
Impact of COVID-19 Pandemic Lockdown on the Prognosis, Morbidity, and Mortality of Patients Undergoing Elective and Emergency Abdominal Surgery: A Retrospective Cohort Study in a Tertiary Center, Saudi Arabia


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Variables and Outcome
2.3. Ethical Statement
2.4. Statistical Analysis
3. Results
3.1. Basic Demographic Characteristics of Patients
3.2. Assessment of the Peri-Operative Variables and Surgical Activities
3.3. Clinical and Surgical Consequences of Patients
3.4. Profile of COVID-19 Patients Who Underwent Surgical Procedures
3.5. Relationships between Complications and Their Risk Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fleming, C.A.; Fullard, A.; Croghan, S.; Pellino, G.; Pata, F. Robotic Abdominal Surgery and COVID-19: A Systematic Review of Published Literature and Peer-Reviewed Guidelines during the SARS-CoV-2 Pandemic. J. Clin. Med. 2022, 11, 2957. [Google Scholar] [CrossRef]
- Al-Qahtani, A.A. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): Emergence, history, basic and clinical aspects. Saudi J. Biol. Sci. 2020, 27, 2531–2538. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Alsofayan, Y.; Alahmari, A.; Alowais, J.; Algwizani, A.; Alserehi, H.; Assiri, A.; Jokhdar, H. COVID-19 in Saudi Arabia: The national health response. East. Mediterr. Health J. 2021, 27, 1114–1124. [Google Scholar] [CrossRef] [PubMed]
- Anil, I.; Alagha, O. The impact of COVID-19 lockdown on the air quality of Eastern Province, Saudi Arabia. Air Qual. Atmos. Health 2021, 14, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Coccolini, F.; Perrone, G.; Chiarugi, M.; Di Marzo, F.; Ansaloni, L.; Scandroglio, I.; Marini, P.; Zago, M.; De Paolis, P.; Forfori, F. Surgery in COVID-19 patients: Operational directives. World J. Emerg. Surg. 2020, 15, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basem, J.I.; Roth, A.F.; White, R.S.; Tangel, V.E.; Jiang, S.Y.; Choi, J.M.; Hoffman, K.L.; Schenck, E.J.; Turnbull, Z.A.; Pryor, K.O. Patient care in rapid-expansion intensive care units during the COVID-19 pandemic crisis. BMC Anesthesiol. 2022, 22, 209. [Google Scholar] [CrossRef]
- Smith, W.R.; Atala, A.J.; Terlecki, R.P.; Kelly, E.E.; Matthews, C.A. Implementation guide for rapid integration of an outpatient telemedicine program during the COVID-19 pandemic. J. Am. Coll. Surg. 2020, 231, 216–222.e2. [Google Scholar] [CrossRef]
- Moletta, L.; Pierobon, E.S.; Capovilla, G.; Costantini, M.; Salvador, R.; Merigliano, S.; Valmasoni, M. International guidelines and recommendations for surgery during COVID-19 pandemic: A systematic review. Int. J. Surg. 2020, 79, 180–188. [Google Scholar] [CrossRef]
- Gotlib Conn, L.; Tahmasebi, H.; Meti, N.; Wright, F.C.; Thawer, A.; Cheung, M.; Singh, S. Cancer treatment during COVID-19: A qualitative analysis of patient-perceived risks and experiences with virtual care. J. Patient Exp. 2021, 8, 23743735211039328. [Google Scholar] [CrossRef] [PubMed]
