Epidemiology of and Risk Factors for COVID-19 Infection among Health Care Workers: A Multi-Centre Comparative Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Case Definition of COVID-19
2.3. Statistical Analysis
3. Results
3.1. General Characteristics of HCW and Non-HCW Cases
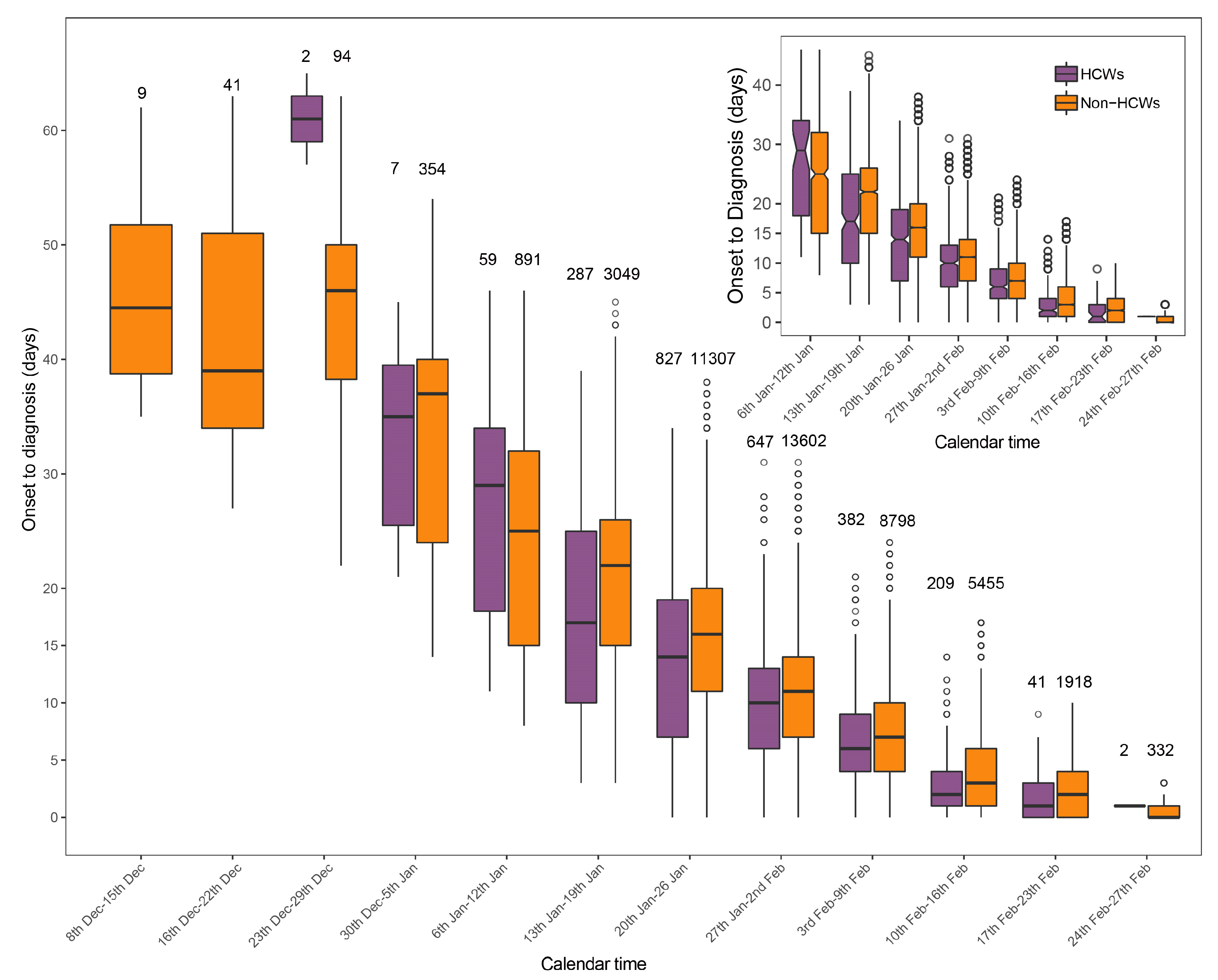
3.2. Time from Symptom Onset to Diagnosis of HCW and Non-HCW Cases
3.3. Spatial-Temporal Distributions of HCW and Non-HCW Cases
3.4. Risk Factors of HCWs for Infection and Deterioration
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Rolling updates on coronavirus disease (COVID-19). 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 29 September 2020).
