
Risk-Perception Change Associated with COVID-19 Vaccine’s Side Effects: The Role of Individual Differences

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
1.1. Conspiracy Theories
1.2. Cognitive Style
1.3. Risk-Perception
2. Materials and Methods
2.1. Aims
2.2. Procedure
2.3. Participants
2.4. Measures
2.5. Analytic Plan
3. Results
3.1. Reliability Analysis
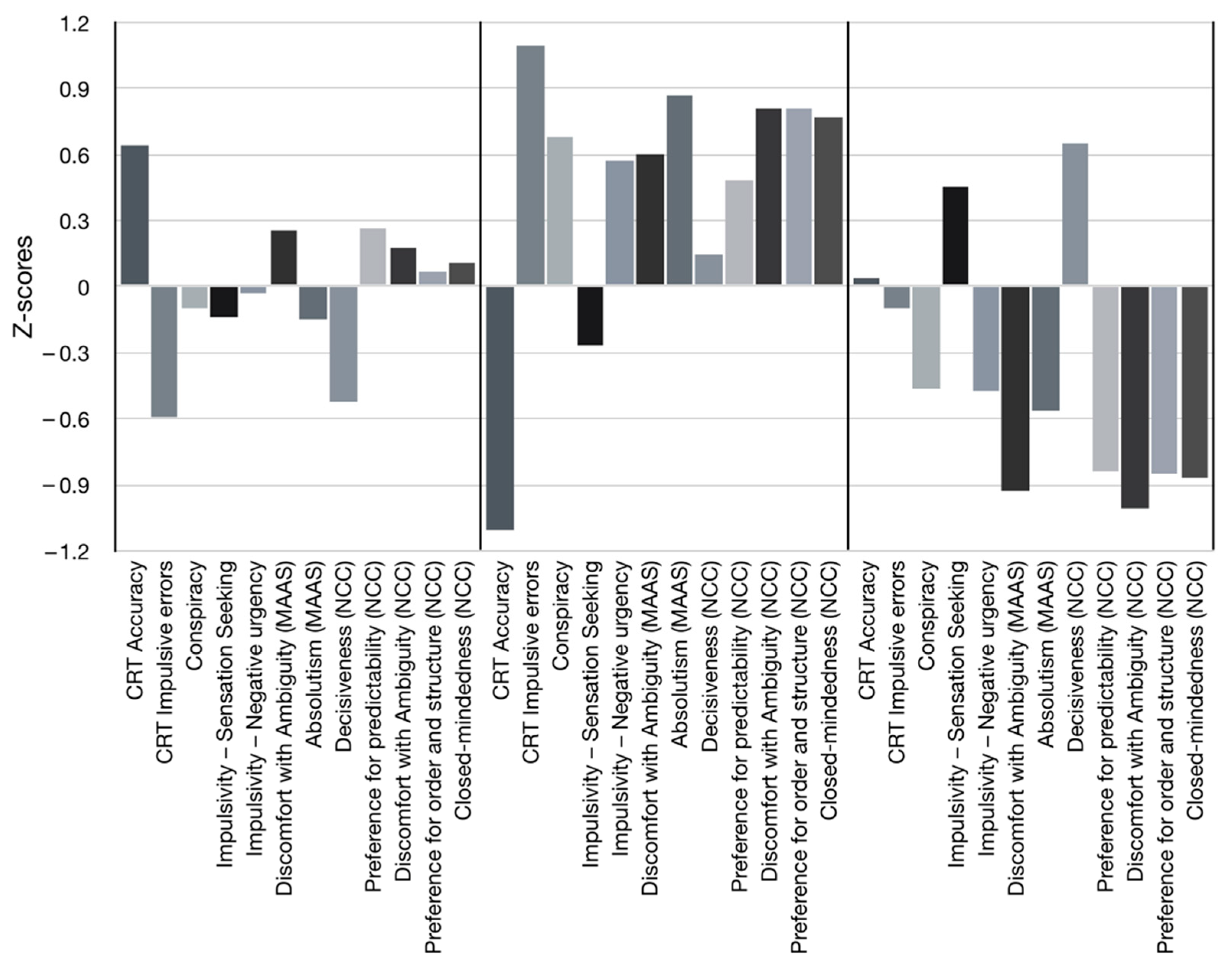
3.2. Cluster Analysis
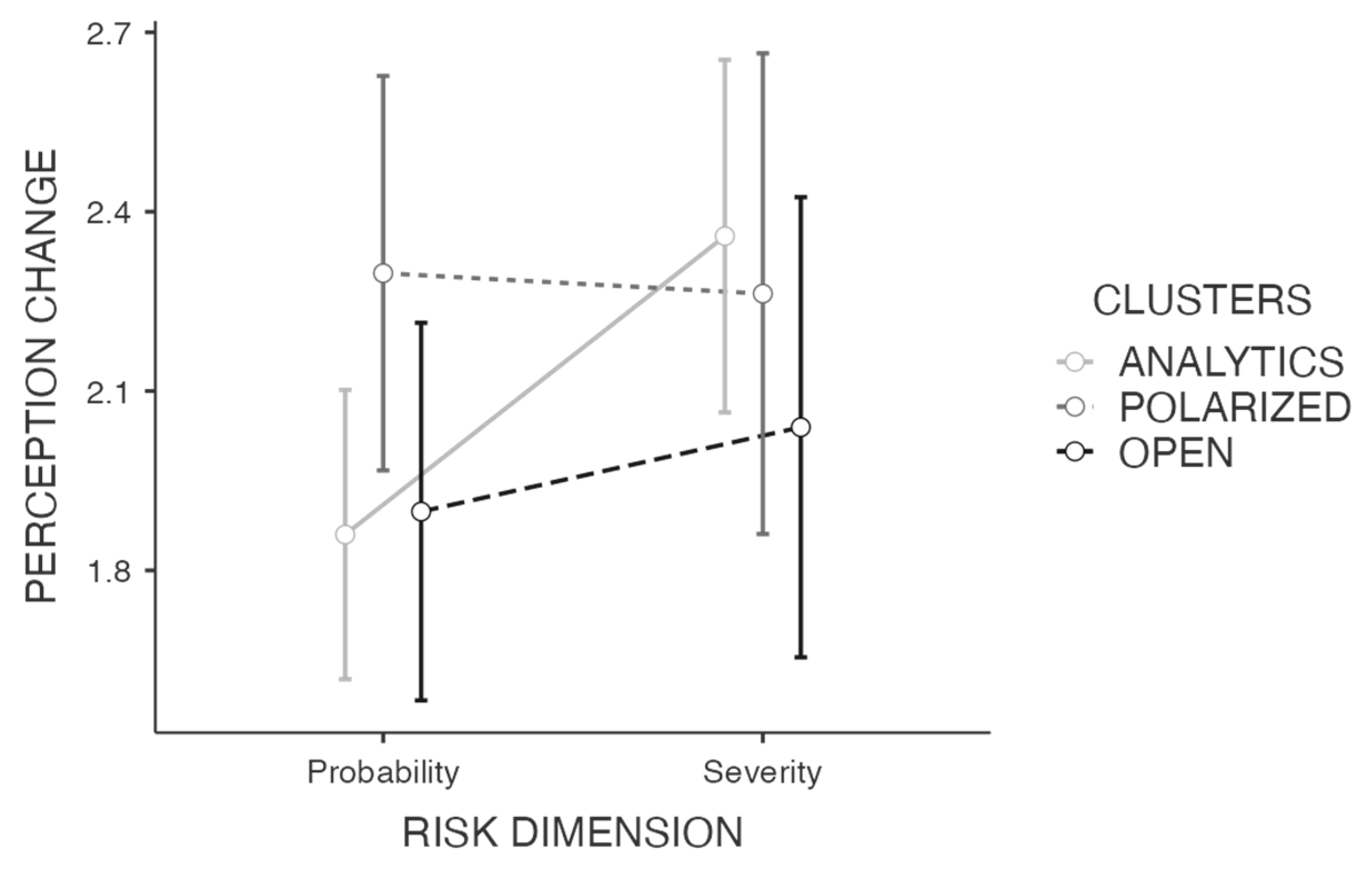
3.3. Risk-Perception Change
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cerami, C.; Santi, G.C.; Galandra, C.; Dodich, A.; Cappa, S.F.; Vecchi, T.; Crespi, C. COVID-19 Outbreak In Italy: Are We Ready for the Psychosocial and the Economic Crisis? Baseline Findings From the PsyCovid Study. Front. Psychiatry 2020, 11, 556. [Google Scholar] [CrossRef] [PubMed]
- AIFA Rapporto Sulla Sorveglianza dei Vaccini COVID-19 27/12/2020–26/08/2021. Available online: https://www.aifa.gov.it/%0D%0Adocuments/20142/1315190/Rapporto_sorveglianza_vaccini_COVID-19_6.pdf%0D%0A (accessed on 18 November 2021).
