
Characteristics of Critically Ill Patients with COVID-19 Compared to Patients with Influenza—A Single Center Experience

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Hospital Setting
2.2. Patient Population
2.2.1. COVID-19 Cohort
2.2.2. Influenza Cohort
2.3. Treatment Protocols
2.3.1. General Treatment
2.3.2. Specific Treatment
2.4. Statistic
3. Results
3.1. Baseline Characteristics of Patient Groups
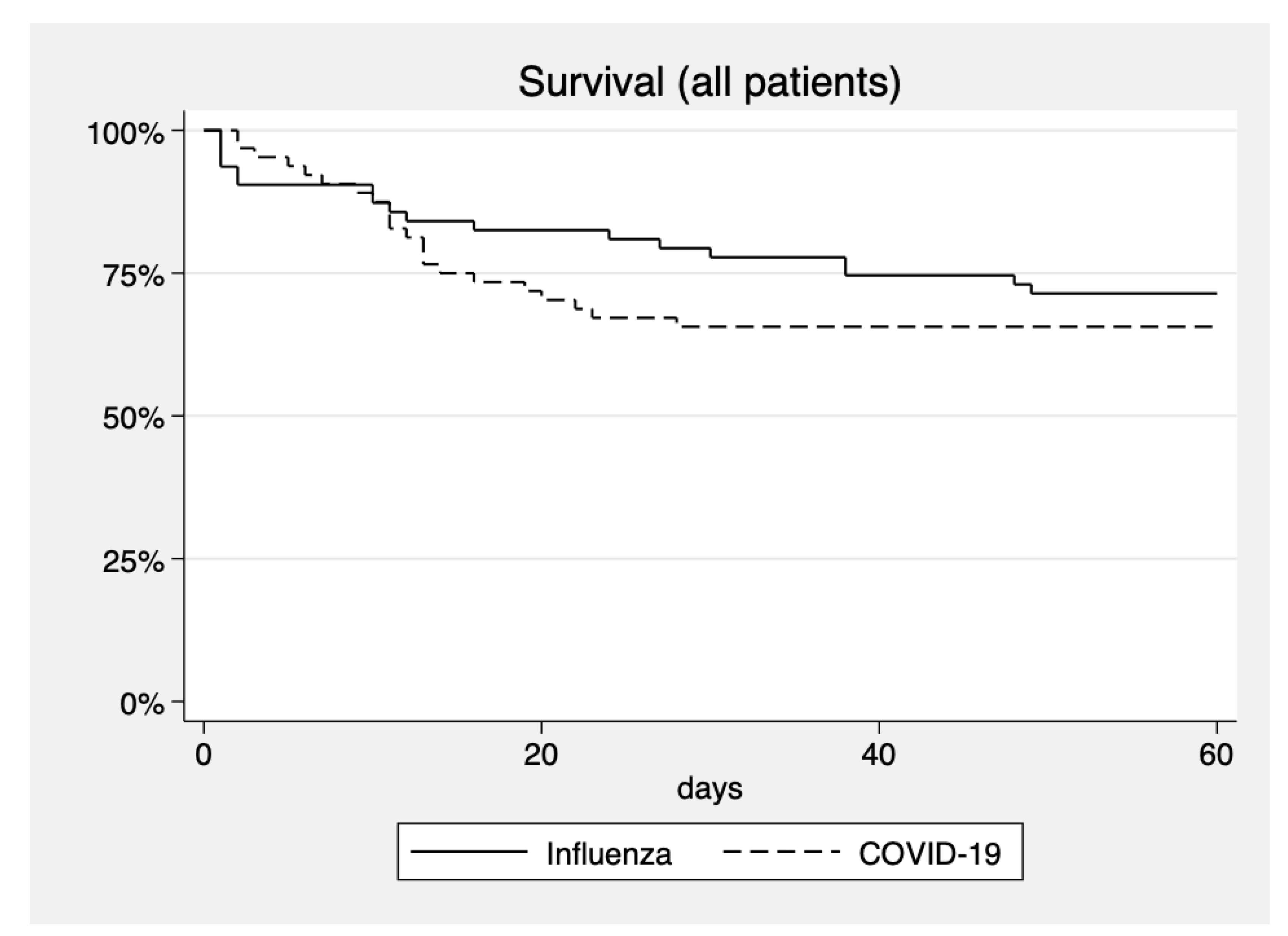
3.2. Clinical Endpoints
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses; Gorbalenya, A.E.; Baker, S.C. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar]
- Wu, Y.-C.; Chen, C.-S.; Chan, Y.-J. The outbreak of COVID-19: An overview. J. Chin. Med. Assoc. 2020, 83, 217–220. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Abate, S.M.; Ali, S.A.; Mantfardo, B.; Basu, B. Rate of Intensive Care Unit admission and outcomes among patients with coronavirus: A systematic review and Meta-analysis. PLoS ONE 2020, 15, e0235653. [Google Scholar] [CrossRef]
- Miller, I.F.; Becker, A.D.; Grenfell, B.T.; Metcalf, C.J.E. Disease and healthcare burden of COVID-19 in the United States. Nat. Med. 2020, 26, 1212–1217. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Altersberger, M.; Binder, C.; Hengstenberg, C.; Binder, T. The COVID-19 burden for health care professionals: Results of a global survey. Eur. J. Intern. Med. 2021, 83, 96–98. [Google Scholar] [CrossRef]
- Sasangohar, F.; Jones, S.L.; Masud, F.N.; Vahidy, F.S.; Kash, B.A. Provider Burnout and Fatigue during the COVID-19 Pandemic: Lessons Learned From a High-Volume Intensive Care Unit. Anesth. Analg. 2020, 131, 106–111. [Google Scholar] [CrossRef]
- Zeng, Y.; Cai, Z.; Xianyu, Y.; Yang, B.X.; Song, T.; Yan, Q. Prognosis when using extracorporeal membrane oxygenation (ECMO) for critically ill COVID-19 patients in China: A retrospective case series. Crit. Care 2020, 24, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, J.P.; Stammers, A.H.; Louis, J.S.; Hayanga, J.W.A.; Firstenberg, M.S.; Mongero, L.B.; Tesdahl, E.A.; Rajagopal, K.; Cheema, F.H.; Coley, T.; et al. Extracorporeal Membrane Oxygenation in the Treatment of Severe Pulmonary and Cardiac Compromise in Coronavirus Disease 2019: Experience with 32 Patients. ASAIO J. 2020, 66, 722–730. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; Yu, T.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, Chi-na: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Krammer, F.; Smith, G.J.D.; Fouchier, R.A.M.; Peiris, M.; Kedzierska, K.; Doherty, P.C.; Palese, P.; Shaw, M.L.; Treanor, J.; Webster, R.G.; et al. Influenza. Nat. Rev. Dis. Primers 2018, 4, 3. [Google Scholar] [CrossRef]
