Rural Healthcare Enterprises in the Vortex of COVID-19: The Impact of Public Policies on the Internal and External Environment

 and
and
Abstract
:1. Introduction
2. Literature Review
3. Methodology
4. Data Analysis
5. Findings
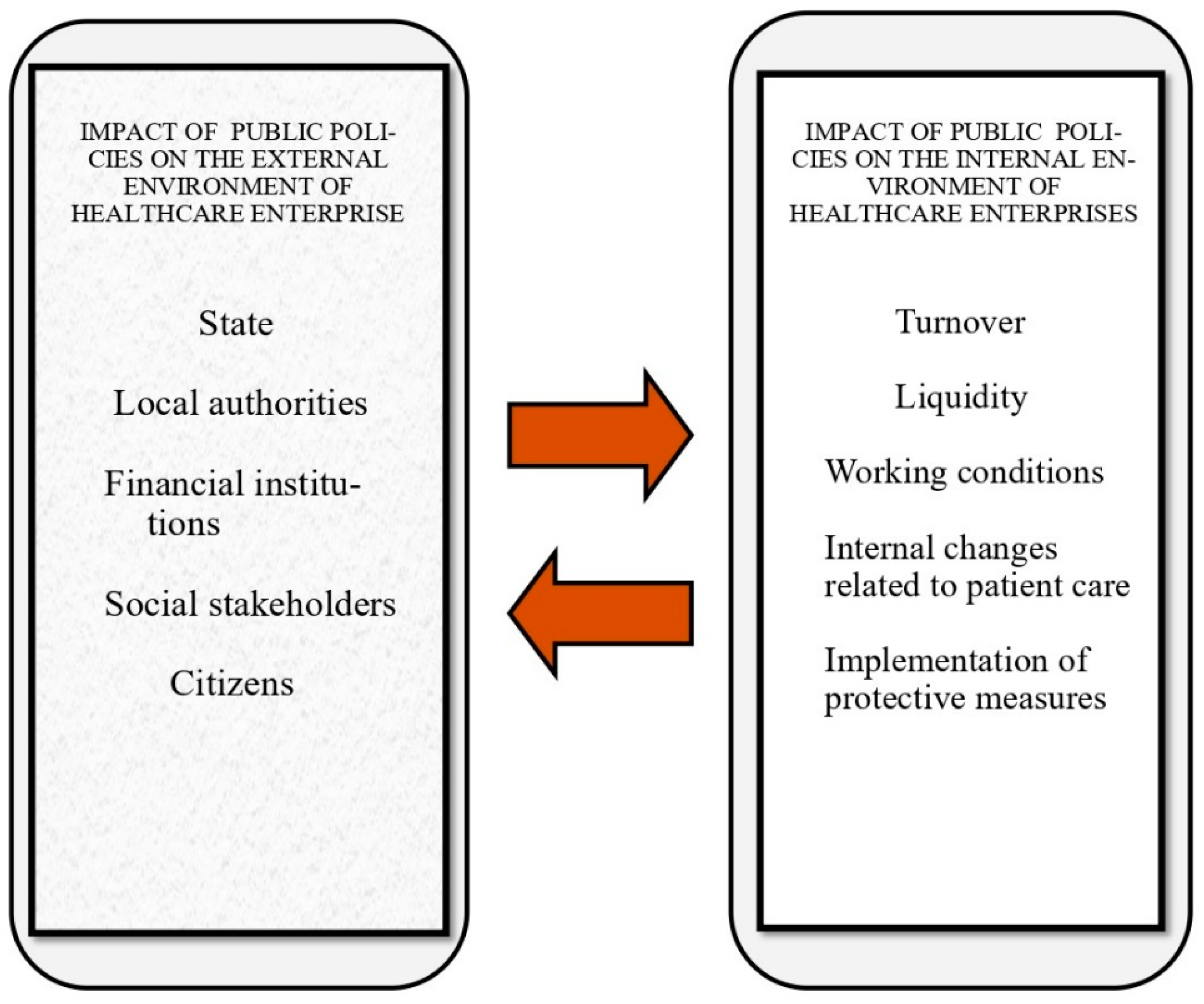
- Impact of public policies to contain the spread of COVID-19 on the external environment of healthcare enterprises in rural areas
“The protective measures taken by the government in view of the pandemic created several problems for our healthcare facility. The costs increased and it is impossible to cover our losses with the financial support provided by the state to enterprises”.(R10)
“Our cooperation with the local administration is ongoing on many issues, however regarding COVID-19 the local administration had limited power and small to minimal involvement with the private healthcare sector”.(R9)
“Right now a large amount of funding is provided in order to give the market a boost. What we don’t want is to be urged toward bank lending again, which is what happened during the financial crisis of 2009. Our experience with the banking system has been negative. The measures taken to support the enterprises must not include bank lending”.(R4)
“Our healthcare facility always had social objectives as well. We are in an ongoing cooperation with many social stakeholders. During COVID-19 we had several cases of individuals from vulnerable social groups sent to us for medical tests and treatment, and we were more than happy to deliver with no remuneration”.(R5)
“At first, before the enforcement of lockdown, business was becoming slow. People were reluctant to come to us for medical tests. But lately, that has changed. People started relaxing and they preferred the private sector as they considered it to be safer”(R3)
- Impact of public policies to contain the spread of COVID-19 on the internal environment of healthcare enterprises in rural areas
“The combination of services provided has changed. There has been a negative change in turnover during the first phase of the pandemic. Now the situation is constantly improving and our turnover is growing”(R8)
“During the COVID-19 pandemic our expenses increased in many areas. All the measures imposed had a financial cost which we carried entirely on our shoulders. In order to maintain our good reputation and the quality of our services, we had to accumulate financial losses. The liquidity problem has aggravated”(R12)
“The COVID-19 pandemic has impacted the working conditions. Our main concern is to prevent the spread of the virus, because there are so many people here. We took strict precautionary measures and our staff is now working in unfavorable conditions. The spread of the virus in our facility would be a disaster first and foremost because we will have human losses, but the investment will also collapse”(R7)
“Everything changed in the way we provide our services to the patients. We acted in strict accordance with the provisions concerning the measures of protection. The appointment is booked via telephone, we perform temperature controls, we keep the necessary distances, the use of mask is required and we are ready to perform Rapid Test”(R5)
“We follow reverently the measures aimed at protecting us from the pandemic and so far this has brought results, since we never had any confirmed COVID-19 case in the facility. The measures are followed both by our staff and out patients”(R9)
