
Vaccines Administration in the Perspective of Patient Safety and Quality of Healthcare: Lesson from the Experience of an Italian Teaching Hospital for Pandemic Preparedness
 , , ,
, , ,
Abstract
:1. Introduction
2. Case Study
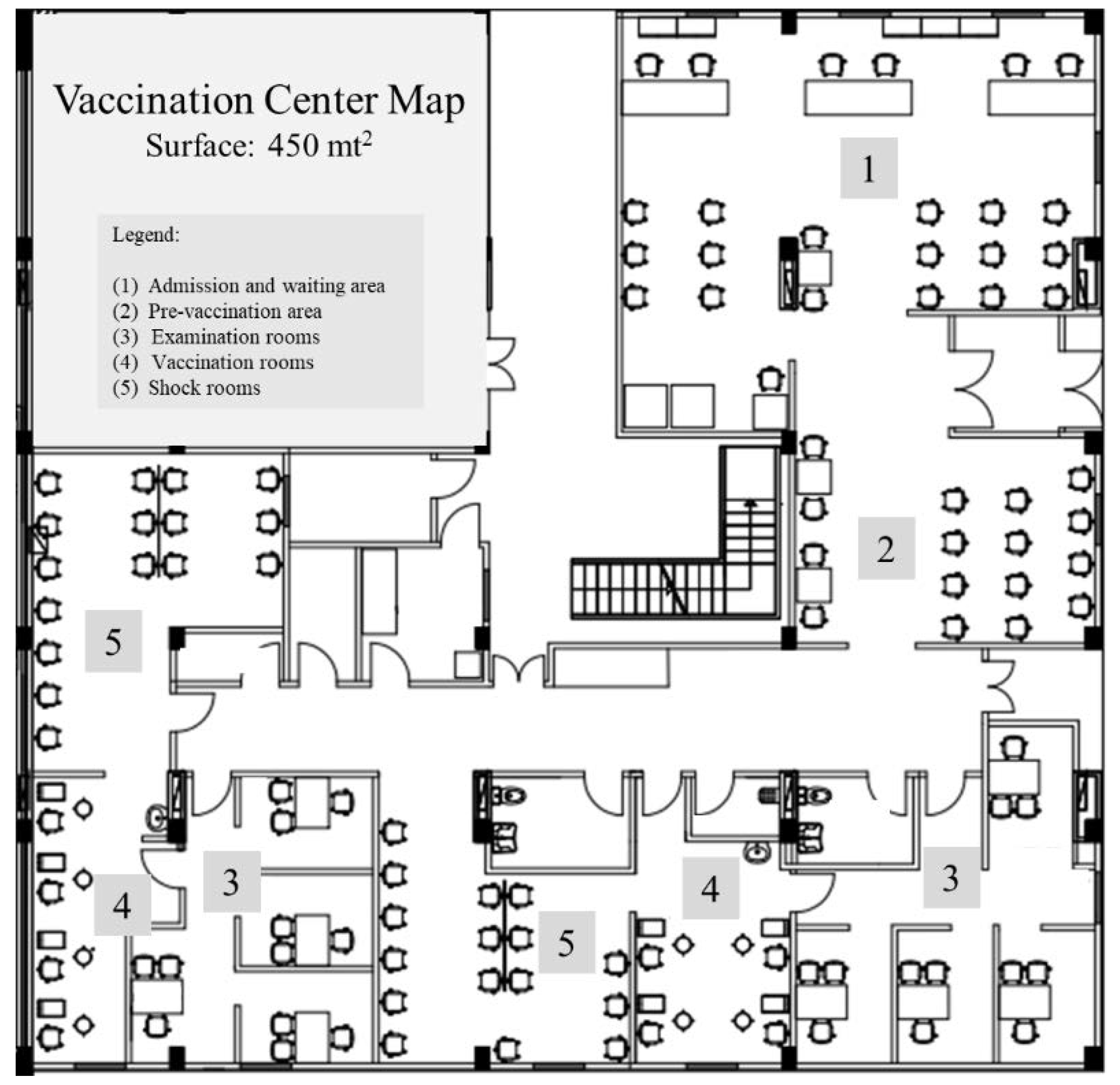
2.1. Organization of the Vaccination Center (VC) Building
2.2. Staff Recruitment and Training
2.3. Vaccines Procurement, Storage, and Transport
2.4. Vaccine Preparation and Administration
2.5. Challenges and Opportunities
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Worobey, M.; Levy, J.I.; Serrano, L.M.; Crits-Christoph, A.; Pekar, J.E.; Goldstein, S.A.; Rasmussen, A.L.; Kraemer, M.; Newman, C.; Koopmans, M.; et al. The Huanan Seafood Wholesale Market in Wuhan was the early epicenter of the COVID-19 pandemic. Science 2022, 377, 951–959. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 27 July 2022).
