
Sampling for SARS-CoV-2 Aerosols in Hospital Patient Rooms

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Data
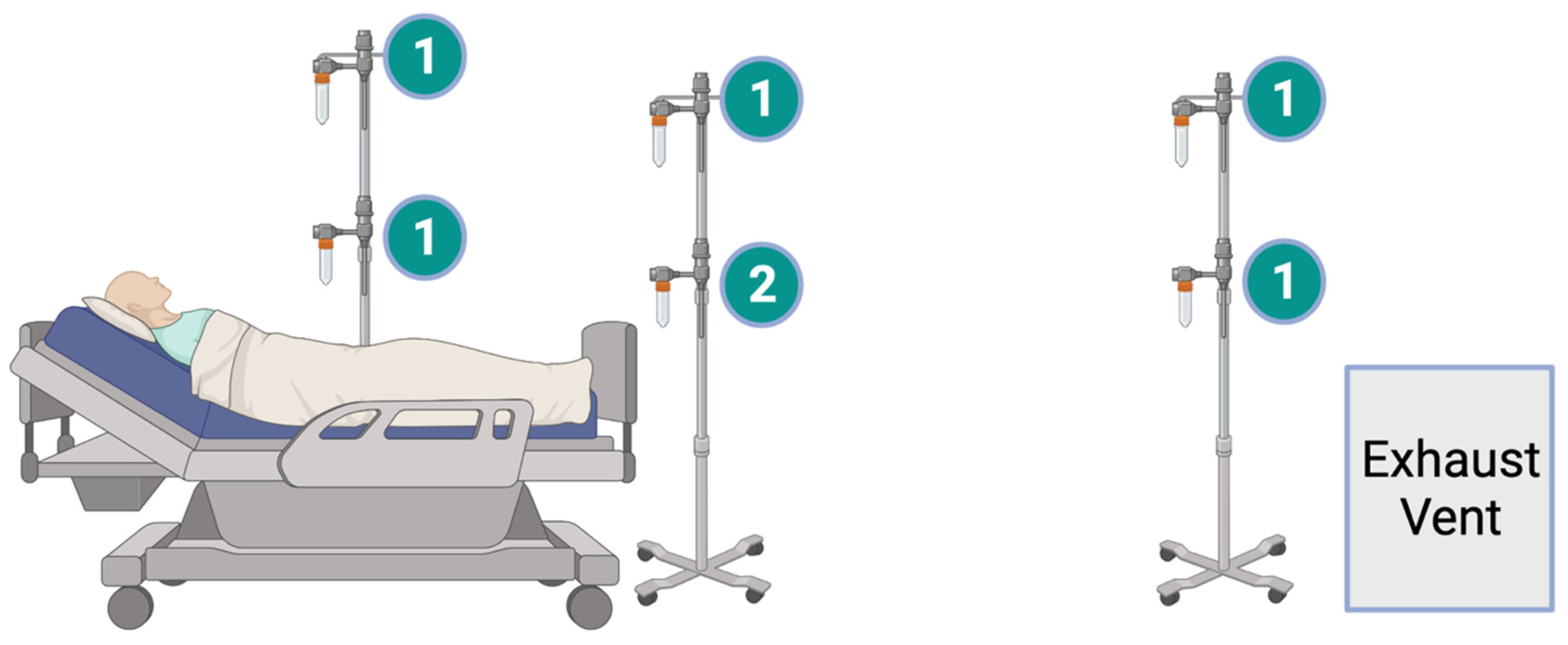
2.2. Sampling Set-Up
2.3. Aerosol Samples Processing
2.4. Viral RNA Isolation
2.5. Reverse Transcription Polymerase Chain Reaction
3. Results
3.1. Patient Characteristics
3.2. Aerosol Samples
3.3. Statistical Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Ma, J.; Qi, X.; Chen, H.; Li, X.; Zhang, Z.; Wang, H.; Sun, L.; Zhang, L.; Guo, J.; Morawska, L.; et al. Exhaled Breath Is a Significant Source of SARS-CoV-2 Emission; Public and Global Health, 2020; Available online: http://medrxiv.org/lookup/doi/10.1101/2020.05.31.20115154 (accessed on 12 November 2021).
- Jayaweera, M.; Perera, H.; Gunawardana, B.; Manatunge, J. Transmission of COVID-19 Virus by Droplets and Aerosols: A Critical Review on the Unresolved Dichotomy. Environ. Res. 2020, 188, 109819. [Google Scholar] [CrossRef]
- CDC. Scientific Brief: SARS-CoV-2 Transmission. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/sars-cov-2-transmission.html (accessed on 14 July 2021).