- Stoye, E. The pandemic in pictures: How coronavirus is changing the world. Nature 2020. Available online: https://pubmed.ncbi.nlm.nih.gov/32265538/ (accessed on 29 September 2020). [CrossRef]
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 29 September 2020).
- The Lancet. COVID-19: Protecting health-care workers. Lancet 2020, 395, 922. [Google Scholar] [CrossRef]
- The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The Epidemiological Characteristics of an Outbreak of 2019 Novel Coronavirus Diseases (COVID-19) in China. Chin. J. Epidemiol. 2020, 41, 145–151. (In Chinese) [Google Scholar]
- Black, J.R.M.; Bailey, C.; Przewrocka, J.; Dijkstra, K.K.; Swanton, C. COVID-19: The case for health-care worker screening to prevent hospital transmission. Lancet 2020, 395, 1418–1420. [Google Scholar] [CrossRef]
- Chou, R.; Dana, T.; Buckley, D.I.; Selph, S.; Fu, R.; Totten, A.M. Update Alert: Epidemiology of and Risk Factors for Coronavirus Infection in Health Care Workers. Ann. Intern. Med. 2020, 173, W46–W47. [Google Scholar] [CrossRef]
- Kulldorff, M.; Heffernan, R.; Hartman, J.; Assunção, R.; Mostashari, F. A space-time permutation scan statistic for disease outbreak detection. PLoS Med. 2005, 2, 0216–0224. [Google Scholar] [CrossRef] [Green Version]
- Vimercati, L.; Dell’Erba, A.; Migliore, G.; De Maria, L.; Caputi, A.; Quarato, M.; Mansi, F. Prevention and protection measures of healthcare workers exposed to SARS-CoV-2 in a university hospital in Bari, Apulia, Southern Italy. J. Hosp. Infect. 2020, 105, 454–458. [Google Scholar] [CrossRef]
- Zheng, L.; Wang, X.; Zhou, C.; Liu, Q.; Li, S.; Sun, Q.; Wang, W. Analysis of the infection status of the health care workers in Wuhan during the COVID-19 outbreak: A cross-sectional study. Clin. Infect. Dis. 2020, 15, ciaa588. [Google Scholar] [CrossRef]
- Treibel, T.A.; Manisty, C.; Burton, M.; McKnight, Á.; Lambourne, J.; Augusto, J.B.; Couto-Parada, X.; Cutino-Moguel, T.; Noursadeghi, M.; Moon, J.C. COVID-19: PCR screening of asymptomatic health-care workers at London hospital. Lancet 2020, 395, 1608–1610. [Google Scholar] [CrossRef]
- Clemency, B.M.; Varughese, R.; Scheafer, D.K.; Ludwig, B.; Welch, J.B.; McCormack, R.F.; Ma, X.; Nan, N.; Giambra, T.; Raab, T. Symptom Criteria for COVID-19 Testing of Heath Care Workers. Acad. Emerg. Med. 2020, 27, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Hsin, D.H.C.; Macer, D.R.J. Heroes of SARS: Professional roles and ethics of health care workers. J. Infect. 2004, 49, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Lai, X.; Wang, M.; Qin, C.; Tan, L.; Ran, L.; Chen, D.; Zhang, H.; Shank, K.; Xia, C.; Shaokang, W.; et al. Coronavirus Disease 2019 (COVID-2019) Infection Among Health Care Workers and Implications for Prevention Measures in a Tertiary Hospital in Wuhan, China. JAMA Netw. Open 2020, 3, e209666. [Google Scholar] [CrossRef] [PubMed]
