
How Did Work-Related Depression, Anxiety, and Stress Hamper Healthcare Employee Performance during COVID-19? The Mediating Role of Job Burnout and Mental Health





Abstract
:1. Introduction
2. Theoretical Background
2.1. Stress and Employee Performance
2.2. Depression and Employee Performance
2.3. Anxiety and Employee Performance
2.4. The Mediating Role of Job Burnout
2.5. The Mediating Role of Mental Health
3. Methods
3.1. Study Procedure
3.2. Common Method Bias
3.3. Measures
3.4. Statistical Analysis
4. Results
Assessment of Model Fit and Measurement Model
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Silva, P.C.; Batista, P.V.; Lima, H.S.; Alves, M.A.; Guimarães, F.G.; Silva, R.C. COVID-ABS: An agent-based model of COVID-19 epidemic to simulate health and economic effects of social distancing interventions. Chaos Solitons Fractals 2020, 139, 110088. [Google Scholar] [CrossRef] [PubMed]
- Xiao, C. A novel approach of consultation on 2019 novel coronavirus (COVID-19)-related psychological and mental problems: Structured letter therapy. Psychiatry Investig. 2020, 17, 175–176. [Google Scholar] [CrossRef] [PubMed]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Razu, S.R.; Yasmin, T.; Arif, T.B.; Islam, S.; Islam, S.M.S.; Gesesew, H.A.; Ward, P. Challenges Faced by Healthcare Professionals during the COVID-19 Pandemic: A Qualitative Inquiry from Bangladesh. Front. Public Health 2021, 9, 647315. [Google Scholar] [CrossRef]
- Khan, A.A.; Lodhi, F.S.; Rabbani, U.; Ahmed, Z.; Abrar, S.; Arshad, S.; Khan, M.I. Impact of coronavirus disease (COVID-19) pandemic on psychological well-being of the Pakistani general population. Front. Psychiatry 2021, 11, 564364. [Google Scholar] [CrossRef]
- Zheng, W. Mental health and a novel coronavirus (2019-nCoV) in China. J. Affect. Disord. 2020, 269, 201–202. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef]
- Sun, J.; Sarfraz, M.; Khawaja, K.F.; Ozturk, I.; Raza, M.A. The Perils of the Pandemic for the Tourism and Hospitality Industries: Envisaging the Combined Effect of COVID-19 Fear and Job Insecurity on Employees’ Job Performance in Pakistan. Psychol. Res. Behav. Manag. 2022, 15, 1325–1346. [Google Scholar] [CrossRef]
- Muller, A.E.; Hafstad, E.V.; Himmels, J.P.W.; Smedslund, G.; Flottorp, S.; Stensland, S.Ø.; Stroobants, S.; Van de Velde, S.; Vist, G.E. The mental health impact of the COVID-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Res. 2020, 293, 113441. [Google Scholar] [CrossRef]
- Greenberg, N.; Docherty, M.; Gnanapragasam, S.; Wessely, S. Managing mental health challenges faced by healthcare workers during COVID-19 pandemic. BMJ 2020, 368, m1211. [Google Scholar] [CrossRef]