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 27 July 2022).
- United Nations. A UN Framework for the Immediate Socio-Economic Response to COVID-19. Available online: https://unsdg.un.org/sites/default/files/2020-04/UN-framework-for-the-immediate-socio-economic-response-to-COVID-19.pdf (accessed on 27 July 2022).
- World Health Organization. COVID-19 Vaccination. Available online: https://www.who.int/europe/emergencies/situations/covid-19/covid-19-vaccination (accessed on 27 July 2022).
- Di Fazio, N.; Delogu, G.; Bertozzi, G.; Fineschi, V.; Frati, P. SARS-CoV2 Vaccination Adverse Events Trend in Italy: A Retrospective Interpretation of the Last Year (December 2020-September 2021). Vaccines 2022, 10, 216. [Google Scholar] [CrossRef]
- Frati, P.; Di Fazio, N.; La Russa, R.; Santoro, P.; Delogu, G.; Fineschi, V. No-Fault Compensation and Anti-COVID-19 Compulsory Vaccination: The Italian Context in a Broad View. Vaccines 2022, 10, 635. [Google Scholar] [CrossRef]
- Governo Italiano. Report Vaccini Anti COVID-19. Available online: https://www.governo.it/it/cscovid19/report-vaccini/ (accessed on 27 July 2022).
- Peruch, M.; Toscani, P.; Grassi, N.; Zamagni, G.; Monasta, L.; Radaelli, D.; Livieri, T.; Manfredi, A.; D’Errico, S. Did Italy Really Need Compulsory Vaccination against COVID-19 for Healthcare Workers? Results of a Survey in a Centre for Maternal and Child Health. Vaccines 2022, 10, 1293. [Google Scholar] [CrossRef]
- Zdravkovic, M.; Popadic, V.; Nikolic, V.; Klasnja, S.; Brajkovic, M.; Manojlovic, A.; Nikolic, N.; Markovic-Denic, L. COVID-19 Vaccination Willingness and Vaccine Uptake among Healthcare Workers: A Single-Center Experience. Vaccines 2022, 10, 500. [Google Scholar] [CrossRef]
- Signorelli, C.; Odone, A.; Gianfredi, V.; Capraro, M.; Kacerik, E.; Chiecca, G.; Scardoni, A.; Minerva, M.; Mantecca, R.; Musarò, P.; et al. Application of the “immunization islands” model to improve quality, efficiency and safety of a COVID-19 mass vaccination site. Ann. Ig. 2021, 33, 499–512. [Google Scholar]
- Ministero della Salute. Piano Nazionale Prevenzione Vaccinale 2017–2019 (PNPV). Available online: https://www.salute.gov.it/portale/vaccinazioni/dettaglioContenutiVaccinazioni.jsp?lingua=italiano&id=4828&area=vaccinazioni&menu=vuoto (accessed on 24 August 2022).
- Goralnick, E.; Kaufmann, C.; Gawande, A.A. Mass-Vaccination Sites—An Essential Innovation to Curb the COVID-19 Pandemic. N. Eng. J. Med. 2021, 384, e67. [Google Scholar] [CrossRef] [PubMed]
- Ministero della Salute. Presidenza del Consiglio dei Ministri, Istituto Superiore di Sanità, Agenzia Nazionale per i Servizi Sanitari Regionali, Agenzia Italiana del Farmaco. Vaccinazione Anti SARS-CoV-2/COVID-19. Piano Strategico. 12 Dicembre 2020. Available online: https://www.trovanorme.salute.gov.it/norme/renderPdf.spring?seriegu=SG&datagu=24/03/2021&redaz=21A01802&artp=1&art=1&subart=1&subart1=10&vers=1&prog=001 (accessed on 27 July 2022).
