N (%) | 237 (21.7) | 225 (22.6) | 12 (12.4) | 0.019 |
| Area of residence, N (%) | ||||
| Attica | 210 (19.3) | 186 (18.8) | 24 (24.5) | |
| Peloponnese | 48 (4.4) | 40 (4.0) | 8 (8.2) | |
| Islands (Aegean and Ionian, Crete) | 39 (3.6) | 34 (3.4) | 5 (5.1) | |
| Thessaly and Central Greece | 48 (4.4) | 44 (4.4) | 4 (4.1) | |
| Epirus | 612 (56.3) | 574 (58.0) | 38 (38.8) | |
| Macedonia and Thrace | 131 (12.0) | 112 (11.3) | 19 (19.4) | 0.006 |
| Minimally Adjusted Model 1 | Maximally Adjusted Model 2 | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Coronavirus existence | ||||
| Definitely not/probably not/do not know | Ref | Ref | ||
| Probably yes | 0.21 (0.09, 0.50) | 0.20 (0.05, 0.82) | ||
| Definitely yes | 0.05 (0.02, 0.12) | 2.1 × 10−13 | 0.05 (0.01, 0.19) | 7.8 × 10−7 |
| Knowledge about COVID-19 | ||||
| Poor knowledge | Ref | Ref | ||
| Moderate knowledge | 0.64 (0.31, 1.30) | 0.48 (0.18, 1.31) | ||
| Good knowledge | 0.45 (0.27, 0.75) | 0.009 | 0.49 (0.25, 0.96) | 0.089 * |
| Following COVID-19 measures of personal protection3,4 | ||||
| Never/rarely/sometimes | Ref | Ref | ||
| Frequently | 0.22 (0.10, 0.46) | 0.33 (0.11, 0.97) | ||
| Almost always/always | 0.06 (0.03, 0.11) | 7.8 × 10−16 | 0.09 (0.03, 0.22) | 2.9 × 10−7 |
| Following COVID-19 measures of public protection3,5 | ||||
| Never/rarely/sometimes | Ref | Ref | ||
| Frequently | 0.22 (0.09, 0.51) | 0.23 (0.07, 0.75) | ||
| Almost always/always | 0.06 (0.03, 0.12) | 2.8×10−14 | 0.06 (0.02, 0.17) | 1.56 × 10−7 |
| Trust in health authorities for minimizing the spread of coronavirus3 | ||||
| No trust | Ref | Ref | ||
| Little trust | 0.29 (0.15, 0.54) | 0.26 (0.11, 0.62) | ||
| Some trust | 0.14 (0.08, 0.25) | 0.12 (0.05, 0.27) | ||
| Absolute trust | 0.05 (0.01, 0.16) | 6.0×10−12 | 0.04 (0.01, 0.19) | 2.3 × 10−7 |
| Trust in official information for the new pandemic3 | ||||
| No trust | Ref | Ref | ||
| Little trust | 0.31 (0.17, 0.58) | 0.48 (0.21, 1.09) | ||
| Some/absolute trust | 0.12 (0.06, 0.23) | 1.6 × 10−10 | 0.08 (0.03, 0.23) | 4.4 × 10−6 |
| Trust in Government for minimizing the spread of coronavirus3 | ||||
| No trust | Ref | Ref | ||
| Little trust | 0.32 (0.16, 0.64) | 0.46 (0.20, 1.08) | ||
| Some trust | 0.21 (0.11, 0.41) | 0.18 (0.07, 0.47) | ||
| Absolute trust | 0.08 (0.02, 0.34) | 1.3 × 10−7 | 0.05 (0.01, 0.35) | 2.0 × 10−4 |
| Seasonal flu vaccination this year3 | ||||
| No | Ref | Ref | ||
| Yes | 0.08 (0.04, 0.17) | 1.2 × 10−11 | 0.08 (0.03, 0.21) | 7.8 × 10−7 |
| Seasonal flu vaccination last year3 | ||||
| No | Ref | Ref | ||
| Yes | 0.18 (0.09, 0.37) | 3.2 × 10−6 | 0.18 (0.07, 0.46) | 4.4 × 10−4 |
| Capability to protect against coronavirus3 | ||||
| No/little capability | Ref | Ref | ||
| Moderate capability | 1.40 (0.41, 4.77) | 1.20 (0.31, 4.71) | ||
| Absolute capability | 2.86 (0.84, 9.75) | 0.010 | 1.79 (0.44, 7.36) | 0.442 * |
| COVID-19 symptoms during last months3,6 | ||||
| No | Ref | Ref | ||
| Yes | 1.85 (0.78, 4.42) | 0.166 * | 0.83 (0.20, 3.34) | 0.787 * |
| COVID-19 tested3 | ||||
| No | Ref | Ref | ||
| Yes | 0.75 (0.44, 1.25) | 0.268 * | 1.11 (0.57, 2.15) | 0.757 * |
| Family member with COVID-19 diagnosis3 | ||||
| No | Ref | Ref | ||
| Yes | 0.69 (0.24, 2.00) | 0.493 * | 0.76 (0.20, 2.85) | 0.685 * |
| Willingness to vaccinate against coronavirus3 | ||||
| No | Ref | |||
| Yes | 0.01 (0.00, 0.04) | 2.3 × 10−7 | ‡ | |
| Willingness to vaccinate their children against coronavirus3 | ||||
| No | Ref | Ref | ||
| Yes | 0.02 (0.01, 0.08) | 9.1 × 10−8 | 0.02 (0.00, 0.12) | 8.1 × 10−5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Derdemezis, C.; Markozannes, G.; Rontogianni, M.O.; Trigki, M.; Kanellopoulou, A.; Papamichail, D.; Aretouli, E.; Ntzani, E.; Tsilidis, K.K. Parental Hesitancy towards the Established Childhood Vaccination Programmes in the COVID-19 Era: Assessing the Drivers of a Challenging Public Health Concern. Vaccines 2022, 10, 814. https://doi.org/10.3390/vaccines10050814
Derdemezis C, Markozannes G, Rontogianni MO, Trigki M, Kanellopoulou A, Papamichail D, Aretouli E, Ntzani E, Tsilidis KK. Parental Hesitancy towards the Established Childhood Vaccination Programmes in the COVID-19 Era: Assessing the Drivers of a Challenging Public Health Concern. Vaccines. 2022; 10(5):814. https://doi.org/10.3390/vaccines10050814
Chicago/Turabian StyleDerdemezis, Christos, Georgios Markozannes, Marina O. Rontogianni, Marianthi Trigki, Afroditi Kanellopoulou, Dimitris Papamichail, Eleni Aretouli, Evangelia Ntzani, and Konstantinos K. Tsilidis. 2022. "Parental Hesitancy towards the Established Childhood Vaccination Programmes in the COVID-19 Era: Assessing the Drivers of a Challenging Public Health Concern" Vaccines 10, no. 5: 814. https://doi.org/10.3390/vaccines10050814