- Sarfraz, M.; Ji, X.; Asghar, M.; Ivascu, L.; Ozturk, I. Signifying the Relationship between Fear of COVID-19, Psychological Concerns, Financial Concerns and Healthcare Employees Job Performance: A Mediated Model. Int. J. Environ. Res. Public Health 2022, 19, 2657. [Google Scholar] [CrossRef]
- Fernandez, R.; Sikhosana, N.; Green, H.; Halcomb, E.J.; Middleton, R.; Alananzeh, I.; Trakis, S.; Moxham, L. Anxiety and depression among healthcare workers during the COVID-19 pandemic: A systematic umbrella review of the global evidence. BMJ Open 2021, 11, e054528. [Google Scholar] [CrossRef] [PubMed]
- Aguiar-Quintana, T.; Nguyen, T.H.H.; Araujo-Cabrera, Y.; Sanabria-Díaz, J.M. Do job insecurity, anxiety and depression caused by the COVID-19 pandemic influence hotel employees’ self-rated task performance? The moderating role of employee resilience. Int. J. Hosp. Manag. 2021, 94, 102868. [Google Scholar] [CrossRef] [PubMed]
- Zahra, M.; Akhtar, A.; Arzoo, H.; Humayun, S.; Aman, H.; Andleeb, S.N. Exploring Stress Coping Strategies of Front-Line Emergency Medical Experts Dealing COVID-19 in Pakistan: A Qualitative Inquiry. Multicult. Educ. 2021, 7. [Google Scholar] [CrossRef]
- Wang, L.; Wang, H.; Shao, S.; Jia, G.; Xiang, J. Job Burnout on Subjective Well-Being among Chinese Female Doctors: The Moderating Role of Perceived Social Support. Front. Psychol. 2020, 11, 435. [Google Scholar] [CrossRef]
- Guixia, L.; Hui, Z. A Study on Burnout of Nurses in the Period of COVID-19. Psychol. Behav. Sci. 2020, 9, 31. [Google Scholar] [CrossRef]
- Yunita, P.I.; Saputra, I.G.N.W.H. Millennial generation in accepting mutations: Impact on work stress and employee performance. Int. J. Soc. Sci. Humanit. 2019, 3, 102–114. [Google Scholar] [CrossRef]
- Prasada, K.D.V.; Vaidyab, R.W.; Mangipudic, M.R. Effect of occupational stress and remote working on psychological well-being of employees: An empirical analysis during COVID-19 pandemic concerning information technology industry in hyderabad. Indian J. Commer. Manag. Stud. 2020, 11, 1–13. [Google Scholar] [CrossRef]
- Darvishmotevali, M.; Ali, F. Job insecurity, subjective well-being and job performance: The moderating role of psychological capital. Int. J. Hosp. Manag. 2020, 87, 102462. [Google Scholar] [CrossRef]
- Tu, Y.; Li, D.; Wang, H.-J. COVID-19-induced layoff, survivors’ COVID-19-related stress and performance in hospitality industry: The moderating role of social support. Int. J. Hosp. Manag. 2021, 95, 102912. [Google Scholar] [CrossRef]
- Galbraith, N.; Boyda, D.; McFeeters, D.; Hassan, T. The mental health of doctors during the COVID-19 pandemic. BJPsych Bull. 2021, 45, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Guo, Y.; Ma, T.; Yang, T.; Tian, X. How job stress influences job performance among Chinese healthcare workers: A cross-sectional study. Environ. Health Prev. Med. 2019, 24, 2. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Gu, Y.; Guo, J.; Liao, L.; Wang, B.; Li, X.; Guo, L.; Tong, Z.; Guan, Q.; Zhou, M.; Wu, Y.; et al. Psychological effects of COVID-19 on hospital staff: A national cross-sectional survey in mainland China. Vasc. Investig. Ther. 2021, 4, 6. [Google Scholar] [CrossRef]