- Rusch, V.W.; Wexner, S.D.; Atala, A.; Atkinson, J.L.; Denneny III, J.C.; Eberlein, T.J.; Elsey, J.K.; Farmer, D.L.; Ford, H.R.; Fried, G.M. The American College of Surgeons Responds to COVID-19. J. Am. Coll. Surg. 2020, 231, 490–496. [Google Scholar] [CrossRef]
- Cano-Valderrama, O.; Morales, X.; Ferrigni, C.J.; Martín-Antona, E.; Turrado, V.; García, A.; Cuñarro-López, Y.; Zarain-Obrador, L.; Duran-Poveda, M.; Balibrea, J.M. Acute care surgery during the COVID-19 pandemic in Spain: Changes in volume, causes and complications. A multicentre retrospective cohort study. Int. J. Surg. 2020, 80, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Pereira, X.; Lima, D.L.; Moran-Atkin, E.; Malcher, F. Where have the surgical patients gone during the COVID-19 pandemic? Rev. Do Colégio Bras. De Cir. 2020, 47, e20202733. [Google Scholar] [CrossRef] [PubMed]
- Nepogodiev, D.; Bhangu, A.; Glasbey, J.C.; Li, E.; Omar, O.M.; Simoes, J.F.; Abbott, T.E.; Alser, O.; Arnaud, A.P.; Bankhead-Kendall, B.K. Mortality and pulmonary complications in patients undergoing surgery with peri-operative SARS-CoV-2 infection: An international cohort study. Lancet 2020, 396, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Paulson, K.R.; Pease, S.A.; Watson, S.; Comfort, H.; Zheng, P.; Aravkin, A.Y.; Bisignano, C.; Barber, R.M.; Alam, T. Estimating excess mortality due to the COVID-19 pandemic: A systematic analysis of COVID-19-related mortality, 2020–2021. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef]
- Cano-Valderrama, O.; Morales, X.; Ferrigni, C.; Martín-Antona, E.; Turrado, V.; García, A.; Cuñarro-López, Y.; Zarain-Obrador, L.; Duran-Poveda, M.; Balibrea, J. Reduction in emergency surgery activity during COVID-19 pandemic in three Spanish hospitals. J. Br. Surg. 2020, 107, e239. [Google Scholar] [CrossRef]
- Patriti, A.; Eugeni, E.; Guerra, F. What happened to surgical emergencies in the era of COVID-19 outbreak? Considerations of surgeons working in an Italian COVID-19 red zone. Updates Surg. 2020, 72, 309–310. [Google Scholar] [CrossRef] [Green Version]
- Hunger, R.; König, V.; Stillger, R.; Mantke, R. Impact of the COVID-19 pandemic on delays in surgical procedures in Germany: A multi-center analysis of an administrative registry of 176,783 patients. Patient Saf. Surg. 2022, 16, 22. [Google Scholar] [CrossRef]
- De Simone, B.; Chouillard, E.; Sartelli, M.; Biffl, W.L.; Di Saverio, S.; Moore, E.E.; Kluger, Y.; Abu-Zidan, F.M.; Ansaloni, L.; Coccolini, F. The management of surgical patients in the emergency setting during COVID-19 pandemic: The WSES position paper. World J. Emerg. Surg. 2021, 16, 14. [Google Scholar] [CrossRef]
- Fu, S.J.; George, E.L.; Maggio, P.M.; Hawn, M.; Nazerali, R. The consequences of delaying elective surgery: Surgical perspective. Ann. Surg. 2020, 272, e79. [Google Scholar] [CrossRef]