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Dajani, Haya, Hammad Akbar, Sara Carter, and Eleonor Shaw. 2019. Defying contextual embeddedness: Evidence from displaced women entrepreneurs in Jordan. Entrepreneurship and Regional Development 31: 198–212. [Google Scholar] [CrossRef]
- Anderson, Julia, Francesco Papadia, and Nicolas Véron. 2021. COVID-19 Credit Support Programs in Europe’s Five Largest Economies. Peterson Institute for International Economics Working Paper No. 21-6. Available online: https://ssrn.com/abstract=3826517 (accessed on 10 June 2021).
- Apostolopoulos, Nikolaos, Panagiotis Liargovas, Pantelis Sklias, and Sotiris Apostolopoulos. 2021a. Healthcare enterprises and public policies on COVID-19: Insights from the Greek rural areas. Strategic Change 30: 127–36. [Google Scholar] [CrossRef]
- Apostolopoulos, Nikolaos, Panagiotis Liargovas, Pantelis Sklias, Ilias Makris, and Sotiris Apostolopoulos. 2021b. Private healthcare entrepreneurship in a free-access public health system: What was the impact of the COVID-19 public policies? Journal of Entrepreneurship and Public Policy. (In press). [Google Scholar]
- Apostolopoulos, Nikolaos, Robert Newbery, and Menelaos Gkartzios. 2019. Social enterprise and community resilience: Examining a Greek response to turbulent times. Journal of Rural Studies 70: 215–24. [Google Scholar] [CrossRef] [Green Version]
- Bamias, Giorgos, Styliani Lagou, Michalis Gizis, George Karampekos, Konstantinos G. Kyriakoulis, Christos Pontas, and Gerassimos J. Mantzaris. 2020. The greek response to COVID-19: A true success story from an IBD perspective. Inflammatory Bowel Diseases 26: 1144–48. [Google Scholar] [CrossRef] [PubMed]
- Bartik, Alexander W., Marianne Bertrand, Zoe Cullen, Edward L. Glaeser, Michael Luca, and Christopher Stanton. 2020. The impact of COVID-19 on small business outcomes and expectations. Proceedings of the National Academy of Sciences 117: 17656–66. [Google Scholar] [CrossRef] [PubMed]
- Baxter, David, and Carter B. Casady. 2020. Proactive and strategic healthcare public-private partnerships (PPPs) in the coronavirus (COVID-19) epoch. Sustainability 12: 5097. [Google Scholar] [CrossRef]
- Bhattacharya, Sudip, Md Mahbub Hossain, and Amarjeet Singh. 2020. Addressing the shortage of personal protective equipment during the COVID-19 pandemic in India-A public health perspective. AIMS Public Health 7: 223. [Google Scholar] [CrossRef]
- Brülhart, Marius, Lalive Rafael, Tobias Lehmann, and Michael Siegenthaler. 2020. COVID-19 financial support to small businesses in Switzerland: Evaluation and outlook. Swiss Journal of Economics and Statistics 156: 1–13. [Google Scholar] [CrossRef]
- Cheong, Mark Wing Loong, Pascale Allotey, and Daniel D. Reidpath. 2020. Unequal Access to Vaccines Will Exacerbate Other Inequalities. Asia Pacific Journal of Public Health 32: 379–80. [Google Scholar] [CrossRef] [PubMed]
- Cirrincione, Luigi, Fulvio Plescia, Caterina Ledda, Venerando Rapisarda, Daniela Martorana, Raluca E. Moldovan, Kelly Theodoridou, and Emanuele Cannizzaro. 2020. COVID-19 pandemic: Prevention and protection measures to be adopted at the workplace. Sustainability 12: 3603. [Google Scholar] [CrossRef]
- Clouston, Sean A. P., Ginny Natale, and Bruce G. Link. 2021. Socioeconomic inequalities in the spread of coronavirus-19 in the United States: A examination of the emergence of social inequalities. Social Science and Medicine 268: 113554. [Google Scholar] [CrossRef]
- Coghlan, Niall, David Archard, Pippa Sipanoun, Thomas Hayes, and Behrad Baharlo. 2020. COVID-19: Legal implications for critical care. Anaesthesia 75: 1517–28. [Google Scholar] [CrossRef] [PubMed]
