
Effectiveness of Telemedicine and Teledentistry after the COVID-19 Pandemic

Abstract
:1. Introduction
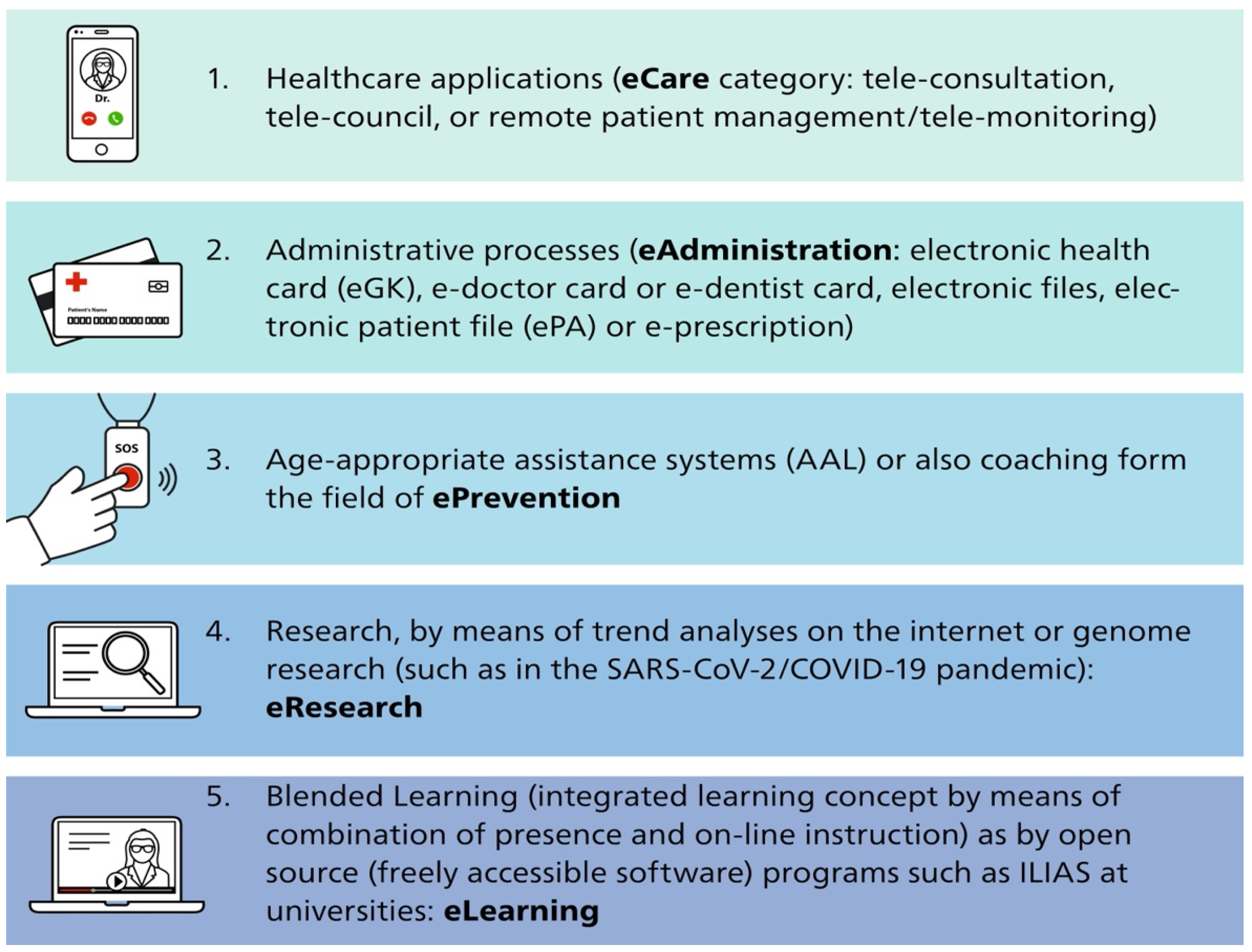
2. Areas of Application of Telemedicine
3. Digital Infrastructure
3.1. Central Directory for Technical and Semantic Standards, Profiles, and Guidelines
3.2. Infrastructural and Technical Challenges
4. Impact of the SARS-CoV-2/COVID-19 Pandemic
Telemedicine/Teledentistry as a Response to Pandemic Challenges
5. Regular Use of Telemedicine Applications for Emergency Treatment & Consilium
5.1. Use of Telemedicine in Aviation
5.2. Use of Telemedicine in Train Traffic and Shipping
5.3. Teledentistry in Dental Disciplines
5.4. Telemedicine Applications in Urban and Rural Areas
5.5. Telemedicine Applications in International Aid Projects
5.6. Telemedicine Application in Continuing Dental/Medical Education
6. Obstacles of Telemedicine and Teledentistry
6.1. Problems of Telemedicine in Dental Education, Training, and Continuing Education
6.2. Challenges, Difficulties, and Risks of Using Telemedicine
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- German Medical Association (Bundesärztekammer). Telemedizin. 2015. Available online: https://www.bundesaerztekammer.de/fileadmin/user_upload/_old-files/downloads/pdf-Ordner/Telemedizin_Telematik/Telemedizin/V-03_Entschliessung_Telemedizin.pdf (accessed on 24 October 2022).
- World Health Organizsation (WHO). 58. World Health Assembly. WHA58.28 eHealth. 2005. Available online: http://apps.who.int/iris/bitstream/10665/20378/1/WHA58_28-en.pdf (accessed on 24 October 2022).
- Working Group Telemedicine of the German Medical Association (Bundesärztekammer). Telemedizinische Methoden in der Patientenversorgung–Begriffliche Verortung. 2015. Available online: https://www.bundesaerztekammer.de/fileadmin/user_upload/_old-files/downloads/pdf-Ordner/Telemedizin_Telematik/Telemedizin/Telemedizinische_Methoden_in_der_Patientenversorgung_Begriffliche_Verortung.pdf (accessed on 24 October 2022).