- Williams, E.P.; Mesidor, M.; Winters, K.; Dubbert, P.M.; Wyatt, S.B. Overweight and obesity: Prevalence, consequences, and causes of a growing public health problem. Curr. Obes. Rep. 2015, 4, 363–370. [Google Scholar] [CrossRef]
- Doyle, D.J.; Goyal, A.; Bansal, P.; Garmon, E.H. American society of anesthesiologists’ classification. In Statpearls [Internet]; StatPearls Publishing: Tampa, FL, USA, 2021. [Google Scholar]
- Misganaw, D.; Linger, B.; Abesha, A. Surgical antibiotic prophylaxis use and surgical site infection pattern in Dessie Referral Hospital, Dessie, Northeast of Ethiopia. Biomed Res. Int. 2020, 2020, 1695683. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Hwang, H.K.; Lee, W.J.; Kang, C.M. Comprehensive Complication Index or Clavien–Dindo classification: Which is better for evaluating the severity of postoperative complications following pancreatectomy? World J. Surg. 2021, 45, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Leaptrot, D.; Otis, M.; Smith, H.; Hebden, J.N.; Wright, M.-O. Health care-associated infections studies project: An American Journal of Infection Control and National Healthcare Safety Network Data Quality Collaboration Case Study–Chapter 9 Surgical site infection event (SSI) case study. Am. J. Infect. Control 2022, 50, 799–800. [Google Scholar] [CrossRef] [PubMed]
- Weiner-Lastinger, L.M.; Pattabiraman, V.; Konnor, R.Y.; Patel, P.R.; Wong, E.; Xu, S.Y.; Smith, B.; Edwards, J.R.; Dudeck, M.A. The impact of coronavirus disease 2019 (COVID-19) on healthcare-associated infections in 2020: A summary of data reported to the National Healthcare Safety Network. Infect. Control Hosp. Epidemiol. 2022, 43, 12–25. [Google Scholar] [CrossRef] [PubMed]
- Kurniawan, A.; Halim, D.A.; Sutandyo, N. Multiple myeloma management in COVID-19 Era. Asian J. Oncol. 2021, 7, 01–07. [Google Scholar] [CrossRef]
- Yun, Y.; Kim, Y.; Min, Y.; Park, S.; Won, Y.; Kim, D.; Choi, I.; Kim, Y.; Park, S.; Kim, J. The influence of hospital volume and surgical treatment delay on long-term survival after cancer surgery. Ann. Oncol. 2012, 23, 2731–2737. [Google Scholar] [CrossRef]
- Garbuz, D.S.; Xu, M.; Duncan, C.P.; Masri, B.A.; Sobolev, B. Delays worsen quality of life outcome of primary total hip arthroplasty. Clin. Orthop. Relat. Res. (1976–2007) 2006, 447, 79–84. [Google Scholar] [CrossRef]
- Grass, F.; Behm, K.T.; Duchalais, E.; Crippa, J.; Spears, G.M.; Harmsen, W.S.; Hübner, M.; Mathis, K.L.; Kelley, S.R.; Pemberton, J.H. Impact of delay to surgery on survival in stage I-III colon cancer. Eur. J. Surg. Oncol. 2020, 46, 455–461. [Google Scholar] [CrossRef]
- Balibrea, J.M.; Badia, J.M.; Pérez, I.R.; Antona, E.M.; Peña, E.Á.; Botella, S.G.; Gallego, M.A.; Pérez, E.M.; Cortijo, S.M.; Miguelanez, I.P. Manejo quirúrgico de pacientes con infección por COVID-19. Recomendaciones de la Asociación Española de Cirujanos. Cirugía Española 2020, 98, 251–259. [Google Scholar] [CrossRef]