- Cope, Jason. 2005. Researching entrepreneurship through phenomenological inquiry: Philosophical and methodological issues. International Small Business Journal 23: 163–89. [Google Scholar] [CrossRef]
- Cousins, Sophie. 2020. COVID-19 has “devastating” effect on women and girls. The Lancet 396: 301–2. [Google Scholar] [CrossRef]
- Creswell, John W., and Cheryl N. Poth. 2016. Qualitative Inquiry and Research Design: Choosing among Five Approaches. New York: Sage Publications. [Google Scholar]
- Danielli, Shaun, Raman Patria, Patrice Donnelly, Hutan Ashrafian, and Ara Darzi. 2021. Economic interventions to ameliorate the impact of COVID-19 on the economy and health: An international comparison. Journal of Public Health 43: 42–46. [Google Scholar] [CrossRef]
- Dantas, Lucas Ogura, Rodrigo Py Gonçalves Barreto, and Cristine Homsi Jorge Ferreira. 2020. Digital physical therapy in the COVID-19 pandemic. Brazilian Journal of Physical Therapy 24: 381–83. [Google Scholar] [CrossRef] [PubMed]
- Deakin, Hannah, and Kelly Wakefield. 2014. Skype interviewing: Reflections of two PhD researchers. Qualitative Research 14: 603–16. [Google Scholar] [CrossRef]
- DeJonckheere, Melissa, and Lisa M. Vaughn. 2019. Semistructured interviewing in primary care research: A balance of relationship and rigour. Family Medicine and Community Health 7: e000057. [Google Scholar] [CrossRef] [Green Version]
- Di Lorenzo, Giuseppe, and Rossella Di Trolio. 2020. Coronavirus disease (COVID-19) in Italy: Analysis of risk factors and proposed remedial measures. Frontiers in Medicine 7: 140. [Google Scholar] [CrossRef] [Green Version]
- Dieckmann, Peter, Friis M. Susanne, Lippert Anne, and Doris Østergaard. 2012. Goals, success factors, and barriers for simulation-based learning: A qualitative interview study in health care. Simulation and Gaming 43: 627–47. [Google Scholar] [CrossRef]
- Donthu, Naveen, and Anders Gustafsson. 2020. Effects of COVID-19 on business and research. Journal of Business Research 117: 284. [Google Scholar] [CrossRef] [PubMed]
- Economou, Charalampos, Daphne Kaitelidou, Marina Karanikolos, and Anna Maresso. 2017. Greece: Health system review. Health Systems in Transition 19: 1–192. [Google Scholar]
- Farsalinos, Konstantinos, Konstantinos Poulas, Dimitrios Kouretas, Apostolos Vantarakis, Michalis Leotsinidis, Dimitrios Kouvelas, Anca O. Docea, Ronald Kostoff, Grigorios T. Gerotziafas, Michael N. Antoniou, and et al. 2021. Improved strategies to counter the COVID-19 pandemic: Lockdowns vs. primary and community healthcare. Toxicology Reports 8: 1–9. [Google Scholar] [CrossRef] [PubMed]
- Fossey, Ellie, Carol Harvey, Fiona McDermott, and Larry Davidson. 2002. Understanding and evaluating qualitative research. Australian and New Zealand Journal of Psychiatry 36: 717–32. [Google Scholar] [CrossRef] [PubMed]
- Fusch, Patricia I., and Lawrence R. Ness. 2015. Are we there yet? Data saturation in qualitative research. The Qualitative Report 20: 1408. [Google Scholar]
- Giannopoulou, Ioanna, and George O. Tsobanoglou. 2020. COVID-19 pandemic: Challenges and opportunities for the Greek health care system. Irish Journal of Psychological Medicine 37: 226–30. [Google Scholar] [CrossRef]
- Gioia, Dennis A., Kevin G. Corley, and Aimee L. Hamilton. 2013. Seeking qualitative rigor in inductive research: Notes on the Gioia methodology. Organizational Research Methods 16: 15–31. [Google Scholar] [CrossRef]
