
The Risk of Spontaneous Abortion Does Not Increase Following First Trimester mRNA COVID-19 Vaccination

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jachowicz, E.; Gębicka, M.; Plakhtyr, D.; Shynkarenko, M.; Urbanowicz, J.; Mach, M.; Czepiel, J.; Marchewka, J.; Wójkowska-Mach, J. Incidence of Vaccine-Preventable Childhood Diseases in the European Union and in the European Free Trade Association Countries. Vaccines 2021, 9, 796. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Filia, A.; Rota, M.C.; Croci, R.; Bellini, L.; Odone, A.; Signorelli, C. Vaccine Procurement: A Conceptual Framework Based on Literature Review. Vaccines 2021, 9, 1434. [Google Scholar] [CrossRef] [PubMed]
- Cadeddu, C.; Sapienza, M.; Castagna, C.; Regazzi, L.; Paladini, A.; Ricciardi, W.; Rosano, A. Vaccine Hesitancy and Trust in the Scientific Community in Italy: Comparative Analysis from Two Recent Surveys. Vaccines 2021, 9, 1206. [Google Scholar] [CrossRef] [PubMed]
- Dri, D.A.; Praticò, G.; Gaucci, E.; Marianecci, C.; Gramaglia, D. Quality Assessment of Investigational Medicinal Products in COVID-19 Clinical Trials: One Year of Activity at the Clinical Trials Office. Pharmaceuticals 2021, 14, 1321. [Google Scholar] [CrossRef] [PubMed]
- Syundyukov, E.; Mednis, M.; Zaharenko, L.; Pildegovica, E.; Danovska, I.; Kistkins, S.; Seidmann, A.; Benis, A.; Pirags, V.; Tzivian, L. Data-Driven Decision Making and Proactive Citizen-Scientist Communication: A Cross-Sectional Study on COVID-19 Vaccination Adherence. Vaccines 2021, 9, 1384. [Google Scholar] [CrossRef]
- Simionescu, A.A.; Streinu-Cercel, A.; Popescu, F.-D.; Stanescu, A.M.A.; Vieru, M.; Danciu, B.M.; Miron, V.D.; Săndulescu, O. Comprehensive Overview of Vaccination during Pregnancy in Europe. J. Pers. Med. 2021, 11, 1196. [Google Scholar] [CrossRef]
- Gorun, F.; Motoi, S.; Malita, D.; Navolan, D.B.; Nemescu, D.; Olariu, T.R.; Craina, M.; Vilibic-Cavlek, T.; Ciohat, I.; Boda, D.; et al. Cytomegalovirus seroprevalence in pregnant women in the western region of Romania: A large-scale study. Exp. Ther. Med. 2020, 20, 2439–2443. [Google Scholar] [CrossRef]
- Siminel, M.A.; Neamtu, C.O.; Ditescu, D.; Fortofoiu, M.C.; Comanescu, A.C.; Novac, M.B.; Neamtu, S.D.; Gluhovschi, A. Apert syn-drome—Clinical case. Rom. J. Morphol. Embryol. 2017, 58, 277–280. [Google Scholar]
- Mazziotta, C.; Pellielo, G.; Tognon, M.; Martini, F.; Rotondo, J.C. Significantly Low Levels of IgG Antibodies Against Oncogenic Merkel Cell Polyomavirus in Sera From Females Affected by Spontaneous Abortion. Front. Microbiol. 2021, 12. [Google Scholar] [CrossRef]
- Mauro, M.A.L.; Aliverti, A. Respiratory physiology of pregnancy. Breathe 2015, 11, 297–301. [Google Scholar] [CrossRef] [Green Version]
- Marincu, I.; Bratosin, F.; Vidican, I.; Bostanaru, A.-C.; Frent, S.; Cerbu, B.; Turaiche, M.; Tirnea, L.; Timircan, M. Predictive Value of Comorbid Conditions for COVID-19 Mortality. J. Clin. Med. 2021, 10, 2652. [Google Scholar] [CrossRef] [PubMed]
- Socolov, R.; Akad, M.; Păvăleanu, M.; Popovici, D.; Ciuhodaru, M.; Covali, R.; Akad, F.; Păvăleanu, I. The Rare Case of a COVID-19 Pregnant Patient with Quadruplets and Postpartum Severe Pneumonia. Case Report and Review of the Literature. Medicina 2021, 57, 1186. [Google Scholar] [CrossRef] [PubMed]