- Dubey, A.D. The Resurgence of Cyber Racism During the COVID-19 Pandemic and its Aftereffects: Analysis of Sentiments and Emotions in Tweets. JMIR Public Health Surveill. 2020, 6, e19833. [Google Scholar] [CrossRef]
- Lwin, M.O.; Lu, J.; Sheldenkar, A.; Schulz, P.J.; Shin, W.; Gupta, R.; Yang, Y. Global Sentiments Surrounding the COVID-19 Pandemic on Twitter: Analysis of Twitter Trends. JMIR Public Health Surveill. 2020, 6, e19447. [Google Scholar] [CrossRef] [PubMed]
- Petersen, E.; Koopmans, M.; Go, U.; Hamer, D.H.; Petrosillo, N.; Castelli, F.; Storgaard, M.; Al Khalili, S.; Simonsen, L. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect. Dis. 2020, 20, e238–e244. [Google Scholar] [CrossRef]
- Wormser, G.P. COVID-19 versus seasonal influenza 2019–2020: USA. Wien. Klin. Wochenschr. 2020, 132, 387–389. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Delaney, M.; Shah, R.K.; Campos, J.M.; Wessel, D.L.; DeBiasi, R.L. Comparison of Clinical Features of COVID-19 vs. Seasonal Influenza A and B in US Children. JAMA Netw. Open 2020, 3, e2020495. [Google Scholar] [CrossRef]
- Brehm, T.T.; van der Meirschen, M.; Hennigs, A.; Roedl, K.; Jarczak, D.; Wichmann, D.; Frings, D.; Nierhaus, A.; Oqueka, T.; Fiedler, W.; et al. Comparison of clinical characteristics and disease outcome of COVID-19 and seasonal influenza. Sci. Rep. 2021, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, J.; Lemeshow, S.; Saulnier, F. A New Simplified Acute Physiology Score (SAPS II) Based on a European/North American Multicenter Study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef] [PubMed]
- Guérin, C.; Reignier, J.; Richard, J.C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- Lescure, F.-X.; Honda, H.; Fowler, R.; Lazar, J.S.; Shi, G.; Wung, P.; Patel, N.; Hagino, O.; Bazzalo, I.J.; Casas, M.M.; et al. Sarilumab in patients admitted to hospital with severe or critical COVID-19: A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir. Med. 2021, 9, 522–532. [Google Scholar] [CrossRef]
- Austin, P.C. Using the standardized difference to compare the prevalence of a binary variable between two groups in obser-vational research. Commun. Stat. Simul. Comput. 2009, 38, 1228–1234. [Google Scholar] [CrossRef]