- Heath, C.; Sommerfield, A.; Von Ungern-Sternberg, B.S. Resilience strategies to manage psychological distress among healthcare workers during the COVID-19 pandemic: A narrative review. Anaesthesia 2020, 75, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Hadi, S.A.; Bakker, A.B.; Häusser, J.A. The role of leisure crafting for emotional exhaustion in telework during the COVID-19 pandemic. Anxiety Stress Coping 2021, 34, 530–544. [Google Scholar] [CrossRef] [PubMed]
- Sarfraz, M.; Hafeez, H.; Abdullah, M.I.; Ivascu, L.; Ozturk, I. The effects of the COVID-19 pandemic on healthcare workers’ psychological and mental health: The moderating role of felt obligation. Work 2022, 71, 539–570. [Google Scholar] [CrossRef]
- Parent-Lamarche, A.; Marchand, A.; Saade, S. Does Depression Mediate the Effect of Work Organization Conditions on Job Performance? J. Occup. Environ. Med. 2020, 62, 296–302. [Google Scholar] [CrossRef]
- Khawaja, K.F.; Sarfraz, M.; Rashid, M.; Rashid, M. How is COVID-19 pandemic causing employee withdrawal behavior in the hospitality industry? An empirical investigation. J. Hosp. Tour. Insights 2022, 5, 687–706. [Google Scholar] [CrossRef]
- Gao, J.; Zheng, P.; Jia, Y.; Chen, H.; Mao, Y.; Chen, S.; Wang, Y.; Fu, H.; Dai, J. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE 2020, 15, e0231924. [Google Scholar] [CrossRef]
- Ullah, I.; Khan, K.S.; Ali, I.; Ullah, A.R.; Mukhtar, S.; de Filippis, R.; Malik, N.I.; Shalbafan, M.; Hassan, Z.; Asghar, M.S. Depression and anxiety among Pakistani healthcare workers amid COVID-19 pandemic: A qualitative study. Ann. Med. Surg. 2022, 78, 103863. [Google Scholar] [CrossRef] [PubMed]
- Khalid, A.; Ali, S. COVID-19 and its Challenges for the Healthcare System in Pakistan. Asian Bioeth. Rev. 2020, 12, 551–564. [Google Scholar] [CrossRef] [PubMed]
- Fu, S.Q.; Greco, L.M.; Lennard, A.C.; Dimotakis, N. Anxiety responses to the unfolding COVID-19 crisis: Patterns of change in the experience of prolonged exposure to stressors. J. Appl. Psychol. 2021, 106, 48–61. [Google Scholar] [CrossRef] [PubMed]
- De Clercq, D.; Azeem, M.U.; Haq, I.U. But they promised! How psychological contracts influence the impact of felt violations on job-related anxiety and performance. Pers. Rev. 2020, 50, 648–666. [Google Scholar] [CrossRef]
- Kumar, P.; Kumar, N.; Aggarwal, P.; Yeap, J.A.L. Working in lockdown: The relationship between COVID-19 induced work stressors, job performance, distress, and life satisfaction. Curr. Psychol. 2021, 40, 6308–6323. [Google Scholar] [CrossRef]
