
Elevated Procalcitonin Is Positively Associated with the Severity of COVID-19: A Meta-Analysis Based on 10 Cohort Studies

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion Criteria and Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Methods
3. Results
3.1. Literature Search and Study Characteristics
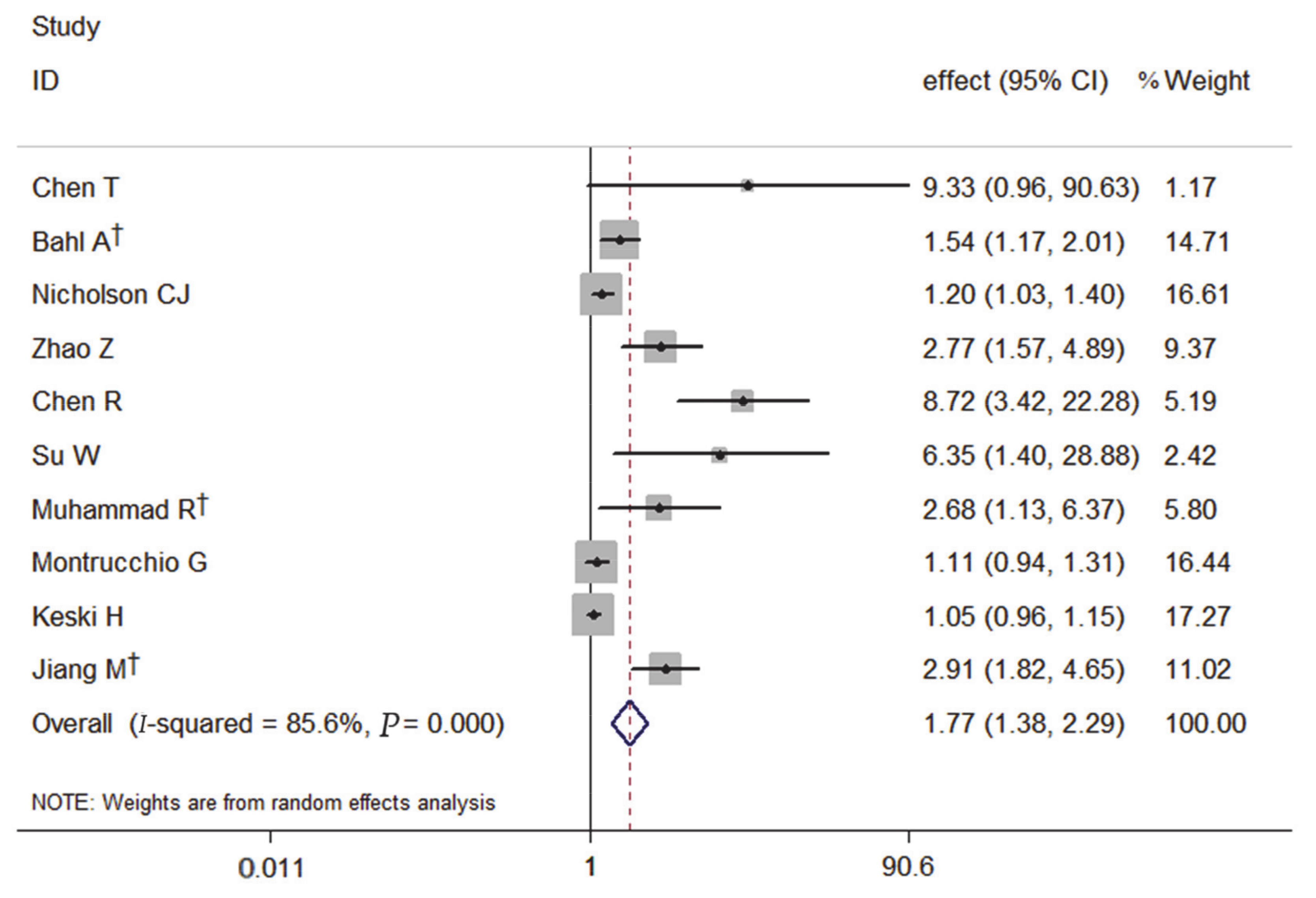
