
Interaction between Health and Financial Status on Coping Behaviors during the COVID-19 Pandemic
Abstract
:1. Introduction
- Why do some people give up or refuse to collaborate in the public’s efforts to control the spread of the virus and restore public life?
- Why are people from low financial status more likely to apply the shift-and-persist strategy during a pandemic?
2. Method
2.1. Sample and Recruitment
2.2. Measures
2.2.1. Active Coping
2.2.2. Give-Up
2.2.3. Confidence in Coping Abilities
2.2.4. Optimism
2.2.5. Denial
2.2.6. Anxiousness
2.2.7. Health Status
2.2.8. Financial Status
2.3. Procedure
2.4. Statistical Analyses
3. Results
3.1. Effect of Financial Status on Active Coping and Give-Up
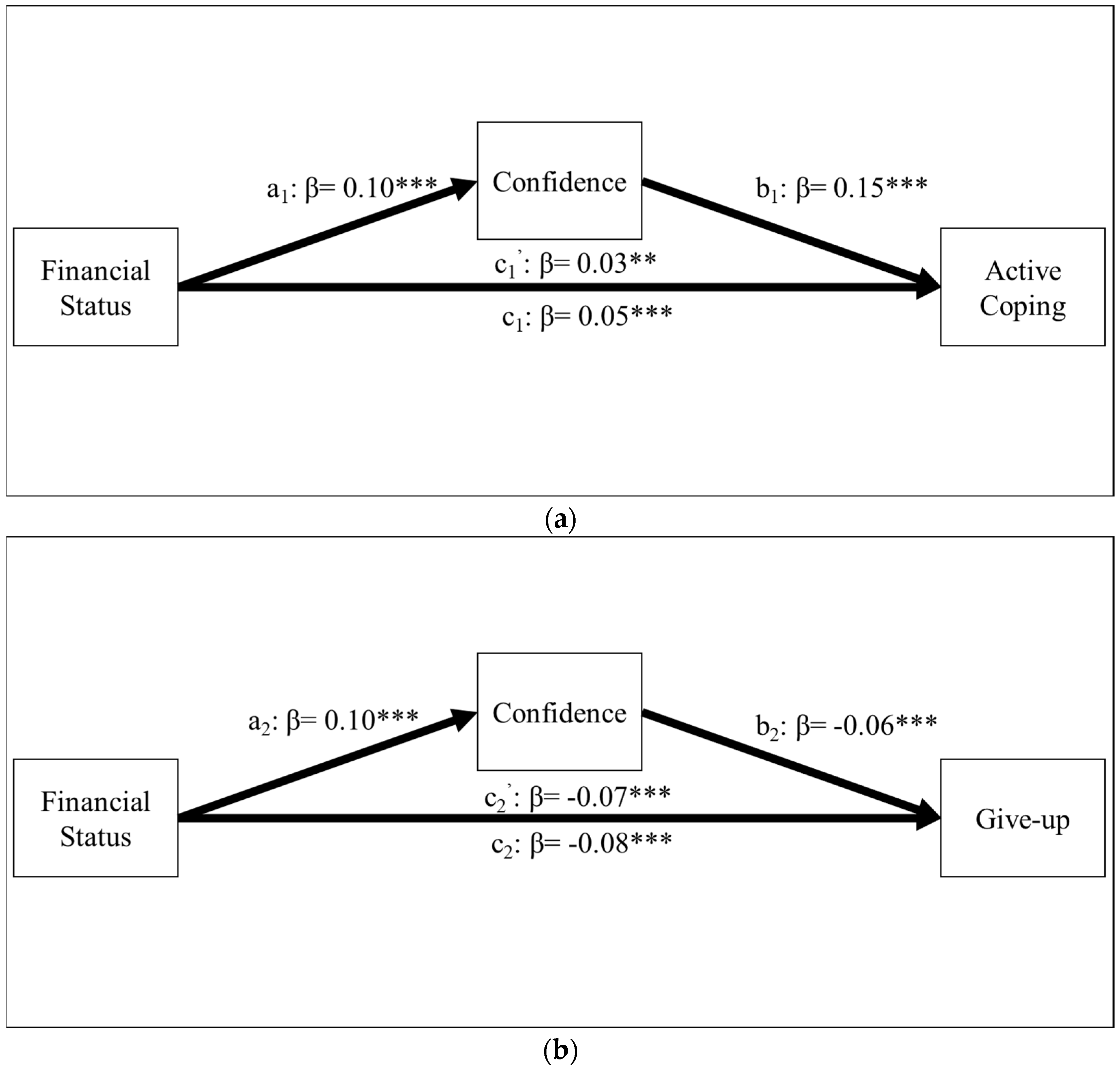
3.2. Mediating Effect of Confidence in Coping Abilities
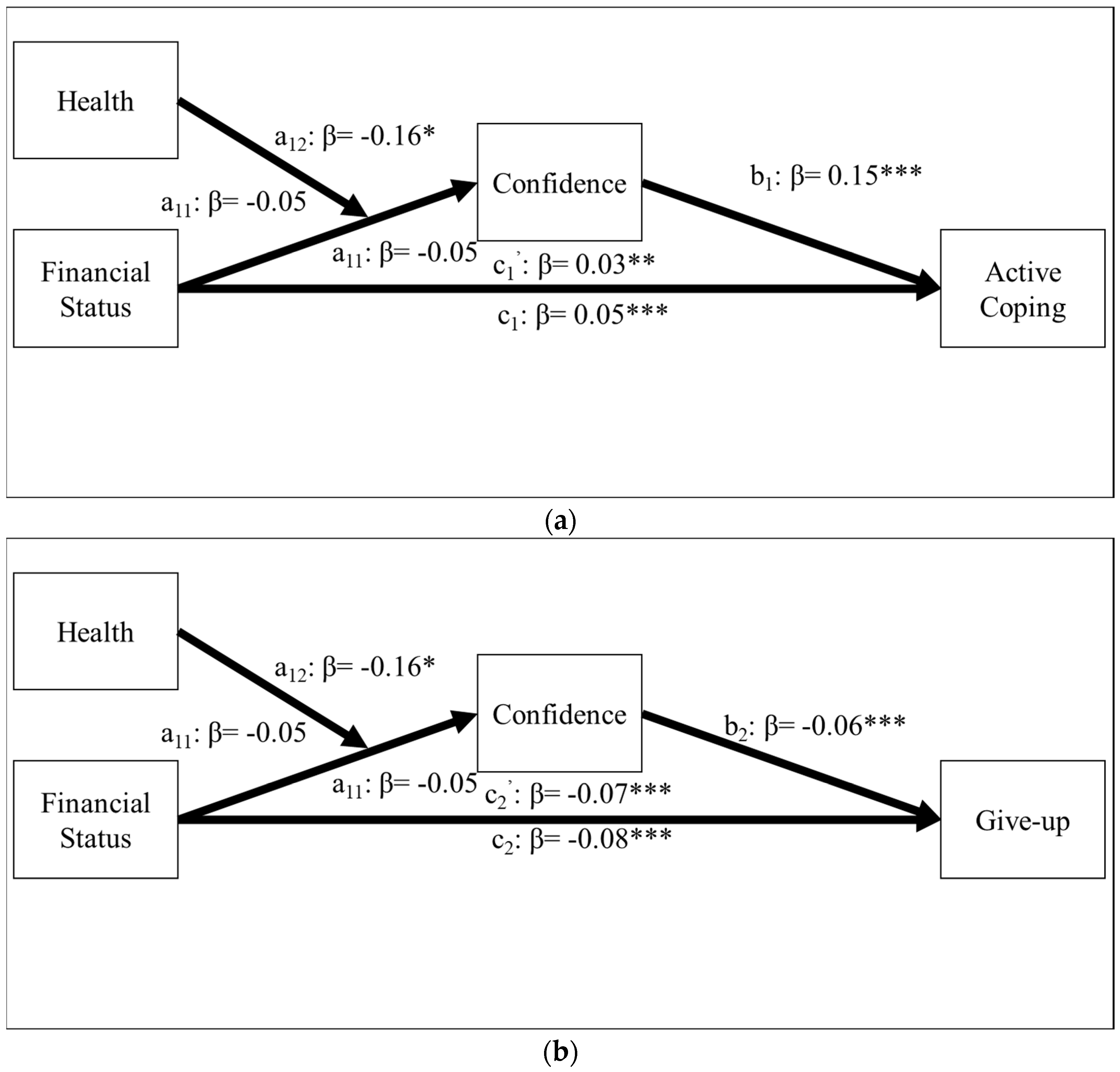
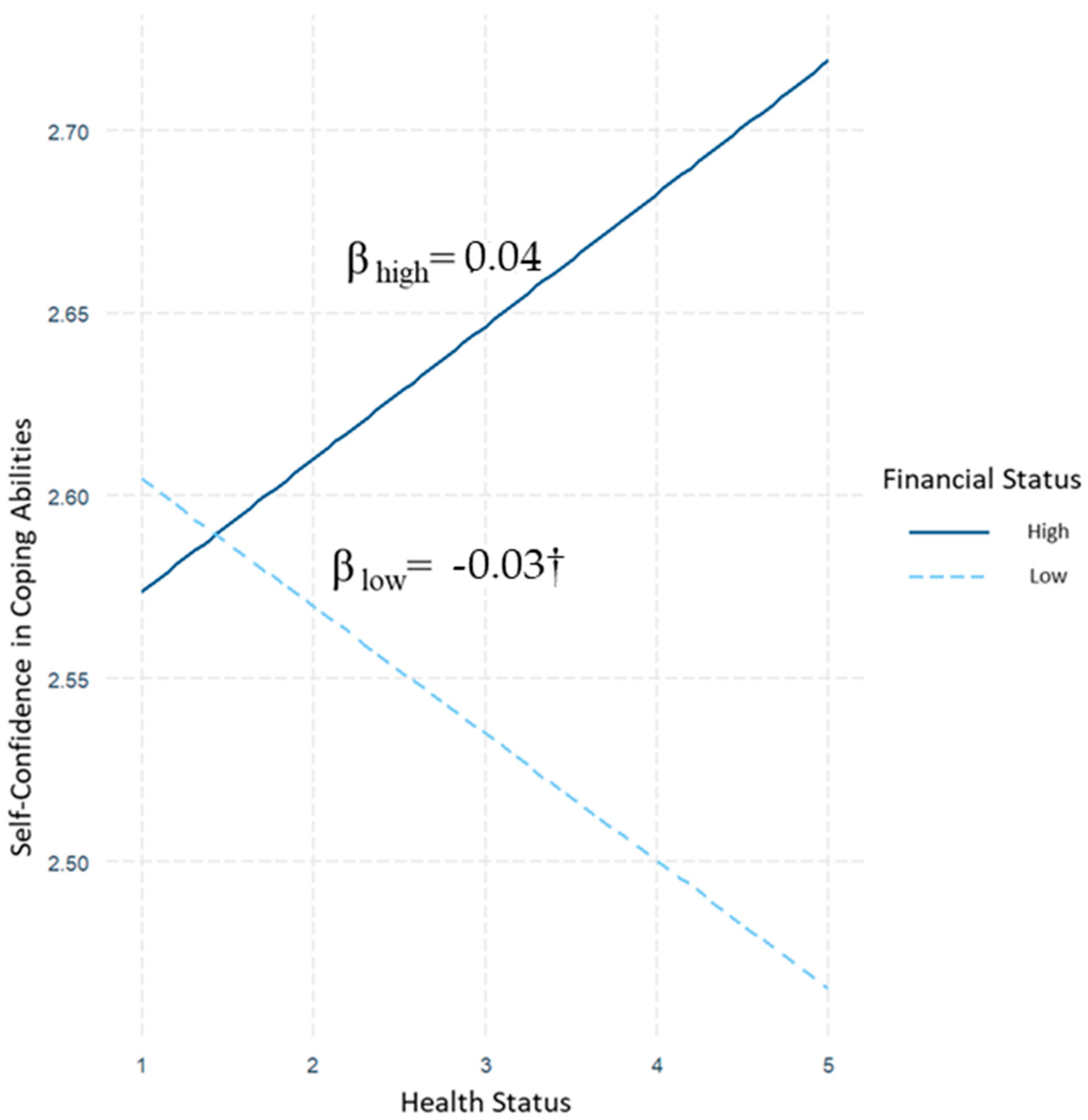
3.3. Moderating Effect of Health Status
3.4. Robustness Check
4. General Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Worldometeter. Available online: https://www.worldometers.info/coronavirus/ (accessed on 7 February 2022).
- Uddin, S.; Imam, T.; Khushi, M.; Khan, A.; Moni, M.A. How did socio-demographic status and personal attributes influence compliance to COVID-19 preventive behaviours during the early outbreak in Japan? Lessons for pandemic management. Pers. Individ. Differ. 2021, 175, 110692. [Google Scholar] [CrossRef] [PubMed]
- Shackle, S. Among the COVID Sceptics: ‘We Are Being Manipulated, without a Shadow of a Doubt. Available online: https://www.theguardian.com/news/2021/apr/08/among-covid-sceptics-we-are-being-manipulated-anti-lockdown (accessed on 6 April 2022).