- Nadeem, F.; Sadiq, A.; Raziq, A.; Iqbal, Q.; Haider, S.; Saleem, F.; Bashaar, M. Depression, Anxiety, and Stress among Nurses During the COVID-19 Wave III: Results of a Cross-Sectional Assessment. J. Multidiscip. Health 2021, 14, 3093–3101. [Google Scholar] [CrossRef]
- Mamo, E.; Tadesse, T.; Kibret, A.; Weldeyohanes, G.; Yesuf, A.; Endazenaw, G. Burn out among Healthcare Workers (HCWs) at Middle Stage of COVID-19 Pandemic in Addis Ababa, Ethiopia: A Multicentre Cross-Sectional Study. Pathol. Lab. Med. 2022, 6, 11–22. [Google Scholar]
- Pfefferbaum, B.; North, C.S. Mental Health and the COVID-19 Pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Bradley, M.; Chahar, P. Burnout of healthcare providers during COVID-19. Cleve. Clin. J. Med. 2020. [Google Scholar] [CrossRef]
- Ahmad, S.; Yaqoob, S.; Safdar, S.; Cheema, H.A.; Islam, Z.; Iqbal, N.; Tharwani, Z.H.; Swed, S.; Ijaz, M.S.; Rehman, M.U.; et al. Burnout in health care workers during the fourth wave of COVID-19: A cross sectional study from Pakistan. Ann. Med. Surg. 2022, 80, 104326. [Google Scholar] [CrossRef]
- Zahid, N.; Syed, M.; Hersi, S.; Danish, S.H.; Ahmed, F. Assessment of Burnout in Healthcare Professionals of Pakistan Amid COVID-19—A Cross-Sectional Study. Int. J. Trop. Dis. Health 2021, 9, 34–41. [Google Scholar] [CrossRef]
- Javed, B.; Sarwer, A.; Soto, E.B.; Mashwani, Z.-R. Is Pakistan’s Response to Coronavirus (SARS-CoV-2) Adequate to Prevent an Outbreak? Front. Med. 2020, 7, 158. [Google Scholar] [CrossRef] [PubMed]
- Çelmeçe, N.; Menekay, M. The Effect of Stress, Anxiety and Burnout Levels of Healthcare Professionals Caring for COVID-19 Patients on Their Quality of Life. Front. Psychol. 2020, 11, 597624. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, M.I.; Huang, D.; Sarfraz, M.; Ivascu, L.; Riaz, A. Effects of internal service quality on nurses’ job satisfaction, commitment and performance: Mediating role of employee well-being. Nurs. Open 2021, 8, 607–619. [Google Scholar] [CrossRef] [PubMed]
- Kok, N.; van Gurp, J.; Teerenstra, S.; van der Hoeven, H.; Fuchs, M.; Hoedemaekers, C.; Zegers, M. Coronavirus Disease 2019 Immediately Increases Burnout Symptoms in ICU Professionals: A Longitudinal Cohort Study. Crit. Care Med. 2021, 49, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, M.; Asadi-Pooya, A.A.; Mousavi-Roknabadi1, R.S. Burnout among Healthcare Providers of COVID-19; a Systematic Review of Epidemiology and Recommendations. Arch. Acad. Emerg. Med. 2021, 9, e7. [Google Scholar]
- Saleem, F.; Malik, M.I.; Qureshi, S.S. Work Stress Hampering Employee Performance during COVID-19: Is Safety Culture Needed? Front. Psychol. 2021, 12, 655839. [Google Scholar] [CrossRef] [PubMed]
- Hofmeyer, A.; Taylor, R.; Kennedy, K. Fostering compassion and reducing burnout: How can health system leaders respond in the COVID-19 pandemic and beyond? Nurse Educ. Today 2020, 94, 104502. [Google Scholar] [CrossRef]
