
Exploring Barriers and Facilitators to Physical Activity during the COVID-19 Pandemic: A Qualitative Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
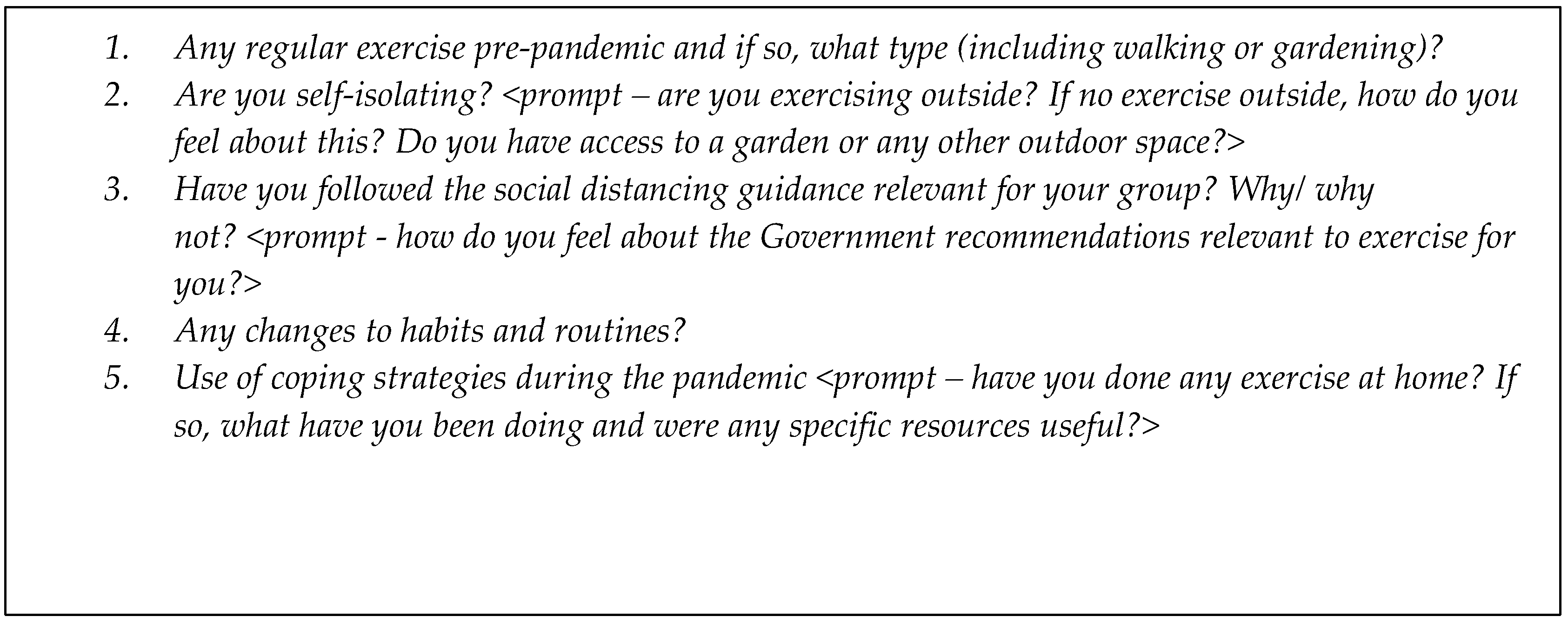
2.3. Qualitative Interviews
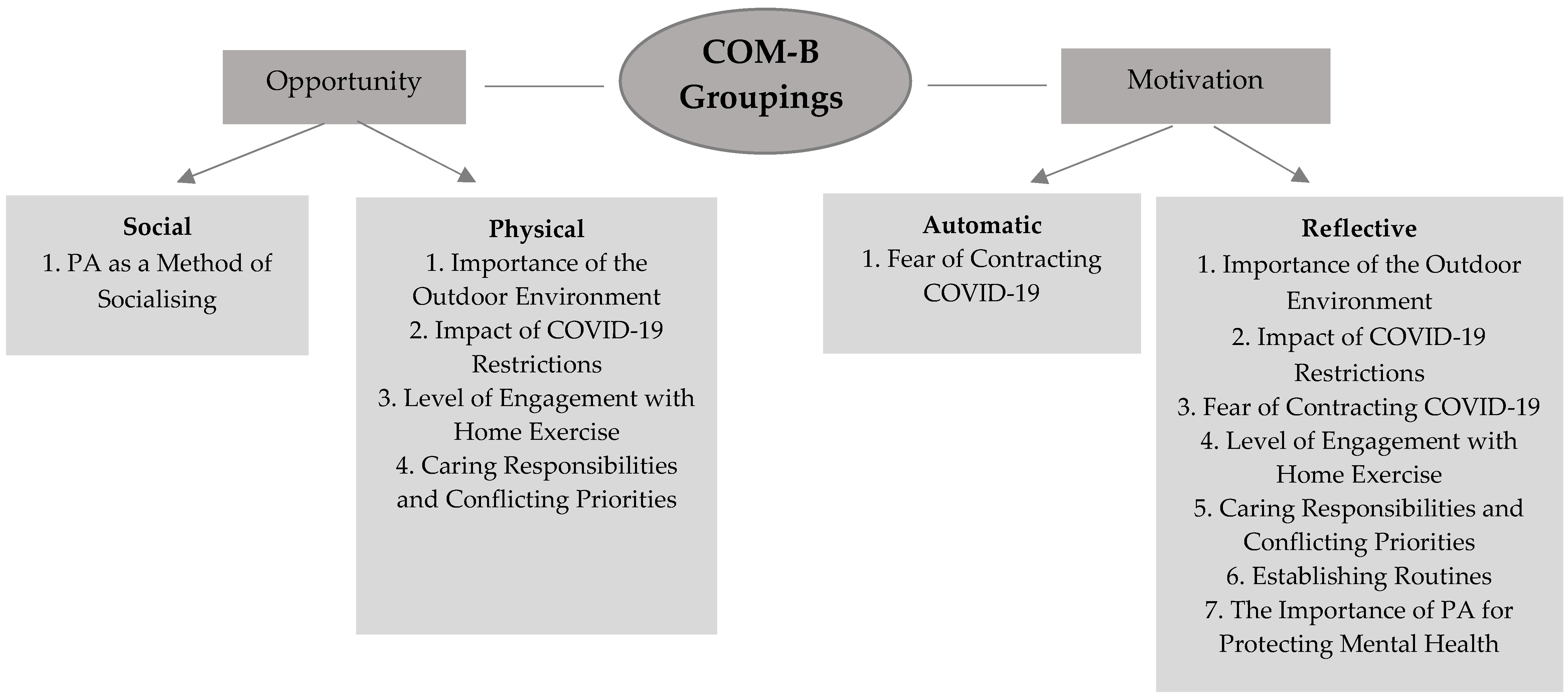
2.4. Analysis
3. Results
3.1. Importance of the Outdoor Environment
3.1.1. Garden Access
“we’ve got two acres of garden…you have to put in a fair amount of work…the garden is really good for weightlifting and everything else”(Age 55–59, LTC)
“Exercising has definitely been a problem, because of not being able to go out and being stuck in a small flat”.(Age 35–39, LTC)
3.1.2. Living in Rural vs. Urban Environments
“We live in a semi-rural (location) and we’ve got beautiful walks near us that are five minutes away. So, I’m exercising every day”(Age 65–69, LTC)
“we’ve got a lot more green space. So, when I want to go for a jog I can still explore for ages and not see another human being. So, it feels safe…”.(Age 25–29, MHC)
“I want to get out and get fresh air, you can see the season changing.And first of all you had the bluebells, and now you’ve got the rhododendrons, and the birdsong was absolutely fantastic, because the weather was so good, and the birds were all building their nests and things”.(Age 70–74, Older Adult)
“They’re all terraced houses here. Everyone lives on top of each other. It just isn’t possible to go out and try and exercise while socially distancing”.(Age 30–34, MHC)
3.1.3. Influence of Weather
“I can go for walks with friends…I haven’t taken advantage of that a lot recently, but I did when lockdown first came up, because the weather was nicer”.(Age 45–49, Parent)
“for the bit of March and April, and most of May, I was going out once every two days, sometimes if the weather wasn’t good, once every three days”.(Age 65–69, LTC)
3.2. Impact of COVID-19 Restrictions
3.2.1. Government Guidance for Clinically Vulnerable Populations (Shielding Advice)
“I got all the texts from the government telling me that I shouldn’t leave the house. And I shouldn’t even put the bins out, or go in the garden if anyone else was going to be around. And so I did follow that really strictly. I didn’t even go in the garden for about six weeks”(Age 30–34, LTC)
“My mum’s been like, can I go for a walk? No, unfortunately, you can’t. If I can’t go for a walk, you have to live the same life as me, which means you can’t go for a walk”.(Age 35–39, LTC)
3.2.2. Restrictions around Exercise
“The one thing that’s been really affected lockdown for me was athletics. I do 400 m training, so I would run at the track in the evenings. However the UK Athletics when social distancing began, put in decisions to not allow sessions to be run in person anymore”.(Age 20–24, Young Adult)
“So obviously my gym closed down so I didn’t do any of that”.(Age 18–19, Young Adult)