- Lowrie, M. Quebec Declares the Beginning of Second-Wave as COVID-19 Gains Steam in Central Canada. Available online: https://www.thestar.com/news/canada/2020/09/21/quebec-declares-beginning-of-second-wave-as-covid-19-gains-steam-in-central-canada.html (accessed on 7 February 2022).
- Newton, P. Crowds of Demonstrators Join Rallies across Canada as COVID-19 Trucker Protests Spread. Available online: https://www.cnn.com/2022/02/05/americas/canada-trucker-protest-covid-19/index.html (accessed on 28 March 2022).
- Hesson, T. Trucks, RVs and Cars Converge on the Outskirts of Washington to Protest COVID-19 Restrictions. Available online: https://www.theglobeandmail.com/world/article-trucks-rvs-and-cars-flock-to-washington-area-to-protest-covid-19/ (accessed on 7 March 2022).
- Liu, Q.; Liu, Y.; Zhang, C.; An, Z.; Zhao, P. Elderly mobility during the COVID-19 pandemic: A qualitative exploration in Kunming, China. J. Transp. Geogr. 2021, 96, 103176. [Google Scholar] [CrossRef] [PubMed]
- Anglim, J.; Horwood, S. Effect of the COVID-19 pandemic and big five personality on subjective and psychological wellbeing. Soc. Psychol. Personal. Sci. 2021, 12, 1527–1537. [Google Scholar] [CrossRef]
- Modersitzki, N.; Phan, L.V.; Kuper, N.; Rauthmann, J.F. Who is impacted? Personality predicts individual differences in psychological consequences of the COVID-19 pandemic in Germany. Soc. Psychol. Personal. Sci. 2021, 12, 1110–1130. [Google Scholar] [CrossRef]
- Chan, H.F.; Moon, J.W.; Savage, D.A.; Skali, A.; Torgler, B.; Whyte, S. Can psychological traits explain mobility behavior during the COVID-19 pandemic? Soc. Psychol. Personal. Sci. 2021, 12, 1018–1029. [Google Scholar] [CrossRef]
- Blagov, P.S. Adaptive and dark personality in the COVID-19 pandemic: Predicting health-behavior endorsement and the appeal of public-health messages. Soc. Psychol. Personal. Sci. 2021, 12, 697–707. [Google Scholar] [CrossRef]
- Oishi, S.; Cha, Y.; Schimmack, U. The social ecology of COVID-19 cases and deaths in New York City: The role of walkability, wealth, and race. Soc. Psychol. Personal. Sci. 2021, 12, 1457–1466. [Google Scholar] [CrossRef]
- Berkessel, J.B.; Ebert, T.; Gebauer, J.E.; Jonsson, T.; Oishi, S. Pandemics initially spread among people of higher (not lower) social status: Evidence from COVID-19 and the Spanish Flu. Soc. Psychol. Personal. Sci. 2021, 13, 19485506211039990. [Google Scholar] [CrossRef]
- Chen, E.; Miller, G.E. “Shift-and-persist” strategies: Why low socioeconomic status isn’t always bad for health. Perspect. Psychol. Sci. 2012, 7, 135–158. [Google Scholar] [CrossRef] [Green Version]
- Chen, E.; Miller, G.E.; Lachman, M.E.; Gruenewald, T.L.; Seeman, T.E. Protective factors for adults from low childhood socioeconomic circumstances: The benefits of shift-and-persist for allostatic load. Psychosom. Med. 2012, 74, 178. [Google Scholar] [CrossRef]
- Lam, P.H.; Miller, G.E.; Chiang, J.J.; Levine, C.S.; Le, V.; Shalowitz, M.U.; Chen, E. One size does not fit all: Links between shift-and-persist and asthma in youth are moderated by perceived social status and experience of unfair treatment. Dev. Psychopathol. 2018, 30, 1699–1714. [Google Scholar] [CrossRef] [Green Version]
- Chen, E.; Miller, G.E. Socioeconomic status and health: Mediating and moderating factors. Annu. Rev. Clin. Psychol. 2013, 9, 723–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kallem, S.; Carroll-Scott, A.; Rosenthal, L.; Chen, E.; Peters, S.M.; McCaslin, C.; Ickovics, J.R. Shift-and-persist: A protective factor for elevated BMI among low-socioeconomic-status children. Obesity 2013, 21, 1759–1763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, E.; McLean, K.C.; Miller, G.E. Shift-and-persist strategies: Associations with socioeconomic status and the regulation of inflammation among adolescents and their parents. Psychosom. Med. 2015, 77, 371. [Google Scholar] [CrossRef] [PubMed]