- de Sousa, Á.F.L.; Teixeira, J.R.B.; Lua, I.; de Oliveira Souza, F.; Ferreira, A.J.F.; Schneider, G.; de Carvalho, H.E.F.; de Oliveira, L.B.; Lima, S.V.M.A.; de Sousa, A.R.; et al. Determinants of COVID-19 Vaccine Hesitancy in Portuguese-Speaking Countries: A Structural Equations Modeling Approach. Vaccines 2021, 9, 1167. [Google Scholar] [CrossRef]
- Schaffer DeRoo, S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 Vaccination Program. JAMA 2020, 323, 2458–2459. [Google Scholar] [CrossRef] [PubMed]
- Guidry, J.P.; Laestadius, L.I.; Vraga, E.K.; Miller, C.A.; Perrin, P.B.; Burton, C.W.; Ryan, M.; Fuemmeler, B.F.; Carlyle, K.E. Willingness to get the COVID-19 vaccine with and without emergency use authorization. Am. J. Infect. Control 2021, 49, 137–142. [Google Scholar] [CrossRef]
- Palamenghi, L.; Barello, S.; Boccia, S.; Graffigna, G. Mistrust in biomedical research and vaccine hesitancy: The forefront challenge in the battle against COVID-19 in Italy. Eur. J. Epidemiol. 2020, 35, 785–788. [Google Scholar] [CrossRef]
- Salvi, C.; Iannello, P.; McClay, M.; Rago, S.; Dunsmoor, J.E.; Antonietti, A. Going Viral: How Fear, Socio-Cognitive Polarization and Problem-Solving Influence Fake News Detection and Proliferation During COVID-19 Pandemic. Front. Commun. 2021, 5, 16. [Google Scholar] [CrossRef]
- Romer, D.; Jamieson, K.H. Conspiracy theories as barriers to controlling the spread of COVID-19 in the U.S. Soc. Sci. Med. 2020, 263, 113356. [Google Scholar] [CrossRef]
- Douglas, K.M.; Uscinski, J.E.; Sutton, R.M.; Cichocka, A.; Nefes, T.; Ang, C.S.; Deravi, F. Understanding conspiracy theories. Political Psychol. 2019, 40, 3–35. [Google Scholar] [CrossRef] [Green Version]
- Marinthe, G.; Brown, G.; Delouvée, S.; Jolley, D. Looking out for myself: Exploring the relationship between conspiracy mentality, perceived personal risk, and COVID-19 prevention measures. Br. J. Health Psychol. 2020, 25, 957–980. [Google Scholar] [CrossRef] [PubMed]
- Shahsavari, S.; Holur, P.; Wang, T.; Tangherlini, T.R.; Roychowdhury, V. Conspiracy in the time of corona: Automatic detection of emerging COVID-19 conspiracy theories in social media and the news. J. Comput. Soc. Sci. 2020, 3, 279–317. [Google Scholar] [CrossRef]
- Havey, N.F. Partisan public health: How does political ideology influence support for COVID-19 related misinformation? J. Comput. Soc. Sci. 2020, 3, 319–342. [Google Scholar] [CrossRef] [PubMed]
- Latkin, C.A.; Dayton, L.; Moran, M.; Strickland, J.C.; Collins, K. Behavioral and psychosocial factors associated with COVID-19 skepticism in the United States. Curr. Psychol. 2021, 1–9. [Google Scholar] [CrossRef]
- Simione, L.; Vagni, M.; Gnagnarella, C.; Bersani, G.; Pajardi, D. Mistrust and beliefs in conspiracy theories differently mediate the effects of psychological factors on propensity for COVID-19 vaccine. Front. Psychol. 2021, 12, 683684. [Google Scholar] [CrossRef] [PubMed]
- Allington, D.; Duffy, B.; Wessely, S.; Dhavan, N.; Rubin, J. Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency. Psychol. Med. 2021, 51, 1763–1769. [Google Scholar] [CrossRef] [PubMed]
- Bierwiaczonek, K.; Kunst, J.R.; Pich, O. Belief in COVID-19 conspiracy theories reduces social distancing over time. Appl. Psychol. Health Well-Being 2020, 12, 1270–1285. [Google Scholar] [CrossRef]