“I drove to a park a couple of times and ran around there, but I think there was such public controversy about people driving to other areas that it just made it really not enjoyable”.(Age 30–34, MHC)
“I should be playing tennis now…you can only play singles unless you’ve got four in the same household…You rely on somebody else then, to find somebody else to play singles with you, when you’re on your own…And I haven’t found anybody yet…So, confusing, shall we say?”(Age 70–74, Older Adult)
3.2.3. Government Guidance to Work from Home
“I had started to gain weight at the beginning of the lockdown, and I realised the very little exercise that I was doing before was the walking to my (university) classes or walking to travel to my classes”(Age 20–24, Young Adult)
“[it’s]…also about having more time. Because my partner would have been sat in an office four days a week nine to five, I would have been doing bits of travelling for my work, sometimes leaving early, coming home late”.(Age 35–39, Parent)
3.2.4. A Reason to Leave the Home
“I guess the exercise was just as much for getting out as it was for exercise”.(Age 30–34, Parent)
“we’ve all made sure we do something outside of our four walls, even if it’s a school run, it gets you out of the house, gets you walking”(Age 40–44, Parent)
“I remember the first time I just went for a run on my own, and I was like, oh, it’s just so nice, 40 min”(Age 35–39, Parent)
“It was easy before to say, I’ll go for a walk tomorrow, whereas now it’s a bit like the forbidden fruit, isn’t it? You’re not allowed out except for one walk so you make sure you get out for that walk”.(Age 70–74, Older Adult)
3.3. Fear of Contracting COVID-19
“It worries me a lot, other people getting ill as a result, maybe if I got it, I could carry it, transmit it to other people. So, I thought no, I will stay at home…I won’t go outside whatsoever”.(Age 20–24, MHC/Young Adult)
“obviously the pandemic is a health thing. It just made me realise how important it is to look after yourself”.(Age 25–29, MHC)
“when the news came out about the greater risks (of COVID-19) for diabetes, I’ve switched to going (walking) every day, unless I absolutely can’t”.(Age 65–69, LTC)
3.4. Level of Engagement with Home Exercise
“Obviously we took the classes online, which has been fantastic…It’s as wonderful as if we were all in the class together, it’s been great”.(Age 65–69, LTC)
“Pilates was run at my office, but that was full. So, I couldn’t get a place, but when it went online, she had more capacity, so I could actually do it”.(Age 45–49, Parent)
“When we realised that lockdown was coming, we went and bought the Pilates machine because we used to go to a weekly one to one Pilates class locally”.(Age 60–64, LTC)
“I did look into getting an exercise bike. It was delivered and…downstairs came upstairs to complain about that”.(Age 40–44, MHC)
