
A Systematic Review and Meta-Analysis of Serologic Response following Coronavirus Disease 2019 (COVID-19) Vaccination in Solid Organ Transplant Recipients


Abstract
:1. Introduction
2. Methodology
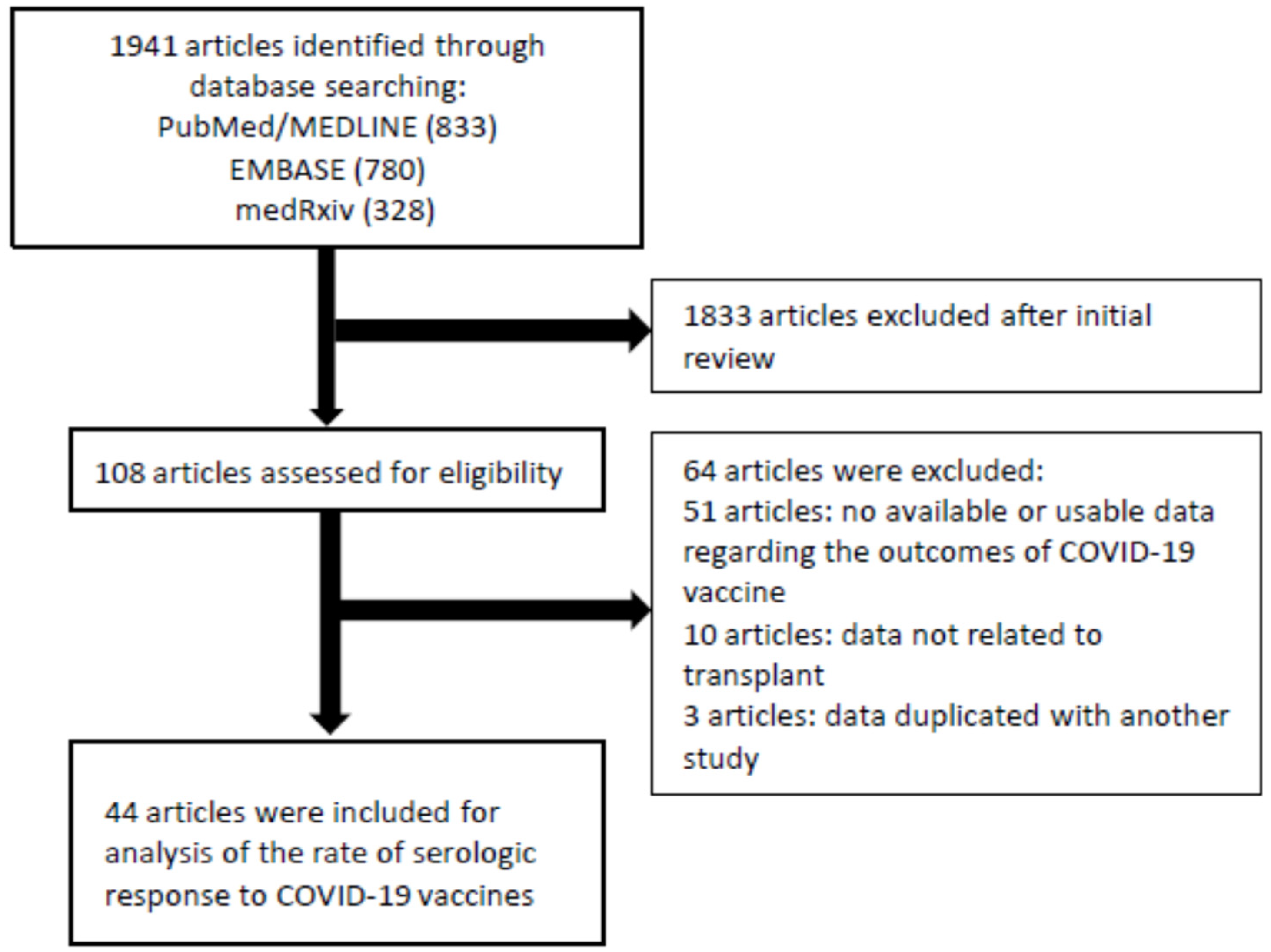
2.1. Search Strategy of Selecting Studies
2.2. Extraction of Data and Assessment of Quality
2.3. Assessment of Outcomes
2.4. Statistical Analysis
2.5. Data Sharing and Access
3. Results
3.1. Study Characteristics
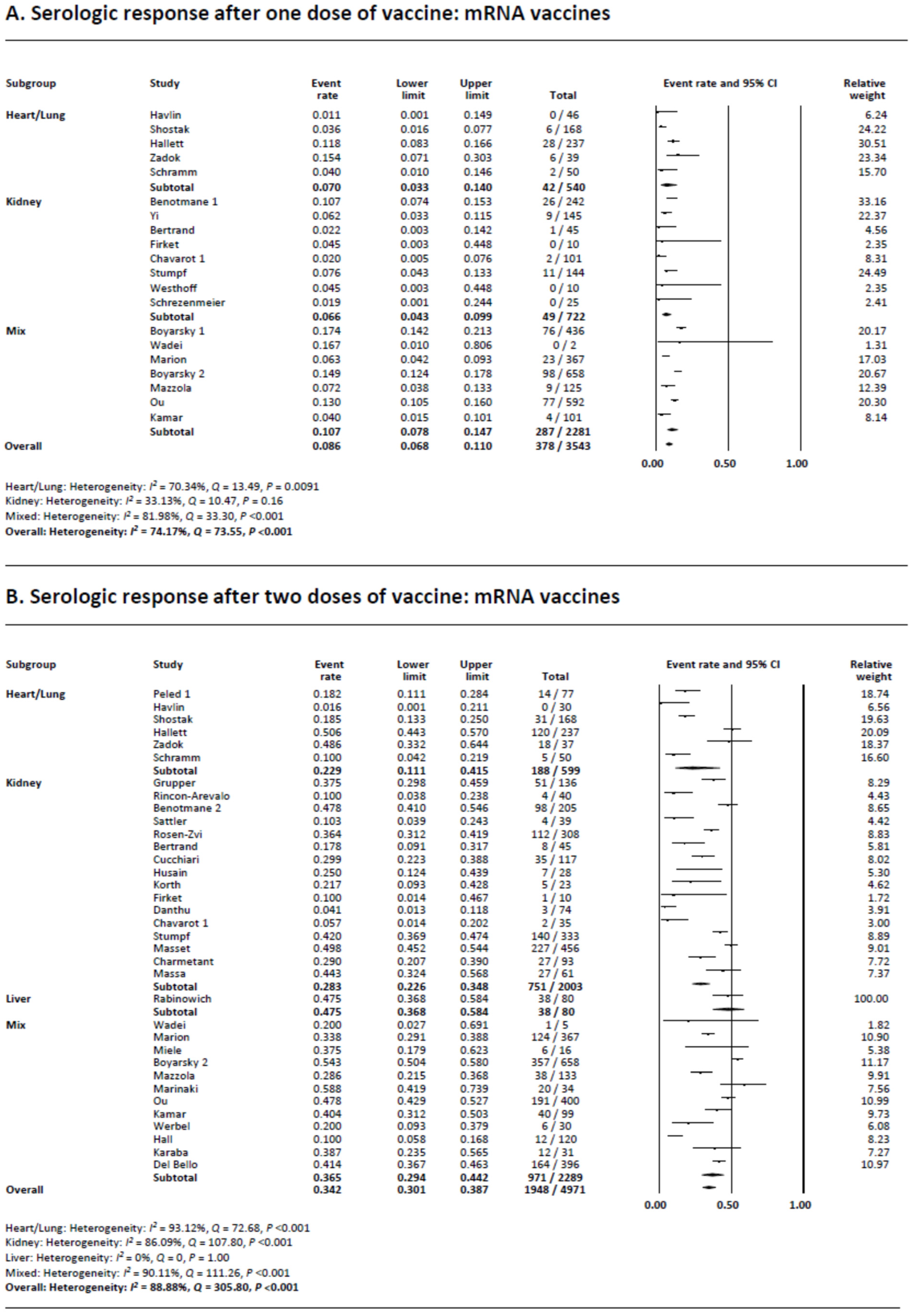
3.2. Serologic Response following a Single Dose of COVID-19 Vaccination
3.3. Serologic Response following Two Doses of COVID-19 Vaccination
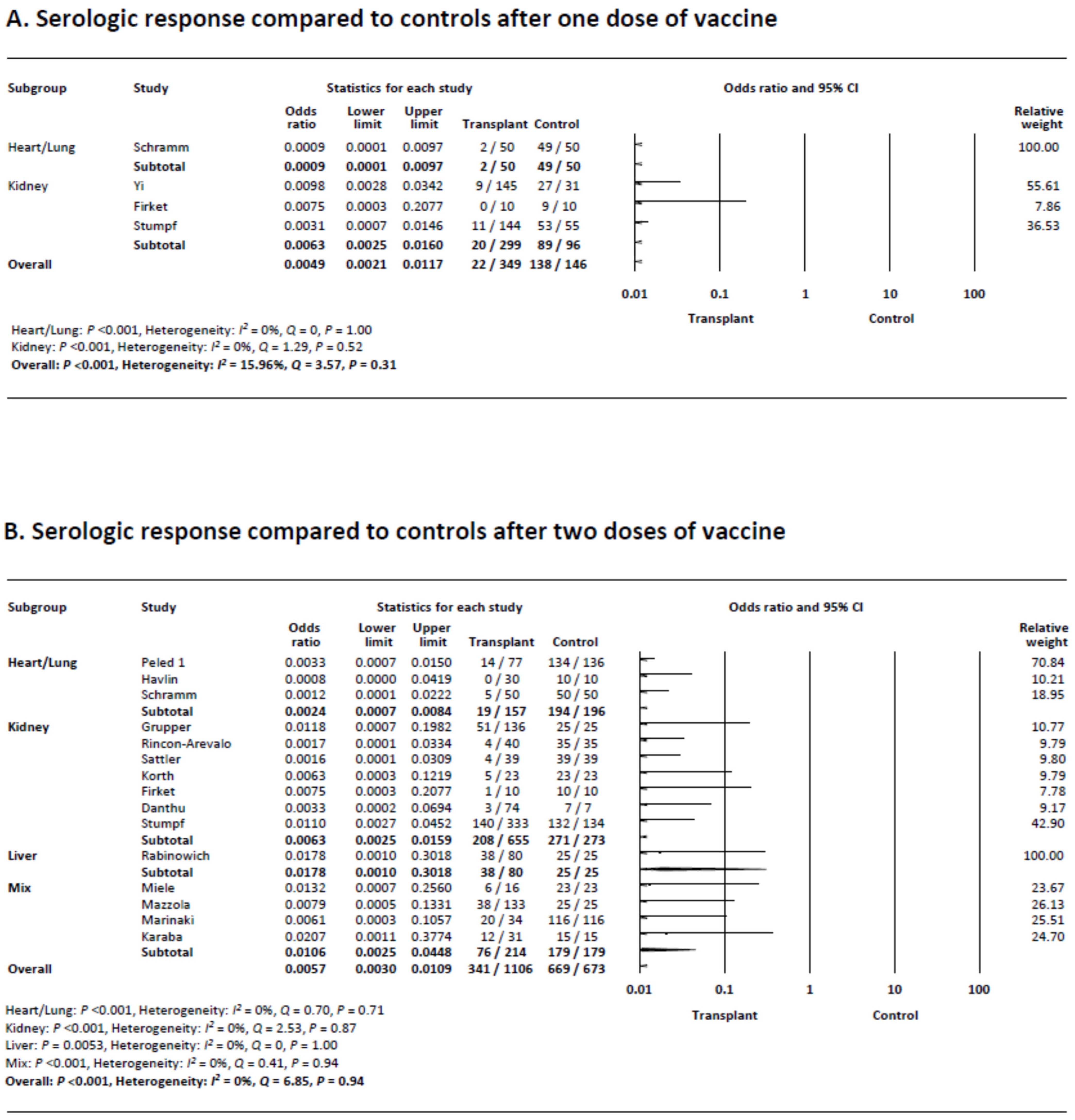
3.4. Serologic Response following a Single Dose of COVID-19 Vaccination Compared to Controls
3.5. Serologic Response following Two Doses of COVID-19 Vaccination Compared to Controls
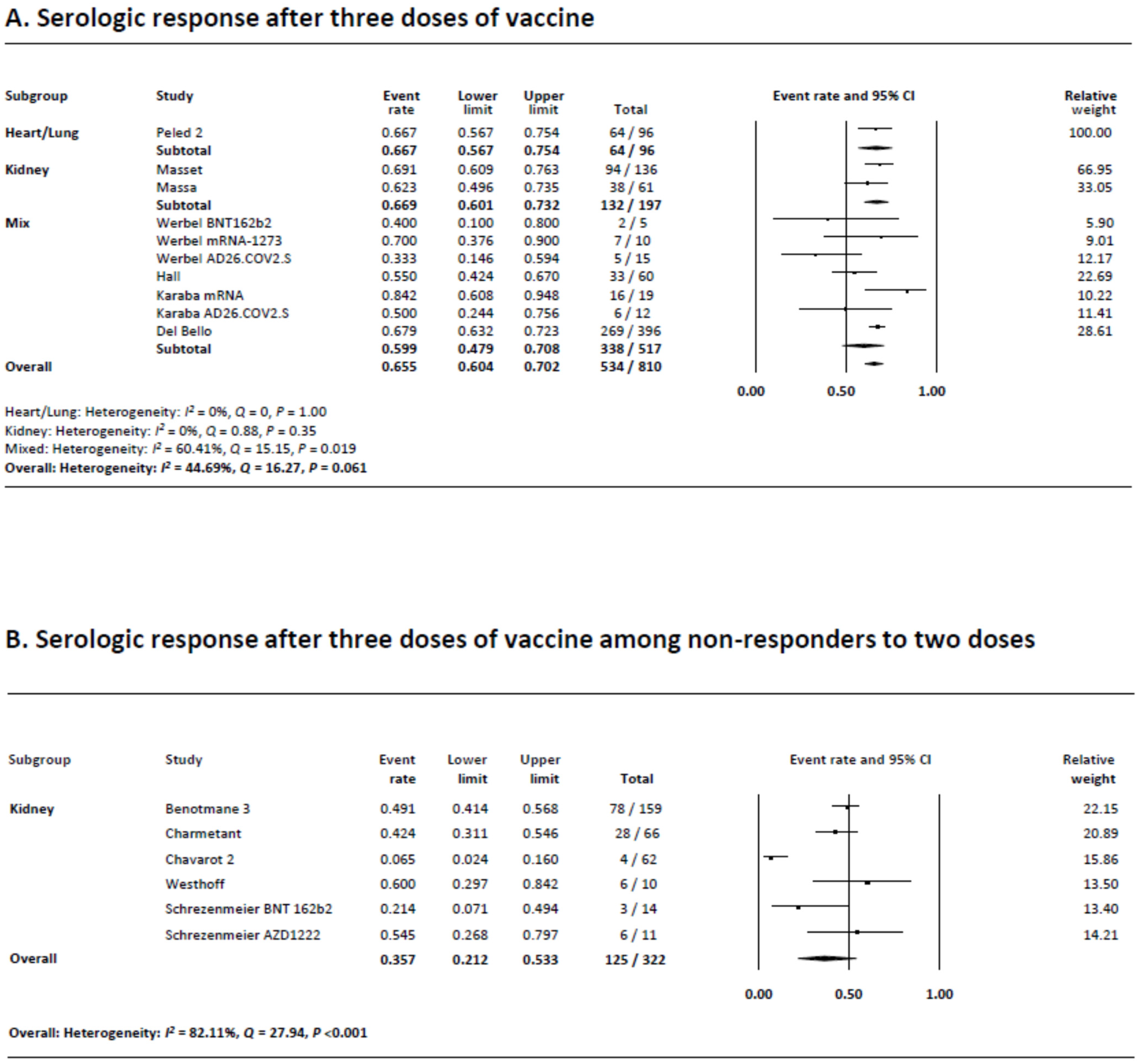
3.6. Serologic Response following Three Doses of COVID-19 Vaccination
3.7. Serologic Response following Three Doses of COVID-19 Vaccination in Non-Responders after Two Doses
3.8. Quality of Evidence Assessed by GRADE