- Aziz, H.; Filkins, A.; Kwon, Y.K. Review of COVID-19 outcomes in surgical patients. Am. Surg. 2020, 86, 741–745. [Google Scholar] [CrossRef]
- Lei, S.; Jiang, F.; Su, W.; Chen, C.; Chen, J.; Mei, W.; Zhan, L.-Y.; Jia, Y.; Zhang, L.; Liu, D. Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. EClinicalMedicine 2020, 21, 100331. [Google Scholar] [CrossRef] [PubMed]
- Alkhlewi, M.N.; Farhat, A.M.; Borah, R.A.; Al Yamani, W.A.A. Tendency of Patients to Delay Emergency Department Visits and Avoid Medical Care During the Viral COVID-19 Pandemic: A Cross-Sectional Survey Study in Saudi Arabia. Saudi J. Emerg. Med. 2021, 2, 125. [Google Scholar] [CrossRef]
- Taylor, S.; Landry, C.A.; Rachor, G.S.; Paluszek, M.M.; Asmundson, G.J. Fear and avoidance of healthcare workers: An important, under-recognized form of stigmatization during the COVID-19 pandemic. J. Anxiety Disord. 2020, 75, 102289. [Google Scholar] [CrossRef] [PubMed]
- Deputy, M.; Rao, C.; Worley, G.; Balinskaite, V.; Bottle, A.; Aylin, P.; Burns, E.; Faiz, O. Effect of the SARS-CoV-2 pandemic on mortality related to high-risk emergency and major elective surgery. Br. J. Surg. 2021, 108, 754–759. [Google Scholar] [CrossRef]
- Challine, A.; Dousset, B.; de’Angelis, N.; Lefèvre, J.H.; Parc, Y.; Katsahian, S.; Lazzati, A. Impact of coronavirus disease 2019 (COVID-19) lockdown on in-hospital mortality and surgical activity in elective digestive resections: A nationwide cohort analysis. Surgery 2021, 170, 1644–1649. [Google Scholar] [CrossRef]
- Collaborative, C. Effect of COVID-19 pandemic lockdowns on planned cancer surgery for 15 tumour types in 61 countries: An international, prospective, cohort study. Lancet Oncol. 2021, 22, 1507–1517. [Google Scholar]
- Thornton, J. COVID-19: A & E Visits in England Fall by 25% in Week after Lockdown; British Medical Journal Publishing Group: London, UK, 2020. [Google Scholar]
- Porreca, A.; Colicchia, M.; D’Agostino, D.; Amenta, M.; Corsaro, A.; Zaramella, S.; Zegna, L.; Gallo, F.; Schenone, M.; Bozzini, G. Urology in the time of coronavirus: Reduced access to urgent and emergent urological care during the coronavirus disease 2019 outbreak in Italy. Urol. Int. 2020, 104, 631–636. [Google Scholar] [CrossRef]
- Das, G.; Khanna, S.; Purkayastha, J.; Talukdar, A.; Kalita, D.; Kamalasanan, K.; Bannoth, S.; Yadav, J.; Ramchandani, S. Impact of COVID-19 Pandemic on a Tertiary Care Center’s Surgical Volume and Outcomes: A Single Institutional Study from Northeast India. Indian J. Surg. Oncol. 2021, 12, 265–269. [Google Scholar] [CrossRef]
- Brunner, M.; Krautz, C.; Kersting, S.; Weber, G.F.; Stinner, B.; Benz, S.R.; Grützmann, R. Oncological colorectal surgery during the COVID-19pandemic—A national survey. Int. J. Colorectal Dis. 2020, 35, 2219–2225. [Google Scholar] [CrossRef]