- Yen, M.-Y.; Lin, Y.E.; Su, I.-J.; Huang, F.-Y.; Ho, M.-S.; Chang, S.-C.; Tan, K.-H.; Chen, K.-T.; Chang, H.; Liu, Y.-C.; et al. Using an integrated infection control strategy during outbreak control to minimize nosocomial infection of severe acute respiratory syndrome among healthcare workers. J. Hosp. Infect. 2006, 62, 195–199. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.-Q.; Ling, W.-H.; Lu, C.-Y.; Hao, Y.-T.; Lin, Z.-N.; Huang, J.; Li, G.; Yan, G.-M. Which preventive measures might protect health care workers from SARS? BMC Public Health 2009, 9, 81. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, M.G.; Bach, H.A.; Vu, H.T.; Montgomery, J.M.; Bausch, D.G.; Shah, J.J.; Maloney, S.; Leitmeyer, K.C.; Huy, V.Q.; Horby, P.; et al. Factors associated with nosocomial SARS-CoV transmission among healthcare workers in Hanoi, Vietnam, 2003. BMC Public Health 2006, 6, 207. [Google Scholar] [CrossRef] [Green Version]
- Pan, F.; Ye, T.; Sun, P. Time course of lung changes at chest CT during recovery from Coronavirus disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Song, F.; Shi, N.; Shan, F.; Zhang, Z.; Shen, J.; Lu, H.; Ling, Y.; Jiang, Y.; Shi, Y. Emerging 2019 novel coronavirus (2019-NCoV) pneumonia. Radiology 2020, 295, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Ran, L.; Chen, X.; Wang, Y.; Wu, W.; Zhang, L.; Tan, X. Risk Factors of Healthcare Workers with Corona Virus Disease 2019: A Retrospective Cohort Study in a Designated Hospital of Wuhan in China. Clin. Infect. Dis. 2020, ciaa287. [Google Scholar] [CrossRef] [Green Version]
- Pan, A.; Liu, L.; Wang, C.; Guo, H.; Hao, X.; Wang, Q.; Huang, J.; He, N.; Yu, H.; Lin, X.; et al. Association of Public Health Interventions with the Epidemiology of the COVID-19 Outbreak in Wuhan, China. JAMA J. Am. Med. Assoc. 2020, 323, 1915–1923. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H. Early lessons from the frontline of the 2019-nCoV outbreak. Lancet 2020, 395, 687. [Google Scholar] [CrossRef] [Green Version]
- Weaver, M.D.; Landrigan, C.P.; Sullivan, J.P.; O’Brien, C.S.; Quadri, S.; Viyaran, N.; Wang, W.; Vetter, C.; Czeisler, C.; Barger, L.K. The Association Between Resident Physician Work-Hour Regulations and Physician Safety and Health. Am. J. Med. 2020, 133. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| HCWs | Non-HCWs | p-Value | |
|---|---|---|---|
| Demographic characteristics | |||
| Male | 703 | 22326 | <0.001 a,* |
| Female | 1760 | 23524 | |
| Female (%) | 71.5 | 51.3 | |
| Age (median [IQR]) | 36 (29, 44) | 56 (44, 66) | <0.001 b,* |
| Days from onset to diagnosis (median [IQR]) | 10 (5, 16) | 10 (5, 16) | 0.68 b |
| Infection status | |||
| Non-infected individual | 107126 | 10925561 | <0.001 a,* |
| Infected individual | 2463 | 45850 | |
| AR (per million people) | 22475 | 4179 | |
| Severity status | |||
| Mild or moderate case | 2053 | 36850 | <0.001 a,* |
| Severe or critical case | 410 | 9000 | |
| PSCC (%) | 16.6 | 19.6 | |
| Death status | |||
| Non-death case | 2454 | 43426 | <0.001 a,* |