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Wang, J.; Sato, T.; Sakuraba, A. Coronavirus Disease 2019 (COVID-19) Meets Obesity: Strong Association between the Global Overweight Population and COVID-19 Mortality. J. Nutr. 2021, 151, 9–10. [Google Scholar] [CrossRef] [PubMed]
- Salto-Alejandre, S.; Jimenez-Jorge, S.; Sabe, N.; Ramos-Martinez, A.; Linares, L.; Valerio, M.; Martin-Davila, P.; Fernandez-Ruiz, M.; Farinas, M.C.; Blanes-Julia, M.; et al. Risk factors for unfavorable outcome and impact of early post-transplant infection in solid organ recipients with COVID-19: A prospective multicenter cohort study. PLoS ONE 2021, 16, e0250796. [Google Scholar] [CrossRef] [PubMed]
- Wojciechowski, D.; Wiseman, A. Long-Term Immunosuppression Management: Opportunities and Uncertainties. Clin. J. Am. Soc. Nephrol. 2021, 16, 1264–1271. [Google Scholar] [CrossRef]
- Pilch, N.A.; Bowman, L.J.; Taber, D.J. Immunosuppression trends in solid organ transplantation: The future of individualization, monitoring, and management. Pharmacotherapy 2021, 41, 119–131. [Google Scholar] [CrossRef]
- Organ Donation Statistics. Available online: https://www.organdonor.gov/learn/organ-donation-statistics (accessed on 20 September 2021).