3.2. PCT and the Severity of COVID-19
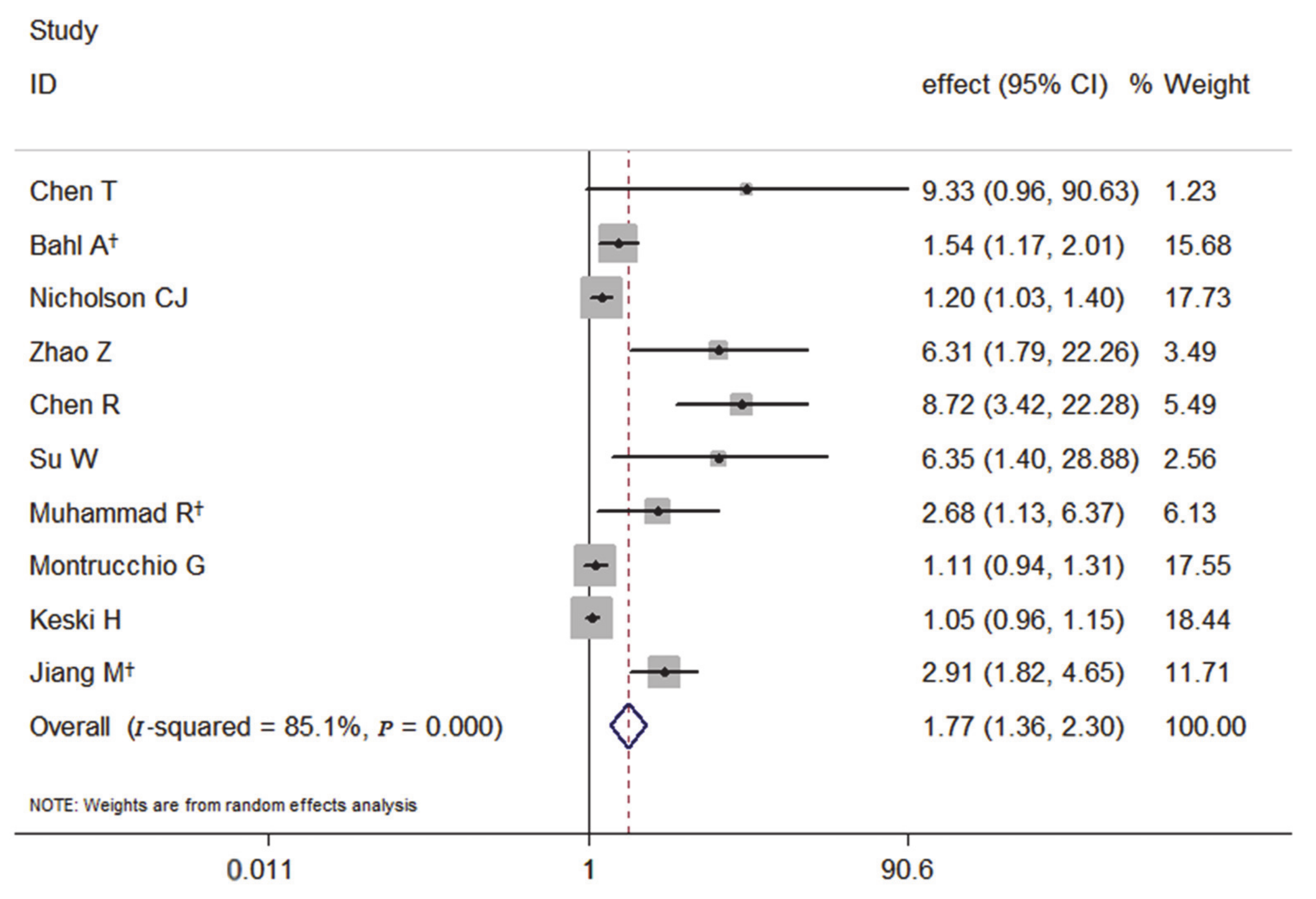
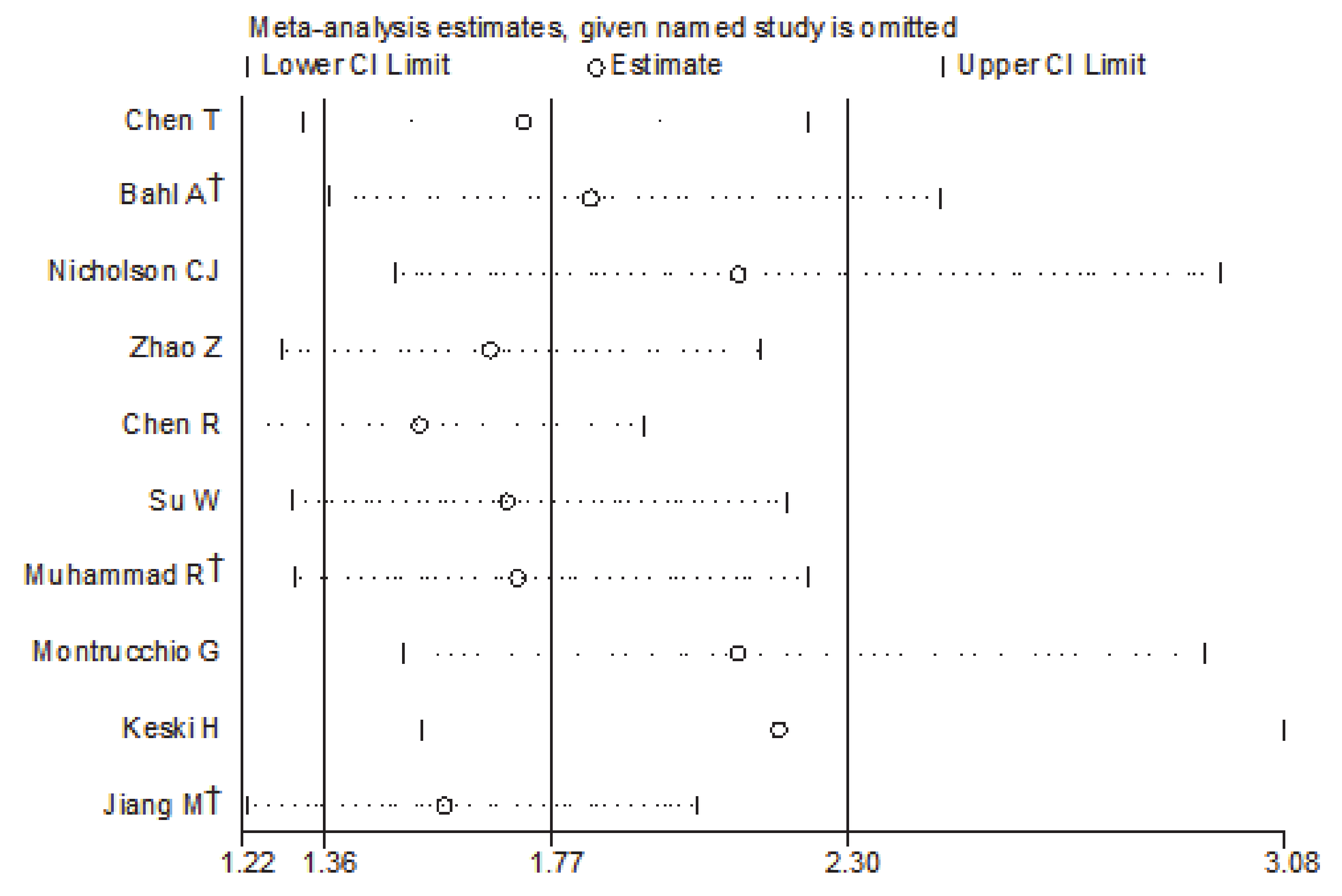
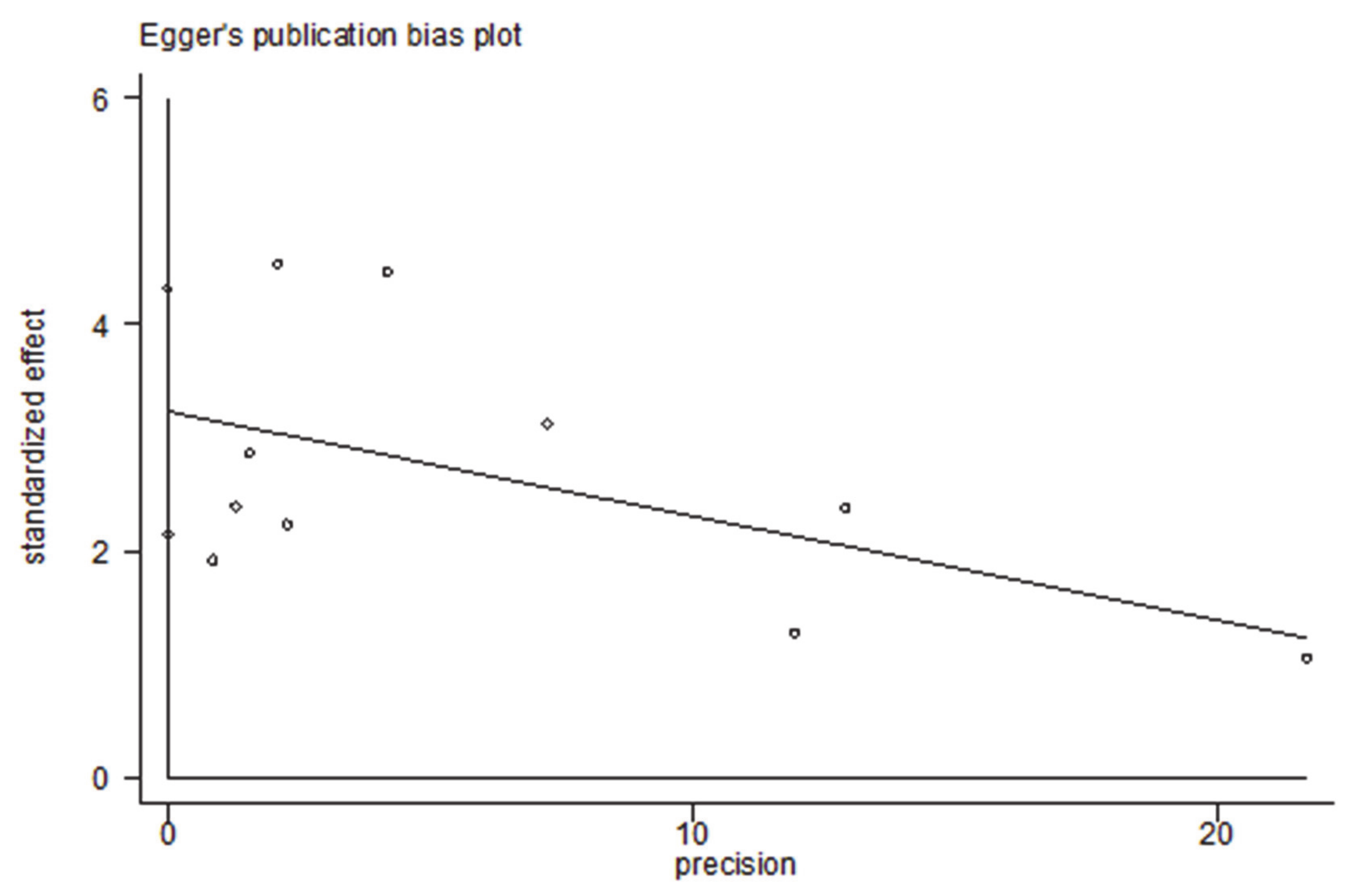
3.3. Subgroup and Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Worldometers.info. The United States: Dadax, Inc. Available online: https://www.worldometers.info/coronavirus/ (accessed on 21 March 2021).