| Death case | 9 | 2424 | |
| CFR (%) | 0.4 | 5.3 |
| Hospital | 23th December–29th December | 30th December–5th January | 6th January–12th January | 13th January–19th January | 20th January–26th January | 27th January–2nd February | 3rd February–9th February | 10th February–16th February | 17th February–23th February | Total Attack Rate |
|---|---|---|---|---|---|---|---|---|---|---|
| Hospital1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Hospital2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Hospital3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Hospital4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Hospital5 | 0 | 0 | 0 | 419 | 419 | 0 | 0 | 419 | 419 | 1678 |
| Hospital6 | 0 | 0 | 0 | 0 | 0 | 0 | 3788 | 0 | 0 | 3788 |
| Hospital7 | 0 | 0 | 238 | 0 | 714 | 714 | 476 | 3094 | 0 | 5236 |
| Hospital8 | 485 | 0 | 0 | 0 | 970 | 1940 | 1940 | 0 | 0 | 5335 |
| Hospital9 | 0 | 0 | 0 | 0 | 0 | 0 | 3394 | 3394 | 0 | 6788 |
| Hospital10 | 0 | 0 | 0 | 0 | 3250 | 1625 | 1083 | 1083 | 542 | 7584 |
| Hospital11 | 0 | 136 | 136 | 544 | 1495 | 3942 | 1631 | 136 | 0 | 8021 |
| Hospital12 | 0 | 0 | 516 | 2581 | 3614 | 1033 | 516 | 0 | 0 | 8260 |
| Hospital13 | 0 | 0 | 0 | 2188 | 2188 | 4376 | 0 | 0 | 0 | 8753 |
| Hospital14 | 0 | 0 | 649 | 649 | 5191 | 1298 | 1947 | 1298 | 1298 | 12330 |
| Hospital15 | 0 | 0 | 0 | 0 | 1810 | 3620 | 3620 | 4525 | 0 | 13575 |
| Hospital16 | 0 | 0 | 0 | 0 | 4000 | 8000 | 0 | 4000 | 0 | 16000 |
| Hospital17 | 0 | 0 | 1297 | 0 | 9079 | 3891 | 1297 | 1297 | 0 | 16861 |
| Hospital18 | 0 | 0 | 0 | 804 | 804 | 1608 | 6431 | 5627 | 1608 | 16881 |
| Hospital19 | 0 | 0 | 0 | 1319 | 1319 | 3958 | 5277 | 3958 | 2639 | 18470 |
| Hospital20 | 0 | 0 | 1104 | 4415 | 4415 | 11038 | 0 | 0 | 0 | 20971 |
| Hospital21 | 0 | 0 | 0 | 2854 | 8563 | 13321 | 3806 | 951 | 0 | 29496 |
| Hospital22 | 0 | 0 | 158 | 6480 | 11222 | 7903 | 1739 | 1739 | 316 | 29556 |
| Hospital23 | 0 | 632 | 632 | 6321 | 10746 | 6953 | 1580 | 5373 | 316 | 32554 |
| Hospital24 | 0 | 0 | 0 | 3155 | 14196 | 11041 | 6309 | 0 | 0 | 34700 |
| Hospital25 | 0 | 0 | 0 | 7022 | 5618 | 11236 | 5618 | 8427 | 0 | 37921 |
| Hospital26 | 0 | 2320 | 8121 | 8121 | 15081 | 1160 | 3480 | 1160 | 0 | 39443 |
| Hospital27 | 0 | 950 | 1899 | 9497 | 15195 | 8547 | 2849 | 950 | 0 | 39886 |
| Hospital28 | 0 | 0 | 0 | 4773 | 14320 | 9547 | 7160 | 4773 | 0 | 40573 |
| Hospital29 | 0 | 0 | 0 | 984 | 11811 | 9843 | 14764 | 2953 | 984 | 41339 |
| Hospital30 | 0 | 0 | 0 | 0 | 14837 | 17804 | 4451 | 2967 | 1484 | 41543 |
| Hospital31 | 0 | 0 | 831 | 7060 | 18688 | 13704 | 2492 | 415 | 0 | 43189 |
| Hospital32 | 343 | 0 | 1029 | 5489 | 19897 | 11321 | 3774 | 1372 | 0 | 43225 |
| Hospital33 | 0 | 0 | 774 | 14706 | 13158 | 16254 | 13158 | 4644 | 774 | 63467 |
| Hospital34 | 0 | 0 | 753 | 3765 | 26355 | 23343 | 17319 | 4518 | 0 | 76054 |
| Hospital35 | 0 | 0 | 0 | 1692 | 43993 | 38917 | 6768 | 8460 | 1692 | 101523 |