- Teo, I.; Chay, J.; Cheung, Y.B.; Sung, S.C.; Tewani, K.G.; Yeo, L.F.; Yang, G.M.; Pan, F.T.; Ng, J.Y.; Aloweni, F.A.B.; et al. Healthcare worker stress, anxiety and burnout during the COVID-19 pandemic in Singapore: A 6-month multi-centre prospective study. PLoS ONE 2021, 16, e0258866. [Google Scholar] [CrossRef]
- Naldi, A.; Vallelonga, F.; Di Liberto, A.; Cavallo, R.; Agnesone, M.; Gonella, M.; Sauta, M.D.; Lochner, P.; Tondo, G.; Bragazzi, N.L.; et al. COVID-19 pandemic-related anxiety, distress and burnout: Prevalence and associated factors in healthcare workers of North-West Italy. BJPsych Open 2021, 7, e27. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Satici, B.; Gocet-Tekin, E.; Deniz, M.E.; Satici, S.A. Adaptation of the Fear of COVID-19 Scale: Its Association with Psychological Distress and Life Satisfaction in Turkey. Int. J. Ment. Health Addict. 2021, 19, 1980–1988. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Lei, L.; Huang, X.; Zhang, S.; Yang, J.; Yang, L.; Xu, M. Comparison of Prevalence and Associated Factors of Anxiety and Depression among People Affected by versus People Unaffected by Quarantine during the COVID-19 Epidemic in Southwestern China. Med. Sci. Monit. 2020, 26, e924609-1. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.-Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879. [Google Scholar] [CrossRef]
- Vignola, R.C.B.; Tucci, A.M. Adaptation and validation of the depression, anxiety and stress scale (DASS) to Brazilian Portuguese. J. Affect. Disord. 2014, 155, 104–109. [Google Scholar] [CrossRef]
- Ninaus, K.; Diehl, S.; Terlutter, R. Employee perceptions of information and communication technologies in work life, perceived burnout, job satisfaction and the role of work-family balance. J. Bus. Res. 2021, 136, 652–666. [Google Scholar] [CrossRef]
- Sharma, P.; Devkota, G. Mental health screening questionnaire: A study on reliability and correlation with perceived stress score. J. Psychiatr. Assoc. Nepal 2019, 8, 4–8. [Google Scholar] [CrossRef]
- Ferozi, S.; Chang, Y. Transformational Leadership and its Impact on Employee Performance: Focus on Public Employees in Afghanistan. Transylv. Rev. Adm. Sci. 2021, 17, 49–68. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice for Structural Equation Modelling, 3rd ed.; Guildford Press: New York, NY, USA, 2010. [Google Scholar]
- Steiger, J.H. Structural model evaluation and modification: An interval estimation approach. Multivar. Behav. Res. 1990, 25, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Bentler, P.M.; Bonett, D.G. Significance tests and goodness of fit in the analysis of covariance structures. Psychol. Bull. 1980, 88, 588. [Google Scholar] [CrossRef]