- Given, Lisa M., ed. 2008. The Sage Encyclopedia of Qualitative Research Methods. Los Angeles: Sage Publications, ISBN 978-1-4129-4163-1. [Google Scholar]
- Gountas, Ilias, Georgios Hillas, and Kyriakos Souliotis. 2020. Act early, save lives: Managing COVID-19 in Greece. Public Health 187: 136–39. [Google Scholar] [CrossRef]
- Govindan, Kannan, Hassan Mina, and Behrouz Alavi. 2020. A decision support system for demand management in healthcare supply chains considering the epidemic outbreaks: A case study of coronavirus disease 2019 (COVID-19). Transportation Research Part E: Logistics and Transportation Review 138: 101967. [Google Scholar] [CrossRef] [PubMed]
- Kathiravan, C., Padmaja Bhagavatham, V. Palanisamy, and A. Rajasekar. 2019. Influence of entrepreneurial creativity on competitive adnvantage in automobile engineering and technologies industries. International Journal of Advanced Science and Technology 27: 166–72. [Google Scholar]
- Kaye, Alan D., Chikezie N. Okeagu, Alex D. Pham, Rayce A. Silva, Joshua J. Hurley, Brett L. Arron, Noeen Sarfraz, Hong N. Lee, Ghali E. Ghali, Jack W. Gamble, and et al. 2020. Economic Impact of COVID-19 Pandemic on Health Care Facilities and Systems: International Perspectives. Best Practice and Research Clinical Anaesthesiology. [Google Scholar] [CrossRef]
- Kousi, Timokleia, Lefkothea-Christina Mitsi, and Jean Simos. 2021. The Early Stage of COVID-19 Outbreak in Greece: A Review of the National Response and the Socioeconomic Impact. International Journal of Environmental Research and Public Health 18: 322. [Google Scholar] [CrossRef] [PubMed]
- Kruse, Florien Margareth, and Patrick P. T. Jeurissen. 2020. For-profit hospitals out of business? Financial sustainability during the COVID-19 epidemic emergency response. International Journal of Health Policy and Management 9: 423. [Google Scholar] [CrossRef] [PubMed]
- Kuwahara, Keisuke, Ai Hori, Norio Ohmagari, and Tetsuya Mizoue. 2020. Early cases of COVID-19 in Tokyo and occupational health. Global Health and Medicine 2: 118–22. [Google Scholar] [CrossRef] [PubMed]
- Leite, Higor, Claire Lindsay, and Maneesh Kumar. 2020. COVID-19 outbreak: Implications on healthcare operations. The TQM Journal 33: 247–56. [Google Scholar] [CrossRef]
- Levi-Sanchez, Suzanne, and Sophie Toupin. 2014. New Social Media and Global Resistance. In Gender Matters in Global Politics: A Feminist Introduction to International Relations. London: Routledge, pp. 389–401. [Google Scholar]
- Liguori, Eric W., and Thomas G. Pittz. 2020. Strategies for small business: Surviving and thriving in the era of COVID-19. Journal of the International Council for Small Business 2: 106–10. [Google Scholar] [CrossRef]
- Liu, Zheng, Yawei Zhang, Xishan Wang, Daming Zhang, Dechang Diao, K. Chandramohan, and Christopher M. Booth. 2020. Recommendations for surgery during the novel coronavirus (COVID-19) epidemic. Indian Journal of Surgery 82: 124–28. [Google Scholar] [CrossRef]
- Lucaci, Ancuța, and Carmen Nastase. 2020. European Rural Businesses During The Covid-19 Pandemic: Designing Initiatives For Current And Future Development. LUMEN Proceedings 13: 419–29. [Google Scholar]
- Lystad, Reidar P., Benjamin T. Brown, Michael S. Swain, and Roger M. Engel. 2020. Impact of the COVID-19 pandemic on manual therapy service utilization within the Australian private healthcare setting. Healthcare 8: 558. [Google Scholar] [CrossRef] [PubMed]
- Maneesriwongul, Wantana, and Jane K. Dixon. 2004. Instrument translation process: A method review. Journal of Advanced Nursing 48: 175–86. [Google Scholar] [CrossRef]