| Hospital36 | 0 | 0 | 6127 | 8578 | 22059 | 37990 | 18382 | 20833 | 4902 | 118873 |
| RR (95% CI) | p-Value | |
|---|---|---|
| Having fever clinic | ||
| No | Ref | Ref |
| Yes | 1.00 (0.97–1.03) | 0.91 |
| Level of hospital | ||
| Provincial | Ref | Ref |
| Municipal | 0.99 (0.97–1.02) | 0.65 |
| County-level | 1.04 (1.01–1.07) | 0.02 * |
| Type of hospital | ||
| Special | Ref | Ref |
| General | 1.02 (0.99–1.06) | 0.11 |
| Chinese medical | 1.01 (0.97–1.06) | 0.59 |
| Nurse/bed ratio | 1.00 (0.98–1.01) | 0.63 |
| The county where hospital was located | ||
| Xinzhou | Ref | Ref |
| Huangpi | 1.01 (0.94–1.08) | 0.79 |
| Jiangxia | 1.01 (0.95–1.08) | 0.67 |
| Caidian | 1.02 (0.95–1.09) | 0.56 |
| Hannan | 1.02 (0.95–1.09) | 0.63 |
| Dongxihu | 1.03 (0.96–1.10) | 0.36 |
| Hongshan | 1.08 (1.02–1.14) | 0.01 * |
| Qingshan | 1.04 (0.98–1.11) | 0.14 |
| Wuchang | 1.08 (1.03–1.14) | 0.01 * |
| Qiaokou | 1.07 (0.99–1.16) | 0.08 |
| Hanyang | 1.08 (1.01–1.15) | 0.03 * |
| Jiang’an | 1.10 (1.03–1.16) | 0.003 * |
| Jianghan | 1.07 (1.00–1.16) | 0.06 |
| Risk Factors | Crude Data | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|---|
| Mild and Moderate Cases | Severe and Critical Cases | OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value | |
| Age | 33 (29, 42) a | 37 (30, 45) a | 1.02 (0.99–1.05) | 0.17 | Removed c | NA |
| Sex | ||||||
| Female | 188 (74.6) b | 27 (58.7) b | Ref | Ref | Ref | Ref |
| Male | 64 (25.4) b | 19 (41.3) b | 2.07 (1.07–3.95) | 0.03 * | 1.88 (0.92–3.77) | 0.08 |
| Days from symptom onset to diagnosis | 7 (2, 13) a | 7 (5, 11) a | 1.01 (0.97–1.05) | 0.78 | Removed c | NA |
| Department | ||||||
| Infection department | 171 (67.9) b | 15 (32.6) b | Ref | Ref | Ref | Ref |
| General department | 45 (17.9) b | 11 (23.9) b | 2.79 (1.17–6.46) | 0.02 * | 2.86 (1.20–6.66) | 0.02 * |
| Ophthalmology department | 30 (11.9) b | 13 (28.3) b | 4.94 (2.12–11.47) | <0.001 * | 4.45 (1.88–10.44) | 0.001 * |
| Respiratory department | 6 (2.4) b | 7 (15.2) b | 13.30 (3.96–46.50) | <0.001 * | 13.35 (3.93–47.23) | <0.001 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, J.-T.; Liu, Z.-D.; Fan, Z.-W.; Zhao, L.; Cao, W.-C. Epidemiology of and Risk Factors for COVID-19 Infection among Health Care Workers: A Multi-Centre Comparative Study. Int. J. Environ. Res. Public Health 2020, 17, 7149. https://doi.org/10.3390/ijerph17197149
Wei J-T, Liu Z-D, Fan Z-W, Zhao L, Cao W-C. Epidemiology of and Risk Factors for COVID-19 Infection among Health Care Workers: A Multi-Centre Comparative Study. International Journal of Environmental Research and Public Health. 2020; 17(19):7149. https://doi.org/10.3390/ijerph17197149
Chicago/Turabian StyleWei, Jia-Te, Zhi-Dong Liu, Zheng-Wei Fan, Lin Zhao, and Wu-Chun Cao. 2020. "Epidemiology of and Risk Factors for COVID-19 Infection among Health Care Workers: A Multi-Centre Comparative Study" International Journal of Environmental Research and Public Health 17, no. 19: 7149. https://doi.org/10.3390/ijerph17197149