- Kampf, G.; Brüggemann, Y.; Kaba, H.E.J.; Steinmann, J.; Pfaender, S.; Scheithauer, S.; Steinmann, E. Potential Sources, Modes of Transmission and Effectiveness of Prevention Measures against SARS-CoV-2. J. Hosp. Infect. 2020, 106, 678–697. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ferro, E.G.; Zhou, G.; Hashimoto, D.; Bhatt, D.L. Association Between Universal Masking in a Health Care System and SARS-CoV-2 Positivity Among Health Care Workers. JAMA 2020, 324, 703. [Google Scholar] [CrossRef]
- Rotondo, J.C.; Martini, F.; Maritati, M.; Mazziotta, C.; Di Mauro, G.; Lanzillotti, C.; Barp, N.; Gallerani, A.; Tognon, M.; Contini, C. SARS-CoV-2 Infection: New Molecular, Phylogenetic, and Pathogenetic Insights. Efficacy of Current Vaccines and the Potential Risk of Variants. Viruses 2021, 13, 1687. [Google Scholar] [CrossRef] [PubMed]
- Chia, P.Y.; Coleman, K.K.; Tan, Y.K.; Ong, S.W.X.; Gum, M.; Lau, S.K.; Lim, X.F.; Lim, A.S.; Sutjipto, S.; Lee, P.H.; et al. Detection of Air and Surface Contamination by SARS-CoV-2 in Hospital Rooms of Infected Patients. Nat. Commun. 2020, 11, 2800. [Google Scholar] [CrossRef]
- Guo, Z.-D.; Wang, Z.-Y.; Zhang, S.-F.; Li, X.; Li, L.; Li, C.; Cui, Y.; Fu, R.-B.; Dong, Y.-Z.; Chi, X.-Y.; et al. Aerosol and Surface Distribution of Severe Acute Respiratory Syndrome Coronavirus 2 in Hospital Wards, Wuhan, China, 2020. Emerg. Infect. Dis. 2020, 26, 1583–1591. [Google Scholar] [CrossRef]
- Lednicky, J.A.; Lauzardo, M.; Fan, Z.H.; Jutla, A.S.; Tilly, T.B.; Gangwar, M.; Usmani, M.; Shankar, S.N.; Mohamed, K.; Eiguren-Fernandez, A.; et al. Viable SARS-CoV-2 in the Air of a Hospital Room with COVID-19 Patients. Int. J. Infect. Dis. 2020, 100, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Santarpia, J.L.; Rivera, D.N.; Herrera, V.L.; Morwitzer, M.J.; Creager, H.M.; Santarpia, G.W.; Crown, K.K.; Brett-Major, D.M.; Schnaubelt, E.R.; Broadhurst, M.J.; et al. Aerosol and Surface Contamination of SARS-CoV-2 Observed in Quarantine and Isolation Care. Sci. Rep. 2020, 10, 12732. [Google Scholar] [CrossRef]
- Santarpia, J.L.; Rivera, D.N.; Herrera, V.; Morwitzer, M.J.; Creager, H.; Santarpia, G.W.; Crown, K.K.; Brett-Major, D.; Schnaubelt, E.; Broadhurst, M.J.; et al. Transmission Potential of SARS-CoV-2 in Viral Shedding Observed at the University of Nebraska Medical Center; Infectious Diseases (except HIV/AIDS). Sci. Rep. 2020, 10, 12732. [Google Scholar] [CrossRef]
- Semelka, C.T.; Ornelles, D.A.; O’ Connell, N.S.; Parsons, E.C.; Blevins, M.W.; Ivey, L.E.; Bischoff, W.E. Detection of Environmental Spread of SARS-CoV-2 and Associated Patient Characteristics. Open Forum Infect. Dis. 2021, 8, ofab107. [Google Scholar] [CrossRef]
- Santarpia, J.L.; Herrera, V.L.; Rivera, D.N.; Ratnesar-Shumate, S.; Reid, S.P.; Ackerman, D.N.; Denton, P.W.; Martens, J.W.S.; Fang, Y.; Conoan, N. The Size and Culturability of Patient-Generated SARS-CoV-2 Aerosol. J. Expo. Sci. Environ. Epidemiol. 2021. Available online: https://www.nature.com/articles/s41370-021-00376-8 (accessed on 20 August 2021). [CrossRef]
- Binder, R.A.; Alarja, N.A.; Robie, E.R.; Kochek, K.E.; Xiu, L.; Rocha-Melogno, L.; Abdelgadir, A.; Goli, S.V.; Farrell, A.S.; Coleman, K.K.; et al. Environmental and Aerosolized SARS-CoV-2 Among Hospitalized COVID-19 Patients. J. Infect. Dis. 2020, 222, jiaa575. [Google Scholar] [CrossRef]