- Presidenza del Consiglio dei Ministri. Piano Vaccinale AntiCovid. 13 marzo 2021. Available online: https://www.governo.it/sites/governo.it/files/210313_Piano_Vaccinale_marzo_2021_1.pdf (accessed on 27 July 2022).
- Tatar, M.; Wilson, F.A. The largest vaccination campaign in history: A golden opportunity for bundling public health interventions. J. Glob. Health 2021, 11, 03076. [Google Scholar] [CrossRef]
- Fleisher, L.A.; Schreiber, M.; Cardo, D.; Srinivasan, A. Health Care Safety during the Pandemic and Beyond - Building a System That Ensures Resilience. NEJM 2022, 386, 609–611. [Google Scholar] [CrossRef]
- Baker, M.A.; Sands, K.E.; Huang, S.S.; Kleinman, K.; Septimus, E.J.; Varma, N.; Blanchard, J.; Poland, R.E.; Coady, M.H.; Yokoe, D.S.; et al. CDC Prevention Epicenters Program. The Impact of Coronavirus Disease 2019 (COVID-19) on Healthcare-Associated Infections. Clin. Infect. Dis. 2022, 74, 1748–1754. [Google Scholar] [CrossRef] [PubMed]
- Fakih, M.G.; Bufalino, A.; Sturm, L.; Huang, R.H.; Ottenbacher, A.; Saake, K.; Winegar, A.; Fogel, R.; Cacchione, J. Coronavirus disease 2019 (COVID-19) pandemic, central-line-associated bloodstream infection (CLABSI), and catheter-associated urinary tract infection (CAUTI): The urgent need to refocus on hardwiring prevention efforts. Infect. Control Hosp. Epidemiol. 2022, 43, 26–31. [Google Scholar] [CrossRef]
- Shakespeare, W.; Bevington, D.M. 1 Henry IV, Part 1; Oxford University Press: Oxford, UK, 1994. [Google Scholar]
- Eftekhar Ardebili, M.; Naserbakht, M.; Bernstein, C.; Alazmani-Noodeh, F.; Hakimi, H.; Ranjbar, H. Healthcare providers experience of working during the COVID-19 pandemic: A qualitative study. AJIC 2021, 49, 547–554. [Google Scholar] [CrossRef]
- Papini, F.; Grassi, N.; Guglielmi, G.; Gattini, V.; Rago, L.; Bisordi, C.; Scateni, M.; Totaro, M.; Tulipani, A.; Porretta, A.; et al. COVID-19 vaccine management (Comirnaty and mrna-1273 Moderna) in a teaching hospital in Italy: A short report on the vaccination campaign. Environ. Health Prev. Med. 2021, 26, 99. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Guidelines for Large Scale Novel H1N1 Influenza Vaccination Clinics. Available online: https://www.cdc.gov/h1n1flu/vaccination/pdf/D_Wortley_H1N1_guidelines_pandemic.pdf (accessed on 27 July 2022).
- Food and Drug Administration. COVID-19 Vaccines 2021. Available online: https://www.fda.gov/emergencypreparedness-and-response/coronavirus-disease-2019-covid-19/covid-19-vaccines (accessed on 27 July 2022).
- Gianfredi, V.; Pennisi, F.; Lume, A.; Ricciardi, G.E.; Minerva, M.; Riccò, M.; Odone, A.; Signorelli, C. Challenges and Opportunities of Mass Vaccination Centers in COVID-19 Times: A Rapid Review of Literature. Vaccines 2021, 9, 574. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, R.L.; Subramanian, L.; Karlage, A.; Ahmad, I.; Rosenberg, J. COVID-19 vaccine to vaccination: Why leaders must invest in delivery strategies now. Health Aff. 2021, 40, 33–41. [Google Scholar] [CrossRef]
- World Health Organization. Patient Safety Curriculum Guide: Multi-Professional Edition. Available online: https://www.who.int/patientsafety/education/curriculum/who_mc_topic-6.pdf (accessed on 27 July 2022).
- The Joint Commission releases improving America’s hospitals: The Joint Commission’s annual report on quality and safety 2007. Jnt. Comm. Perspect. 2007, 27, 1–3.