“My daughter was supposed to do a virtual dancing, but I ruled it out straight away because of the fact that we’re in such a small property, with so many of us”.(Age 30–34, Parent/MHC)
“I tried to do Tai-Chi with my teacher, an online link and video. But it just is not the same. So, I stopped doing that”.(Age 35–39, Parent)
3.5. Caring Responsibilities and Conflicting Priorities
“So, previously, I could take my daughter to a breakfast club very regularly, and that would allow me to go to the gym before work…therefore it started to become very difficult without a breakfast club”.(Age 45–49, Parent)
“I used to run a lot…Since not having an au pair it’s been more difficult. I started running again but it’s just having the time. There’s something’s got to give in a day and it’s usually not having time to do the garden or not going for a run if I’ve got things to do”.(Age 45–49, Parent/LTC)
“there has been a difficulty of separating work from home…You keep thinking, just one more email that I really need to respond to and that just snowballs. You just don’t know when to stop”.(Age 40–44, LTC)
3.6. PA as A Method of Socialising
“I was going to circuit training once, two days a week…It was more for the social side of it rather than fitness”(Age 20–24, Young Adult)
“I’ve got a friend who just lives across the railway tracks and we meet up quite frequently because it’s just a case of just walking up the road and we can meet at the canal and go for a walk”.(Age 30–34, Parent)
“Walking has become a massive thing…I try to go for a walk at least every day, I’ve never done that before. So, we’ve found other ways that we can socially interact or meet up with each other, rather than just sitting in the pub”.(Age 40–44, MHC)
“I’ve done the Keep Fit, and other people from work do it as well, so we see each other on Zoom and we laugh about it”.(Age 50–54, LTC)
3.7. Establishing New Routines
“…actually getting out for exercise on a daily basis becomes more of a part of what we do”.(Age 70–74, LTC)
“And I took up the walking locally. I would just leave my house, walk up the road, round the block and come back for 20 min initially, and then gradually increased that to the point where I’m now doing up to an hour”.(Age 80–84, Older Adult)
“I wonder if this is something that we will take post-pandemic because now having exercised every day feels like it’s an absolute must have”.(Age 35–39, Parent)
3.8. The Importance of PA for Protecting Mental Health
“I did go out for the once a day exercise. I usually tried to do it after work just to give me that break to change from my mindset from work mode to coming back to relaxing”.(Age 20–24, Young Adult)
“I think that’s why my mental health’s been kind of okay after those few weeks when we started going out for a walk, because it was too much to just be totally indoors”(Age 30–34, LTC)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-11-march-2020 (accessed on 23 June 2022).