- Batah, S.S.; Fabro, A.T. Pulmonary pathology of ARDS in COVID-19: A pathological review for clinicians. Respir. Med. 2021, 176, 106239. [Google Scholar] [CrossRef] [PubMed]
- Zafer, M.M.; El-Mahallawy, H.A.; Ashour, H.M. Severe COVID-19 and sepsis: Immune pathogenesis and laboratory markers. Microorganisms 2021, 9, 159. [Google Scholar] [CrossRef] [PubMed]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; Macary, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Recovery Collaborative Group. Azithromycin in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 605–612. [Google Scholar] [CrossRef]
- Ji, P.; Zhu, J.; Zhong, Z.; Li, H.; Pang, J.; Li, B. Association of elevated inflammatory markers and severe COVID-19: A me-ta-analysis. Medicine 2020, 99, e23315. [Google Scholar] [CrossRef]
- Becker, K.L.; Nylen, E.S.; White, J.C. Procalcitonin and the calcitonin gene family of peptides in inflammation, infection, and sepsis: A journey from calcitonin back to its precursors. J. Clin. Endocrinol. Metab. 2004, 89, 1512. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Wang, J.; Wei, B. The diagnostic value of Fe(3+) and inflammation indicators in the death of sepsis patients: A retrospective study of 428 patients. Ther. Clin. Risk Manag. 2021, 17, 55–63. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Zeng, Z.; Yu, H.; Chen, H.; Qi, W.; Chen, L.; Chen, G.; Yan, W.; Chen, T.; Ning, Q.; Han, M.; et al. Longitudinal changes of inflammatory parameters and their correlation with disease severity and outcomes in patients with COVID-19 from Wuhan, China. Crit. Care 2020, 24, 1–12. [Google Scholar] [CrossRef]
- Su, W.; Qiu, Z.; Zhou, L.; Hou, J.; Wang, Y.; Huang, F.; Zhang, Y.; Jia, Y.; Zhou, J.; Liu, D.; et al. Sex differences in clinical characteristics and risk factors for mortality among severe patients with COVID-19: A retrospective study. Aging 2020, 12, 18833–18843. [Google Scholar] [CrossRef]
- Keski, H. Hematological and inflammatory parameters to predict the prognosis in COVID-19. Indian J. Hematol. Blood Transfus. 2021, 2, 1–9. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; A Ioannidis, J.P.; Clarke, M.; Devereaux, P.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease Is Suspected: Interim Guidance, 13 March 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- The National Health Commission. Diagnosis and treatment protocol for COVID-19 patients (tentative 8th edition). Infect. Dis. Immun. 2021, 1, 17. [Google Scholar]
- Farace, D.J. Proceedings of the 4th International Conference on Grey Literature: New Frontiers in Grey Literature, Washington, DC, USA, 4–5 October 1999; Available online: https://doi.org/10.1108/al.1999.17308gab.010 (accessed on 1 July 1999).