- Matthews-Trigg, Nathaniel, David Citrin, Scott Halliday, Bibhav Acharya, Sheela Maru, Stephen Bezruchka, and Duncan Maru. 2019. Understanding perceptions of global healthcare experiences on provider values and practices in the USA: A qualitative study among global health physicians and program directors. BMJ Open 9: e026020. [Google Scholar] [CrossRef] [Green Version]
- McCracken, Grant. 1988. The Long Interview. New York: Sage. [Google Scholar]
- McFadden, Paula, Jana Ross, John Moriarty, John Mallett, Heike Schroder, Jermaine Ravalier, Jill Manthorpe, Denise Currie, Jaclyn Harron, and Patricia Gillen. 2021. The role of coping in the wellbeing and work-related quality of life of UK health and social care workers during COVID-19. International Journal of Environmental Research and Public Health 18: 815. [Google Scholar] [CrossRef]
- McIntosh, Michele J., and Janice M. Morse. 2015. Situating and constructing diversity in semi-structured interviews. Global Qualitative Nursing Research. [Google Scholar] [CrossRef] [PubMed]
- Menéndez, Uría. 2020. Spain’s response to Covid-19: Emergency measures; gradual relaxation. International Financial Law Review. Available online: https://www.iflr.com/article/b1lxmrrfr4gkfs/spains-response-to-covid19-emergency-measures-gradual-relaxation (accessed on 15 March 2021).
- Mitropoulos, Panagiotis, Kostas Kounetas, and Ioannis Mitropoulos. 2016. Factors affecting primary health care centers’ economic and production efficiency. Annals of Operations Research 247: 807–22. [Google Scholar] [CrossRef]
- Molliqaj, Granit, and Karl Schaller. 2020. How neurosurgeons are coping with COVID-19 and how it impacts our neurosurgical practice: Report from Geneva University Medical Center. World Neurosurgery 139: 624–27. [Google Scholar] [CrossRef]
- Moris, Dimitrios, and Dimitrios Schizas. 2020. Lockdown during COVID-19: The Greek success. In Vivo 34: 1695–99. [Google Scholar] [CrossRef] [PubMed]
- Moser, Albine, and Irene Korstjens. 2017. Series: Practical guidance to qualitative research. Part 1: Introduction. European Journal General Practice 23: 271–73. [Google Scholar] [CrossRef] [Green Version]
- Moser, Albine, and Irene Korstjens. 2018. Series: Practical guidance to qualitative research. Part 3: Sampling, data collection and analysis. European Journal of General Practice 24: 9–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musumeci, Maria Letizia, Maria Rita Nasca, and Giuseppe Micali. 2021. COVID-19: The Italian experience. Clinics in Dermatology. [Google Scholar] [CrossRef]
- Nicola, Maria, Zaid Alsafi, Catrin Sohrabi, Ahmed Kerwan, Ahmed Al-Jabir, Christos Iosifidis, Maliha Agha, and Riaz Agha. 2020. The socio-economic implications of the coronavirus and COVID-19 pandemic: A review. International Journal of Surgery 78: 185–93. [Google Scholar] [CrossRef]
- Nimako, Belinda Afriyie, Frank Baiden, and John Koku Awoonor-Williams. 2020. Towards effective participation of the private health sector in Ghana’s COVID-19 response. The Pan African Medical Journal 35: 47. [Google Scholar] [CrossRef]
- Norlyk, Annelise, and Ingegerd Harder. 2010. What makes a phenomenological study phenomenological? An analysis of peer-reviewed empirical nursing studies. Qualitative Health Research 20: 420–31. [Google Scholar] [CrossRef]
- Nouhjah, Sedigheh, and Shayesteh Jahanfar. 2020. Challenges of diabetes care management in developing countries with a high incidence of COVID-19: A brief report. Diabetes and Metabolic Syndrome: Clinical Research and Reviews 14: 731–32. [Google Scholar] [CrossRef]