- GOV UK. Prime Minister Announces National Lockdown. Available online: https://www.gov.uk/government/news/prime-minister-announces-national-lockdown (accessed on 2 May 2022).
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2020, 7, e000960. [Google Scholar] [CrossRef]
- Savage, M.J.; Hennis, P.J.; Magistro, D.; Donaldson, J.; Healy, J.C.; James, R.M. Nine Months into the COVID-19 Pandemic: A Longitudinal Study Showing Mental Health and Movement Behaviours Are Impaired in UK Students. Int. J. Environ. Res. Public Health 2021, 18, 2930. [Google Scholar] [CrossRef]
- McCarthy, H.; Potts, H.W.W.; Fisher, A. Physical Activity Before, During and After COVID-19 Restrictions: Longitudinal Smartphone-Tracking Study of Adults in the United Kingdom. J. Med. Internet Res. 2021, 23, e23701. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Jacob, L.; Butler, L.; Schuch, F.; Barnett, Y.; Grabovac, I.; Veronese, N.; Caperchione, C.; Lopez-Sanchez, G.F.; Meyer, J.; et al. Prevalence and correlates of physical activity in a sample of UK adults observing social distancing during the COVID-19 pandemic. BMJ Open Sport Exerc. Med. 2020, 6, e000850. [Google Scholar] [CrossRef]
- Rogers, N.T.; Waterlow, N.R.; Brindle, H.; Enria, L.; Eggo, R.M.; Lees, S.; Roberts, C.H. Behavioral Change Towards Reduced Intensity Physical Activity Is Disproportionately Prevalent Among Adults with Serious Health Issues or Self-Perception of High Risk During the UK COVID-19 Lockdown. Front. Public Health 2020, 8, 575091. [Google Scholar] [CrossRef] [PubMed]
- To, Q.G.; Duncan, M.J.; Van Itallie, A.; Vandelanotte, C. Impact of COVID-19 on Physical Activity Among 10,000 Steps Members and Engagement with the Program in Australia: Prospective Study. J. Med. Internet Res. 2021, 23, e23946. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Y.; Bennell, K.; White, D.K.; Wei, J.; Wu, Z.; He, H.; Liu, S.; Luo, X.; Hu, S.; et al. Physical Distancing Measures and Walking Activity in Middle-aged and Older Residents in Changsha, China, during the COVID-19 Epidemic Period: Longitudinal Observational Study. J. Med. Internet Res. 2020, 22, e21632. [Google Scholar] [CrossRef]
- Schmidt, T.; Pawlowski, C.S. Physical Activity in Crisis: The Impact of COVID-19 on Danes’ Physical Activity Behaviour. Front. Sports Act. Living 2021, 2, 610255. [Google Scholar] [CrossRef]
- Strain, T.; Sharp, S.J.; Spiers, A.; Price, H.; Williams, C.; Fraser, C.; Brage, S.; Wijndaele, K.; Kelly, P. Population level physical activity before and during the first national COVID-19 lockdown: A nationally representative repeat cross-sectional study of 5 years of Active Lives data in England. Lancet Reg. Health. Eur. 2022, 12, 100265. [Google Scholar] [CrossRef]
- Office for National Statistics. Coronavirus and Shielding of Clinically Extremely Vulnerable People in England: 28 May to 3 June 2020. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/coronavirusandshieldingofclinicallyextremelyvulnerablepeopleinengland/28mayto3june2020 (accessed on 23 June 2022).