- Wells, G. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomised Studies in Meta Analyses; Ottawa Health Research Institute: Ottawa, ON, Canada, 2019. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials. 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088. [Google Scholar] [CrossRef]
- Chen, T.; Dai, Z.; Mo, P.; Li, X.; Ma, Z.; Song, S.; Chen, X.; Luo, M.; Liang, K.; Gao, S.; et al. Clinical characteristics and outcomes of older patients with coronavirus disease 2019 (COVID-19) in Wuhan, China: A single-centered, retrospective study. J. Gerontol. Biol. Sci. Med. Sci. 2020, 75, 1788–1795. [Google Scholar] [CrossRef]
- Bahl, A.; Van Baalen, M.N.; Ortiz, L.; Chen, N.W.; Todd, C.; Milad, M. Early predictors of in-hospital mortality in patients with COVID-19 in a large American cohort. Intern. Emerg. Med. 2020, 15, 1485–1499. [Google Scholar] [CrossRef]
- Nicholson, C.J.; Wooster, L.; Sigurslid, H.H.; Li, R.H.; Jiang, W.; Tian, W.; Cardenas, C.L.L.; Malhotra, R. Estimating risk of mechanical ventilation and in-hospital mortality among adult COVID-19 patients admitted to Mass General Brigham: The VICE and DICE scores. medRxiv 2021, 33, 100765. [Google Scholar] [CrossRef]
- Zhao, Z.; Chen, A.; Hou, W.; Graham, J.M.; Li, H.; Richman, P.S.; Thode, H.C.; Singer, A.J.; Duong, T.Q. Prediction model and risk scores of ICU admission and mortality in COVID-19. PLoS ONE 2020, 15, e0236618. [Google Scholar] [CrossRef]
- Chen, R.; Liang, W.; Jiang, M.; Guan, W.; Zhan, C.; Wang, T.; Tang, C.; Sang, L.; Liu, J.; Ni, Z.; et al. Risk factors of fatal outcome in hospitalized subjects with coronavirus disease 2019 from a nationwide analysis in China. Chest 2020, 158, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, R.; Ogunti, R.; Ahmed, B.; Munawar, M.; Donaldson, S.; Sumon, M.; Kibreab, A.; Thomas, A.N.; Mehari, A. Clinical characteristics and predictors of mortality in minority patients hospitalized with COVID-19 infection. J. Racial Ethn. Heal. Disparities 2021, 2, 1–11. [Google Scholar] [CrossRef]
- Montrucchio, G.; Sales, G.; Rumbolo, F.; Palmesino, F.; Fanelli, V.; Urbino, R. Effectiveness of mid-regional pro-adrenomedullin (MR-proADM) as prognostic marker in COVID-19 critically ill patients: An observational prospective study. PLoS ONE 2021, 16, e0246771. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Li, C.; Zheng, L.; Lv, W.; He, Z.; Cui, X.; Dietrich, C.F. A biomarker-based age, biomarkers, clinical history, sex (ABCS)-mortality risk score for patients with coronavirus disease 2019. Ann. Transl. Med. 2021, 9, 230. [Google Scholar] [CrossRef]
- Sayah, W.; Berkane, I.; Guermache, I.; Sabri, M.; Lakhal, F.Z.; Rahali, S.Y.; Djidjeli, A.; Mahammed, L.L.; Merah, F.; Belaid, B.; et al. Interleukin-6, procalcitonin and neutrophil-to-lymphocyte ratio: Potential immune-inflammatory parameters to identify severe and fatal forms of COVID-19. Cytokine 2021, 141, 155428. [Google Scholar] [CrossRef]
- Bustros, A.D.; Ball, D.W.; Peters, R.; Compton, D.; Nelkin, B.D. Regulation of human calcitonin gene transcription by cyclic AMP. Biochem. Biophys. Res. Commun. 1992, 189, 1157–1164. [Google Scholar] [CrossRef]