- Ozturk, Ayce B., Ayce Baççıoğlu, Ozge Soyer, Ersoy Civelek, Bulent E. Şekerel, and Sevim Bavbek. 2021. Change in allergy practice during the COVID-19 pandemic. International Archives of Allergy and Immunology 182: 49–52. [Google Scholar] [CrossRef]
- Pang, Karl H., Diego M. Carrion, Juan G. Rivas, Guglielmo Mantica, Angelika Mattigk, Benjamin Pradere, Francesco Esperto, and European Society of Residents in Urology. 2020. The impact of COVID-19 on European health care and urology trainees. European Urology 78: 6–8. [Google Scholar] [CrossRef]
- Pappas, Takis S. 2014. Populist democracies: Post-authoritarian Greece and post-communist Hungary. Government and Opposition 49: 1–23. [Google Scholar] [CrossRef] [Green Version]
- Peine, Arne, Pia Paffenholz, Lucas Martin, Sandra Dohmen, Gernot Marx, and Sven H. Loosen. 2020. Telemedicine in Germany during the COVID-19 pandemic: Multi-professional national survey. Journal of Medical Internet Research 22: e19745. [Google Scholar] [CrossRef]
- Pelicioni, Paulo H. S., and Stephen R. Lord. 2020. COVID-19 will severely impact older people’s lives, and in many more ways than you think! Brazilian Journal of Physical Therapy 24: 293–94. [Google Scholar] [CrossRef]
- Petersen, Eskild, Daniel Lucey, Lucille Blumberg, Laura D. Kramer, Seif Al-Abri, Shui S. Lee, Tatiana C. A. Pinto, Christina W. Obiero, Alfonso J. Rodriguez-Morales, Richard Yapi, and et al. 2021. COVID-19 vaccines under the International Health Regulations–We must use the WHO International Certificate of Vaccination or Prophylaxis. International Journal of Infectious Diseases 104: 175–77. [Google Scholar] [CrossRef]
- Pinto, Fernandes T., and Celso R. F. de Carvalho. 2020. SARS CoV-2 (COVID-19): Lessons to be learned by Brazilian Physical Therapists. Brazilian Journal of Physical Therapy 24: 185. [Google Scholar] [CrossRef]
- Polit, Denise F., and Cheryl Tatano Beck. 2017. Nursing Research: Generating and Assessing Evidence for Nursing Practice, 10th ed. Philadelphia: Lippincott. [Google Scholar]
- Pringle, Jan, Charles Hendry, and Ella McLafferty. 2011. Phenomenological approaches: Challenges and choices. Nurse Researcher 18: 7–18. [Google Scholar] [CrossRef]
- Qu, Sandy Q., and John Dumay. 2011. The qualitative research interview. Qualitative Research in Accounting and Management 8: 238–64. [Google Scholar] [CrossRef]
- Ramírez de la Cruz, Edgar E., Eduardo J. Grin, Pablo Sanabria-Pulido, Daniel Cravacuore, and Arturo Orellana. 2020. The Transaction Costs of Government Responses to the COVID-19 Emergency in Latin America. Public Administration Review 80: 683–95. [Google Scholar] [CrossRef] [PubMed]
- Satiani, Bhagwan, Todd A. Zigrang, and Jessica L. Bailey-Wheaton. 2020. COVID-19 financial resources for physicians. Journal of Vascular Surgery 72: 1161–65. [Google Scholar] [CrossRef] [PubMed]
- Sethi, Ahmed B., Ahsan Sethi, Sadaf Ali, and Hira S. Aamir. 2020. Impact of Coronavirus disease (COVID-19) pandemic on health professionals. Pakistan Journal of Medical Sciences 36: 6–11. [Google Scholar] [CrossRef] [PubMed]
- Sharma, Gagan D., Gaurav Talan, Mrinalini Srivastava, Anshita Yadav, and Ritika Chopra. 2020. A qualitative enquiry into strategic and operational responses to Covid-19 challenges in South Asia. Journal of Public Affairs 20: e2195. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, Richard E., Jr., Brian S. Kuszyk, and Mahmud Mossa-Basha. 2021. Special report of the RSNA COVID-19 task force: The short-and long-term financial impact of the COVID-19 pandemic on private radiology practices. Radiology 298: 11–18. [Google Scholar] [CrossRef]