- Winter, K.; Pummerer, L.; Hornsey, M.J.; Sassenberg, K. Pro-vaccination subjective norms moderate the relationship between conspiracy mentality and vaccination intentions. Br. J. Health Psychol. 2021. [Google Scholar] [CrossRef]
- Motta, M. The dynamics and political implications of anti-intellectualism in the United States. Am. Politics Res. 2018, 46, 465–498. [Google Scholar] [CrossRef]
- Merkley, E.; Bridgman, A.; Loewen, P.J.; Owen, T.; Ruths, D.; Zhilin, O. A rare moment of cross-partisan consensus: Elite and public response to the COVID-19 pandemic in Canada. Can. J. Political Sci. 2020, 53, 311–318. [Google Scholar] [CrossRef] [Green Version]
- Pivetti, M.; Melotti, G.; Bonomo, M.; Hakoköngäs, E. Conspiracy Beliefs and Acceptance of COVID-Vaccine: An Exploratory Study in Italy. Soc. Sci. 2021, 10, 108. [Google Scholar] [CrossRef]
- Miller, J.M.; Saunders, K.L.; Farhart, C.E. Conspiracy endorsement as motivated reasoning: The moderating roles of political knowledge and trust. Am. J. Political Sci. 2016, 60, 824–844. [Google Scholar] [CrossRef] [Green Version]
- Kata, A. A postmodern Pandora’s box: Anti-vaccination misinformation on the Internet. Vaccine 2010, 28, 1709–1716. [Google Scholar] [CrossRef]
- Plohl, N.; Musil, B. Modeling compliance with COVID-19 prevention guidelines: The critical role of trust in science. Psychol. Health Med. 2021, 26, 1–12. [Google Scholar] [CrossRef]
- Evans, J.S.B.T. Dual-processing accounts of reasoning, judgment, and social cognition. Annu. Rev. Psychol. 2008, 59, 255–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberali, J.M.; Reyna, V.F.; Furlan, S.; Stein, L.M.; Pardo, S.T. Individual Differences in Numeracy and Cognitive Reflection, with Implications for Biases and Fallacies in Probability Judgment. J. Behav. Decis. Mak. 2012, 25, 361–381. [Google Scholar] [CrossRef] [PubMed]
- Čavojová, V.; Šrol, J.; Ballová Mikušková, E. How scientific reasoning correlates with health-related beliefs and behaviors during the COVID-19 pandemic? J. Health Psychol. 2020, 1359105320962266. [Google Scholar] [CrossRef]
- Fasce, A.; Picó, A. Science as a vaccine. Sci. Educ. 2019, 28, 109–125. [Google Scholar] [CrossRef]
- Tomljenovic, H.; Bubic, A.; Erceg, N. Contribution of rationality to vaccine attitudes: Testing two hypotheses. J. Behav. Decis. Mak. 2021. [Google Scholar] [CrossRef]
- Patton, J.H.; Stanford, M.S.; Barratt, E.S. Factor structure of the Barratt impulsiveness scale. J. Clin. Psychol. 1995, 51, 768–774. [Google Scholar] [CrossRef]
- Granö, N.; Virtanen, M.; Vahtera, J.; Elovainio, M.; Kivimäki, M. Impulsivity as a predictor of smoking and alcohol consumption. Personal. Individ. Differ. 2004, 37, 1693–1700. [Google Scholar] [CrossRef]
- Alper, S.; Bayrak, F.; Yilmaz, O. Psychological correlates of COVID-19 conspiracy beliefs and preventive measures: Evidence from Turkey. Curr. Psychol. 2020, 40, 5708–5717. [Google Scholar] [CrossRef]
- Browne, M.; Thomson, P.; Rockloff, M.J.; Pennycook, G. Going against the Herd: Psychological and Cultural Factors Underlying the “Vaccination Confidence Gap”. PLoS ONE 2015, 10, e0132562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pennycook, G.; Fugelsang, J.A.; Koehler, D.J. Everyday consequences of analytic thinking. Curr. Dir. Psychol. Sci. 2015, 24, 425–432. [Google Scholar] [CrossRef] [Green Version]