- Thrall, J.H. Teleradiology. Part I. History and clinical applications. Radiology 2007, 243, 613–617. [Google Scholar] [CrossRef] [PubMed]
- American College of Radiology (ACR). Standards for Teleradadiology; ACR: Reston, VA, USA, 1994. [Google Scholar]
- VeSta Informationsportal. Available online: https://www.informationsportal.VeSta-gematik.de/ueber-VeSta/ (accessed on 24 October 2022).
- Ericsson. Ericsson Mobility Report–On the Pulse of the Networked Society. 2015. Available online: https://www.ericsson.com/49df10/assets/local/reports-papers/mobility-report/documents/2015/ericsson-mobility-report-june-2015.pdf (accessed on 24 October 2022).
- Nier, H. Mobiles Internet–Die Schnellsten LTE-Netze Europas. 2018. Available online: https://de.statista.com/infografik/12986/schnellste-lte-netze-europas/ (accessed on 24 October 2022).
- Robert Koch Institute (RKI). COVID-19 in Germany. 2022. Available online: https://www.rki.de/EN/Home/homepage_node.html (accessed on 24 October 2022).
- Wolf, T.G.; Deschner, J.; Schrader, H.; Bührens, P.; Kaps-Richter, G.; Cagetti, M.G.; Campus, G. Dental Workload Reduction during First SARS-CoV-2/COVID-19 Lockdown in Germany: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2021, 18, 3164. [Google Scholar] [CrossRef] [PubMed]
- Cagetti, M.G.; Balian, A.; Camoni, N.; Campus, G. Influence of the COVID-19 Pandemic on Dental Emergency Admissions in an Urgent Dental Care Service in North Italy. Int. J. Environ. Res. Public Health 2021, 18, 1812. [Google Scholar] [CrossRef] [PubMed]
- COVIDental Collaboration Group. The COVID-19 pandemic and its global effects on dental practice. An international survey. J. Dent. 2021, 114, 103749. [Google Scholar] [CrossRef] [PubMed]
- Kassenzahnärztliche Bundesvereinigung und Bundeszahnärztekammer. Maßnahmen der Zahnärzteschaft für Die Aufrechterhaltung der Versorgung. 2020. Available online: https://www.bzaek.de/berufsausuebung/sars-cov-2covid-19/massnahmenpaket-der-zahnaerzteschaft.html (accessed on 24 October 2022).