- Assaloni, R.; Pellino, V.C.; Puci, M.V.; Ferraro, O.E.; Lovecchio, N.; Girelli, A.; Vandoni, M. Coronavirus disease (COVID-19): How does the exercise practice in active people with type 1 diabetes change? A preliminary survey. Diabetes Res. Clin. Pract. 2020, 166, 108297. [Google Scholar] [CrossRef]
- Ghosh, A.; Arora, B.; Gupta, R.; Anoop, S.; Misra, A. Effects of a nationwide lockdown during COVID-19 epidemic on lifestyle and other medical issues of patients with type 2 diabetes in north India. Diabetes Metab. Syndr. 2020, 14, 917–920. [Google Scholar] [CrossRef] [PubMed]
- Roberts-Lewis, S.F.; Ashworth, M.; White, C.M.; Rose, M.R. COVID-19 lockdown impact on the physical activity of adults with progressive muscle diseases. BMJ Neurol. Open 2021, 3, e000140. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, J.; Borges-Machado, F.; Pizarro, A.N.; Bohn, L.; Barros, D. Home Confinement in Previously Active Older Adults: A Cross-Sectional Analysis of Physical Fitness and Physical Activity Behavior and Their Relationship with Depressive Symptoms. Front. Psychol. 2021, 12, 643832. [Google Scholar] [CrossRef] [PubMed]
- Mishra, R.; Park, C.; York, M.K.; Kunik, M.E.; Wung, S.; Naik, A.D.; Najafi, B. Decrease in Mobility during the COVID-19 Pandemic and Its Association with Increase in Depression among Older Adults: A Longitudinal Remote Mobility Monitoring Using a Wearable Sensor. Sensors 2021, 21, 3090. [Google Scholar] [CrossRef] [PubMed]
- Creese, B.; Khan, Z.; Henley, W.; O’Dwyer, S.; Corbett, A.; Da Silva, M.V.; Mills, K.; Wright, N.; Testad, I.; Aarsland, D.; et al. Loneliness, physical activity, and mental health during COVID-19: A longitudinal analysis of depression and anxiety in adults over the age of 50 between 2015 and 2020. Int. Psychogeriatr. 2021, 33, 505–514. [Google Scholar] [CrossRef]
- Institute for Government. Schools and Coronavirus: The Government’s Handling of Education during the Pandemic. Available online: https://www.instituteforgovernment.org.uk/sites/default/files/publications/schools-and-coronavirus.pdf (accessed on 23 June 2022).
- Mata, J.; Wenz, A.; Rettig, T.; Reifenscheid, M.; Möhring, K.; Krieger, U.; Friedel, S.; Fikel, M.; Cornesse, C.; Blom, A.G.; et al. Health behaviors and mental health during the COVID-19 pandemic: A longitudinal population-based survey in Germany. Soc. Sci. Med. 2021, 287, 114333. [Google Scholar] [CrossRef]
- Robbins, L.B.; Ling, J. Lifestyle Behaviors and Parents’ Mental Wellbeing Among Low-Income Families During COVID-19 Pandemic. Nurs. Res. 2022, 71, 257–265. [Google Scholar] [CrossRef]
- Curtis, R.G.; Olds, T.; Ferguson, T.; Fraysse, F.; Dumuld, D.; Esterman, A.; Hendrie, G.A.; Brown, W.J.; Lagiseti, R.; Maher, C.A. Changes in diet, activity, weight and wellbeing of parents during COVID-19 lockdown. PLoS ONE 2021, 16, e0248008. [Google Scholar] [CrossRef]
- Ng, Y.L.; Hill, K.D.; Burton, E. Exploring physical activity changes and experiences of older adults living in retirement villages during a pandemic. Australas. J. Ageing 2021, 41, e103–e111. [Google Scholar] [CrossRef]
- Goethals, L.; Barth, N.; Guyot, J.; Hupin, D.; Celarier, T.; Bongue, B. Impact of Home Quarantine on Physical Activity Among Older Adults Living at Home During the COVID-19 Pandemic: Qualitative Interview Study. JMIR Aging 2020, 3, e19007. [Google Scholar] [CrossRef]
- Greenwood-Hickman, M.A.; Dahlquist, J.; Cooper, J.; Holden, E.; McClure, J.B.; Mettert, K.D.; Perry, S.R.; Rosenberg, D.E. “They’re Going to Zoom It”: A Qualitative Investigation of Impacts and Coping Strategies During the COVID-19 Pandemic Among Older Adults. Front. Public Health 2021, 9, 679976. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.O.; Belderson, P.; Dainty, J.R.; Birt, L.; Durrant, K.; Chipping, J.R.; Tsigarides, J.; Yates, M.; Naughton, F.; Werry, S.; et al. Impact of COVID-19 pandemic social restriction measures on people with rheumatic and musculoskeletal diseases in the UK: A mixed-methods study. BMJ Open 2021, 11, e048772. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.; Cooper, J.; McHale, F.; Clifford, J.; Woods, C. Barriers and facilitators to changes in adolescent physical activity during COVID-19. BMJ Open Sport Exerc. Med. 2020, 6, e000919. [Google Scholar] [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howlett, N.; Schulz, J.; Trivedi, D.; Troop, N.; Chater, A. A prospective study exploring the construct and predictive validity of the COM-B model for physical activity. J. Health Psychol. 2017, 24, 1378–1391. [Google Scholar] [CrossRef] [Green Version]
- Burton, A.; McKinlay, A.; Dawes, J.; Roberts, A.; Fynn, W.; May, T.; Fancourt, D. Understanding barriers and facilitators to compliance with UK social distancing guidelines during the COVID-19 pandemic: A qualitative interview study. Behav. Chang. 2022, 1–21. [Google Scholar] [CrossRef]
- Knight, R.L.; McNarry, M.A.; Sheeran, L.; Runacres, A.W.; Thatcher, R.; Shelley, J.; Mackintosh, K.A. Moving Forward: Understanding Correlates of Physical Activity and Sedentary Behaviour during COVID-19–An Integrative Review and Socioecological Approach. Int. J. Environ. Res. Public Health 2021, 18, 10910. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Social Study. Home. Available online: https://www.covidsocialstudy.org/ (accessed on 23 May 2022).