- Bronstein, M.V.; Pennycook, G.; Bear, A.; Rand, D.G.; Cannon, T.D. Belief in fake news is associated with delusionality, dogmatism, religious fundamentalism, and reduced analytic thinking. J. Appl. Res. Mem. Cogn. 2019, 8, 108–117. [Google Scholar] [CrossRef]
- Budner, S. Intolerance of ambiguity as a personality variable. J. Personal. 1962, 30, 29–50. [Google Scholar] [CrossRef]
- Furnham, A.; Ribchester, T. Tolerance of ambiguity: A review of the concept, its measurement and applications. Curr. Psychol. 1995, 14, 179–199. [Google Scholar] [CrossRef]
- Iannello, P.; Mottini, A.; Tirelli, S.; Riva, S.; Antonietti, A. Ambiguity and uncertainty tolerance, need for cognition, and their association with stress. A study among Italian practicing physicians. Med. Educ. Online 2017, 22, 1270009. [Google Scholar]
- Petrocchi, S.; Iannello, P.; Ongaro, G.; Antonietti, A.; Pravettoni, G. The interplay between risk and protective factors during the initial height of the COVID-19 crisis in Italy: The role of risk aversion and intolerance of ambiguity on distress. Curr. Psychol. 2021, 41, 437–448. [Google Scholar] [CrossRef]
- Endler, N.S.; Speer, R.L.; Johnson, J.M.; Flett, G.L. Controllability, coping, efficacy, and distress. Eur. J. Personal. 2000, 14, 245–264. [Google Scholar] [CrossRef]
- Webster, D.M.; Kruglanski, A.W. Individual differences in need for cognitive closure. J. Personal. Soc. Psychol. 1994, 67, 1049–1062. [Google Scholar] [CrossRef]
- Berenbaum, H.; Bredemeier, K.; Thompson, R.J. Intolerance of uncertainty: Exploring its dimensionality and associations with need for cognitive closure, psychopathology, and personality. J. Anxiety Disord. 2008, 22, 117–125. [Google Scholar] [CrossRef]
- Roets, A.; Kruglanski, A.W.; Kossowska, M.; Pierro, A.; Hong, Y. The motivated gatekeeper of our minds: New directions in need for closure theory and research. In Advances in Experimental Social Psychology; Elsevier: Amsterdam, The Netherlands, 2015; pp. 221–283. [Google Scholar]
- Roets, A.; Van Hiel, A. Why some hate to dilly-dally and others do not: The arousal-invoking capacity of decision-making for low-and high-scoring need for closure individuals. Soc. Cogn. 2008, 26, 333–346. [Google Scholar] [CrossRef]
- White, H.A. Need for cognitive closure predicts stress and anxiety of college students during COVID-19 pandemic. Personal. Individ. Differ. 2022, 187, 111393. [Google Scholar] [CrossRef]
- Caligiuri, P.; Tarique, I. Dynamic cross-cultural competencies and global leadership effectiveness. J. World Bus. 2012, 47, 612–622. [Google Scholar] [CrossRef]
- Schumpe, B.M.; Brizi, A.; Giacomantonio, M.; Panno, A.; Kopetz, C.; Kosta, M.; Mannetti, L. Need for cognitive closure decreases risk taking and motivates discounting of delayed rewards. Personal. Individ. Differ. 2017, 107, 66–71. [Google Scholar] [CrossRef]
- Lauriola, M.; Levin, I.P.; Hart, S.S. Common and distinct factors in decision making under ambiguity and risk: A psychometric study of individual differences. Organ. Behav. Hum. Decis. Process. 2007, 104, 130–149. [Google Scholar] [CrossRef]