- Brborovi’c, O.; Brborovi´c, H.; Hrain, L. The COVID-19 Pandemic Crisis and Patient Safety Culture: A Mixed-Method Study. Int. J. Environ. Res. Public Health 2022, 19, 2237. [Google Scholar] [CrossRef]
- The Agency for Healthcare Research and Quality’s. Patient Safety Events and the Role of Patient Safety Organizations during the COVID-19 Pandemic. Available online: https://psnet.ahrq.gov/perspective/patient-safety-events-and-role-patient-safety-organizations-during-covid-19-pandemic (accessed on 27 July 2022).
- NPSD Data Spotlight, Patient Safety and COVID-19: A Qualitative Analysis of Concerns during the Public Health Emergency, 2021. Rockville, MD: Agency for Healthcare Research and Quality; November 2021. AHRQ Pub. No. 22-0005. Available online: https://www.ahrq.gov/sites/default/files/wysiwyg/npsd/data/spotlights/spotlight-ptsafety-and-covid-19.pdf (accessed on 27 July 2022).
- La Regina, M.; Tanzini, M.; Toccafondi, G.V.; Fineschi, V.; Lachman, P.; Arnoldo, L.; Bacci, I.; De Palma, A.; Di Tommaso, M.; Fagiolini, A.; et al. Patient Safety Recommendations for COVID-19 Epidemic Outbreak. Lessons from the Italian Experience. Available online: https://www.insafetyhealthcare.it/wpcontent/uploads/2020/04/PATIENT_SAFETY_RECOMMENDATIONS_Final_version.pdf (accessed on 27 July 2022).
- Horton, R. The COVID-19 Catastrophe: What’s Gone Wrong and How to Stop It Happening Again; Polity Pr: Cambridge, UK, 2020. [Google Scholar]
- Fineberg, H.V. Pandemic preparedness and response--lessons from the H1N1 influenza of 2009. NEJM 2014, 370, 1335–1342. [Google Scholar] [CrossRef]
- World Health Organization. Strengthening Response to Pandemics and Other Public-Health Emergencies: Report of the Review Committee on the Functioning of the International Health Regulations (2005) and on Pandemic Influenza (H1N1) 2009. Available online: https://apps.who.int/iris/bitstream/handle/10665/75235/9789241564335_eng.pdf?sequence=1,2011 (accessed on 27 July 2022).
- Comitato Nazionale di Bioetica. COVID-19: La Decisione Clinica in Condizioni di Carenza di Risorse e il Criterio del “Triage in Emergenza Pandemica”. Available online: https://bioetica.governo.it/it/pareri/pareri-e-risposte/covid-19-la-decisione-clinica-in-condizioni-di-carenza-di-risorse-e-il-criterio-del-triage-in-emergenza-pandemica/ (accessed on 27 July 2022).
- World Health Organization (WHO). Global Patient Safety Action Plan 2021–2030. Available online: https://www.who.int/publications/i/item/9789240032705 (accessed on 27 July 2022).
- Organisation for Economic Co-Operation and Development (OECD). Developing International Benchmarks of Patient Safety Culture in Hospital Care. Available online: https://one.oecd.org/document/DELSA/HEA/WD/HWP(2022)2/en/pdf (accessed on 27 July 2022).
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of health-care providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e798. [Google Scholar] [CrossRef]
- De Benedictis, A.; Gualandi, R.; Saccoccia, S.; Pensieri, C.; Piredda, M.; De Micco, F.; Marchetti, A.; Facchinetti, G.; Pasquarelli, A.; De Carolis, C.; et al. Back to the Roots of Nursing: Qualitative Study on the Experience of Nurses in the Front Line During the COVID-19 Pandemic. Front. Med. 2022, 9, 903517. [Google Scholar] [CrossRef]
- Kuhn, T.S. The Structure of Scientific Revolutions; University of Chicago Press: Chicago, IL, USA, 1970. [Google Scholar]
- Moretti, V. Sensitivity Theory for Nonlinear Systems. I. Nonlinear Functional Analysis Approach; Springer: Berlin, Germany, 2017. [Google Scholar]
- Berto, F. There’s Something about Gödel: The Complete Guide to the Incompleteness Theorem; Wiley-Blackwell: Hoboken, NJ, USA, 2010. [Google Scholar]