- Singh, S.K.; Gupta, A.; Sandhu, H.; Mani, R.; Sharma, J.; Kumar, P.; Rajput, D.; Kumar, N.; Huda, F.; Basu, S.P. Surgical Diseases Management during COVID-19 Crisis at a Tertiary Care Hospital of India: Our Institutional Strategy. Surg. J. 2021, 7, e366–e373. [Google Scholar] [CrossRef]
- Krutsri, C.; Singhatas, P.; Sumpritpradit, P.; Thampongsa, T.; Phuwapraisirisan, S.; Gesprasert, G.; Jirasiritham, J. Impact of the COVID-19 pandemic on the outcome, morbidity, and mortality of acute care surgery patients: A retrospective cohort study. Int. J. Surg. Open 2021, 28, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Surgeons, A. COVID-19: Elective case triage guidelines for surgical care. Am. Coll. Surg. 2020, 24, 11–13. [Google Scholar]
- Ciarleglio, F.A.; Rigoni, M.; Mereu, L.; Tommaso, C.; Carrara, A.; Malossini, G.; Tateo, S.; Tirone, G.; Bjerklund Johansen, T.E.; Benetollo, P.P. The negative effects of COVID-19 and national lockdown on emergency surgery morbidity due to delayed access. World J. Emerg. Surg. 2021, 16, 37. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Interim Guidance for Healthcare Facilities: Preparing for Community Transmission of COVID-19 in the United States; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020. [Google Scholar]
- Ti, L.K.; Ang, L.S.; Foong, T.W.; Ng, B.S.W. What we do when a COVID-19 patient needs an operation: Operating room preparation and guidance. Can. J. Anesth. J. Can. D’anesthésie 2020, 67, 756–758. [Google Scholar] [CrossRef] [Green Version]
- Li, C.-I.; Pai, J.-Y.; Chen, C.-H. Characterization of smoke generated during the use of surgical knife in laparotomy surgeries. J. Air Waste Manag. Assoc. 2020, 70, 324–332. [Google Scholar] [CrossRef]
- De Simone, B.; Chouillard, E.; Di Saverio, S.; Pagani, L.; Sartelli, M.; Biffl, W.; Coccolini, F.; Pieri, A.; Khan, M.; Borzellino, G. Emergency surgery during the COVID-19 pandemic: What you need to know for practice. Ann. R. Coll. Surg. Engl. 2020, 102, 323–332. [Google Scholar] [CrossRef]
- Gacaferi, H.; Collaborative, G.; Collaborative, C. Timing of surgery following SARS-CoV-2 infection: An international prospective cohort study. Anaesthesia 2021, 76. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Control | Lockdown | p-Value |
|---|---|---|---|
| (n = 403) | (n = 253) | ||
| Age * (Mean ± SD) | 43.7 ± 16.03 | 44.5 ± 16.89 | 0.531 |
| Gender ** (Number and %) | 0.646 | ||
| Male | 189 (46.9%) | 114 (45.1%) | |
| Female | 214 (53.1%) | 139 (54.9%) | |
| Nationality ** | 0.775 | ||
| Saudi | 297 (73.7%) | 189 (74.7%) | |
| Non-Saudi | 106 (26.3%) | 64 (25.3%) | |
| BMI ** | 0.005 | ||
| Underweight | 18 (4.5%) | 14 (5.57%) | |
| Healthy | 104 (26%) | 89 (35.45%) | |
| Overweight | 127 (31.75%) | 85 (33.8%) | |
| Obese | 154 (38.21%) | 63 (25.1%) | |
| Smoker ** | 33 (8.19%) | 9 (3.55%) | 0.018 |
| Non-Smoker | 370 (91.81%) | 244 (96.45%) | |