- Peters, E.; Slovic, P. The springs of action: Affective and analytical information processing in choice. Personal. Soc. Psychol. Bull. 2000, 26, 1465–1475. [Google Scholar] [CrossRef]
- Brewer, N.T.; Chapman, G.B.; Gibbons, F.X.; Gerrard, M.; McCaul, K.D.; Weinstein, N.D. Meta-analysis of the relationship between risk perception and health behavior: The example of vaccination. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2007, 26, 136–145. [Google Scholar] [CrossRef] [Green Version]
- Lowrance, W.W. Of Acceptable Risk: Science and the Determination of Safety; William Kaufmann, Inc.: Los Altos, CA, USA, 1976. [Google Scholar]
- Aven, T. On some recent definitions and analysis frameworks for risk, vulnerability, and resilience. Risk Anal. 2011, 31, 515–522. [Google Scholar] [CrossRef]
- Slovic, P.; Peters, E. Risk perception and affect. Curr. Dir. Psychol. Sci. 2006, 15, 322–325. [Google Scholar] [CrossRef]
- Lichtenstein, S.; Slovic PFischhoo¤, B.; Layman, M.; Combs, B. Judged Frequency of Lethal Events. J. Exp. Psychol. Hum. Learn. Mem. 1978, 4, 551–578. [Google Scholar] [CrossRef]
- Slovic, P.; Finucane, M.L.; Peters, E.; MacGregor, D.G. Risk as analysis and risk as feelings: Some thoughts about affect, reason, risk, and rationality. Risk Anal. 2004, 24, 311–322. [Google Scholar] [CrossRef]
- Tversky, A.; Kahneman, D. Judgment under Uncertainty: Heuristics and Biases. Science 1974, 185, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Frederick, S. Cognitive reflection and decision making. J. Econ. Perspect. 2005, 19, 25–42. [Google Scholar] [CrossRef] [Green Version]
- D’Orta, I.; Burnay, J.; Aiello, D.; Niolu, C.; Siracusano, A.; Timpanaro, L.; Khazaal, Y.; Billieux, J. Development and validation of a short Italian UPPS-P Impulsive Behavior Scale. Addict. Behav. Rep. 2015, 2, 19–22. [Google Scholar] [CrossRef]
- Pierro, A.; Mannetti, L.; Garsia, V.; Miglietta, A.; Converso, D.; Ravenna, M.; Rubini, M. Caratteristiche strutturali della versione italiana della Scala di Bisogno di Chiusura (di Webster & Kruglanski). Inst. Res. Inf. Syst. 1995, 2, 3–4. [Google Scholar]
- Lauriola, M.; Foschi, R.; Mosca, O.; Weller, J. Attitude Toward Ambiguity: Empirically Robust Factors in Self-Report Personality Scales. Assessment 2016, 23, 353–373. [Google Scholar] [CrossRef]
- Faisal, R.A.; Jobe, M.C.; Ahmed, O.; Sharker, T. Replication analysis of the COVID-19 Worry Scale. Death Stud. 2020, 1–7. [Google Scholar] [CrossRef]
- Brotherton, R.; French, C.C.; Pickering, A.D. Measuring belief in conspiracy theories: The generic conspiracist beliefs scale. Front. Psychol. 2013, 4, 279. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.I. A concordance correlation coefficient to evaluate reproducibility. Biometrics 1989, 45, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Swami, V.; Voracek, M.; Stieger, S.; Tran, U.S.; Furnham, A. Analytic thinking reduces belief in conspiracy theories. Cognition 2014, 133, 572–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobato, E.; Mendoza, J.; Sims, V.; Chin, M. Examining the relationship between conspiracy theories, paranormal beliefs, and pseudoscience acceptance among a university population. Appl. Cogn. Psychol. 2014, 28, 617–625. [Google Scholar] [CrossRef]
- Adorno, T.W. The Autoritarian Personality; Harper & Brothers: New York, NY, USA, 1950. [Google Scholar]