- Stein, G.L.; Jensen, M.; Christophe, N.K.; Cruz, R.A.; Martin Romero, M.; Robins, R. Shift and Persist in Mexican American Youth: A Longitudinal Test of Depressive Symptoms. J. Res. Adolesc. 2022, 1–19. [Google Scholar] [CrossRef]
- Kraus, M.W.; Piff, P.K.; Keltner, D. Social class, sense of control, and social explanation. J. Pers. Soc. Psychol. 2009, 97, 992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, M.; Abraham, C.; Bond, R. Psychological correlates of university students’ academic performance: A systematic review and meta-analysis. Psychol. Bull. 2012, 138, 353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowe, N.K. Maternal confidence in coping with labor a self-efficacy concept. J. Obstet. Gynecol. Neonatal. Nurs. 1991, 20, 457–463. [Google Scholar] [CrossRef]
- Holahan, C.J.; Moos, R.H. Personal and contextual determinants of coping strategies. J. Pers. Soc. Psychol. 1987, 52, 946. [Google Scholar] [CrossRef]
- O’Toole, J.K.; Burkhardt, M.C.; Solan, L.G.; Vaughn, L.; Klein, M.D. Resident confidence addressing social history: Is it influenced by availability of social and legal resources? Clin. Pediatr. 2012, 51, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Ingham, G. The Nature of Money; John Wiley & Sons: Hoboken, NJ, USA, 2004. [Google Scholar]
- Diefenbach, T. Intangible resources: A categorical system of knowledge and other intangible assets. J. Intellect. Cap. 2006, 7, 406–420. [Google Scholar] [CrossRef] [Green Version]
- Buka, S.L.; Stichick, T.L.; Birdthistle, I.; Earls, F.J. Youth exposure to violence: Prevalence, risks, and consequences. Am. J. Orthopsychiatry 2001, 71, 298–310. [Google Scholar] [CrossRef] [PubMed]
- De Cremer, D.; Van Knippenberg, D. Leader self-sacrifice and leadership effectiveness: The moderating role of leader self-confidence. Organ. Behav. Hum. Decis. Process. 2004, 95, 140–155. [Google Scholar] [CrossRef]
- Hollenbeck, J.R.; Klein, H.J. Goal commitment and the goal-setting process: Problems, prospects, and proposals for future research. J. Appl. Psychol. 1987, 72, 212. [Google Scholar] [CrossRef] [Green Version]
- Adler, N.E.; Snibbe, A.C. The role of psychosocial processes in explaining the gradient between socioeconomic status and health. Curr. Dir. Psychol. Sci. 2003, 12, 119–123. [Google Scholar] [CrossRef]
- Adler, N.E.; Epel, E.S.; Castellazzo, G.; Ickovics, J.R. Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy, White women. Health Psychol. 2000, 19, 586. [Google Scholar] [CrossRef]
- Song, Y.; Liu, T.; Wang, X.; Guan, T. Fragmented restrictions, fractured resonances: Grassroots responses to Covid-19 in China. Crit. Asian Stud. 2020, 52, 494–511. [Google Scholar] [CrossRef]
- Chinazzi, M.; Davis, J.T.; Ajelli, M.; Gioannini, C.; Litvinova, M.; Merler, S.; Vespignani, A. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science 2020, 368, 395–400. [Google Scholar] [CrossRef] [Green Version]
- Pan, S.L.; Cui, M.; Qian, J. Information resource orchestration during the COVID-19 pandemic: A study of community lockdowns in China. Int. J. Inf. Manag. 2020, 54, 102143. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Yang, Z.; Qiu, H.; Wang, Y.; Jian, L.; Ji, J.; Li, K. Anxiety and depression among general population in China at the peak of the COVID-19 epidemic. World Psychiatry 2020, 19, 249. [Google Scholar] [CrossRef] [PubMed]