- Holbrow, C.H.; Lloyd, J.N.; Amato, J.C. The Heisenberg Uncertainty Principle. In Modern Introductory Physics; Holbrow, C.H., Lloyd, J.N., Amato, J.C., Galvez, E., Parks, M.E., Eds.; Springer: New York, NY, USA, 1999. [Google Scholar]
- Einstein, A. Relativity: The Special and General Theory; Pi Press: New York, NY, USA, 2005. [Google Scholar]
- Mehta, N.; Pandit, A.; Shukla, S. Transforming healthcare with big data analytics and artificial intelligence: A systematic mapping study. J. Biomed. Inform. 2019, 100, 103311. [Google Scholar] [CrossRef] [PubMed]
- De Micco, F.; De Benedictis, A.; Fineschi, V.; Frati, P.; Ciccozzi, M.; Pecchia, L.; Alloni, R.; Petrosillo, N.; Filippi, S.; Ghilardi, G.; et al. From Syndemic Lesson after COVID-19 Pandemic to a “Systemic Clinical Risk Management” Proposal in the Perspective of the Ethics of Job Well Done. Int. J. Environ. Res. Public Health 2021, 19, 15. [Google Scholar] [CrossRef] [PubMed]
- Tambone, V.; Ghilardi, G. Philosophy and Deontology of Medical Practice, Ethics of the Job Well Done in Bio-Medical Sciences; Società Editrice Universo: Rome, Italy, 2020. [Google Scholar]
- De Micco, F.; Fineschi, V.; Banfi, G.; Frati, P.; Oliva, A.; Travaini, G.V.; Picozzi, M.; Curcio, G.; Pecchia, L.; Petitti, T.; et al. From COVID-19 Pandemic to Patient Safety: A New “Spring” for Telemedicine or a Boomerang Effect? Front. Med. 2022, 9, 901788. [Google Scholar] [CrossRef] [PubMed]
- Quintiliani, L.; Sisto, A.; Vicinanza, F.; Curcio, G.; Tambone, V. Resilience and psychological impact on Italian university students during COVID-19 pandemic. Distance learning and health. Psychol. Health Med. 2022, 27, 69–80. [Google Scholar] [CrossRef]
- Hofstetter, A.M.; Rao, S.; Jhaveri, R. Beyond Influenza Vaccination: Expanding Infrastructure for Hospital-based Pediatric COVID-19 Vaccine Delivery. Clin. Ther. 2022, 44, 450–455. [Google Scholar] [CrossRef]
- Delgado, E.J.; Cabezas, X.; Martin-Barreiro, C.; Leiva, V.; Rojas, F. An Equity-Based Optimization Model to Solve the Location Problem for Healthcare Centers Applied to Hospital Beds and COVID-19 Vaccination. Mathematics 2022, 10, 1825. [Google Scholar] [CrossRef]
- Skoglund, P. Safety first, the motto for a disaster response plan. J. Healthc. Manag. 2011, 27, 114–120. [Google Scholar]


{kind=link}
| Given Doses | N. |
|---|---|
| Total doses administered | 279,056 |
| Mean per day | 503 |
| Max. per day | 1543 |
| Min. per day | 3 |
| Given Doses | N. |
|---|---|
| First doses | 100,360 |
| Second doses | 96,199 |
| Third doses | 74,981 |
| Fourth doses | 7516 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Micco, F.; De Benedictis, A.; Sommella, L.; Di Mattia, A.; Campanozzi, L.L.; Alloni, R.; Tambone, V. Vaccines Administration in the Perspective of Patient Safety and Quality of Healthcare: Lesson from the Experience of an Italian Teaching Hospital for Pandemic Preparedness. Vaccines 2022, 10, 1495. https://doi.org/10.3390/vaccines10091495
De Micco F, De Benedictis A, Sommella L, Di Mattia A, Campanozzi LL, Alloni R, Tambone V. Vaccines Administration in the Perspective of Patient Safety and Quality of Healthcare: Lesson from the Experience of an Italian Teaching Hospital for Pandemic Preparedness. Vaccines. 2022; 10(9):1495. https://doi.org/10.3390/vaccines10091495
Chicago/Turabian StyleDe Micco, Francesco, Anna De Benedictis, Lorenzo Sommella, Andrea Di Mattia, Laura Leondina Campanozzi, Rossana Alloni, and Vittoradolfo Tambone. 2022. "Vaccines Administration in the Perspective of Patient Safety and Quality of Healthcare: Lesson from the Experience of an Italian Teaching Hospital for Pandemic Preparedness" Vaccines 10, no. 9: 1495. https://doi.org/10.3390/vaccines10091495