- Costa, P.T., Jr.; McCrae, R.R. Four ways five factors are basic. Personal. Individ. Differ. 1992, 13, 653–665. [Google Scholar] [CrossRef]
- Zuckerman, M. Sensation seeking and risk taking. In Emotions in Personality and Psychopathology; Springer: Berlin/Heidelberg, Germany, 1979; pp. 161–197. [Google Scholar]
- Kellermann, K.; Reynolds, R. When ignorance is bliss: The role of motivation to reduce uncertainty in uncertainty reduction theory. Hum. Commun. Res. 1990, 17, 5–75. [Google Scholar] [CrossRef]
- Neuberg, S.L.; West, S.G.; Judice, T.N.; Thompson, M.M. On dimensionality, discriminant validity, and the role of psychometric analyses in personality theory and measurement: Reply to Kruglanski et al.’s (1997) defense of the Need for Closure Scale. J. Personal. Soc. Psychol. 1997, 73, 1017–1029. [Google Scholar] [CrossRef]
- Litman, J.A. Relationships between measures of I-and D-type curiosity, ambiguity tolerance, and need for closure: An initial test of the wanting-liking model of information-seeking. Personal. Individ. Differ. 2010, 48, 397–402. [Google Scholar] [CrossRef]
- Slovic, P.; Lichtenstein, S.; Fischhoff, B. Images of disaster: Perception and acceptance of risks from nuclear power. In Energy Risk Management; Goodman, G., Rowe, W., Eds.; Academic: London, UK, 1979; pp. 223–245. [Google Scholar]
- Sjoberg, L. Consequences of perceived risk: Demand for mitigation. J. Risk Res. 1999, 2, 129–149. [Google Scholar] [CrossRef]
- Hakes, J.K.; Viscusi, W.K. Dead reckoning: Demographic determinants of the accuracy of mortality risk perceptions. Risk Anal. 2004, 24, 651–664. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, C.; Dunning, D. Jumping to conclusions: Implications for reasoning errors, false belief, knowledge corruption, and impeded learning. J. Personal. Soc. Psychol. 2021, 120, 789–815. [Google Scholar] [CrossRef]
- Pytlik, N.; Soll, D.; Mehl, S. Thinking Preferences and Conspiracy Belief: Intuitive Thinking and the Jumping to Conclusions-Bias as a Basis for the Belief in Conspiracy Theories. Front. Psychiatry 2020, 11, 568942. [Google Scholar] [CrossRef] [PubMed]
- Belhekar, V.M. Cognitive and non-cognitive determinants of heuristics of judgment and decision-making: General ability and personality traits. J. Indian Acad. Appl. Psychol. 2017, 43, 75. [Google Scholar]
- Oh, S.-H.; Paek, H.-J.; Hove, T. Cognitive and emotional dimensions of perceived risk characteristics, genre-specific media effects, and risk perceptions: The case of H1N1 influenza in South Korea. Asian J. Commun. 2015, 25, 14–32. [Google Scholar] [CrossRef]
- Slovic, P.; Finucane, M.; Peters, E.; MacGregor, D.G. The Affect Heuristic in Judgement of Risks and Benefits. J. Behav. Decis. Mak. 2000, 13, 1–17. [Google Scholar]
- Schmelz, K.; Bowles, S. Overcoming COVID-19 vaccination resistance when alternative policies affect the dynamics of conformism, social norms, and crowding out. Proc. Natl. Acad. Sci. USA 2021, 118, e2104912118. [Google Scholar] [CrossRef]
- Sata Shanka, M.; Moges Menebo, M. When and How Trust in Government Leads to Compliance towards COVID-19 Precautionary Measures. J. Bus. Res. 2021. [Google Scholar] [CrossRef]