- Roberts, M.B.; Fishman, J.A. Immunosuppressive Agents and Infectious Risk in Transplantation: Managing the “Net State of Immunosuppression”. Clin. Infect. Dis. 2021, 73, e1302–e1317. [Google Scholar] [CrossRef]
- Fishman, J.A. Infection in Organ Transplantation. Am. J. Transplant. 2017, 17, 856–879. [Google Scholar] [CrossRef]
- Kronbichler, A.; Gauckler, P.; Windpessl, M.; Il Shin, J.; Jha, V.; Rovin, B.H.; Oberbauer, R. COVID-19: Implications for immunosuppression in kidney disease and transplantation. Nat. Rev. Nephrol. 2020, 16, 365–367. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Ledford, H. Six months of COVID vaccines: What 1.7 billion doses have taught scientists. Nature 2021, 594, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA Vaccine against SARS-CoV-2-Preliminary Report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef] [PubMed]
- Stucchi, R.S.B.; Lopes, M.H.; Kumar, D.; Manuel, O. Vaccine Recommendations for Solid-Organ Transplant Recipients and Donors. Transplantation 2018, 102, S72–S80. [Google Scholar] [CrossRef] [PubMed]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Immunogenicity of a Single Dose of SARS-CoV-2 Messenger RNA Vaccine in Solid Organ Transplant Recipients. JAMA 2021, 325, 1784–1786. [Google Scholar] [CrossRef] [PubMed]
- Massa, F.; Cremoni, M.; Gerard, A.; Grabsi, H.; Rogier, L.; Blois, M.; Couzin, C.; Hassen, N.B.; Rouleau, M.; Barbosa, S.; et al. Safety and cross-variant immunogenicity of a three-dose COVID-19 mRNA vaccine regimen in kidney transplant recipients. EBioMedicine 2021, 73, 103679. [Google Scholar] [CrossRef] [PubMed]
- Masset, C.; Kerleau, C.; Garandeau, C.; Ville, S.; Cantarovich, D.; Hourmant, M.; Kervella, D.; Houzet, A.; Guillot-Gueguen, C.; Guihard, I.; et al. A third injection of the BNT162b2 mRNA COVID-19 vaccine in kidney transplant recipients improves the humoral immune response. Kidney Int. 2021, 100, 1132–1135. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Booth, A. PROSPERO’s progress and activities 2012/13. Syst. Rev. 2013, 2, 111. [Google Scholar] [CrossRef]
- Aromataris, E.M.Z. JBI Manual for Evidence Synthesis. JBI. 2020. Available online: https://synthesismanual.jbi.global (accessed on 1 August 2021).
- Sakuraba, A.; Luna, A.; Micic, D. Serologic response following SARS-COV2 vaccination in patients with cancer: A systematic review and meta-analysis. J. Hematol. Oncol. 2022, 15, 15. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y.; et al. GRADE guidelines: 4. Rating the quality of evidence--study limitations (risk of bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef]
- Sakuraba, A.; Luna, A.; Micic, D. Serologic Response to Coronavirus Disease 2019 (COVID-19) Vaccination in Patients With Immune-Mediated Inflammatory Diseases: A Systematic Review and Meta-analysis. Gastroenterology 2022, 162, 88–108.e9. [Google Scholar] [CrossRef] [PubMed]
- Di Meo, A.; Miller, J.J.; Fabros, A.; Brinc, D.; Hall, V.; Pinzon, N.; Ierullo, M.; Ku, T.; Ferreira, V.H.; Kumar, D.; et al. Evaluation of Three Anti-SARS-CoV-2 Serologic Immunoassays for Post-Vaccine Response. J. Appl. Lab. Med. 2022, 7, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Bmj 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0.; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. Bmj 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Clyne, B.; Walsh, K.A.; O’Murchu, E.; Sharp, M.K.; Comber, L.; KK, O.B.; Smith, S.M.; Harrington, P.; O’Neill, M.; Teljeur, C.; et al. Using preprints in evidence synthesis: Commentary on experience during the COVID-19 pandemic. J. Clin. Epidemiol. 2021, 138, 203–210. [Google Scholar] [CrossRef]
- Chavarot, N.; Morel, A.; Leruez-Ville, M.; Vilain, E.; Divard, G.; Burger, C.; Serris, A.; Sberro-Soussan, R.; Martinez, F.; Amrouche, L.; et al. Weak antibody response to three doses of mRNA vaccine in kidney transplant recipients treated with belatacept. Am. J. Transplant. 2021, 21, 4043–4051. [Google Scholar] [CrossRef]
- Hall, V.G.; Ferreira, V.H.; Ku, T.; Ierullo, M.; Majchrzak-Kita, B.; Chaparro, C.; Selzner, N.; Schiff, J.; McDonald, M.; Tomlinson, G.; et al. Randomized Trial of a Third Dose of mRNA-1273 Vaccine in Transplant Recipients. N. Engl. J. Med. 2021, 385, 1244–1246. [Google Scholar] [CrossRef]
- Peled, Y.; Ram, E.; Lavee, J.; Segev, A.; Matezki, S.; Wieder-Finesod, A.; Halperin, R.; Mandelboim, M.; Indenbaum, V.; Levy, I.; et al. Third dose of the BNT162b2 vaccine in heart transplant recipients: Immunogenicity and clinical experience. J. Heart Lung Transplant. 2022, 41, 148–157. [Google Scholar] [CrossRef]
- Benotmane, I.; Gautier, G.; Perrin, P.; Olagne, J.; Cognard, N.; Fafi-Kremer, S.; Caillard, S. Antibody Response After a Third Dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients With Minimal Serologic Response to 2 Doses. JAMA 2021, 326, 1063–1065. [Google Scholar] [CrossRef]
- Del Bello, A.; Abravanel, F.; Marion, O.; Couat, C.; Esposito, L.; Lavayssiere, L.; Izopet, J.; Kamar, N. Efficiency of a boost with a third dose of anti-SARS-CoV-2 messenger RNA-based vaccines in solid organ transplant recipients. Am. J. Transplant. 2022, 22, 322–323. [Google Scholar] [CrossRef] [PubMed]
- Charmetant, X.; Espi, M.; Barba, T.; Ovize, A.; Morelon, E.; Thaunat, O. Predictive factors of response to 3rd dose of COVID-19 mRNA vaccine in kidney transplant recipients. medRxiv 10.1101/2021.08.23.21262293, 2021.2008.2023.21262293. 2021. [Google Scholar] [CrossRef]
- Westhoff, T.H.; Seibert, F.S.; Anft, M.; Blazquez-Navarro, A.; Skrzypczyk, S.; Zgoura, P.; Meister, T.L.; Pfaender, S.; Stumpf, J.; Hugo, C.; et al. A third vaccine dose substantially improves humoral and cellular SARS-CoV-2 immunity in renal transplant recipients with primary humoral nonresponse. Kidney Int. 2021, 100, 1135–1136. [Google Scholar] [CrossRef] [PubMed]
- Schrezenmeier, E.; Rincon-Arevalo, H.; Stefanski, A.L.; Potekhin, A.; Straub-Hohenbleicher, H.; Choi, M.; Bachmann, F.; Pross, V.; Hammett, C.; Schrezenmeier, H.; et al. B and T Cell Responses after a Third Dose of SARS-CoV-2 Vaccine in Kidney Transplant Recipients. J. Am. Soc. Nephrol. 2021, 32, 3027–3033. [Google Scholar] [CrossRef]
- Mamode, N.; Ahmed, Z.; Jones, G.; Banga, N.; Motallebzadeh, R.; Tolley, H.; Marks, S.; Stojanovic, J.; Khurram, M.A.; Thuraisingham, R.; et al. Mortality Rates in Transplant Recipients and Transplantation Candidates in a High-prevalence COVID-19 Environment. Transplantation 2021, 105, 212–215. [Google Scholar] [CrossRef]