- Sheth, Jagdish. 2020. Business of business is more than business: Managing during the Covid crisis. Industrial Marketing Management 88: 261–64. [Google Scholar] [CrossRef]
- Siettos, Constantinos, Cleo Anastassopoulou, Constantinos Tsiamis, Georgia Vrioni, and Athanasios Tsakris. 2021. A bulletin from Greece: A health system under the pressure of the second COVID-19 wave. Pathogens and Global Health 115: 133–34. [Google Scholar] [CrossRef] [PubMed]
- Singh, Devendra. R., Dev R. Sunuwar, Sunil K. Shah, Kshitij Karki, Lalita K. Sah, Bipin Adhikari, and Rajeeb K. Sah. 2021. Impact of COVID-19 on health services utilization in Province-2 of Nepal: A qualitative study among community members and stakeholders. BMC Health Services Research 21: 1–14. [Google Scholar] [CrossRef]
- Tandon, Ajay, Tomas Roubal, Lacklan McDonald, Peter Cowley, Toomas Palu, Valeria O. Cruz, Patrick Eozenou, Jewelwayne Cain, Hui S. Teo, Martin Schmidt, and et al. 2020. Economic Impact of COVID-19: Implications for Health Financing in Asia and Pacific. Health, Nutrition and Population Discussion Paper. Washington, DC: World Bank. ©World Bank, Available online: https://openknowledge.worldbank.org/handle/10986/34572 (accessed on 10 June 2021).
- Temple, Bogusia, and Alys Young. 2004. Qualitative research and translation dilemmas. Qualitative Research 4: 161–78. [Google Scholar] [CrossRef]
- Thomas, Brian, and Swaroopa Chackole. 2021. Economic Impacts Of Covid 19. European Journal of Molecular and Clinical Medicine 7: 5812–19. [Google Scholar]
- Thomas, Sandra P., and Howard R. Pollio. 2002. Listening to Patients: A Phenomenological Approach to Nursing Research and Practice. Berlin/Heidelberg: Springer. [Google Scholar]
- Thorne, Sally. 1997. The art (and science) of critiquing qualitative research. In Completing a Qualitative Project: Details and Dialogue. Edited by J. M. Morse. Thousand Oaks: Sage, pp. 117–32. [Google Scholar]
- Tountas, Yannis, Nikolaos Oikonomou, Georgia Pallikarona, Christine Dimitrakaki, Chara Tzavara, Kyriakos Souliotis, Anargiros Mariolis, Evelina Pappa, Nick Kontodimopoulos, and Dimitris Niakas. 2011. Sociodemographic and socioeconomic determinants of health services utilisation in Greece: The Hellas Health I study. Health Service Management Research 24: 8–18. [Google Scholar] [CrossRef]
- Van Burg, Elco, Joep Cornelissen, Wouter Stam, and Sarah Jack. 2020. Advancing Qualitative Entrepreneurship Research: Leveraging Methodological Plurality for Achieving Scholarly Impact. Entrepreneurship Theory and Practice. [Google Scholar] [CrossRef]
- Van der Walt, Johannes L. 2020. Interpretivism-Constructivism as a Research Method in the Humanities and Social Sciences–More to It Than Meets the Eye. International Journal 8: 59–68. [Google Scholar]
- Van Nes, Fenna, Tineke Abma, Hans Jonsson, and Dorly Deeg. 2010. Language differences in qualitative research: Is meaning lost in translation? European Journal of Ageing 7: 313–16. [Google Scholar] [CrossRef] [Green Version]
- Vardiampasis, Vasileios, Maria Tsironi, M. Athanasios Nikolentzo, Ioannis Moisoglou, Petros Galanis, Helen Stavropoulou, Georgia Athanasopoulou, and Panagiotis Prezerakos. 2014. Health services staffing with physicians in the remote areas: Recruitment and retention incentives. Archives of Hellenic Medicine/Arheia Ellenikes Iatrikes 31: 48–54. [Google Scholar]