- Bollen, K.A. Overall fit in covariance structure models: Two types of sample size effects. Psychol. Bull. 1990, 107, 256. [Google Scholar] [CrossRef]
- Tucker, L.R.; Lewis, C. A reliability coefficient for maximum likelihood factor analysis. Psychometrika 1973, 38, 1–10. [Google Scholar] [CrossRef]
- Byrne, B.M. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming; Routledge: London, UK, 2016. [Google Scholar]
- Hoyle, R.H. Evaluating measurement models in clinical research: Covariance structure analysis of latent variable models of self-conception. J. Consult. Clin. Psychol. 1991, 59, 67. [Google Scholar] [CrossRef]
- Hair, J.; Anderson, R.; Mehta, R.; Babin, B. Sales Management: Building Customer Relationships and Partnerships; Nelson Education: Toronto, ON, Canada, 2008. [Google Scholar]
- Nunnally, J.C. Psychometric Theory 3E; Tata McGraw-Hill Education: New York, NY, USA, 1994. [Google Scholar]
- Bagozzi, R.P.; Yi, Y. On the evaluation of structural equation models. J. Acad. Mark. Sci. 1988, 16, 74–94. [Google Scholar] [CrossRef]
- Kline, T. Psychological Testing: A Practical Approach to Design and Evaluation; Sage Publications: Thousand Oaks, CA, USA, 2005. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Hair, F.H., Jr.; Hult, G.T.M.; Ringle, C.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); Sage Publications: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Wong, A.K.F.; Kim, S.S.; Kim, J.; Han, H. How the COVID-19 pandemic affected hotel Employee stress: Employee perceptions of occupational stressors and their consequences. Int. J. Hosp. Manag. 2021, 93, 102798. [Google Scholar] [CrossRef]
- Hennekam, S.; Richard, S.; Grima, F. Coping with mental health conditions at work and its impact on self-perceived job performance. Empl. Relations Int. J. 2020, 42, 626–645. [Google Scholar] [CrossRef]
- Labrague, L.J.; Santos, J.A.A. COVID-19 anxiety among front-line nurses: Predictive role of organisational support, personal resilience and social support. J. Nurs. Manag. 2020, 28, 1653–1661. [Google Scholar] [CrossRef] [PubMed]
- Dyrbye, L.N.; Shanafelt, T.D.; Johnson, P.O.; Johnson, L.A.; Satele, D.; West, C.P. A cross-sectional study exploring the relationship between burnout, absenteeism, and job performance among American nurses. BMC Nurs. 2019, 18, 57. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Wang, G.; Gao, L. Modelling the Impact of Tourism on Mental Health of Chinese Residents: An Empirical Study. Discret. Dyn. Nat. Soc. 2022, 2022, 1–6. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Items | Frequency (N = 669) | (%) |
|---|---|---|
| Gender | ||
| Male | 311 | 46.5 |
| Female | 358 | 53.5 |
| Age | ||
| 19–30 | 92 | 13.8 |
| 31–40 | 182 | 27.2 |
| 41–50 | 158 | 23.6 |
| 51–60 | 141 | 21.1 |
| >60 | 96 | 14.3 |
| Education | ||
| Intermediate | 130 | 19.4 |
| Bachelor | 216 | 32.3 |