- Bao, W. Bridging the gap between research and practice: Identifying high-impact educational practices for Chinese undergraduate education. Peking Univ. Edu. Rev. 2019, 1, 105–129. [Google Scholar]
- Wang, X. Rethinking Universalism in the Context of China. Soc. Democr. 2012, 26, 18–35. [Google Scholar] [CrossRef]
- Lee, J.K.; Bullen, C.; Ben Amor, Y.; Bush, S.R.; Colombo, F.; Gaviria, A.; Karim, S.S.A.; Kim, B.; Lavis, J.N.; Lazarus, J.V. Lancet COVID-19 Commission Task Force for Public Health Measures to Suppress the Pandemic. Institutional and behaviour-change interventions to support COVID-19 public health measures: A review by the Lancet Commission Task Force on public health measures to suppress the pandemic. Int. Health 2021, 13, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Sebhatu, A.; Wennberg, K.; Arora-Jonsson, S.; Lindberg, S.I. Explaining the homogeneous diffusion of COVID-19 nonpharmaceutical interventions across heterogeneous countries. Proc. Natl. Acad. Sci. USA 2020, 117, 21201–21208. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Pers. Soc. Psychol. 2013, 56, 267–283. [Google Scholar] [CrossRef]
- Heppner, P. The Problem-Solving Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1988. [Google Scholar]
- Zhang, W.; Gao, F.; Gross, J.; Shrum, L.J.; Hayne, H. How does social distancing during COVID-19 affect negative moods and memory? Memory 2021, 29, 90–97. [Google Scholar] [CrossRef]
- Brcic, V.; Eberdt, C.; Kaczorowski, J. Development of a tool to identify poverty in a family practice setting: A pilot study. Int. J. Family Med. 2011, 2011, 812182. [Google Scholar] [CrossRef] [Green Version]
- Asadullah, M.N.; Chaudhury, N. Subjective wellbeing and relative poverty in rural Bangladesh. J. Econ. Psychol. 2012, 33, 940–950. [Google Scholar] [CrossRef] [Green Version]
- Hayes, A.F. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modeling. 2012. Available online: http://www.afhayes.com/public/process2012.pdf (accessed on 21 September 2021).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Xie, W.; Campbell, S.; Zhang, W. Working memory capacity predicts individual differences in social-distancing compliance during the COVID-19 pandemic in the United States. Proc. Natl. Acad. Sci. USA 2020, 117, 17667–17674. [Google Scholar] [CrossRef]
- Galasso, V.; Pons, V.; Profeta, P.; Becher, M.; Brouard, S.; Foucault, M. Gender differences in COVID-19 attitudes and behavior: Panel evidence from eight countries. Proc. Natl. Acad. Sci. USA 2020, 117, 27285–27291. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, M.J.; Jackson, J.C.; Pan, X.; Nau, D.; Pieper, D.; Denison, E.; Wang, M. The relationship between cultural tightness–looseness and COVID-19 cases and deaths: A global analysis. Lancet Planet. Health 2021, 5, e135–e144. [Google Scholar] [CrossRef]
- Gadarian, S.K.; Goodman, S.W.; Pepinsky, T. Partisan endorsement experiments do not affect mass opinion on COVID-19. J. Elect. Public Opin. Parties 2021, 31 (Suppl. 1), 122–131. [Google Scholar] [CrossRef]
- Siritzky, M.; Condon, D.; Weston, S. The role of personality in shaping pandemic response: Systemic sociopolitical factors drive country differences. Soc. Psychol. Personal. Sci. 2022, 13, 246–263. [Google Scholar] [CrossRef]
- Woo, R.; Liu, R. With Carrot and Stick, China Presses Ahead with COVID Vaccinations for Elderly. Available online: https://www.reuters.com/world/china/with-carrot-stick-china-presses-ahead-with-covid-vaccinations-elderly-2022-04-01/ (accessed on 3 May 2022).