- Cheng, V.C.C.; Wong, S.-C.; Chen, J.H.K.; Yip, C.C.Y.; Chuang, V.W.M.; Tsang, O.T.Y.; Sridhar, S.; Chan, J.F.W.; Ho, P.-L.; Yuen, K.-Y. Escalating Infection Control Response to the Rapidly Evolving Epidemiology of the Coronavirus Disease 2019 (COVID-19) Due to SARS-CoV-2 in Hong Kong. Infect. Control Hosp. Epidemiol. 2020, 41, 493–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, V.C.-C.; Wong, S.-C.; Chan, V.W.-M.; So, S.Y.-C.; Chen, J.H.-K.; Yip, C.C.-Y.; Chan, K.-H.; Chu, H.; Chung, T.W.-H.; Sridhar, S.; et al. Air and Environmental Sampling for SARS-CoV-2 around Hospitalized Patients with Coronavirus Disease 2019 (COVID-19). Infect. Control Hosp. Epidemiol. 2020, 41, 1258–1265. [Google Scholar] [CrossRef]
- Ding, Z.; Qian, H.; Xu, B.; Huang, Y.; Miao, T.; Yen, H.-L.; Xiao, S.; Cui, L.; Wu, X.; Shao, W.; et al. Toilets Dominate Environmental Detection of Severe Acute Respiratory Syndrome Coronavirus 2 in a Hospital. Sci. Total Environ. 2021, 753, 141710. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.H.; Fan, Y.Z.; Jiang, L.; Wang, H.B. Aerosol and Environmental Surface Monitoring for SARS-CoV-2 RNA in a Designated Hospital for Severe COVID-19 Patients. Epidemiol. Infect. 2020, 148, e154. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdahl, D.; et al. Aerodynamic Characteristics and RNA Concentration of SARS-CoV-2 Aerosol in Wuhan Hospitals during COVID-19 Outbreak. Microbiology 2020, 582, 557–560. Available online: http://biorxiv.org/lookup/doi/10.1101/2020.03.08.982637 (accessed on 12 November 2021).
- Liu, Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdahl, D.; et al. Aerodynamic Analysis of SARS-CoV-2 in Two Wuhan Hospitals. Nature 2020, 7813, 557–560. [Google Scholar] [CrossRef]
- Ong, S.W.X.; Tan, Y.K.; Chia, P.Y.; Lee, T.H.; Ng, O.T.; Wong, M.S.Y.; Marimuthu, K. Air, Surface Environmental, and Personal Protective Equipment Contamination by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) From a Symptomatic Patient. JAMA 2020, 323, 1610. [Google Scholar] [CrossRef] [Green Version]
- Lane, M.A.; Brownsword, E.A.; Morgan, J.S.; Babiker, A.; Vanairsdale, S.A.; Lyon, G.M.; Mehta, A.K.; Ingersoll, J.M.; Lindsley, W.G.; Kraft, C.S. Bioaerosol Sampling of a Ventilated Patient with COVID-19. Am. J. Infect. Control. 2020, 48, 1540–1542. [Google Scholar] [CrossRef]
- Lane, M.A.; Brownsword, E.A.; Babiker, A.; Ingersoll, J.M.; Waggoner, J.; Ayers, M.; Klopman, M.; Uyeki, T.M.; Lindsley, W.G.; Kraft, C.S. Bioaerosol Sampling for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in a Referral Center with Critically Ill Coronavirus Disease 2019 (COVID-19) Patients March–May 2020. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, e1790–e1794. [Google Scholar] [CrossRef] [PubMed]
- Birgand, G.; Peiffer-Smadja, N.; Fournier, S.; Kerneis, S.; Lescure, F.-X.; Lucet, J.-C. Assessment of Air Contamination by SARS-CoV-2 in Hospital Settings. JAMA Netw. Open 2020, 3, e2033232. [Google Scholar] [CrossRef]
- Ong, S.W.X.; Tan, Y.K.; Coleman, K.K.; Tan, B.H.; Leo, Y.-S.; Wang, D.L.; Ng, C.G.; Ng, O.-T.; Wong, M.S.Y.; Marimuthu, K. Lack of Viable Severe Acute Respiratory Coronavirus Virus 2 (SARS-CoV-2) among PCR-Positive Air Samples from Hospital Rooms and Community Isolation Facilities. Infect. Control Hosp. Epidemiol. 2021, 42, 1327–1332. [Google Scholar] [CrossRef]