- Vasilopoulou, Sofia, Daphne Halikiopoulou, and Theofanis Exadaktylos. 2014. Greece in Crisis: Austerity, Populism and the Politics of Blame. JCMS: Journal of Common Market Studies 52: 388–402. [Google Scholar]
- Whiting, Lisa. 2001. Analysis of phenomenological data: Personal reflections on Giorgi’s method. Nurse Researcher (Through 2013) 9: 60. [Google Scholar] [CrossRef] [PubMed]
- Williams, David Owain, Ka Chun Yung, and Karen A. Grépin. 2021. The failure of private health services: COVID-19 induced crises in low-and middle-income country (LMIC) health systems. Global Public Health 16: 1–14. [Google Scholar]
- Williams, Elizabeth Nutt, and Susan L. Morrow. 2009. Achieving trustworthiness in qualitative research: A pan-paradigmatic perspective. Psychotherapy Research 19: 576–82. [Google Scholar] [CrossRef] [PubMed]
- Williams, Owain D. 2020. COVID-19 and Private Health: Market and Governance Failure. Development 63: 181–90. [Google Scholar] [CrossRef] [PubMed]
- Wright, Carl. 2020. Local government fighting Covid-19. The Round Table 109: 338–39. [Google Scholar] [CrossRef]
- Wu, Kevin Y., David T. Wu, Thomas T. Nguyen, and Simon D. Tran. 2020. COVID-19’s impact on private practice and academic dentistry in North America. Oral Diseases 27: 684–87. [Google Scholar] [CrossRef]
- Yin, Robert K. 1994. Discovering the future of the case study. Method in Evaluation Research. Evaluation Practice 15: 283–29. [Google Scholar]


{kind=link}
| Enterprise | Year of Establishment | Number of Employees | Type of Enterprise |
|---|---|---|---|
| R1 | 1983 | 2 | Physiotherapy Center |
| R2 | 1996 | 1 | Speech Therapy and Counseling Center |
| R3 | 2010 | 5 | Diagnostic and Microbiological Center |
| R4 | 1982 | 1 | Cardiology Center |
| R5 | 2010 | 120 | Rehabilitation and Recovery Center |
| R6 | 1997 | 10 | Diagnostic Center |
| R7 | 2012 | 70 | Mental Health Clinic |
| R8 | 2003 | 2 | Pharmacy |
| R9 | 2020 | 33 | Polyclinic |
| R10 | 1991 | 3 | Physiotherapy Center |
| R11 | 2005 | 5 | Diagnostic and Microbiological Center |
| R12 | 2007 | 7 | Medical and dental care center |
| External business environment | In relation to the state |
|
| In relation to the local administration |
| |
| In relation to the financial institutions as a result of public government policies |
| |
| In relation to the social stakeholders |
| |
| In relation to the citizens |
| |
| Internal business environment | In relation to its turnover |
|
| In relation to liquidity |
| |
| In relation to working conditions |
| |
| In relation to the internal changes in patient care |
| |
| In relation to the protective measures taken |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Apostolopoulos, N.; Apostolopoulos, S.; Makris, I.; Stavroyiannis, S. Rural Healthcare Enterprises in the Vortex of COVID-19: The Impact of Public Policies on the Internal and External Environment. Adm. Sci. 2021, 11, 82. https://doi.org/10.3390/admsci11030082
Apostolopoulos N, Apostolopoulos S, Makris I, Stavroyiannis S. Rural Healthcare Enterprises in the Vortex of COVID-19: The Impact of Public Policies on the Internal and External Environment. Administrative Sciences. 2021; 11(3):82. https://doi.org/10.3390/admsci11030082
Chicago/Turabian StyleApostolopoulos, Nikolaos, Sotiris Apostolopoulos, Ilias Makris, and Stavros Stavroyiannis. 2021. "Rural Healthcare Enterprises in the Vortex of COVID-19: The Impact of Public Policies on the Internal and External Environment" Administrative Sciences 11, no. 3: 82. https://doi.org/10.3390/admsci11030082