- MARCH Network. Home Page: March Legacy. Available online: https://www.marchlegacy.org/ (accessed on 16 May 2022).
- House of Commons Library. Coronavirus: A History of English Lockdown Laws. Available online: https://researchbriefings.files.parliament.uk/documents/CBP-9068/CBP-9068.pdf (accessed on 2 May 2022).
- GOV UK. COVID-19 Response—Spring 2021 (Summary). Available online: https://www.gov.uk/government/publications/covid-19-response-spring-2021/covid-19-response-spring-2021-summary (accessed on 26 June 2022).
- GOV UK. Prime Minister’s Statement on Coronavirus (COVID-19): 10 May 2020. Available online: https://www.gov.uk/government/speeches/pm-address-to-the-nation-on-coronavirus-10-may-2020 (accessed on 26 June 2022).
- GOV UK. Prime Minister’s Statement on Coronavirus (COVID-19): 3 July 2020. Available online: https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-3-july-2020 (accessed on 26 June 2022).
- GOV UK. COVID-19 Response: Summer 2021. Available online: https://www.gov.uk/government/publications/covid-19-response-summer-2021-roadmap/covid-19-response-summer-2021 (accessed on 26 June 2022).
- GOV UK. PM Opening Statement at COVID-19 Press Conference: 8 December 2021. Available online: https://www.gov.uk/government/speeches/pm-opening-statement-at-covid-19-press-conference-8-december-2021 (accessed on 26 June 2022).
- Burton, A.; McKinlay, A.; Aughterson, H.; Fancourt, D. Impact of the COVID-19 pandemic on the mental health and well-being of adults with mental health conditions in the UK: A qualitative interview study. J. Ment. Health 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- McKinlay, A.; May, T.; Dawes, J.; Fancourt, D.; Burton, A. “You’re just there, alone in your room with your thoughts” A qualitative study about the impact of lockdown among young people during the COVID-19 pandemic. BMJ Open 2022, 12, e053676. [Google Scholar] [CrossRef] [PubMed]
- McKinlay, A.; Fancourt, D.; Burton, A. A qualitative study about the mental health and wellbeing of older adults in the UK during the COVID-19 pandemic. BMC Geriatr. 2021, 21, 439. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.; Roberts, A.; McKinlay, A.; Fancourt, D.; Burton, A. The impact of the COVID-19 pandemic mental health and well-being of people living with a long-term physical health condition: A qualitative study. BMC Public Health 2021, 21, 1801. [Google Scholar] [CrossRef] [PubMed]
- Dawes, J.; May, T.; McKinlay, A.; Fancourt, D.; Burton, A. Impact of the COVID-19 pandemic on the mental health and wellbeing of parents with young children: A qualitative interview study. BMC Psychol. 2021, 9, 194. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Sundler, A.J.; Lindberg, E.; Nilsson, C.; Palmér, L. Qualitative thematic analysis based on descriptive phenomenology. Nurs. Open 2019, 6, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual. Res. Psychol. 2021, 18, 328–352. [Google Scholar] [CrossRef]
- Atkins, L.; Francis, J.; Islam, R.; O’Connor, D.; Patey, A.; Ivers, N.; Foy, R.; Duncan, E.M.; Colquhoun, H.; Grimshaw, J.M.; et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement. Sci. 2017, 12, 77. [Google Scholar] [CrossRef]
- Spence, J.C.; Rhodes, R.E.; McCurdy, A.; Mangan, A.; Hopkins, D.; Mummery, W.K. Determinants of physical activity among adults in the United Kingdom during the COVID-19 pandemic: The DUK-COVID study. Br. J. Health Psychol. 2021, 26, 588–605. [Google Scholar] [CrossRef]
- CDC COVID-19 Response Team. Geographic Differences in COVID-19 Cases, Deaths, and Incidence–United States, 12 February –7 April 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 465–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Public Health England. Disparities in the Risk and Outcomes of COVID-19. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/908434/Disparities_in_the_risk_and_outcomes_of_COVID_August_2020_update.pdf (accessed on 23 June 2022).