- Timsit, J.F.; Sonneville, R.; Kalil, A.C.; Bassetti, M.; Ferrer, R.; Jaber, S.; Lanternier, F.; Luyt, C.E.; Machado, F.; Mikulska, M.; et al. Diagnostic and therapeutic approach to infectious diseases in solid organ transplant recipients. Intensive Care Med. 2019, 45, 573–591. [Google Scholar] [CrossRef]
- Shrotri, M.; Fragaszy, E.; Geismar, C.; Nguyen, V.; Beale, S.; Braithwaite, I.; Byrne, T.E.; Erica Fong, W.L.; Kovar, J.; Navaratnam, A.M.D.; et al. Spike-antibody responses to ChAdOx1 and BNT162b2 vaccines by demographic and clinical factors (Virus Watch study). medRxiv 2021. [Google Scholar] [CrossRef]
- Natori, Y.; Shiotsuka, M.; Slomovic, J.; Hoschler, K.; Ferreira, V.; Ashton, P.; Rotstein, C.; Lilly, L.; Schiff, J.; Singer, L.; et al. A Double-Blind, Randomized Trial of High-Dose vs. Standard-Dose Influenza Vaccine in Adult Solid-Organ Transplant Recipients. Clin. Infect. Dis. 2018, 66, 1698–1704. [Google Scholar] [CrossRef]
- Corti, D.; Purcell, L.A.; Snell, G.; Veesler, D. Tackling COVID-19 with neutralizing monoclonal antibodies. Cell 2021, 184, 3086–3108. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. Covid-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Chemaitelly, H.; AlMukdad, S.; Joy, J.P.; Ayoub, H.H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Tang, P.; Hasan, M.R.; Coyle, P.; et al. SARS-CoV-2 vaccine effectiveness in immunosuppressed kidney transplant recipients. medRxiv 2021. [Google Scholar] [CrossRef]
- Marra, A.R.; Kobayashi, T.; Suzuki, H.; Alsuhaibani, M.; Tofaneto, B.M.; Bariani, L.M.; Auler, M.A.; Salinas, J.L.; Edmond, M.B.; Doll, M.; et al. Short-term effectiveness of COVID-19 vaccines in immunocompromised patients: A systematic literature review and meta-analysis. J. Infect. 2022, 84, 297–310. [Google Scholar] [CrossRef] [PubMed]
- Shrotri, M.; Navaratnam, A.M.D.; Nguyen, V.; Byrne, T.; Geismar, C.; Fragaszy, E.; Beale, S.; Fong, W.L.E.; Patel, P.; Kovar, J.; et al. Spike-antibody waning after second dose of BNT162b2 or ChAdOx1. Lancet 2021, 398, 385–387. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country | Year | Patient Numbers and Description | Control Numbers and Description | Age of Patients (years) | Sex of Patients (% Females) | Cases, % of Patients on Immunosuppression | Cases, % of Patients on Steroids | Type of Vaccine | Number of Patients Receiving 1 Dose | Number of Patients Receiving 2 Doses | Number of Patients Receiving 3 Doses | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
1 Grupper (Full paper) | Israel | 2021 | 136 (Kidney 100%) | 25 (HCWs) | Cases mean: 58.6 (SD 12.7), Controls mean: 52.7 (SD 11.5) | Cases 18.3%, Controls 68% | ATG last 12 months 7.35%, Rituximab last 12 months 2.9%, CNIs 90.4%, mTORs 7.35%, MMF 76.5% Triple maintenance immunosuppression 78.8% | High-dose steroids last 12 months 23.5%, Low-dose prednisone 89.0% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 161 | NA | |||
| 2 Boyarsky 1 (Letter) | United States | 2021 | 436 (Kidney 50.2%, Liver 17.9%, Heart 15.1%, Lung 11.2% Pancreas 1.1%, Multiorgan 3.2%) | None | Median: 55.9 (IQR 41.3–67.4) | 61% | 100% (Tacrolimus 83%, MMF 66%, Azathioprine 9%, Sirolimus 4%, Everolimus 2%) | 54% | BNT162b2 (Pfizer-BioNTech) 52%, mRNA-1273 (Moderna) 48% | 436 | NA | NA | |||
| 3. Wadei (Letter) | United States | 2021 | 7 (Double lung 14.3%, Kidney 28.6%, Heart and kidney 14.3%, Kidney and pancreas 14.3%) | None | Mean: 59 (Range 42–69) | 0% | 100% (Tacrolimus 85.7%, MMF 100%, Belatacept 14.3%) | 100% | BNT162b2 (Pfizer-BioNTech) 57.1%, mRNA-1273 (Moderna) 42.9% | 2 | 5 | NA | |||
| 4. Rincon-Arevalo (Full paper) | Germany | 2021 | 40 (Kidney 100%) | 35 (Mainly HCWs) | Cases median: 62.4 (IQR 51.3–69.5), Controls median: 51.0 (IQR 34.0–80) | Cases 30%, Controls 42.9% | 100% (MMF 97.5%, Tacrolimus 55%, Cyclosporine 37.5%, Azathioprine 0.9%, mTOR inhibitors 3.7%) | 92.5% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 75 | NA | |||
| 5. Benotmane 1 (Letter) | France | 2021 | 242 (Kidney 100%) | None | 57.7 (49.3–67.6) | 35.50% | 100% (Induction treatment; ATG 59.5%, anti-CD25 37.9%, no induction 2.6%, CNIs; Tacrolimus 55.2%, cyclosporine 34%, no CNI 10.8%, Others; MMF/MPA 79.3%, Azathioprine 2.9%, mTOR inhibitors 14.5%, Belatacept 3.8%) | 58.9% | mRNA-1273 (Moderna) 100% | 242 | NA | NA | |||
| 6. Benotmane 2 (Letter) | France | 2021 | 205 (Kidney 100%) | None | 57.7 (49.4–67.5) | 36.60% | 100% (Induction treatment: ATG 60.5%, anti-CD25 35.9%, no induction 3.6%, CNIs; Tacrolimus 56.4%, Cyclosporine 35.8%, no CNI 7.8%, Others; MMF/MPA 78.9%, Azathioprine 2.9%, mTOR inhibitors 13.2%, Tacrolimus + MMF/MPA 48%, Tacrolimus + MMF/MPA + steroids 31.3%, Belatacept 2.5%) | 59.8% | mRNA-1273 (Moderna) 100% | NA | 205 | NA | |||
| 7. Rabinowich (Full paper) | Israel | 2021 | 80 (Liver 100%) | 25 (HCWs) | Cases mean: 60.1 (SD 12.8) Controls mean: 52.7 (SD 11.5) | Cases 30%, Controls 68% | 97.5% (Tacrolimus 81.3%, Cyclosporine 12.5%, Everolimus 22.5%, Azathioprine 5%, MMF 50%) | High dose steroids last 12 months 20%, prednisone 30% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 105 | NA | |||
| 8. Yi (Letter) | United States | 2021 | 145 (Kidney 100%) | 31 (ESRD patients, 4 on immunosuppression) | NA | NA | 100% | NA | BNT162b2 (Pfizer-BioNTech), mRNA-1273 (Moderna) | 176 | NA | NA | |||
| 9. Peled (Full paper) | Israel | 2021 | 77 (Heart 100%) | 136 (Healthy controls) | Cases median: 62.0 (49.0–68.0) Controls mean: 63 (SD 13) | Cases 36%, Controls 63% | 100% (MPA 53.2%, MMF 22.1%, Everolimus 26.0%) | 75.3% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 213 | NA | |||
| 10. Sattler (Full paper) | Germany | 2021 | 39 (Kidney 100%) | 39 (HCWs) | Cases mean: 57.38 (SD 14.04) Controls mean: 53.03 (SD 17.58) | Cases 28.21%, Controls 48.72% | 100% | 89.7–97.4% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 78 | NA | |||
| 11. Marion (Letter) | France | 2021 | 367 (Kidney 73.8%, Liver 15.8%, Thoracic organs 9.0%, Pancreas 1.4%) (Includes 5 patients with prior COVID-19 exposure) | None | Cases mean: 59 (Standard error 1) | 36.8% | 100% (Tacrolimus 78.2%, Cyclosporine 7.1%, MPA 68.4%, mTOR inhibitors 25.6%, Belatacept 9.3%) | 81.7% | mRNA vaccine 100%: Of original cohort of 950, 942 received BNT162b2 (Pfizer-BioNTech) and 8 received mRNA-1273 (Moderna) | 367 | 367 | NA | |||