- Organisation for Economic Co-Operation and Development. What Is the Impact of the COVID-19 Pandemic on Immigrants and Their Children; OECD Publishing: Paris, France, 2020. [Google Scholar]
- Siegel, R.M.; Mallow, P.J. The impact of COVID-19 on vulnerable populations and implications for children and health care policy. Clin. Pediatr. 2021, 60, 93–98. [Google Scholar] [CrossRef]
- Shadmi, E.; Chen, Y.; Dourado, I.; Faran-Perach, I.; Furler, J.; Hangoma, P.; Willems, S. Health equity and COVID-19: Global perspectives. Int. J. Equity Health 2020, 19, 104. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Liu, Z.; Kang, T.; Zhu, L.; Zhao, P. Transport inequities through the lens of environmental racism: Rural-urban migrants under Covid-19. Transp. Policy 2022, 122, 26–38. [Google Scholar] [CrossRef]
- d’Errico, A.; Punnett, L.; Cifuentes, M.; Boyer, J.; Tessler, J.; Gore, R.; Slatin, C. Hospital injury rates in relation to socioeconomic status and working conditions. Occup. Environ. Med. 2007, 64, 325–333. [Google Scholar] [CrossRef]
- Fischer, R.; Karl, J.A. Predicting behavioral intentions to prevent or mitigate COVID-19: A cross-cultural meta-analysis of attitudes, norms, and perceived behavioral control effects. Soc. Psychol. Personal. Sci. 2022, 13, 264–276. [Google Scholar] [CrossRef]
- Dawkins, G. Man Charged in Hit and Run during Freedom Convoy Protest, Injuring Four. Available online: https://www.saltwire.com/atlantic-canada/news/man-charged-in-hit-and-run-during-freedom-convoy-protest-injuring-four-100689469/ (accessed on 6 April 2022).
- Edsall, T.B. Where Does All That Hate We Feel Come from? Available online: https://www.nytimes.com/2022/04/27/opinion/rich-poor-immigration-fear.html (accessed on 3 May 2022).
- Chen, X. Growing up in a collectivist culture: Socialization and socioemotional development in Chinese children. In International Perspectives on Human Development; Pabst Science Publishers: Lengerich, Germany, 2000; pp. 331–353. [Google Scholar]
- Huang, Y. Collectivism, political control, and gating in Chinese cities. Urban Geogr. 2006, 27, 507–525. [Google Scholar] [CrossRef] [Green Version]
- Gong, W.; Zhu, M.; Gürel, B.; Xie, T. The lineage theory of the regional variation of individualism/collectivism in China. Front. Psychol. 2021, 11, 4047. [Google Scholar] [CrossRef] [PubMed]
- Newitz, A. Don’t Shame Your Neighbors. Available online: https://www.nytimes.com/2020/10/16/opinion/shame-masks-coronavirus-covid.html (accessed on 6 April 2022).
- Daniel, E.; Bardi, A.; Fischer, R.; Benish-Weisman, M.; Lee, J.A. Changes in personal values in pandemic times. Soc. Psychol. Personal. Sci. 2021, 13, 19485506211024026. [Google Scholar] [CrossRef]
- Pennycook, G.; McPhetres, J.; Zhang, Y.; Lu, J.G.; Rand, D.G. Fighting COVID-19 misinformation on social media: Experimental evidence for a scalable accuracy-nudge intervention. Psychol. Sci. 2020, 31, 770–780. [Google Scholar] [CrossRef] [PubMed]
- Koetke, J.; Schumann, K.; Porter, T. Intellectual humility predicts scrutiny of COVID-19 misinformation. Soc. Psychol. Personal. Sci. 2021, 13, 1948550620988242. [Google Scholar] [CrossRef]
- Pummerer, L.; Böhm, R.; Lilleholt, L.; Winter, K.; Zettler, I.; Sassenberg, K. Conspiracy theories and their societal effects during the COVID-19 pandemic. Soc. Psychol. Personal. Sci. 2022, 13, 49–59. [Google Scholar] [CrossRef]
- Gollwitzer, A.; McLoughlin, K.; Martel, C.; Marshall, J.; Höhs, J.M.; Bargh, J.A. Linking self-reported social distancing to real-world behavior during the COVID-19 pandemic. Soc. Psychol. Personal. Sci. 2021, 13, 19485506211018132. [Google Scholar] [CrossRef]