- Konstantinou, P.; Georgiou, K.; Kumar, N.; Kyprianidou, M.; Nicolaides, C.; Karekla, M.; Kassianos, A. Transmission of Vaccination Attitudes and Uptake Based on Social Contagion Theory: A Scoping Review. Vaccines 2021, 9, 607. [Google Scholar] [CrossRef]
- Shrader-Frechette, K.S. Perceived risks versus actual risks: Managing hazards through negotiation. Risk 1990, 1, 341. [Google Scholar]
- Iachini, T.; Frassinetti, F.; Ruotolo, F.; Sbordone, F.; Ferrara, A.; Arioli, M.; Pazzaglia, F.; Bosco, A.; Candini, M.; Lopez, A.; et al. Social Distance during the COVID-19 Pandemic Reflects Perceived Rather Than Actual Risk. Int J. Environ. Res. Public Health 2021, 18, 5504. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Age (M, SD) | 30.2 | 13.0 |
| Gender | ||
| Male | 29 | 36.7 |
| Female | 50 | 63.3 |
| Educational level | ||
| Middle school | 1 | 1.2 |
| High school | 28 | 35.4 |
| Bachelor’s degree | 21 | 26.6 |
| Graduate/Master | 16 | 20.3 |
| MD/PhD | 10 | 12.7 |
| Other | 3 | 3.8 |
| Region | ||
| Northern Italy | 60 | 75.9 |
| Center Italy | 12 | 15.19 |
| Southern Italy | 7 | 8.86 |
| Marital status | ||
| Single | 56 | 70.9 |
| Married/partnered | 21 | 26.6 |
| Divorced/widowed | 2 | 2.5 |
| Health state | ||
| Quite good | 24 | 30.4 |
| Good | 34 | 43.0 |
| Very good | 21 | 26.6 |
| Employment status | ||
| Students | 41 | 51.9 |
| Employed | 33 | 41.8 |
| Retired | 5 | 6.3 |
| News sources quantity (M, SD) | 2.82 | 1.28 |
| Previous COVID-19 infection | 10 | 12.7 |
| Analytics | Polarized | Open | Comparison (F, p) | |
|---|---|---|---|---|
| CRT Accuracy | 0.64 | −1.11 | 0.04 | 50.36, 0.001 |
| CRT Impulsive Errors | −0.59 | 1.10 | −0.10 | 33.33, 0.001 |
| Conspiracy | −0.10 | 0.68 | −0.46 | 8.91, 0.001 |
| Impulsivity—Sensation Seeking | −0.14 | −0.27 | 0.45 | 3.56, 0.037 |
| Impulsivity—Negative Urgency | −0.03 | 0.57 | −0.47 | 6.35, 0.004 |
| Discomfort with Ambiguity (MAAS) | 0.26 | 0.60 | −0.93 | 24.46, 0.001 |
| Absolutism (MAAS) | −0.15 | 0.87 | −0.56 | 14.59, 0.001 |
| Decisiveness (NCC) | −0.52 | 0.15 | 0.65 | 13.45, 0.001 |
| Preference for Predictability (NCC) | 0.27 | 0.48 | −0.84 | 19.78, 0.001 |
| Discomfort with Ambiguity (NCC) | 0.18 | 0.81 | −1.01 | 26.71, 0.001 |
| Preference for Order and Structure (NCC) | 0.07 | 0.81 | −0.85 | 19.81, 0.001 |
| Closed-mindedness (NCC) | 0.11 | 0.77 | −0.87 | 17.62, 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colautti, L.; Cancer, A.; Magenes, S.; Antonietti, A.; Iannello, P. Risk-Perception Change Associated with COVID-19 Vaccine’s Side Effects: The Role of Individual Differences. Int. J. Environ. Res. Public Health 2022, 19, 1189. https://doi.org/10.3390/ijerph19031189
Colautti L, Cancer A, Magenes S, Antonietti A, Iannello P. Risk-Perception Change Associated with COVID-19 Vaccine’s Side Effects: The Role of Individual Differences. International Journal of Environmental Research and Public Health. 2022; 19(3):1189. https://doi.org/10.3390/ijerph19031189
Chicago/Turabian StyleColautti, Laura, Alice Cancer, Sara Magenes, Alessandro Antonietti, and Paola Iannello. 2022. "Risk-Perception Change Associated with COVID-19 Vaccine’s Side Effects: The Role of Individual Differences" International Journal of Environmental Research and Public Health 19, no. 3: 1189. https://doi.org/10.3390/ijerph19031189