| 12. Miele (Letter) | Italy | 2021 | 16 (Kidney 31.3%, Lung 31.3%, Liver 25%, Heart 12.5%) | 23 (HCWs) | Cases mean: 57 (SD 15.9) Controls mean: 44 (SD 7.2) | Cases 18.8%, Controls 56.5% | Tacrolimus 93.7%, Everolimus 6.3%, MMF 62.5% | 56.3% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 39 | NA | |||
| 13. Havlin (Communication) | Czech Republic | 2021 | 48 (Lung 100%) | 10 (Healthy volunteers) | Cases mean: 52.1 (SD 14.3) Controls median: 39.8 (IQR 33.3–47.8) | Cases 39.6%, Controls NA | 100% (Tacrolimus 97.9%, Cyclosporine 2.1%, MMF 91.7%) | 97.9% | BNT162b2 (Pfizer-BioNTech) 100% | 46 | 30 | NA | |||
| 14. Rosen-Zvi (Full paper) | Israel | 2021 | 308 (Kidney 100%) | None | Mean: 57.51 ± 13.84 | 36% | 100% (MPA 73.4%, Tacrolimus 92.5%, Cyclosporine 7.5%, mTOR inhibitor 8.4%, Rituximab 1.9%, ATG 4.5%) | 8.4% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 308 | NA | |||
| 15. Shostak (Letter) | Israel | 2021 | 168 (Lung 100%) | None | Median: 60.5 (IQR 49.3–67.8) | 33% | Includes mTOR inhibitors (patients treated with combination therapy of CNI and Everolimus) 17%, includes antimetabolite (patients treated with MMF/MPA or Azathioprine) 92% | Mean prednisone dose (5.0 mg, IQR 5.0–10.0) | BNT162b2 (Pfizer-BioNTech) 100% | 168 | 168 | NA | |||
| 16. Bertrand (Full paper) | France | 2021 | 45 (Kidney 100%) | None | Mean: 63.5 ± 16.3 | 48.9% | 100% (Tacrolimus 53.3%, Cyclosporine 17.8%, MMF 82.2%, Azathioprine 8.9%, Everolimus 6.7%, Belatacept 22.2%) | 46.7% | BNT162b2 (Pfizer-BioNTech) 100% | 45 | 45 | NA | |||
| 17. Cucchiari (Full paper) | Spain | 2021 | 117 (Kidney 93.2%, Kidney and pancreas 6.8%) | None | Mean: 59.00 ± 52.42 | 32.3% | 100% (Tacrolimus 83.8%, Cyclosporine 4.3%, MMF 61.5%, mTOR inhibitors 32.5%, Azathioprine 3.4%, Belatacept 6.8%, Eculizumab 1.7%) | 79.5% | mRNA-1273 (Moderna) 100% | NA | 148 | NA | |||
| 18. Husain (Letter) | United States | 2021 | 28 (Kidney 100%) (Includes 3 patients with prior COVID-19 exposure) | None | Median: 66 (Range 42–87) | 39% | Tacrolimus 75%, Belatacept 21%, MMF/MPA 61%, Azathioprine 11%, Leflunomide 4%, Sirolimus/everolimus 14% | 32% | BNT162b2 (Pfizer-BioNTech) 57%, mRNA-1273 (Moderna) 43% | NA | 28 | NA | |||
| 19. Korth (Communication) | Germany | 2021 | 23 (Kidney 100%) | 23 (HCWs) | Cases mean: 57.7 ± 13.5 Controls mean: 44.4 ± 9.2 | Cases 52%, Controls 61% | MMF 78.3%, Tacrolimus 60.9%, Cyclosporine 17.4%, Sirolimus 21.7%, Everolimus 4.3%, Belatacept 4.3%, Azathioprine 4.3% | 60.8% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 46 | NA | |||
| 20. Boyarsky 2 (Letter) | United States | 2021 | 658 (Kidney 48.9%, Liver 19.6%, Heart 14.7%, Lung 10.8%, Pancreas 0.8%, Multiorgan 4.0%) | None | Median: ≥60 (Range 18—≥60) | 58.7% | 100% (Antimetabolites 71.9%, Other 28.1%) | NA | BNT162b2 (Pfizer-BioNTech) 52.0%, mRNA-1273 (Moderna) 46.7% | 658 | 658 | NA | |||
| 21. Mazzola (Full paper) | France | 2021 | 143 (Liver 40.6%, Kidney 41.3%, Heart 18.2%) (Includes 8 patients with prior COVID-19 exposure) | 25 (HCWs) | Cases median: 61.0 (IQR 55.0–67.0) Controls median: 55.0 (IQR 38.0–62.0) | Cases 28.7%, Controls 72% | CNIs 82.5%, MMF 72.0%, mTOR inhibitor 18.9%, Tri-therapy 50.4% | 62.2% | BNT162b2 (Pfizer-BioNTech) 100% | 125 | 158 | NA | |||
| 22. Firket (Letter) | Belgium | 2021 | 10 (Kidney 100%) | 10 (Belgian vaccination program) | Cases mean: 49.7 (SD 13.8) Controls mean: 51.5 (SD 10.5) | Cases 50%, Controls 30% | 100% (CNIs 100%, Antimetabolites 100%) | 40% | BNT162b2 (Pfizer-BioNTech) 100% | 20 | 20 | NA | |||
| 23. Danthu (Communication) | France | 2021 | 74 (Kidney 100%) | 7 (HCWs) | Cases mean: 64.8 ± 11.5 Controls mean: 51.6 ± 6.8 | Cases 40.5%, Controls 42.9% | 100% (CNIs 91.8%, Belatacept 2.7%, Everolimus 10.8%, MMF 70.3%, MPA 9.5%, Azathioprine 2.7%) | 45.9% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 81 | NA | |||
| 24. Boyarsky 3 (Letter) | United States | 2021 | 12 (Kidney 58%, Liver 25%, Heart 8%, Lung 8%) | None (compared to mRNA cohort data) | Median: 56 (IQR 42–60) | 58.3% | 100% (Rapamycin 8.3%, Azathioprine 16.7%, Tacrolimus 83.3%, MMF 66.7%, Everolimus 8.3%) | 58.3% | Ad26.COV2.S (Janssen/Johnson & Johnson) 100% | 12 | NA | NA | |||
| 25. Marinaki (Letter) | Greece | 2021 | 34 (Heart 70.6%, Kidney 29.4%) | 116 (HCWs) | Cases median: 60 (IQR 49.1–68.4) Controls: Age and sex matched HCW | Cases 20.6%, Controls Age and sex matched HCW | 100% (CNIs 94%, Antimetabolite therapy 44%, mTOR inhibitor 62%) | 15% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 150 | NA | |||
| 26. Chavarot 1 (Letter) | France | 2021 | 101 (Kidney 100%) | None | Cases median: 64 (53–73) | 32.7% | 100% (Belatacept 100%, MPA 78.2%, mTOR inhibitors 11.9%, Tacrolimus 7.9%, Azathioprine 2.0%) | 96.0% | BNT162b2 (Pfizer-BioNTech) 100% | 101 | 35 | NA | |||
| 27. Ou (Full paper) | United States | 2021 | 609 (Kidney 100%, Pancreas 6%, Liver 4%, Heart 2%, Lung 1%) | None | Median: 58 (IQR 45–68) | 59.2% | 100% (Belatacept 3.9%, MMF 71.9%, Tacrolimus 77.2%, Azathioprine 9,7%, Sirolimus 8.4%) | 68.5% | BNT162b2 (Pfizer-BioNTech) 51.9%, mRNA-1273 (Moderna) 44.8% | 592 | 400 | NA | |||
| 28. Kamar (Correspondence) | France | 2021 | 101 (Kidney 77.2%, Liver 11.9%, Lung 7.9%, Pancreas 3.0%) | None | Mean: 58 ± 2 | 30.3% | CNIs 79%, Anti-metabolites 66%, mTOR inhibitors 30%, Belatacept 12% | 87% | BNT162b2 (Pfizer-BioNTech) 100% | 101 | 99 | 99 (Included in Del Bello) | |||
| 29. Hallett (Full paper) | United States | 2021 | 237 (Heart 57%, Lung 43%) | None | Median: 62 (46–69) (Heart 60 (44–69), Lung 63 (48–70)) | 55% (Heart 51%, Lung 59%) | 100% (Tacrolimus 86%, MMF 62%, Sirolimus 14%, Cyclosporine 8%, Azathioprine8%, Everolimus7%, Belatacept 1%) | 57% | BNT162b2 (Pfizer-BioNTech) 53%, mRNA-1273 (Moderna) 47% | 237 | 237 | NA | |||
| 30. Stumpf (Full paper) | Germany | 2021 | 368 (Kidney 100%) | 144 (HCWs) | Cases mean: 57.3 ± 13.7 Controls mean: 48 ± 11.9 | 34.5% | 99.7% (CNIs 87.5%, MMF 76.1%, mTOR Inhibitor 16%, Belatacept 4.6%) | 48.4% | BNT162b2 (Pfizer-BioNTech) 28%, mRNA-1273 (Moderna) 72% | 144 | 333 | NA | |||
| 31. Zadok (Short report) | Israel | 2021 | 42 (Heart 100%) | None | Median: 61 (IQR 44–69) | 17% | 99.7% (CNIs 81%, MMF 55%%, mTOR Inhibitor 57%,) | 69% | BNT162b2 (Pfizer-BioNTech) 100% | 42 | NA | NA | |||