- Chambon, M.; Dalege, J.; Elberse, J.E.; van Harreveld, F. A psychological network approach to attitudes and preventive behaviors during pandemics: A COVID-19 study in the United Kingdom and the Netherlands. Soc. Psychol. Personal. Sci. 2022, 13, 233–245. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | M | SD | Reliability |
|---|---|---|---|
| Active | 2.49 | 0.86 | r = 0.75 |
| Give-up | 1.49 | 0.82 | r = 0.87 |
| Confidence | 2.59 | 0.84 | α = 0.90 |
| Optimism | 2.39 | 0.85 | r = 0.62 |
| Denial | 1.74 | 0.88 | r = 0.79 |
| Anxiousness | 2.26 | 1.21 | N/A |
| Health | 4.36 | 0.84 | N/A |
| Financial Status | 4.70 | 1.04 | α = 0.78 |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| Active | - | |||||||
| Give-up | 0.18 *** | - | ||||||
| Confidence | 0.33 *** | 0.02 | - | |||||
| Optimism | 0.59 *** | 0.32 *** | 0.32 *** | - | ||||
| Denial | 0.36 *** | 0.53 *** | 0.09 *** | 0.33 *** | - | |||
| Anxiousness | –0.02 | 0.11 *** | –0.16 *** | –0.03 | 0.12 *** | - | ||
| Health | –0.04 * | –0.10 *** | –0.01 | –0.07 *** | –0.15 *** | –0.07 *** | - | |
| Financial Status | 0.07 *** | –0.18 *** | 0.18 *** | 0.07 *** | –0.23 *** | –0.19 *** | 0.04 * | - |
| Step and Variable | Model 1: Active Coping | Model 2: Give-Up |
|---|---|---|
| Step 1 | ||
| Age | –0.02 (0.01) † | –0.01 (0.01) |
| Sex (Men) | 0.02 (0.02) | 0.04 (0.02) † |
| Marital Status (Married) | –0.04 (0.03) | –0.05 (0.03) † |
| Education Level | 0.05 (0.01) *** | –0.03 (0.01) ** |
| Optimism | 0.52 (0.01) *** | 0.17 (0.01) *** |
| Denial | 0.19 (0.01) *** | 0.42 (0.01) *** |
| Anxiousness | –0.02 (0.01) * | 0.04 (0.01) *** |
| Health | 0.02 (0.01) | –0.05 (0.01) *** |
| Adjusted R-squared | 0.3852 | 0.3080 |
| Step 2 | ||
| Age | –0.03 (0.01) * | 0.002 (0.01) |
| Sex (Men) | 0.03 (0.02) | 0.03 (0.02) |
| Marital Status (Married) | –0.04 (0.03) | –0.05 (0.03) † |
| Education | 0.04 (0.01) *** | –0.01 (0.01) |
| Optimism | 0.52 (0.01) *** | 0.18 (0.01) *** |
| Denial | 0.20 (0.01) *** | 0.41 (0.01) *** |
| Anxiousness | –0.01 (0.01) | 0.02 (0.01) ** |
| Health | 0.01 (0.01) | –0.04 (0.01) ** |
| Financial Status | 0.05 (0.01) *** | –0.08 (0.01) *** |
| Adjusted R-squared | 0.3878 | 0.3158 |
| Δ R-squared | 0.0026 *** | 0.0078 *** |
| F-test | 17.13 | 44.22 |
| Variables | Model 1: Active Coping | Model 2: Give-Up |
|---|---|---|
| Age | –0.03 * | 0.004 |
| (0.01) | (0.01) | |
| Sex (Men) | 0.01 | 0.04 † |
| (0.02) | (0.02) | |
| Marital Status (Not married) | –0.05 † | –0.05 † |
| (0.03) | (0.03) | |
| Education | 0.03 ** | –0.002 |
| (0.01) | (0.01) | |
| Confidence | 0.15 *** | –0.06 *** |
| (0.01) | (0.01) | |
| Optimism | 0.47 *** | 0.20 *** |
| (0.01) | (0.01) | |
| Denial | 0.19 *** | 0.41 *** |
| (0.01) | (0.01) | |
| Anxiousness | –0.004 | 0.02 * |
| (0.01) | (0.01) | |
| Financial Status | 0.03 ** | –0.07 *** |
| (0.01) | (0.01) | |
| Index of Mod. Med. | [0.001, 0.01] | [–0.004, –0.0003] |
| Potential Mediators | Active C | Give-Up |
|---|---|---|
| 95% CI | 95% CI | |
| Optimism | [–0.01, 0.02] | [–0.003, 0.01] |
| Denial | [–0.003, 0.01] | [–0.01, 0.02] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yanit, M.; Shi, K.; Wan, F.; Gao, F. Interaction between Health and Financial Status on Coping Behaviors during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 13498. https://doi.org/10.3390/ijerph192013498
Yanit M, Shi K, Wan F, Gao F. Interaction between Health and Financial Status on Coping Behaviors during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(20):13498. https://doi.org/10.3390/ijerph192013498
Chicago/Turabian StyleYanit, Mehmet, Kan Shi, Fang Wan, and Fei Gao. 2022. "Interaction between Health and Financial Status on Coping Behaviors during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 20: 13498. https://doi.org/10.3390/ijerph192013498