- Schubert, J.; Nokaj, M. Patientenkommunikation. Telemedizin: Auch für Zahnärzte Sinnvoll. 2020. Available online: https://www.quintessence-publishing.com/deu/de/news/praxis/patientenkommunikation/telemedizin-auch-fuer-zahnaerzte-sinnvoll (accessed on 24 October 2022).
- KV FUX. 2019. Available online: https://www.kv-fux.de/2019/03/19/fernbehandlungsverbot/ (accessed on 24 October 2022).
- International Air Transport Association (IATA). Annual Review 2021. 2021. Available online: https://www.iata.org/contentassets/c81222d96c9a4e0bb4ff6ced0126f0bb/iata-annual-review-2021.pdf (accessed on 24 October 2022).
- International Air Transport Association (IATA). World Air Transport Statistics (WAtS). 2022. Available online: https://www.iata.org/en/publications/store/world-air-transport-statistics/ (accessed on 24 October 2022).
- Lufthansa. Arzt an Bord–News. 2022. Available online: https://www.lufthansa.com/et/de/arzt-an-bord-news (accessed on 24 October 2022).
- Siedenburg, J. Kompendium Flug- und Reisemedizin; BOD: Norderstedt, Germany, 2005. [Google Scholar]
- Siedenburg, J.; Küpper, T. Moderne Flugmedizin; Gentner Verlag: Stuttgart, Germany, 2015. [Google Scholar]
- Graf, J.; Stüben, U.; Pump, S. Medizinische Notfallsituationen im Flugzeug. Dtsch. Arztebl. Int. 2012, 109, 591–602. [Google Scholar] [PubMed]
- Mazareanu, E. Global Air Traffic–Scheduled Passengers 2004–2022. 2021. Available online: https://www.statista.com/statistics/564717/airline-industry-passenger-traffic-globally/ (accessed on 24 October 2022).
- Operation Karriere. Von Beruf Arzt. Telemedizin: Kooperation Optimiert Versorgung auf AIDA-Schiffe. 2016. Available online: https://www.operation-karriere.de/karriereweg/von-beruf-arzt/telemedizin-optimiert-versorgung-auf-aida-schiffen.html (accessed on 24 October 2022).
- Choi, J.W. Clinical usefulness of teleradiology in general dental practice. Imaging Sci. Dent. 2013, 43, 99–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brüllmann, D.; Schmidtmann, I.; Warzecha, K.; d’Hoedt, B. Recognition of root canal orifices at a distance–a preliminary study of teledentistry. J. Telemed. Telecare 2011, 1, 154–157. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Kim, J.H.; Rogowski, L.; Al Shami, S.; Howell, S.E.I. Implementation of teledentistry for orthodontic practices. J. World Fed. Orthod. 2021, 10, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Ignatius, E.; Perälä, S.; Mäkelä, K. Use of videoconferencing for consultation in dental prosthetics and oral rehabilitation. J. Telemed. Telecare 2010, 16, 467–470. [Google Scholar] [CrossRef] [PubMed]
- Kopycka-Kedzierawski, D.T.; Billings, R.J. Teledentistry in inner-city child-care centres. J. Telemed. Telecare 2006, 12, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Jampani, N.D.; Nutalapati, R.; Dontula, B.S.; Boyapati, R. Applications of teledentistry: A literature review and update. J. Int. Soc. Prev. Community Dent. 2011, 1, 37–44. [Google Scholar] [PubMed]
- Lienert, N.; Zitzmann, N.C.; Filippi, A.; Weiger, R.; Krastl, G. Teledental Consultations Related to Trauma in a Swiss Telemedical Center-A Retrospective Survey. Dent. Traumatol. 2010, 26, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Clark, G.T. Teledentistry: What is it Now, and What Will it be Tomorrow? J. Calif. Dent. Assoc. 2000, 28, 121–127. [Google Scholar] [PubMed]
- Ibraheim, A.; Sanalla, A.; Eyeson, J. The role of teledentistry in oral surgery during the COVID-19 pandemic. Adv. Oral Maxillofac. Surg. 2021, 1, 100005. [Google Scholar] [CrossRef]
- Diener, E. Medinside: Neue Krankenversicherung: Zuerst zur App statt zum Arzt. Article in German: New Health Insurance: First to the App Instead of the Doctor. Available online: https://www.medinside.ch/post/neue-krankenversicherung-zuerst-zur-app-statt-zum-arzt (accessed on 24 October 2022).