| 32. Schramm (Full paper) | Germany | 2021 | 50 (Heart 84%, Lung 14%, Heart/lung 2%) | 50 (HCWs) | Mean: 55 ± 10 | 36% | 100% (Tacrolimus/MMF 82%, Cyclosporine/MMF 10%, Tacrolimus/mTOR-Inhibitor 8%) | NA | BNT162b2 (Pfizer-BioNTech) 100% | ||||||
| 33. Werbel (Letter) | United States | 2021 | 30 (Kidney 73.3%, Heart 6,7%, Lung 3.3%, Liver 10%, Pancreas 3.3%, Kidney and pancreas 3.3%) | None | Median: 57 (IQR 44–62) | 56.7% | Tacrolimus or Cyclosporine + MMF 83.3%, Sirolimus 3.3%, Belatacept 3.3% | 80% | Initial doses: BNT162b2 (Pfizer-BioNTech) 56.7%, mRNA-1273 (Moderna) 43.3% Third dose: BNT162b2 (Pfizer-BioNTech) 16.7%, mRNA-1273 (Moderna) 33.3%, AD26.COV2.S (Janssen/Johnson & Johnson) 50% Combinations: Pfizer-BioNTech + Janssen/Johnson & Johnson 23.3%, Pfizer-BioNTech + Moderna 23.3%, Pfizer-BioNTech + Pfizer-BioNTech 10%, Moderna + Janssen/Johnson & Johnson 26.7%, Moderna + Moderna 10%, Moderna + Pfizer-BioNTech 6.7% | NA | 30 | 30 | |||
| 34. Hall (Correspondence) | Canada | 2021 | 120 (Lung 24.2%, Heart 15%, Kidney 24.2%, Liver 16.7%, Pancreas/kidney-pancreas 20%) (60 experimental, 60 placebo) | None (Randomized controlled trial contained all solid organ transplant patients) | Third dose median: 66.9 (IQR 64.0–71.8), Placebo median: 65.9 (IQR 62.9–70.3) | Third dose: 38.3%, Placebo: 30% | 100% (Tacrolimus 77.5%, Cyclosporine 20.8%, Sirolimus 9.2%, MMF 75%, Azathioprine 10%) | Third dose 83.3%, Placebo 70% | mRNA-1273 (Moderna) 100% | NA | 120 | 60 | |||
| 35. Karaba (Preprint) | United States | 2021 | 31 (Kidney 61.3%, Liver 22.6%, Heart 9.7%, Pancreas 3.2%, Lung 3.2%) | None (15 Healthy controls receiving 2 mRNA vaccine doses) | Median: 60 (IQR 49–67) | Cases 54.8%, Controls 33.3% | (CNI 80.6%, mTORi 9.7%, Anti-metabolites 64.5%) | 51.6% | Transplant recipients: First two doses: mRNA vaccine 100%, Third dose: mRNA vaccine (19, 61.3%), Ad26.COV2.S (Janssen/Johnson & Johnson) (12, 38.7%) Healthy controls: 2 doses of an mRNA vaccine (15, 100%) | NA | 46 | 46 | |||
| 36. Peled 2 (Full paper) | Israel | 2021 | 96 (Heart 100%) | None | Median: 61.0 (IQR 49.8–68.0) | 29.2% | 100% (Tacrolimus 82.3%, Mycophenolate sodium 54.2%, MMF 24.0%, Cyclosporine 11.5%, Everolimus 21.9%) | 80.2% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 96 | 96 | |||
| 37. Benotmane 3 (Letter) | France | 2021 | 159 (Kidney 100%) | None | Median: 57.6 (IQR 49.6–66.1) | 38.4% | 100% (Tacrolimus + MMF/MPA + steroids 52.8%, All other regimens 47.2%) | Tacrolimus + MMF/MPA + steroids (84, 52.8%) All other regimens (75, 47.2%) | mRNA-1273 (Moderna) 100% | NA | 159 | 159 | |||
| 38. Masset (Letter) | France | 2021 | 136 (Kidney 91.2%, kidney-pancreas/pancreas 8.8%) | None | Mean: 63.7 (SD 11.7) | 36.8% | (CNI 84.6%, mTORi 14.7%, Antimetabolites 74.3%, NA 1.47%) | 31.6% (NA 1.47%) | BNT162b2 (Pfizer-BioNTech) 100% | NA | 456 | 136 | |||
| 39. Del Bello (Letter) | France | 2021 | 396 (Kidney 69.9%, Liver 17.4%, Heart 8.33%, Lung 0.3%, Pancreas 1.5%, Multiple organs 2.5%) | None | Mean: 59 (SD 15) | 34.8% | 100% (CNI 86.1%, MPA 72.0%, mTORi 26.8%, Belatacept 8.8%) | 82.1% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 396 | 396 | |||
| 40. Charmetant (Preprint) | France | 2021 | 66 (Kidney 100%) | None | Mean: 56.3 (SD 12.3) | 56.1% | 100% (CNI 92.4%, MMF/MPA 81.8%, mTORi 7.6%, Belatacept 1.5%) | 86.4% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 66 | 66 | |||
| 41. Chavarot 2 (Communication) | France | 2021 | 62 (Kidney 100%) | None | Median 63.5 years (IQR 51–72) | 41.9% | 100% (Belatacept 100%, Everolimus 12.9%, MPA 71.0%, Azathioprine 4.8%, CNI 3.2%) | 100% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 62 | 62 | |||
| 42. Westhoff (Letter) | Germany | 2021 | 10 (Kidney 100%) | None | Mean: 59.5 (Range 41–76) | 20% | 100% (CNI 80%, mTORi 10%, Belatacept 10%, MPA 90%) | 100% | First two doses: BNT162b2 (Pfizer-BioNTech) 100% Third dose: mRNA-1273 (Moderna) 100% | 10 | 10 | 10 | |||
| 43. Massa (Preprint) | France | 2021 | 61 (Kidney 100%) | None | Median 58 years (IQR 47.1–66.1) | 27.9% | 100% (Antimetabolites 62.3%, CNI 93.4%, mTORi 9.8%, Belatacept 1.6%) | 88.5% | BNT162b2 (Pfizer-BioNTech) 100% | NA | 61 | 61 | |||
| 44. Schrezenmeier (Preprint) | Germany | 2021 | 25 (Kidney 100%) | None | Mean: 59.7 (SD 13.8) | 44.0% | 100% (Tacrolimus 56%, Cyclosporine 32%, MMF 96%, mTORi 16%) | 96% | First two doses: BNT162b2 (Pfizer-BioNTech) 100% Third dose: BNT162b2 (Pfizer-BioNTech) 56%, AZD1222 (Oxford-AstraZenaca) 44% | 25 | 25 | 25 | |||
| Author | Used to Check Antibody Response | Timing of Test | After One Dose | After Two Doses | After Three Doses | ||||||||||
| Cases Responders | Controls Responders | Cases Ab Titers | Controls Ab Titers | Cases Responders | Controls Responders | Cases Ab Titers | Controls Ab Titers | Cases Responders | Controls Responders | Cases Ab Titers | Controls Ab Titers | ||||
| 1. Grupper | DiaSorin LIAISON SARS-CoV-2 S1/S2 IgG chemiluminescent assay | 10–20 days after the second dose | - | - | - | - | 51/136 | 25/25 | Median: 71.8 AU/mL (IQR 37.6–111.7 AU/mL) | Median: 189.0 AU/mL (IQR 141.10–248 AU/mL) | - | - | - | - | |
| 2. Boyarsky 1 | EUROIMMUN anti-S1 IgG assay or Roche Elecsys anti-RBD pan-Ig assay | 14–21 days after the first dose | 76/436 | - | NA | - | - | - | - | - | - | - | - | - | |
| 3. Wadei | Antispike antibody, manufacturer NA | Median 28 days (Range 6–44 days) after the first dose | 0/2 | - | NA | - | 1/5 | - | 1.4 U/mL | - | - | - | - | - | |
| 4. Rincon-Arevalo | EUROIMMUN anti-SARS-CoV-2 ELISA, GenScript Surrogate SARS-CoV-2 virus neutralization ELISA | 7 ± 2 days after the second dose | - | 4/40 (IgG 1/40, IgA 4/40, Neutralizing antibodies 0/40) | 35/35 | IgG median: 0.09 (IQR 0.07–0.15) IgA median: 0.20 (IQR 0.15–0.40) NC median: 0.07 (IQR 0.05–0.13) | IgG median: 58.59 (IQR 31.90–71.96) IgA median: 41.10 (IQR 27.03–58.37) NC median: 0.08 (IQR 0.06–0.11) | - | - | - | - | ||||
| 5. Benotmane 1 | ARCHITECT IgG II Quant test | 28 days after the first dose | 26/242 | - | Median: 224 AU/mL (IQR 76–496 AU/mL) | - | - | - | - | - | - | - | - | - | |
| 6. Benotmane 2 | Abbott ARCHITECT IgG II Quant test | 1 month after the second dose | - | - | - | - | 98/205 | - | Median: 803.2 AU/mL (IQR 142.6–4609.6 AU/mL) | - | - | - | - | - | |
| 7. Rabinowich | DiaSorin LIAISON SARS-CoV-2 S1/S2 IgG chemiluminescent assay | Cases: Mean 14.8 (±3.2) days after the second dose, Controls: Mean 15.8 (±2.9) days after the second dose | Median: 1:150 COVID-19 IgG titer (Range 1:50 to >1:1350) | 38/80 | 25/25 | Mean: 95.41 (±92.4) AU/mL | Mean: 200.5 (±65.1) AU/mL | - | - | - | - | ||||