- Hughes, R.P.; Hughes, D.A. Impact of Relaxing Covid-19 Social Distancing Measures on Rural North Wales: A Simulation Analysis. Front. Public Health 2020, 8, 562473. [Google Scholar] [CrossRef]
- Pringle, A.; Kime, N.; Zwolinsky, S.; Rutherford, Z.; Roscoe, C.M.P. An Investigation into the Physical Activity Experiences of People Living with and beyond Cancer during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2022, 19, 2945. [Google Scholar] [CrossRef] [PubMed]
- Hajat, C.; Hasan, A.; Subel, S.; Noach, A. The impact of short-term incentives on physical activity in a UK behavioural incentives programme. NPJ Dig. Med. 2019, 2, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Klaiber, P.; Wen, J.H.; DeLongis, A.; Sin, N.L. The Ups and Downs of Daily Life During COVID-19: Age Differences in Affect, Stress, and Positive Events. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e30–e37. [Google Scholar] [CrossRef] [PubMed]
- Malkin, G.; Hayat, T.; Amichai-Hamburger, Y.; Ben-David, B.M.; Regev, T.; Nakash, O. How well do older adults recognise mental illness? A literature review. Psychogeriatrics 2019, 19, 491–504. [Google Scholar] [CrossRef] [PubMed]
- Kwong, A.S.F.; Pearson, R.M.; Adams, M.J.; Northstone, K.; Tilling, K.; Smith, D.; Fawns-Ritchie, C.; Bould, H.; Warne, N.; Zammit, S.; et al. Mental health before and during the COVID-19 pandemic in two longitudinal UK population cohorts. Br. J. Psychiatry 2020, 218, 334–343. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, R.C.; Wetherall, K.; Cleare, S.; McClelland, H.; Melson, A.J.; Niedzwiedz, C.L.; O’Carroll, R.E.; O’Connor, D.B.; Platt, S.; Scowcroft, E.; et al. Mental health and well-being during the COVID-19 pandemic: Longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. Br. J. Psychiatry 2020, 218, 326–333. [Google Scholar] [CrossRef]
- Office for National Statistics. Coronavirus and Depression in Adults, Great Britain: January to March 2021. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/articles/coronavirusanddepressioninadultsgreatbritain/januarytomarch2021 (accessed on 23 June 2022).
- Zhang, Y.; Zhang, H.; Ma, X.; Di, Q. Mental Health Problems during the COVID-19 Pandemics and the Mitigation Effects of Exercise: A Longitudinal Study of College Students in China. Int. J. Environ. Res. Public Health 2020, 17, 3722. [Google Scholar] [CrossRef] [PubMed]
- Coyle, C.; Ghazi, H.; Georgiou, I. The mental health and well-being benefits of exercise during the COVID-19 pandemic: A cross-sectional study of medical students and newly qualified doctors in the UK. Ir. J. Med. Sci. 2020, 190, 925–926. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Date | Timeline of COVID-19 News and Restrictions |
|---|---|
| 23 March 2020 | National lockdown begins. Legal exemptions for leaving home include essential shopping, going to work, medical reasons, exercising once per day. |
| 10 May 2020 | Those who cannot work from home encouraged to return to work but avoid public transport. Unlimited outdoor exercise is permitted. |
| 13 May 2020 | Outdoor recreation added as a legal exemption or leaving home. People allowed to meet someone from one other household outside. |
| 1 June 2020 | ‘Stay at home’ order removed. Outdoor gatherings of six people from different households permitted. |
| 3 July 2020 | Local lockdowns are introduced for areas where the rates of positive cases of COVID-19 are higher. |
| 14 September 2020 | Socialising is limited to groups of six people. Gatherings of above six people are banned. |
| 14 October 2020 | Tier system is introduced where different regions of the country will live under different restrictions depending on local infection rates. Tier 1 (medium alert)—Rule of six when socialising, work from home if possible. Tier 2 (high alert)—Rule of six outside but no inside contact with other households, work from home if possible. Tier 3 (very high alert)—Socialising with other households not permitted in most settings, work from home if possible, sports facilities are open but close contact sports should be avoided, indoor exercise only permitted with your household. |