- Zeiher, J.; Kuntz, B.; Lange, C. Smoking among adults in Germany. J. Health Monit. 2017, 2, 57–63. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal stud-ies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Verweij, P.E.; Rijnders, B.J.A.; Brüggemann, R.J.M.; Azoulay, E.; Bassetti, M.; Blot, S.; Calandra, T.; Clancy, C.J.; Cornely, O.A.; Chiller, T.; et al. Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: An expert opinion. Intensive Care Med. 2020, 46, 1524–1535. [Google Scholar] [CrossRef] [PubMed]
- Cullen, D.J.; Civetta, J.M.; Briggs, B.; Ferrara, L.C. Therapeutic intervention scoring system: A method for quantitative comparison of patient care. Crit. Care Med. 1974, 2, 57–60. [Google Scholar] [CrossRef]
- Kaye, A.D.; Okeagu, C.N.; Pham, A.D.; Silva, R.A.; Hurley, J.J.; Arron, B.L.; Sarfraz, N.; Lee, H.N.; Ghali, G.E.; Liu, H.; et al. Economic impact of COVID-19 pandemic on healthcare facilities and systems: In-ternational perspectives [published online ahead of print, 2020 November 17]. Best Pract. Res. Clin. Anaesthesiol. 2020. [Google Scholar] [CrossRef]
- Trick, W.E.; Badri, S.; Doshi, K.; Zhang, H.; Rezai, K.; Hoffman, M.J.; Weinstein, R.A. Epidemiology of COVID-19 vs. influenza: Differential failure of COVID-19 mitigation among Hispanics, Cook County Health, Illinois. PLoS ONE 2021, 16, e0240202. [Google Scholar] [CrossRef]
- Teunis, P.F.; Brienen, N.; Kretzschmar, M.E. High infectivity and pathogenicity of influenza a virus via aerosol and droplet transmission. Epidemics 2010, 2, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Pettrone, K.; Burnett, E.; Link-Gelles, R.; Haight, S.C.; Schrodt, C.; England, L.; Gomes, D.J.; Shamout, M.; O’Laughlin, K.; Kimball, A.; et al. Characteristics and Risk Factors of Hospitalized and Nonhospitalized COVID-19 Patients, Atlanta, Georgia, USA, March–April 2020. Emerg. Infect. Dis. 2021, 27, 1164–1168. [Google Scholar] [CrossRef]
- Jiang, M.; Li, C.; Zheng, L.; Lv, W.; He, Z.; Cui, X.; Dietrich, C.F. A biomarker-based age, biomarkers, clinical history, sex (ABCS)-mortality risk score for patients with coronavirus disease 2019. Ann. Transl. Med. 2021, 9, 230. [Google Scholar] [CrossRef] [PubMed]
- González-Rubio, J.; Navarro-López, C.; López-Nájera, E.; López-Nájera, A.; Jiménez-Díaz, L.; Navarro-López, J.D.; Nájera, A. A Systematic Review and Meta-Analysis of Hospitalised Current Smokers and COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 7394. [Google Scholar] [CrossRef]