- Dils, E.S.; Lefebvre, C.; Abeyta, K. Teledentistry in the United States: A New Horizon of Dental Care. Int. J. Dent. Hyg. 2004, 2, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.W.; Hobdell, M.H.; Dunn, K.; Johnson, K.A.; Zhang, J. Teledentistry and its use in dental education. Am. Dent. Assoc. 2003, 134, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Spallek, H.; Pilcher, E.; Lee, J.Y.; Schleyer, T. Evaluation of Web-based dental CE course service. J. Dent. Educ. 2002, 66, 393–404. [Google Scholar] [CrossRef] [PubMed]
- Younai, F.S.; Messadi, D.V. E-mail-based oral medicine consultation. J. Calif. Dent. Assoc. 2002, 28, 144–151. [Google Scholar]
- Logitel. Netzabdeckung in Deutschland–der Große Überblick! 2018. Available online: https://www.logitel.de/blog/handys/netzabdeckung-in-deutschland-der-grosse-ueberblick/ (accessed on 24 October 2022).
- Golder, D.T.; Brennan, K.A. Practicing dentistry in the age of telemedicine. JADA 2000, 131, 734–744. [Google Scholar] [CrossRef] [PubMed]
- Biegel, S. Virtual Health Care: Unresolved Legal Issues. J. Calif. Dent. Assoc. 2000, 28, 128–132. [Google Scholar] [PubMed]
- Olk, J. Zahnschienen. Koalition will Tele-Zahnmedizin Schärfer Regulieren. 2021. Available online: https://www.handelsblatt.com/inside/digital_health/zahnschienen-koalition-will-tele-zahnmedizin-schaerfer-regulieren/27206608.html?ticket=ST-13107287-xd0fQyNhCmksGTMegixz-ap1 (accessed on 24 October 2022).
- Europäischer Wirtschafts- und Sozialausschuss (EWSA). Die Lage der Freien Berufe in Ihrer Funktion und Bedeutung für die Europäische Zivilgesellschaft. Zusammenfassung. EESC/COMM/05/2013. 2013. Available online: https://www.eesc.europa.eu/sites/default/files/resources/docs/qe-01-13-678-de-c.pdf (accessed on 24 October 2022).

{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolf, T.G.; Schulze, R.K.W.; Ramos-Gomez, F.; Campus, G. Effectiveness of Telemedicine and Teledentistry after the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 13857. https://doi.org/10.3390/ijerph192113857
Wolf TG, Schulze RKW, Ramos-Gomez F, Campus G. Effectiveness of Telemedicine and Teledentistry after the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(21):13857. https://doi.org/10.3390/ijerph192113857
Chicago/Turabian StyleWolf, Thomas Gerhard, Ralf Kurt Willy Schulze, Francisco Ramos-Gomez, and Guglielmo Campus. 2022. "Effectiveness of Telemedicine and Teledentistry after the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 21: 13857. https://doi.org/10.3390/ijerph192113857