| 5 November 2020 | Second national lockdown begins. |
| 2 December 2020 | End to national lockdown and return to tier system. |
| 19 December 2020 | Tier 4 introduced—restrictions are similar to a lockdown with a ‘stay at home’ order, non-essential shops, hospitality and sports facilities are closed. |
| 6 January 2021 | Third national lockdown begins. |
| 8 March 2021 | Schools begin to reopen. Two people are permitted to meet for outdoor recreation. |
| 29 March 2021 | Groups of six people or two households can meet outside. Outdoor sports facilities reopen. |
| 12 April 2021 | Non-essential shops, outdoor hospitality and gyms re-open. |
| 17 May 2021 | Groups of six people or two households can meet inside. Most indoor venues reopen. |
| 19 July 2021 | Most COVID-19 restrictions end. -Self-isolation rules remain. |
| 8 December 2021 | COVID-19 restrictions re-introduced in the UK as part of winter ‘Plan B’. These include working from home where possible, proof of vaccination or negative lateral flow test required for large gatherings and mandatory use of face coverings in most public indoor settings. |
| Young Adult | Older Adult | MHC | LTC | Parents of Young Children | Total | |
|---|---|---|---|---|---|---|
| Sample Size | 16 | 20 | 22 | 33 | 25 | 116 |
| Gender | ||||||
| Male | 6 (37.50%) | 11 (55%) | 9 (40.91%) | 12 (36.36%) | 7 (28%) | 45 (38.79%) |
| Female | 10 (62.50%) | 9 (45%) | 13 (59.09%) | 21 (63.64%) | 18 (72%) | 71 (61.21%) |
| Age (years) | ||||||
| Mean | 21.06 | 79.30 | 43.23 | 56.36 | 40.32 | 49.50 |
| SD | 2.05 | 5.50 | 14.00 | 12.73 | 6.49 | 20.00 |
| Ethnicity | ||||||
| White British | 12 (75%) | 16 (80%) | 14 (63.64%) | 24 (72.73%) | 16 (64%) | 82 (70.70%) |
| White Irish | 0 | 0 | 1 (4.55%) | 0 | 2 (8%) | 3 (2.59%) |
| White and Asian | 0 | 0 | 2 (9.09%) | 1 (3.03%) | 1 (4%) | 4 (3.45%) |
| White and Black Caribbean | 1 (6.25%) | 0 | 0 | 1 (3.03%) | 0 | 2 (1.72%) |
| Black British Caribbean | 0 | 0 | 0 | 2 (6.06%) | 0 | 2 (1.72%) |
| Black British African | 0 | 0 | 2 (9.09%) | 0 | 1 (4%) | 3 (2.59%) |
| Indian | 1 (6.25%) | 0 | 2 (9.09%) | 2 (6.06%) | 2 (8%) | 7 (6.03%) |
| Chinese | 0 | 0 | 0 | 0 | 1 (4%) | 1 (0.86%) |
| Pakistani | 0 | 0 | 1 (4.55%) | 0 | 0 | 1 (0.86%) |
| Other | 2 (12.50%) | 4 (20%) | 0 | 3 (9.09%) | 2 (8%) | 11 (9.48%) |
| Education | ||||||
| No qualifications | 1 (6.25%) | 0 | 0 | 0 | 0 | 1 (0.86%) |
| Post-16 vocational course | 0 | 0 | 2 (9.09%) | 0 | 0 | 2 (1.72%) |
| GCSE/equivalent | 0 | 3 (15%) | 1 (4.55%) | 3 (9.09%) | 1 (4%) | 8 (6.90%) |
| A-levels/equivalent | 9 (56.25%) | 1 (5%) | 5 (22.73%) | 5 (15.15%) | 0 | 20 (17.24%) |
| Undergraduate degree/professional qualification | 5 (31.25%) | 7 (35%) | 10 (45.45%) | 12 (36.36%) | 9 (36%) | 43 (37.07%) |
| Postgraduate degree | 1 (6.25%) | 9 (45%) | 4 (18.18%) | 13 (39.39%) | 15 (60%) | 42 (36.21%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roche, C.; Fisher, A.; Fancourt, D.; Burton, A. Exploring Barriers and Facilitators to Physical Activity during the COVID-19 Pandemic: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 9169. https://doi.org/10.3390/ijerph19159169
Roche C, Fisher A, Fancourt D, Burton A. Exploring Barriers and Facilitators to Physical Activity during the COVID-19 Pandemic: A Qualitative Study. International Journal of Environmental Research and Public Health. 2022; 19(15):9169. https://doi.org/10.3390/ijerph19159169
Chicago/Turabian StyleRoche, Charlotte, Abigail Fisher, Daisy Fancourt, and Alexandra Burton. 2022. "Exploring Barriers and Facilitators to Physical Activity during the COVID-19 Pandemic: A Qualitative Study" International Journal of Environmental Research and Public Health 19, no. 15: 9169. https://doi.org/10.3390/ijerph19159169