| 8. Yi | Anti-SARS-CoV-2 IgG and total antibody, anti-SARS-CoV-2 Nucleocapsid IgG, and anti-Spike IgG titer | At the time of second dose | 9/145 | 27/31 | Median: 1:150 COVID-19 IgG titer (Range 1:50 to <1:450) | Median: 1:150 COVID-19 IgG titer (Range 1:50 to >1:1350) | - | - | - | - | - | - | - | - | |
| 9. Peled 1 | An "in-house" ELISA that detects IgG antibodies against SARS-CoV-2 RBD. A SARS-CoV-2 pseudo-virus (psSARS-2) neutralization assay was performed to detect SARS-CoV-2 neutralizing antibodies using a propagation-competent VSV-spike | Transplant: 21 ± 10 days after the second dose Control: 13.3 ± 1.4 days after the second dose | - | - | - | - | 14/77 | 134/136 | NA | NA | - | - | - | - | |
| 10. Sattler | Euroimmun ELISA-based analysis of SARS-CoV2 spike S1 domain-specific IgG and IgA | 8 ± 1 days after the second dose | - | - | - | - | 4/39 (IgG 1/39, IgA 4/39, Neutralizing antibodies 0/39) | 39/39 | NA | NA | - | - | - | - | |
| 11. Marion | Beijing Wantai Biological Pharmacy Enterprise SARS-CoV-2 total antibodies ELISA or another validated anti–SARS-CoV-2 spike protein assay | 28 days after the first or second dose | 23/367 | - | NA | - | 124/367 | - | NA | - | - | - | - | - | |
| 12. Miele | DiaSorin LIAISON SARS-CoV-2 S1/S2-IgG chemiluminescent assay | Cases: Median 20 days (Range 15–76) after the second dose, Controls: Median 15 days (Range 15–20) after the second dose | - | - | - | - | 6/16 | 23/23 | Median: 3.8 AU/mL Mean: 87.32 AU/mL | Median: 212 AU/mL Mean: 233 AU/mL | - | - | - | - | |
| 13. Havlin | Euroimmun anti-SARS-CoV-2 Spike S1 IgG ELISA, confirmed independently by TestLine Microblot-Array COVID-19 IgG and DiaSorin Liaison SARS-CoV-2 Trimeric S IgG | Cases: At baseline, before the second dose, 7 days after the second dose, 4–6 weeks after the second dose, Controls: 31 days (IQR 19–41 days) after the second dose | 0/46 | - | NA | - | 7 days after second vaccination: 0/30 (4–6 weeks after second vaccination: 0/21) | 10/10 | NA | NA | - | - | - | - | |
| 14. Rosen-Zvi | Abbott SARS-CoV-2 IgG II Quant assay | Median 28 days (IQR 22–34 days) after the second dose | - | - | - | - | 112/308 | - | Median: 15.5 AU/mL (IQR 3.5–163.6 AU/mL) | - | - | - | - | - | |
| 15. Shostak | Abbott SARS-CoV-2 IgG II Quant assay | Median 16 days (IQR 15–18) after the second dose | 6/168 | - | Geometric mean S-IgG titer: 3.12 (SD 4.05) | - | 31/168 | - | Geometric mean S-IgG titer: 9.29 (SD 9.22) | - | - | - | - | - | |
| 16. Bertrand | Abbott ARCHITECT IgG II Quant test | Three weeks after the first dose and one month after the second dose | 1/45 | - | 311 AU/mL | - | 8/45 | - | Responder median: 671 AU/mL (IQR 172–1523 AU/mL) | - | - | - | - | - | |
| 17. Cucchiari | A serological assay based on the Luminex technique measuring antibodies against the Receptor-Binding Domain (RBD) of the spike glycoprotein of SARS-CoV-2 | 2 weeks after the second dose | - | - | - | - | 35/117 (IgG/IgM 5/117, IgG 27/117, IgM 3/117) | - | NA | - | - | - | - | - | |
| 18. Husain | DiaSorin LIAISON anti-S IgG immunoassay or Roche Diagnostics Elecsys anti-S IgG immunoassay | Median 29 days (Range 12–59) after the second dose | - | - | - | - | 7/28 | - | NA | - | - | - | - | - | |
| 19. Korth | DiaSorin LIAISON® SARS-CoV-2 TrimericS IgG assay | Cases: Mean 15.8 ± 3.0 days after the second dose Controls: Mean 13.7 ± 1.8 days after the second dose | - | - | - | - | 5/23 | 23/23 | Mean: 50.9 ± 138.7 AU/mL | Mean: 727.7 ± 151.3 AU/mL | - | - | - | - | |
| 20. Boyarsky 2 | EUROIMMUN anti-S1 IgG assay 28.6%, Roche Elecsys anti-RBD pan-Ig assay 71.4% | Median 21 days (IQR 18–25) after the first dose, Median 29 days (IQR 28–31) after the second dose | 98/658 | - | NA | - | 357/658 | - | Roche median: 2.14 U/mL (IQR <0.4–245.8), EUROIMMUN median: 1.23 AU (IQR 0.13–6.38) | - | - | - | - | - | |
| 21. Mazzola | Abbott Diagnostics Alinity I chemiluminescent microparticle immunoassays | 28 days after the first and second dose | 9/125 | - | Responder median: 153 AU/mL (IQR 129–860 AU/mL) | - | 38/133 | 25/25 | Responder median: 759 AU/mL (IQR 257–3269 AU/mL) | NA | - | - | - | - | |
| 22. Firket | DiaSorin LIAISON® chemiluminescence immunoassay | At time of second dose, ~15 days after the second dose, ~50 days after the second dose for transplant patients | 0/10 | 9/10 | Median: 0 AU/mL (Range 0–0 AU/mL) | Median: 35.5 AU/mL (Range 0–118 AU/mL) | 15 days after second dose 1/10 (50 days after second dose 3/10) | 15 days after second dose: 10/10 | 15 days after second dose median: 0 AU/mL (0–60 AU/mL) 50 days after second dose median: 0 AU/mL (0–46 AU/mL) | 15 days after second dose median: 263 AU/mL (Range 153–2090 AU/mL) | - | - | - | - | |
| 23. Danthu | DiaSorin LIAISON SARS-CoV-2 TrimericS IgG | 14, 28, 36, and 58 days after the first dose | - | - | - | - | 3/74 | 7/7 | NA (low number of responders) | Day 14: 59 AU/mL (IQR 26.5–216.5 AU/mL) Day 36: 1082 AU/mL (IQR 735.0–1662 AU/mL) Day 58: 925 AU/mL (IQR 637–3624.5 AU/mL) | - | - | - | - | |
| 24. Boyarsky 3 | Roche Elecsys anti-SARS-CoV-2 S enzyme immunoassay | Median 33 days (IQR 31–44 days) after the first dose | 2/12 | - | Median: 2.39 U/mL (Range 1.33–3.45 U/mL) | - | - | - | - | - | - | - | - | - | |
| 25. Marinaki | Abbott SARS-CoV-2 IgG II Quant anti-SARS-CoV-2-RBD IgG assay | Median 10 days (IQR 9–10 days) after thesecond dose | - | - | - | - | 20/34 | 116/116 | Median: 1370 AU/mL Geometric mean: 948 AU/mL | Median: 11,710 AU/mL Geometric mean: 11,300 AU/ML | - | - | - | - | |
| 26. Chavarot | Abbott SARS-CoV-2 IgG II Quant antibody test or Beijing Wantai Biological Pharmacy Enterprise SARS-CoV-2 total antibodies ELISA | 28 and 60 days after first dose | 2/101 | - | NA | - | 2/35 | - | NA | - | - | - | - | - | |
| 27. Ou | EUROIMMUN anti-S1 IgG assay or Roche Elecsys anti-RBD pan-Ig assay | After 1 dose: Non-belatacept: Median 21 days (IQR 19–26) Belatacept: Median 22 days (IQR 19 -26) After 2 doses: Non-belatacept: Median 29 days (IQR 28–32) Belatacept: Median 29 days (IQR 28–31) | 77/592 (Belatacept 0/24, Non-belatacept 77/568) | - | EUROIMMUN median IgG titer: 2.33 AU (IQR 1.68 – 4.77) Roche median IgG titer: 4.24 U/mL (IQR 1.81 – 15.05) | - | 191/400 (Belatacept 1/19, Non-belatacept 190/381) | - | Non-belatacept: EUROIMMUN median IgG titer: 6.23 AU (IQR 3.12 – 8.74 AU) Roche median IgG titer: 78.10 U/mL (IQR 7.42 – 250 U/mL) Belataceot: 48.07 U/mL | - | - | - | - | - | |