- Russwurm, S.; Wiederhold, M.; Oberhoffer, M.; Stonāns, I.; Zipfel, P.F.; Reinhart, K. Molecular aspects and natural source of procalcitonin. Clin. Chem. Lab. Med. 1999, 37, 789–797. [Google Scholar] [CrossRef]
- Conti, P.; Ronconi, G.; Caraffa, A.; Gallenga, C.E.; Ross, R.; Frydas, I. Induction of pro-inflammatory cytokines (IL-1 and IL-6) and lung inflammation by Coronavirus-19 (COVI-19 or SARS-CoV-2): Anti-inflammatory strategies. J. Biol. Regul. Homeost. Agents 2020, 34, 327–331. [Google Scholar]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Wan, S.; Yi, Q.; Fan, S.; Lv, J.; Zhang, X.; Guo, L. Characteristics of lymphocyte subsets and cytokines in peripheral blood of 123 hospitalized patients with 2019 novel coronavirus pneumonia (NCP). medRxiv 2020, 2. [Google Scholar] [CrossRef] [Green Version]
- Meisner, M. Pathobiochemistry and clinical use of procalcitonin. Clin. Chim. Acta 2002, 323, 17–29. [Google Scholar] [CrossRef]
- Hamade, B.; Huang, D.T. Procalcitonin: Where are we now? Crit. Care Clin. 2020, 36, 23–40. [Google Scholar] [CrossRef]
- Liu, D.; Su, L.; Guan, W.; Xiao, K.; Xie, L. Prognostic value of procalcitonin in pneumonia: A systematic review and meta-analysis. Respirology 2015, 21, 280–288. [Google Scholar] [CrossRef] [Green Version]
- Gautam, S.; Cohen, A.J.; Stahl, Y.; Toro, P.V.; Young, G.M.; Datta, R.; Yan, X.; Ristic, N.T.; Bermejo, S.D.; Sharma, L.; et al. Severe respiratory viral infection induces procalcitonin in the absence of bacterial pneumonia. Thorax 2020, 75, 974–981. [Google Scholar] [CrossRef]
- Gao, Y.-D.; Ding, M.; Dong, X.; Zhang, J.-J.; Azkur, A.K.; Azkur, D.; Gan, H.; Sun, Y.-L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Wang, J.; Cao, B. Procalcitonin and other markers to guide antibiotic use in chronic obstructive pulmonary disease exacerbations in the era of antimicrobial resistance. Curr. Opin. Pulm. Med. 2019, 25, 158–164. [Google Scholar] [CrossRef]
- Raji, H.; Borsi, H.; Nia, E.P.; Mal-Amir, M.D. Relationship between serum procalcitonin level and chronic obstructive pulmonary disease. J. Fam. Med. Prim. Care 2019, 8, 738. [Google Scholar] [CrossRef]
- Sim, J.K.; Oh, J.Y.; Lee, E.J.; Hur, G.Y.; Lee, S.H.; Lee, S.Y.; Lee, S.Y.; Kim, J.H.; Shin, C.; Shim, J.J.; et al. Serum procalcitonin for differential diagnosis of acute exacerbation and bacterial pneumonia in patients with interstitial lung disease. Am. J. Med. Sci. 2016, 351, 499–505. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Country | Cases (n) | Age (years) | Male n (%) | Study Design | Outcomes | Adjusted OR/RR/HR (95% CI) | Confounders |
|---|---|---|---|---|---|---|---|---|
| Chen | China | 55 | NA | NA | R | death | OR 9.33 (0.96, 90.63) | Age, Comorbidities, Breath Shortness, Time From Illness Onset To First Hospital Admission, AST, Cr, LDH, CRP |
| Bahl | USA | 1461 | 62 ± 17.8 | 770 (52.7) | R | death | HR 1.23 (0.78, 1.94) | Age, Sex, Race, BMI, CAD, Diabetes Mellitus, Hypertension, Respiratory Rate, Breaths Per Minute, Blood Oxygen Saturation, WBC, Hemoglobin, ALT, Creatinine, D-Dimer, Lactic Acid |
| HR 1.37 (0.84, 2.23) | ||||||||
| HR 2.11 (1.34, 3.31) | ||||||||