- Farsalinos, K.; Barbouni, A.; Niaura, R. Systematic review of the prevalence of current smoking among hospitalized COVID-19 patients in China: Could nicotine be a therapeutic option? Intern. Emerg. Med. 2020, 15, 845–852. [Google Scholar] [CrossRef]
- Piao, W.-H.; Campagnolo, D.; Dayao, C.; Lukas, R.J.; Wu, J.; Shi, F.-D. Nicotine and inflammatory neurological disorders. Acta Pharmacol. Sin. 2009, 30, 715–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zivkovic, A.R.; Decker, S.O.; Zirnstein, A.C.; Sigl, A.; Schmidt, K.; Weigand, M.A.; Hofer, S.; Brenner, T. A Sustained Reduction in Se-rum Cholinesterase Enzyme Activity Predicts Patient Outcome following Sepsis. Mediat. Inflamm. 2018, 2018, 1942193. [Google Scholar] [CrossRef] [Green Version]
- Alqahtani, J.S.; Oyelade, T.; Aldhahir, A.M.; Alghamdi, S.M.; Almehmadi, M.; Alqahtani, A.S.; Quaderi, S.; Mandal, S.; Hurst, J.R. Preva-lence, Severity and Mortality associated with COPD and Smoking in patients with COVID-19: A Rapid Systematic Review and Meta-Analysis. PLoS ONE 2020, 15, e0233147. [Google Scholar] [CrossRef]
- Barbaro, R.P.; MacLaren, G.; Boonstra, P.S.; Iwashyna, T.J.; Slutsky, A.S.; Fan, E.; Bartlett, R.H.; Tonna, J.E.; Hyslop, R.; Fanning, J.J.; et al. Extracorporeal Life Sup-port Organization. Extracorporeal membrane oxygenation support in COVID-19: An international cohort study of the Extra-corporeal Life Support Organization registry. Lancet 2020, 396, 1071–1078. [Google Scholar] [CrossRef]
- Machado, M.; Valerio, M.; Álvarez-Uría, A.; Olmedo, M.; Veintimilla, C.; Padilla, B.; De la Villa, S.; Guinea, J.; Escribano, P.; Ruiz-Serrano, M.J.; et al. Invasive pulmo-nary aspergillosis in the COVID-19 era: An expected new entity. Mycoses 2021, 64, 132–143. [Google Scholar] [CrossRef]
- Koehler, P.; Cornely, O.A.; Böttiger, B.W.; Dusse, F.; Eichenauer, D.A.; Fuchs, F.; Hallek, M.; Jung, N.; Klein, F.; Persigehl, T.; et al. COVID-19 associated pulmonary aspergillosis. Mycoses 2020, 63, 528–534. [Google Scholar] [CrossRef]
- van Arkel, A.L.; Rijpstra, T.A.; Belderbos, H.N.; Van Wijngaarden, P.; Verweij, P.E.; Bentvelsen, R.G. COVID-19-associated Pul-monary Aspergillosis. Am. J. Respir. Crit. Care Med. 2020, 202, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Arastehfar, A.; Carvalho, A.; van de Veerdonk, F.L.; Jenks, J.D.; Koehler, P.; Krause, R.; Cornely, O.A.; Perlin, D.; Lass-Flörl, C.; Hoenigl, M. COVID-19 Associated Pulmonary Aspergillosis (CAPA)-From Immu-nology to Treatment. J. Fungi 2020, 6, 91. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 24 March 2021).