- Robie, E.R.; Abdelgadir, A.; Binder, R.A.; Gray, G.C. Live SARS-CoV-2 Is Difficult to Detect in Patient Aerosols. Influenza Other Respir. Viruses 2021, 15, 554. [Google Scholar] [CrossRef]
- van Kampen, J.J.A.; van de Vijver, D.A.M.C.; Fraaij, P.L.A.; Haagmans, B.L.; Lamers, M.M.; Okba, N.; van den Akker, J.P.C.; Endeman, H.; Gommers, D.A.M.P.J.; Cornelissen, J.J.; et al. Duration and Key Determinants of Infectious Virus Shedding in Hospitalized Patients with Coronavirus Disease-2019 (COVID-19). Nat. Commun. 2021, 12, 267. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.A.; Ausiello, D.; Salzman, J.; Devlin, T.; Langer, R.; Beddingfield, B.J.; Fears, A.C.; Doyle-Meyers, L.A.; Redmann, R.K.; Killeen, S.Z.; et al. Exhaled Aerosol Increases with COVID-19 Infection, Age, and Obesity. Proc. Natl. Acad. Sci. USA 2021, 118, e2021830118. [Google Scholar] [CrossRef] [PubMed]
- Grassin-Delyle, S.; Roquencourt, C.; Moine, P.; Saffroy, G.; Carn, S.; Heming, N.; Fleuriet, J.; Salvator, H.; Naline, E.; Couderc, L.-J.; et al. Metabolomics of Exhaled Breath in Critically Ill COVID-19 Patients: A Pilot Study. EBioMedicine 2021, 63, 103154. [Google Scholar] [CrossRef]
- Li, X.; Li, J.; Ge, Q.; Du, Y.; Li, G.; Li, W.; Zhang, T.; Tan, L.; Zhang, R.; Yuan, X.; et al. Detecting SARS-CoV-2 in the Breath of COVID-19 Patients. Front. Med. 2021, 8, 210. [Google Scholar] [CrossRef]
- Guzman, M.I. An Overview of the Effect of Bioaerosol Size in Coronavirus Disease 2019 Transmission. Int. J. Health Plan. Manag. 2021, 36, 257–266. [Google Scholar] [CrossRef]
- Madas, B.G.; Füri, P.; Farkas, Á.; Nagy, A.; Czitrovszky, A.; Balásházy, I.; Schay, G.G.; Horváth, A. Deposition Distribution of the New Coronavirus (SARS-CoV-2) in the Human Airways upon Exposure to Cough-Generated Droplets and Aerosol Particles. Sci. Rep. 2020, 10, 22430. [Google Scholar] [CrossRef]
- CDC Coronavirus Disease 2019 (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/how-to-make-cloth-face-covering.html (accessed on 24 June 2020).
- Wong, C.K.H.; Wong, J.Y.H.; Tang, E.H.M.; Au, C.H.; Lau, K.T.K.; Wai, A.K.C. Impact of National Containment Measures on Decelerating the Increase in Daily New Cases of COVID-19 in 54 Countries and 4 Epicenters of the Pandemic: Comparative Observational Study. J. Med. Internet Res. 2020, 22, e19904. [Google Scholar] [CrossRef]
- Blachere, F.M.; Lindsley, W.G.; Pearce, T.A.; Anderson, S.E.; Fisher, M.; Khakoo, R.; Meade, B.J.; Lander, O.; Davis, S.; Thewlis, R.E.; et al. Measurement of Airborne Influenza Virus in a Hospital Emergency Department. Clin. Infect. Dis. 2009, 48, 438–440. [Google Scholar] [CrossRef] [Green Version]
- Lindsley, B. NIOSH Influenza Transmission Research; 2013; Available online: https://ia803201.us.archive.org/29/items/NioshPersonalProtectiveTechnologyProgramHealthcareStakeholderMeeting/PresentLindsleyInfluenzaTransmissionResearch.pdf (accessed on 12 November 2021).
- CDC Guidelines for Environmental Infection Control in Health-Care Facilities: Appendix B. Air. Available online: https://www.cdc.gov/infectioncontrol/guidelines/environmental/appendix/air.html (accessed on 9 September 2021).