| Master | 240 | 35.9 |
| MPhil/Others | 83 | 12.4 |
| Occupation | ||
| Nurses | 310 | 46.3 |
| Doctors | 220 | 32.8 |
| Technicians | 90 | 13.4 |
| Others | 49 | 7.3 |
| Marital Status | ||
| Single | 118 | 17.6 |
| Married | 551 | 82.4 |
| Model Fit Indexes | |||||
|---|---|---|---|---|---|
| Fit Index | Cited | Fit Criteria | Results | Fit (Yes/No) | |
| X2 | 1454.113 | ||||
| DF | 1415 | ||||
| X2/DF | Kline [61] | 1.00–5.00 | 1.028 | Yes | |
| RMSEA | Steiger [62] | <0.08 | 0.006 | Yes | |
| SRMR | Hu & Bentler [63] | <0.08 | 0.0248 | Yes | |
| NFI | Bentler & G. Bonnet [64] | >0.80 | 0.935 | Yes | |
| IFI | Bollen [65] | >0.90 | 0.932 | Yes | |
| TLI | Tucker & Lewis [66] | >0.90 | 0.998 | Yes | |
| CFI | Byrne [67] | >0.90 | 0.998 | Yes | |
| GFI | Hoyle [68] | >0.90 | 0.929 | Yes | |
| Alpha, composite reliability and validity analysis | |||||
| Construct | Items | Loading | Alpha | CR | AVE |
| >0.704 | >0.7 | >0.7 | >0.5 | ||
| Depression | DEP_1 | 0.721 *** | 0.896 | 0.896 | 0.553 |
| DEP_2 | 0.739 *** | ||||
| DEP_3 | 0.753 *** | ||||
| DEP_4 | 0.745 *** | ||||
| DEP_5 | 0.753 *** | ||||
| DEP_6 | 0.749 *** | ||||
| DEP_7 | 0.744 *** | ||||
| Stress | STR_1 | 0.715 *** | 0.897 | 0.897 | 0.555 |
| STR_2 | 0.752 *** | ||||
| STR_3 | 0.753 *** | ||||
| STR_4 | 0.739 *** | ||||
| STR_5 | 0.748 *** | ||||
| STR_6 | 0.771 *** | ||||
| STR_7 | 0.739 *** | ||||
| Anxiety | ANX_1 | 0.758 *** | 0.902 | 0.902 | 0.567 |
| ANX_2 | 0.763 *** | ||||
| ANX_3 | 0.753 *** | ||||
| ANX_4 | 0.723 *** | ||||
| ANX_5 | 0.763 *** | ||||
| ANX_6 | 0.754 *** | ||||
| ANX_7 | 0.758 *** | ||||
| Job Burnout | JBO_1 | 0.746 *** | 0.773 | 0.773 | 0.532 |
| JBO_2 | 0.730 *** | ||||
| JBO_3 | 0.713 *** | ||||
| Mental Health Problems | MHP_1 | 0.725 *** | 0.945 | 0.945 | 0.533 |
| MHP_2 | 0.736 *** | ||||
| MHP_3 | 0.753 *** | ||||
| MHP_4 | 0.716 *** | ||||
| MHP_5 | 0.742 *** | ||||
| MHP_6 | 0.723 *** | ||||
| MHP_7 | 0.757 *** | ||||
| MHP_8 | 0.718 *** | ||||
| MHP_9 | 0.729 *** | ||||
| MHP_10 | 0.716 *** | ||||
| MHP_11 | 0.754 *** | ||||
| MHP_12 | 0.714 *** | ||||
| MHP_13 | 0.736 *** | ||||
| MHP_14 | 0.734 *** | ||||
| MHP_15 | 0.697 *** | ||||
| Employee Performance | EP_1 | 0.721 *** | 0.945 | 0.945 | 0.520 |
| EP_2 | 0.729 *** | ||||
| EP_3 | 0.722 *** | ||||
| EP_4 | 0.710 *** | ||||
| EP_5 | 0.742 *** | ||||
| EP_6 | 0.728 *** | ||||
| EP_7 | 0.726 *** | ||||
| EP_8 | 0.726 *** | ||||
| EP_9 | 0.709 *** | ||||
| EP_10 | 0.718 *** | ||||
| EP_11 | 0.708 *** | ||||
| EP_12 | 0.737 *** | ||||
| EP_13 | 0.709 *** | ||||
| EP_14 | 0.692 *** | ||||
| EP_15 | 0.730 *** | ||||
| EP_16 | 0.725 *** | ||||
| Constructs | Mean | SD | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|---|
| 1. Depression | 3.59 | 0.839 | 0.743 | 0.598 | 0.586 | 0.668 | 0.632 | 0.557 |