| ASA Score ** | 0.019 | ||
| Class 1 | 157 (39.05%) | 76 (30.0%) | |
| Class 2 | 182 (45.3%) | 115 (45.45%) | |
| Class 3 | 57 (14.16%) | 56 (22.1%) | |
| Class 4 or more | 7 (1.49%) | 6 (2.27%) | |
| Chronic anticoagulant use ** | 15 (3.72%) | 15 (5.92%) | 0.188 |
| Immunosuppression therapy use ** | 29 (7.19%) | 23 (9.09%) | 0.382 |
| Characteristic | Control | Lockdown | p-Value |
|---|---|---|---|
| (n = 403) | (n = 253) | ||
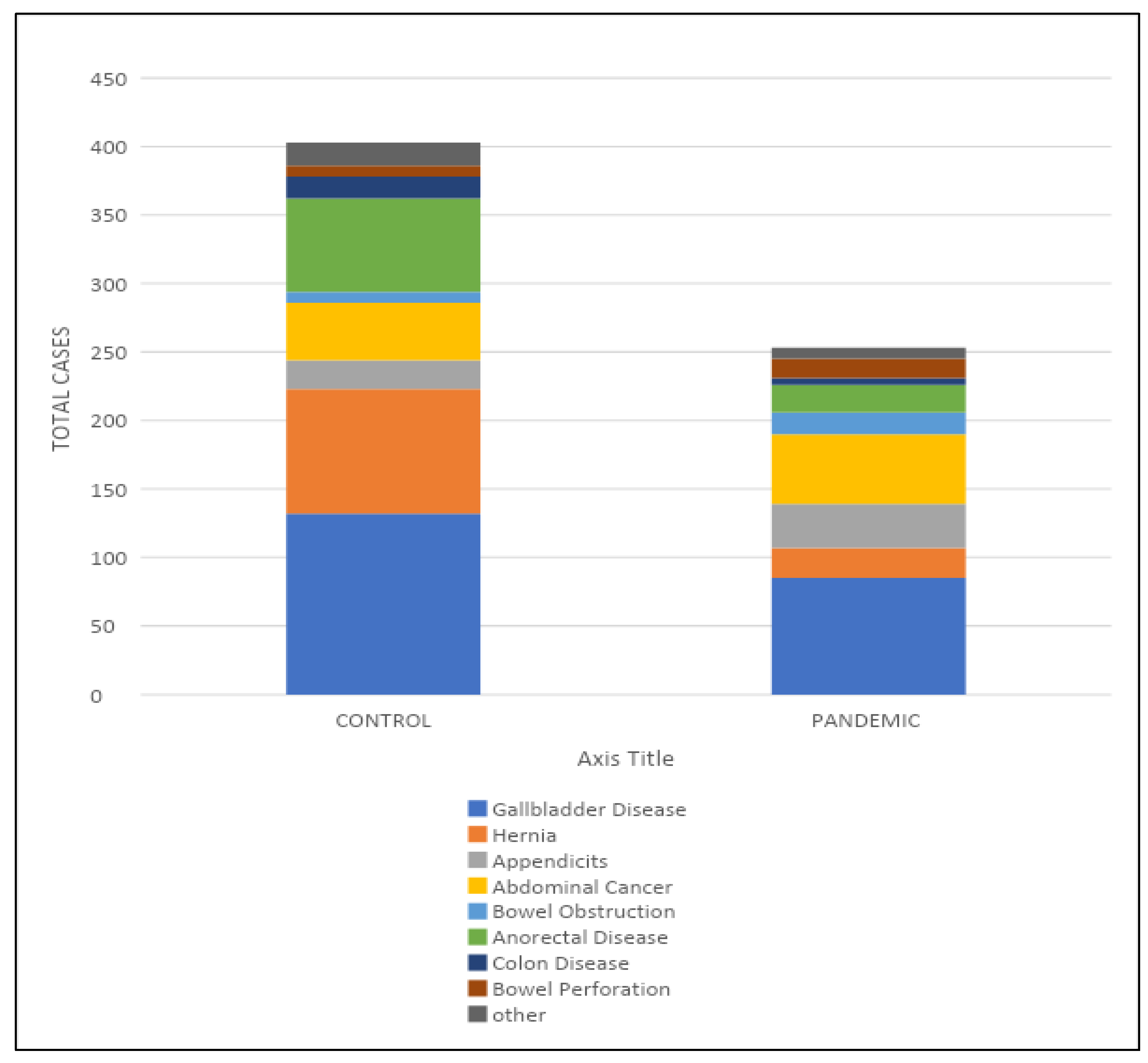
| Diagnosis ** | 0.001 | ||
| Gallbladder disease | 132 (32.75%) | 85 (33.6%) | |
| Hernia | 91 (22.58%) | 22 (8.7%) | |
| Appendicitis | 21 (5.21%) | 32 (12.6%) | |
| Abdominal cancer | 42 (10.42%) | 51 (20.2%) | |
| Bowel obstruction | 8 (1.98%) | 16 (6.3%) | |
| Anorectal disease | 68 (16.87%) | 20 (7.9%) | |
| Colon disease | 16 (3.97%) | 5 (1.98%) | |
| Bowel perforation | 8 (1.98%) | 14 (5.53%) | |
| Others | 17 (4.2%) | 8 (3.1%) | |
| DVT prophylaxis use ** | 166 (41.19%) | 99 (39.1%) | 0.601 |
| Duration of surgery * (minutes) | 133.7 (120.32) | 166.8 (135.10) | 0.002 |
| Mean (SD) | |||
| Status of surgery ** | <0.001 | ||
| Elective | 326 (80.89%) | 95 (37.5%) | |
| emergency | 77 (19.1%) | 158 (62.4%) | |
| Re-operation ** | 3 (0.74%) | 11 (4.34%) | 0.002 |
| Intra-operative blood transfusion ** | 33 (8.18%) | 35 (13.8%) | 0.021 |
| Post-operative blood transfusion ** | 17 (4.21%) | 22 (8.7%) | 0.018 |
| Infection category ** | <0.001 | ||
| Clean | 80 (21.85%) | 18 (7.1%) | |
| Clean/contaminated | 179 (45%) | 130 (51.4%) | |
| Contaminated | 127 (31.9%) | 96 (37.9%) | |
| Dirty | 7 (1.25%) | 9 (3.6%) |
| Characteristic | Control | Lockdown | p-Value |
|---|---|---|---|
| (n = 403) | (n = 253) | ||
| Length of stay * | 3.43 (8.78) | 5.83 (10.21) | 0.002 |
| Mean (SD) | |||
| Clavien-Dindo Classification ** | 0.003 | ||
| Grade 1 | 54 (41.5%) | 88 (49.4%) | |
| Grade 2 | 11 (8.46%) | 17 (9.55%) | |
| Grade 3 | 2 (1.53%) | 18 (10.11%) | |
| Grade 4 | 58 (44.6%) | 48 (26.96%) | |
| Grade 5 | 5(3.84%) | 7 (3.93%) | |
| Discharge ** | 341 (84.7%) | 198 (78.3%) | 0.039 |
| Not-discharge | 62 (15.3%) | 55 (21.7%) | |
| Complication ** | 41 (10.1%) | 48 (18.9%) | 0.001 |
| Risk Factors | p-Value | OR | 95% C.I. for OR | Nagelkerke R Square | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Age at Diagnosis | 0.005 | 1.027 | 1.008 | 1.047 | 0.051 | |
| Sex | Male | Ref. | ||||
| Female | 0.019 | 0.464 | 0.244 | 0.882 | 0.035 | |
| BMI | Underweight (<18.5 kg/m2) | Ref. | 0.018 | |||
| Healthy (18.5–24.9 kg/m2) | 0.204 | 0.456 | 0.136 | 1.529 | ||
| Overweight (25–29.9 kg/m2) | 0.128 | 0.386 | 0.113 | 1.316 | ||
| Obese (≥30 kg/m2) | 0.100 | 0.340 | 0.094 | 1.228 | ||
| Smoker | Yes | 0.800 | 1.230 | 0.247 | 6.115 | 0.000 |
| Diagnosis | Gallbladder disease | Ref. | 0.360 | |||
| Hernia | 0.288 | 2.733 | 0.428 | 17.466 | ||