- Patterson, T.F.; Thompson, G.R., III; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Executive Summary: Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, 433–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansuy, J.; Bourcier, M.; Trémeaux, P.; Dimeglio, C.; Izopet, J. COVID-19 pandemic period, where are the seasonal viruses? J. Med. Virol. 2021. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Influenza (n = 64) | COVID-19 (n = 64) | |
|---|---|---|
| 2016/2017 flu season | 27 | 0 |
| 2017/2018 flu season | 11 | 0 |
| 2018/2019 flu season | 17 | 0 |
| 2019/2020 flu season | 9 | 0 |
| January 2020–July 2020 | n/a | 64 |
| Influenza A (non H1N1) | 22 | |
| Influenza A (H1N1) | 36 | |
| Influenza B | 6 | |
| SARS-CoV-2 | 64 |
| Standardized Protocol for ARDS |
|---|
| Diagnostics on Admission |
|
|
|
|
| Therapy |
|
|
|
|
| Specific Treatment | n |
|---|---|
| Influenza—patients | |
| 60 |
| COVID-19—patients | |
| 12 |
| 26 |
| 8 |
| 2 |
| Influenza (n = 64) | COVID-19 (n = 64) | Std Diff # | p-Value | |
|---|---|---|---|---|
| Age [years] | 54.1 (49.8; 58.4) | 60.1 (56.9; 63.3) | 0.39 | 0.0211 § |
| Sex [male] | 41 (64%) | 54 (84%) | 0.40 | 0.0292 $ |
| BMI [kg m−2] | 30.2 (27.9; 32.5) | 28.8 (25.2; 32.4) | 0.18 | 0.5669 § |
| Charlson Comorbidity Index | 2.53 (1.93; 3.13) | 2.48 (2.00; 2.97) | 0.02 | 0.9847 § |
| Active Smoker | 16 (25%) | 4 (6.3%) | 0.53 | 0.0037 $ |
| Transfer from other hospital | 39 (60.9%) | 43 (67.2%) | 0.12 | 0.4651 $ |
| SAPS II on admission | 30.92 (26.56; 35.27) | 36.90 (33.89; 39.91) | 0.40 | 0.0261 § |
| Influenza (n = 64) | COVID-19 (n = 64) | p-Value | |
|---|---|---|---|
| Mortality | 19 (29.7%) | 22 (34.3%) | 0.568 |
| Any ECMO | 29 (45.3%) | 18 (28.1%) | 0.044 |
| Mortality with ECMO | 11/29 (37.9%) | 12/18 (66.7%) | 0.055 |
| Invasive ventilation | 56 (87.5%) | 50 (78.1%) | 0.160 |
| Time in ICU [days] | 23.1 (15.9; 30.3) | 15.5 (12.3; 18.7) | 0.0549 |
| Any dialysis (CVVHD) in ICU | 32 (50.0%) | 24 (37.5%) | 0.131 |
| Any bacteremia | 46 (71.9%) | 33 (51.6%) | 0.023 |
| Any invasive aspergillosis | 12 (18.8%) | 5 (7.8%) | 0.063 |
| TISS points per day | 15.50 (12.77; 18.21) | 17.14 (13.77; 20.51) | 0.448 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herbstreit, F.; Overbeck, M.; Berger, M.M.; Skarabis, A.; Brenner, T.; Schmidt, K. Characteristics of Critically Ill Patients with COVID-19 Compared to Patients with Influenza—A Single Center Experience. J. Clin. Med. 2021, 10, 2056. https://doi.org/10.3390/jcm10102056
Herbstreit F, Overbeck M, Berger MM, Skarabis A, Brenner T, Schmidt K. Characteristics of Critically Ill Patients with COVID-19 Compared to Patients with Influenza—A Single Center Experience. Journal of Clinical Medicine. 2021; 10(10):2056. https://doi.org/10.3390/jcm10102056
Chicago/Turabian StyleHerbstreit, Frank, Marvin Overbeck, Marc Moritz Berger, Annabell Skarabis, Thorsten Brenner, and Karsten Schmidt. 2021. "Characteristics of Critically Ill Patients with COVID-19 Compared to Patients with Influenza—A Single Center Experience" Journal of Clinical Medicine 10, no. 10: 2056. https://doi.org/10.3390/jcm10102056