| 28. Kamar | Beijing Wantai Biological Pharmacy Enterprise SARS-CoV-2 total antibodies ELISA | 4 weeks after the third dose | 4/101 | - | NA | - | 40/99 | - | NA | - | 67/99 (Included in Del Bello) | ||||
| 29. Hallett | Roche Elecsys for antibodies against the receptor-binding domain (RBD) or EUROIMMUN for antibodies to the S1 domain | Median of 21 days (IQR 19–26 days) after the first dose, median of 29 days (IQR 28–32 days) after the second dose | 28/237 (Heart 19/134, Lung 9/103) | - | - | - | 120/237 (Heart 83/134, Lung 37/103) | - | Anti-spike RBD assay: 250 U/mL (IQR, 174–250 U/mL) for first dose responders, 23.8 U/mL (IQR, 3.9–244.2 U/mL) for second dose responders, and 0 U/mL (IQR, 0–0 U/mL) for non-responders | - | - | - | - | - | |
| 30. Stumpf | SARS-CoV-2 specific IgG- or IgA-antibody reactions (Euroimmun) against the Spike protein subunit S1 | 3–4 weeks after the first dose, 4–5 weeks after the second dose | 11/144 | 53/55 | NA | NA | 140/333 | 132/134 | NA | NA | - | - | - | - | |
| 31. Zadok | Anti-spike IgG (S-IgG) antibodies | 21–26 days and 35–40 days after the first dose | 6/39 | - | NA | - | 18/37 | - | NA | - | - | - | - | - | |
| 32. Schramm | SARS-CoV-2 IgG II Quant assay (Abbott) which was used for the quantitative measurement of IgG antibodies against the spike receptor-binding domain (RBD) | 21 days after the first and the second dose | 2/50 | 49/50 | NA | Median 82 (41;149) BAU/ml | 5/50 | 50/50 | NA | median 1417 (732; 2589) BAU/ml | - | - | - | - | |
| 33. Werbel | EUROIMMUN anti-S1 IgG assay or Roche Elecsys anti-RBD pan-Ig assay | Median 9 days (IQR 2–33) before the third dose, Median 14 days (IQR 14–17 days) after the third dose | - | - | - | - | 6/30 | - | EUROIMMUN median 0.15 AU, Roche median 0.4 U/mL | - | 14/30 (BNT162b2 2/5, mRNA-1273 7/10, Ad26.COV2.S: 5/15) | - | EUROIMMUN median 0.37 AU, Roche median NA | - | |
| 34. Hall | Roche Elecsys anti-SARS-CoV-2 S enzyme immunoassay | 1 month after third vaccination | - | - | - | - | 12/120 (Third dose: 7/60 Placebo third dose: 5/60) | - | Third dose: Median 0.37 U/mL (IQR 0.2 – 27.64) Placebo: Median 0.44 U/mL (IQR 0.2 – 18.19) | - | Third dose: 33/60 (Placebo third dose: 10/57) | - | Third dose: Mean: 3145 U/mL (SD 7517), Median: 313.8 U/ML (IQR 0.2–2191)Placebo: Mean: 86 U/mL (SD 231), Median: 1.19 U/mL (IQR 0.2–63.4) | - | |
| 35. Karaba | Meso Scale Diagnostics (MSD) V-PLEX COVID-19 155 Respiratory Panel 3 multiplex chemiluminescent kit | 14 days after third vaccination | - | - | - | - | 12/31 (Anti-RBD IgG: 12/31, Anti-S IgG: 8/31, Anti-N IgG: 0/31) | 15/15 | NA | NA | 24/31 (Anti-RBD IgG: 24/31, Anti-S IgG: 22/31 (mRNA: 16/19 Ad26.COV2.S: 6/12)) | - | NA | - | |
| 36. Peled 2 | An "in-house" enzyme-linked immunosorbent assay that detects IgG antibodies against SARS-CoV-2 RBD. A SARS-CoV-2 pseudo-virus (psSARS-2) neutralization assay was performed to detect SARS-CoV-2 neutralizing antibodies using a propagation-competent VSV-spike | Mean 17.5 days (SD 3.9) after third vaccination | - | - | - | - | 26/96 (May overlap with previous Peled 1 study) | - | IgG GMT: 0.49 (95% CI 0.39–0.62) Neutralizing antibody GMT: 3.05 (95% CI, 2.05–4.55) | - | 64/96 | - | IgG GMT: 1.58 (95% CI 1.24–2.00)Neutralizing antibody GMT: 27.25 (95% CI, 15.70–47.30) | - | |
| 37. Benotmane | Abbott ARCHITECT IgG II Quant test | Median 28 days (IQR 27–33) after third vaccination | - | - | - | - | 0/159 (95 pts had no antibody response, 64 pts had an antibody response below the seropositivity threshold of 50 AU/mL) | - | <50 AU/mL | - | 78/159 | - | Responder median: 586 AU/mL (IQR 197.2–1920.1)Non-responder median: <50 AU/mL | - | |
| 38. Masset | Abbott Architect chemiluminescent microparticle immunoassay, Siemens Atellica chemiluminescence immunoassay, Roche Elecsys electrochemiluminescence immunoassay | Median 30 days (IQR 28–32) | - | - | - | - | 227/456 (Assessed after second and third dose: 34/85) | - | NA | - | 94/136 | - | NA | - | |
| 39. Del Bello | Beijing Wantai enzyme-linked immunosorbent assay (228, 57.6%) or other anti-SARS-CoV-2 spike assay (168, 42.4%) | 4 weeks after third vaccination | - | - | - | - | 164/396 | - | NA | - | 269/396 | - | NA | - | |
| 40. Charmetant | Snibe Diagnostic Maglumi SARS-CoV-2 S-RBD IgG test on a Maglumi 2000 analyser | 14 days after third vaccination | - | - | - | - | 27/93 | - | <142 BAU/mL | - | 28/66 (All 66 had no response after two doses) | - | NA | - | |
| 41. Chavarot 2 | Abbott SARS-CoV-2 IgG II Quant antibody test | Median 28 (IQR 28–33) days after third vaccination | - | - | - | - | 0/62 | - | <50 AU/mL | - | 4/62 | - | Median 209 AU/mL (IQR 20–409 AU/ml) | - | |
| 42. Westhoff | Roche Elecsys anti-SARS-CoV-2 S enzyme immunoassay | 14 days after third vaccination | 0/10 | - | <0.8 U/mL | - | 0/10 | - | <0.8 U/mL | - | 6/10 | - | Responder median 542 U/mL (IQR 478–923) | - | |
| 43. Massa | Abbott ELISA on the Abbott Architect I1000 analyser | 28 days after third vaccination | - | - | - | - | 27/61 | - | GMT IgG: 528.3 AU/mL (95% CI 300.0–930.1) | - | 38/61 | - | GMT IgG: 2395 AU/mL (95% CI 1214–4724) | - | |
| 44. Schrezenmeier | Euroimmun ELISA-based analysis of SARS-CoV2 spike S1 domain-specific IgG and IgA | 7 ± 2 days after the second and third vaccination, and 19–27 days after each vaccination | 0/25 | - | NA | - | 0/25 | - | NA | - | 9/25 (BNT162b2: 3/14, AZD1222: 6/11) | - | NA | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakuraba, A.; Luna, A.; Micic, D. A Systematic Review and Meta-Analysis of Serologic Response following Coronavirus Disease 2019 (COVID-19) Vaccination in Solid Organ Transplant Recipients. Viruses 2022, 14, 1822. https://doi.org/10.3390/v14081822
Sakuraba A, Luna A, Micic D. A Systematic Review and Meta-Analysis of Serologic Response following Coronavirus Disease 2019 (COVID-19) Vaccination in Solid Organ Transplant Recipients. Viruses. 2022; 14(8):1822. https://doi.org/10.3390/v14081822
Chicago/Turabian StyleSakuraba, Atsushi, Alexander Luna, and Dejan Micic. 2022. "A Systematic Review and Meta-Analysis of Serologic Response following Coronavirus Disease 2019 (COVID-19) Vaccination in Solid Organ Transplant Recipients" Viruses 14, no. 8: 1822. https://doi.org/10.3390/v14081822