| 2. Stress | 3.60 | 0.847 | 0.598 | 0.745 | 0.599 | 0.655 | 0.637 | 0.584 |
| 3. Anxiety | 3.60 | 0.849 | 0.586 | 0.601 | 0.753 | 0.636 | 0.656 | 0.555 |
| 4. Job Burnout | 3.62 | 0.886 | 0.666 | 0.653 | 0.636 | 0.730 | 0.681 | 0.587 |
| 5. Mental Health Problems | 3.63 | 0.785 | 0.633 | 0.638 | 0.656 | 0.681 | 0.730 | 0.603 |
| 6. Employee Performance | 3.65 | 0.608 | −0.557 | −0.584 | −0.553 | −0.587 | −0.601 | 0.721 |
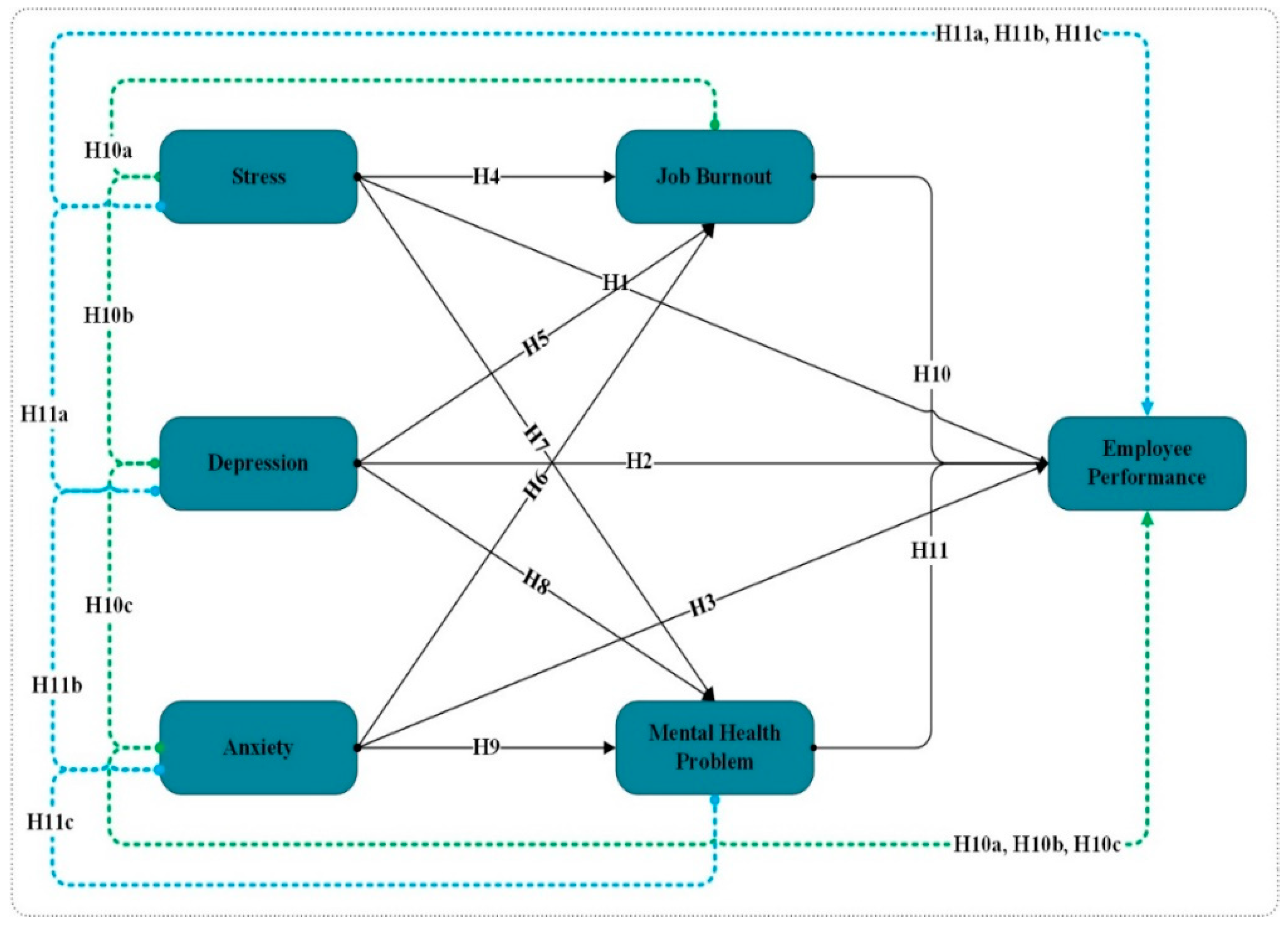
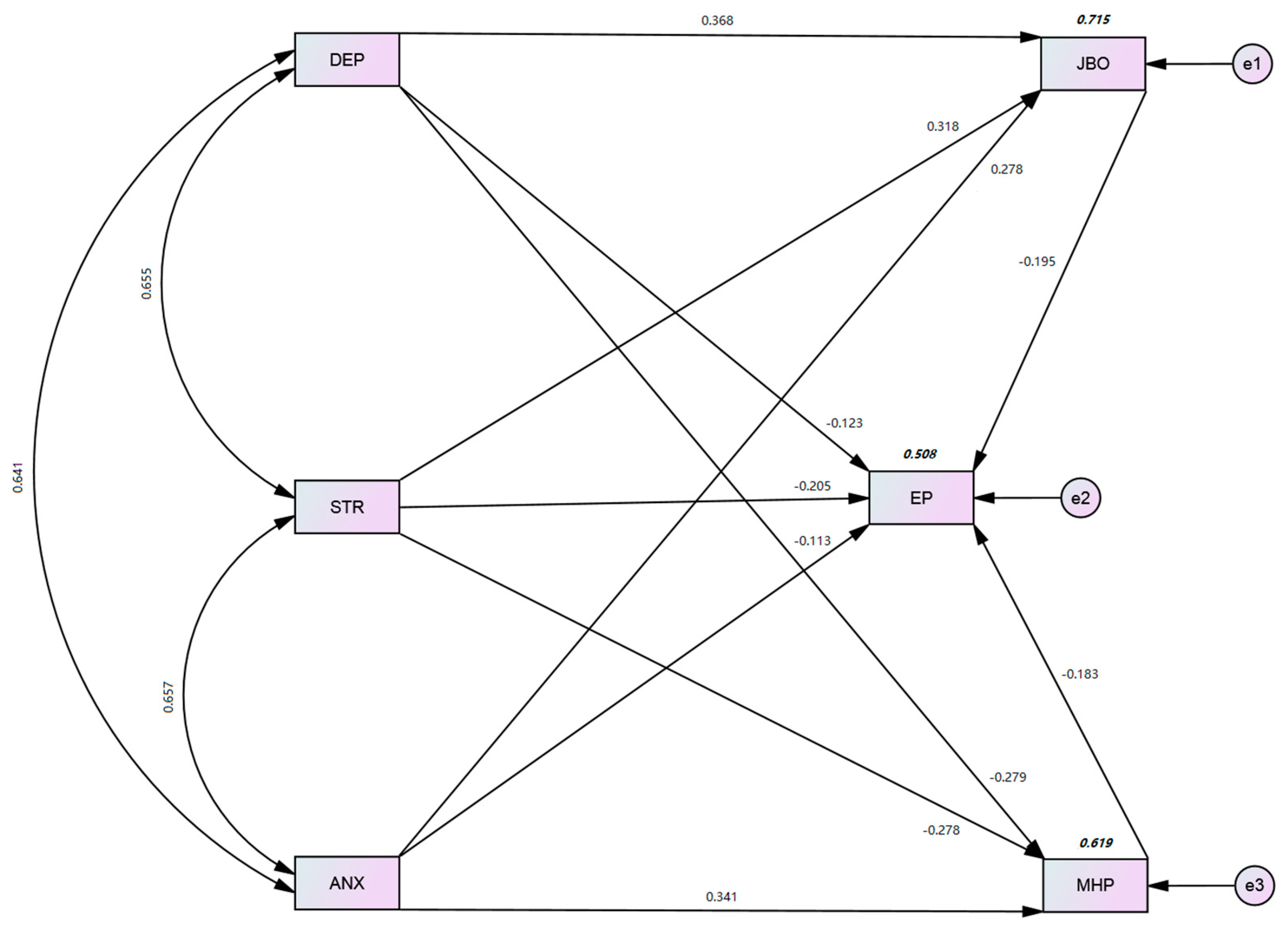
| Hypothesis | Direct | Std. | Std. | T | p |
|---|---|---|---|---|---|
| Relationships | Beta | Error | Values | Values | |
| H1 | STR 🡺 EP | −0.205 | 0.037 | −5.541 | *** |
| H2 | DEP 🡺 EP | −0.123 | 0.041 | −3.000 | ** |
| H3 | ANX 🡺 EP | −0.113 | 0.039 | −2.897 | * |
| H4 | STR 🡺 JBO | 0.318 | 0.032 | 9.938 | *** |
| H5 | DEP 🡺 JBO | 0.368 | 0.031 | 11.871 | *** |
| H6 | ANX 🡺 JBO | 0.278 | 0.031 | 8.968 | *** |
| H7 | STR 🡺 MHP | 0.278 | 0.040 | 6.950 | *** |
| H8 | DEP 🡺 MHP | 0.279 | 0.037 | 7.541 | *** |
| H9 | ANX 🡺 MHP | 0.341 | 0.038 | 8.974 | *** |
| H10 | JBO 🡺 EP | −0.195 | 0.050 | −3.900 | *** |
| H11 | MHP 🡺 EP | −0.183 | 0.053 | −3.453 | *** |
| Hypothesis | Indirect | Std. | Lower | Upper | p |
|---|---|---|---|---|---|
| Relationships | Beta | Limit | Limit | Values | |
| H10a | STR 🡺 JBO 🡺 EP | −0.062 | −0.058 | −0.019 | *** |
| H10b | DEP 🡺 JBO 🡺 EP | −0.072 | −0.077 | −0.031 | ** |
| H10c | ANX 🡺 JBO 🡺 EP | −0.054 | −0.059 | −0.020 | *** |
| H11a | STR 🡺 MHP 🡺 EP | −0.051 | −0.068 | −0.027 | ** |
| H11b | DEP 🡺 MHP 🡺 EP | −0.051 | −0.058 | −0.022 | ** |
| H11c | ANX 🡺 MHP 🡺 EP | −0.063 | −0.071 | −0.021 | ** |
| Latent Variables | R2 |
|---|---|
| MHP | 0.619 |
| JBO | 0.715 |
| EP | 0.508 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, J.; Sarfraz, M.; Ivascu, L.; Iqbal, K.; Mansoor, A. How Did Work-Related Depression, Anxiety, and Stress Hamper Healthcare Employee Performance during COVID-19? The Mediating Role of Job Burnout and Mental Health. Int. J. Environ. Res. Public Health 2022, 19, 10359. https://doi.org/10.3390/ijerph191610359
Sun J, Sarfraz M, Ivascu L, Iqbal K, Mansoor A. How Did Work-Related Depression, Anxiety, and Stress Hamper Healthcare Employee Performance during COVID-19? The Mediating Role of Job Burnout and Mental Health. International Journal of Environmental Research and Public Health. 2022; 19(16):10359. https://doi.org/10.3390/ijerph191610359
Chicago/Turabian StyleSun, Jianmin, Muddassar Sarfraz, Larisa Ivascu, Kashif Iqbal, and Athar Mansoor. 2022. "How Did Work-Related Depression, Anxiety, and Stress Hamper Healthcare Employee Performance during COVID-19? The Mediating Role of Job Burnout and Mental Health" International Journal of Environmental Research and Public Health 19, no. 16: 10359. https://doi.org/10.3390/ijerph191610359