| Nicholson | China | 1042 | 64 ± 16.3 | 592 (56.8) | R | death | OR 1.202 (1.033, 1.399) | Age, Sex, Diabetes Mellitus, Statin (Chronic Use), ALB, CRP, MCV, Neut: Lymph Ratio, PLT |
| Zhao | China | 641 | 60 | 384 (59.9) | R | death | OR 6.31 (1.79, 22.26) | Age, Heart Failure, LDH, COPD, SpO2, Heart Rate |
| ICU | OR2.77 (1.57, 4.89) | LDH, Smoking, SpO2, LYM count | ||||||
| Chen | China | 1590 | 47.0 ± 65.2 | 904 (56.9) | R | death | HR 8.72 (3.42, 22.28) | Age, CHD, CVD, Dyspnea, AST, TBIL, Creatinine |
| Su | China | 651 | 60.7 ± 16.3 | 332 (51.0) | R | death | OR 6.350 (1.396, 28.882) | Sex, Age, WBC, NEU, LYM Count, PLT Count, CD3, CD4, CD8 |
| Muhammad | United States | 200 | 58.9 ± 15.1 | 121 (60.5) | R | death | OR 2.68 (1.13, 6.37) | Age, Hypertension, CAD, Dyslipidemia, Chronic Kidney Disease, Stroke, Oxygen Saturation, Creatinine, BUN, CPK, Troponin, Lactic Acid, LDH, CRP, Initial D-Dimer, Ferritin, Highest D-Dimer |
| Montrucchio | Italy | 57 | 63.0 ± 12.9 | 50 (87.7) | p | death | OR 1.113 (0.945, 1.312) | Age, Gender, CVD, Diabetes Mellitus, MR-proADM |
| Keski | Turkey | 302 | 57.1 ± 17.6 | 148 (49.0) | R | death | HR 1.05 (0.96, 1.15) | Age, Hypertension, NLR, C-reactive protein, Ferritin, Prothrombin time, aPTT |
| Jiang | China | 1717 | 61.3 ± 14.1 | 739 (48.17) | R | death | HR 2.91 (1.82, 4.65) | Age, Gender, COPD, AST, hs-CRP, hs-TnI, WBC, LYM count, D-dimer |
| Subgroup | Number of Study | Pooled Effects (95% CI) | I2 (%) | P |
|---|---|---|---|---|
| All studies | 10 | 1.77 (1.38–2.29) | 85.6 | 0.000 |
| Effect estimate | ||||
| OR | 6 | 1.65 (1.18–2.31) | 75.0 | 0.001 |
| HR | 4 | 2.16 (1.21–3.84) | 92.7 | 0.000 |
| Sex (male, %) | ||||
| ≥55 | 5 | 1.90 (1.28–2.83) | 86.3 | 0.000 |
| <55 | 4 | 1.81 (1.09–3.00) | 89.4 | 0.000 |
| NA | 1 | 9.33 (0.96–90.63) | ||
| Sample size | ||||
| ≥500 | 6 | 2.47 (1.55–3.94) | 86.6 | 0.000 |
| <500 | 4 | 1.16 (0.93–1.45) | 63.4 | 0.042 |
| Outcomes | ||||
| Death | 9 | 1.66 (1.29–2.14) | 85.1 | 0.000 |
| others | 1 | 2.77 (1.57–4.89) | ||
| Age | ||||
| ≥60 | 6 | 1.68 (1.25–2.25) | 82.4 | 0.000 |
| <60 | 3 | 2.73 (0.75–9.88) | 91.6 | 0.000 |
| NA | 1 | 9.33 (0.96–90.63) | ||
| Diabetes | ||||
| 1 | 3 | 1.23 (1.06–1.44) | 50.7 | 0.132 |
| 0 | 7 | 3.20 (1.59–6.45) | 89.6 | 0.000 |
| Hypertension | ||||
| 1 | 3 | 1.40 (0.94–2.08) | 81.9 | 0.004 |
| 0 | 7 | 2.31 (1.52–3.51) | 86.8 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, Y.; Cheng, C.; Zheng, X.; Jin, Y.; Duan, G.; Chen, M.; Chen, S. Elevated Procalcitonin Is Positively Associated with the Severity of COVID-19: A Meta-Analysis Based on 10 Cohort Studies. Medicina 2021, 57, 594. https://doi.org/10.3390/medicina57060594
Shen Y, Cheng C, Zheng X, Jin Y, Duan G, Chen M, Chen S. Elevated Procalcitonin Is Positively Associated with the Severity of COVID-19: A Meta-Analysis Based on 10 Cohort Studies. Medicina. 2021; 57(6):594. https://doi.org/10.3390/medicina57060594
Chicago/Turabian StyleShen, Yue, Cheng Cheng, Xue Zheng, Yuefei Jin, Guangcai Duan, Mengshi Chen, and Shuaiyin Chen. 2021. "Elevated Procalcitonin Is Positively Associated with the Severity of COVID-19: A Meta-Analysis Based on 10 Cohort Studies" Medicina 57, no. 6: 594. https://doi.org/10.3390/medicina57060594