- Waggoner, J.J.; Stittleburg, V.; Pond, R.; Saklawi, Y.; Sahoo, M.K.; Babiker, A.; Hussaini, L.; Kraft, C.S.; Pinsky, B.A.; Anderson, E.J.; et al. Triplex Real-Time RT-PCR for Severe Acute Respiratory Syndrome Coronavirus 2. Emerg. Infect. Dis. 2020, 26, 1633–1635. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. CDC 2019-Novel Coronavirus (2019-NCoV) Real-Time RT-PCR Diagnostic Panel; CDC/DDID/NCIRD/ Division of Viral Diseases, 2020. Available online: https://www.fda.gov/media/134922/download (accessed on 12 November 2021).
- Singanayagam, A.; Patel, M.; Charlett, A.; Lopez Bernal, J.; Saliba, V.; Ellis, J.; Ladhani, S.; Zambon, M.; Gopal, R. Duration of Infectiousness and Correlation with RT-PCR Cycle Threshold Values in Cases of COVID-19, England, January to May 2020. Eurosurveillance 2020, 25, 2001483. [Google Scholar] [CrossRef]
- La Scola, B.; Le Bideau, M.; Andreani, J.; Hoang, V.T.; Grimaldier, C.; Colson, P.; Gautret, P.; Raoult, D. Viral RNA Load as Determined by Cell Culture as a Management Tool for Discharge of SARS-CoV-2 Patients from Infectious Disease Wards. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1059–1061. [Google Scholar] [CrossRef]
- Ratnesar-Shumate, S.; Williams, G.; Holland, B.; Bohannon, J.; Krause, M.; Green, B.; Freeburger, D.; Dabisch, P. Comparison of the Performance of Personal Biological Aerosol Samplers for SARS-CoV-2. Aerosol Sci. Technol. 2020, 55, 975–998. Available online: https://aaarabstracts.com/2020/viewabstract.php?pid=388 (accessed on 29 September 2020). [CrossRef]
- CDC Interim Infection Prevention and Control Recommendations for Healthcare Personnel During the Coronavirus Disease 2019 (COVID-19) Pandemic. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html (accessed on 19 July 2021).

{kind=link}
| Group | No. per Group | Avg. Days since Symptom Onset | Ambulatory | Rec. Oxygen | Coughing | Co-Morbid. Present 1 | Pneumonia | Rec. Treat. (D & R) 2 | Avg. Treat. Duration 3 | Avg. Ct Value of NP Swab 4 |
|---|---|---|---|---|---|---|---|---|---|---|
| Total | 32 | 8.5 | 25 | 15 | 14 | 28 | 21 | 24 | 4.4 | 27.3 |
| Positive Aerosol Samples | 9 | 6.6 | 6 | 6 | 5 | 9 | 6 | 7 | 1.6 | 26.8 |
| Negative Aerosol Samples | 23 | 9.3 | 19 | 9 | 9 | 19 | 15 | 15 | 3.6 | 27.6 |
| Location | High Sampler | Low Sampler | |||
|---|---|---|---|---|---|
| 15 mL | 1.5 mL | 15 mL | 1.5 mL | Filter | |
| Head of bed | 1 | 4 | 1 | 2 | 0 |
| Foot of bed | 0 | 6 | 0 | 2 | 1 |
| Exhaust Vent | 0 | 1 | 0 | 1 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lane, M.A.; Walawender, M.; Webster, A.S.; Brownsword, E.A.; Ingersoll, J.M.; Miller, C.; Waggoner, J.; Uyeki, T.M.; Lindsley, W.G.; Kraft, C.S. Sampling for SARS-CoV-2 Aerosols in Hospital Patient Rooms. Viruses 2021, 13, 2347. https://doi.org/10.3390/v13122347
Lane MA, Walawender M, Webster AS, Brownsword EA, Ingersoll JM, Miller C, Waggoner J, Uyeki TM, Lindsley WG, Kraft CS. Sampling for SARS-CoV-2 Aerosols in Hospital Patient Rooms. Viruses. 2021; 13(12):2347. https://doi.org/10.3390/v13122347
Chicago/Turabian StyleLane, Morgan A., Maria Walawender, Andrew S. Webster, Erik A. Brownsword, Jessica M. Ingersoll, Candace Miller, Jesse Waggoner, Timothy M. Uyeki, William G. Lindsley, and Colleen S. Kraft. 2021. "Sampling for SARS-CoV-2 Aerosols in Hospital Patient Rooms" Viruses 13, no. 12: 2347. https://doi.org/10.3390/v13122347