| Appendicitis | 0.522 | 1.822 | 0.290 | 11.444 | ||
| Abdominal cancer | 0.001 | 12.495 | 3.422 | 45.623 | ||
| Bowel obstruction | 0.001 | 27.333 | 6.023 | 124.042 | ||
| Anorectal disease | 0.758 | 1.439 | 0.142 | 14.603 | ||
| Colon disease | 0.001 | 109.333 | 9.195 | 1299.994 | ||
| Bowel perforation | 0.001 | 49.200 | 10.051 | 240.836 | ||
| Other | 0.003 | 16.400 | 2.611 | 102.997 | ||
| Known case of cancer | Yes | 0.002 | 4.232 | 1.706 | 10.498 | 0.056 |
| Cardiac disease | Yes | 0.046 | 2.746 | 1.019 | 7.399 | 0.023 |
| Chronic immunosuppressive therapy | Yes | 0.003 | 3.887 | 1.588 | 9.510 | 0.051 |
| Chronic anticoagulation | Yes | 0.001 | 7.654 | 2.577 | 22.731 | 0.083 |
| Status of surgery | Elective | 0.012 | ||||
| Emergency | 0.185 | 1.586 | 0.802 | 3.139 | ||
| Reoperation | Yes | 0.001 | 23.423 | 4.873 | 112.589 | 0.132 |
| Blood transfusion intraoperatively | Yes | 0.001 | 17.636 | 7.689 | 40.452 | 0.294 |
| Blood transfusion post-operative | Yes | 0.001 | 16.583 | 6.041 | 45.522 | 0.203 |
| Duration of surgery (minutes) | 0.001 | 1.005 | 1.003 | 1.007 | 0.121 | |
| Infection category | Clean | Ref. | 0.211 | |||
| Clean/contaminated | 0.829 | 1.264 | 0.151 | 10.613 | ||
| Contaminated | 0.034 | 9.323 | 1.189 | 73.123 | ||
| Dirty | 0.034 | 13.600 | 1.225 | 151.045 | ||
| LOS | 0.001 | 1.332 | 1.219 | 1.456 | 0.496 | |
| ASAC | Class 1 | Ref. | 0.251 | |||
| Class 2 | 0.026 | 4.221 | 1.192 | 14.944 | ||
| Class 3 | 0.001 | 16.960 | 4.756 | 60.477 | ||
| Class 4 or more | 0.001 | 121.667 | 10.628 | 1392.816 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alelyani, R.H.; Alghamdi, A.H.; Mahrous, S.M.; Alamri, B.M.; Alhiniah, M.H.; Abduh, M.S.; Aldaqal, S.M. Impact of COVID-19 Pandemic Lockdown on the Prognosis, Morbidity, and Mortality of Patients Undergoing Elective and Emergency Abdominal Surgery: A Retrospective Cohort Study in a Tertiary Center, Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 15660. https://doi.org/10.3390/ijerph192315660
Alelyani RH, Alghamdi AH, Mahrous SM, Alamri BM, Alhiniah MH, Abduh MS, Aldaqal SM. Impact of COVID-19 Pandemic Lockdown on the Prognosis, Morbidity, and Mortality of Patients Undergoing Elective and Emergency Abdominal Surgery: A Retrospective Cohort Study in a Tertiary Center, Saudi Arabia. International Journal of Environmental Research and Public Health. 2022; 19(23):15660. https://doi.org/10.3390/ijerph192315660
Chicago/Turabian StyleAlelyani, Rakan H., Ali H. Alghamdi, Saad M. Mahrous, Bader M. Alamri, Mudhawi H. Alhiniah, Maisa S. Abduh, and Saleh M. Aldaqal. 2022. "Impact of COVID-19 Pandemic Lockdown on the Prognosis, Morbidity, and Mortality of Patients Undergoing Elective and Emergency Abdominal Surgery: A Retrospective Cohort Study in a Tertiary Center, Saudi Arabia" International Journal of Environmental Research and Public Health 19, no. 23: 15660. https://doi.org/10.3390/ijerph192315660