- Di Toro, F.; Gjoka, M.; Di Lorenzo, G.; De Santo, D.; De Seta, F.; Maso, G.; Risso, F.M.; Romano, F.; Wiesenfeld, U.; Levi-D’Ancona, R.; et al. Impact of COVID-19 on maternal and neonatal outcomes: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Celewicz, A.; Celewicz, M.; Michalczyk, M.; Woźniakowska-Gondek, P.; Krejczy, K.; Misiek, M.; Rzepka, R. Pregnancy as a Risk Factor of Severe COVID-19. J. Clin. Med. 2021, 10, 5458. [Google Scholar] [CrossRef]
- Chmielewska, B.; Barratt, I.; Townsend, R.; Kalafat, E.; van der Meulen, J.; Gurol-Urganci, I.; O’Brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; et al. Effects of the COVID-19 pandemic on maternal and perinatal outcomes: A systematic review and meta-analysis. Lancet Glob. Health 2021, 9, e759–e772. [Google Scholar] [CrossRef]
- Musa, S.S.; Bello, U.M.; Zhao, S.; Abdullahi, Z.U.; Lawan, M.A.; He, D. Vertical Transmission of SARS-CoV-2: A Systematic Review of Systematic Reviews. Viruses 2021, 13, 1877. [Google Scholar] [CrossRef]
- Citu, C.; Neamtu, R.; Sorop, V.-B.; Horhat, D.I.; Gorun, F.; Tudorache, E.; Gorun, O.M.; Boarta, A.; Tuta-Sas, I.; Citu, I.M. Assessing SARS-CoV-2 Vertical Transmission and Neonatal Complications. J. Clin. Med. 2021, 10, 5253. [Google Scholar] [CrossRef]
- Principi, N.; Esposito, S. Is the Immunization of Pregnant Women against COVID-19 Justified? Vaccines 2021, 9, 970. [Google Scholar] [CrossRef]
- Male, V. Are COVID-19 vaccines safe in pregnancy? Nat. Rev. Immunol. 2021, 21, 200–201. [Google Scholar] [CrossRef]
- Swamy, G.K.; Heine, R.P. Vaccinations for Pregnant Women. Obstet. Gynecol. 2015, 125, 212–226. [Google Scholar] [CrossRef]
- Mackin, D.W.; Walker, S.P. The historical aspects of vaccination in pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2021, 76, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Cavaliere, A.F.; Zaami, S.; Pallottini, M.; Perelli, F.; Vidiri, A.; Marinelli, E.; Straface, G.; Signore, F.; Scambia, G.; Marchi, L. Flu and Tdap Maternal Immunization Hesitancy in Times of COVID-19: An Italian Survey on Multiethnic Sample. Vaccines 2021, 9, 1107. [Google Scholar] [CrossRef] [PubMed]
- Fouda, G.G.; Martinez, D.R.; Swamy, G.K.; Permar, S.R. The Impact of IgG Transplacental Transfer on Early Life Immunity. ImmunoHorizons 2018, 2, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Kalampokas, T.; Rapani, A.; Papageorgiou, M.; Grigoriadis, S.; Maziotis, E.; Anifandis, G.; Triantafyllidou, O.; Tzanakaki, D.; Neofytou, S.; Bakas, P.; et al. The Current Evidence Regarding COVID-19 and Pregnancy: Where Are We Now and Where Should We Head to Next? Viruses 2021, 13, 2000. [Google Scholar] [CrossRef]
- World Health Organization. Update on WHO Interim Recommendations on COVID-19 Vaccination of Pregnant and Lactating Women—Updated 10 June 2021. Available online: https://www.who.int/publications/m/item/update-on-who-interim-recommendations-on-COVID-19-vaccination-of-pregnant-and-lactating-women (accessed on 10 December 2021).
- Cohain, J.S.; Buxbaum, R.E.; Mankuta, D. Spontaneous first trimester miscarriage rates per woman among parous women with 1 or more pregnancies of 24 weeks or more. BMC Pregnancy Childbirth 2017, 17, 437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trostle, M.E.; Limaye, M.A.; Avtushka, M.V.; Lighter, J.L.; Penfield, C.A.; Roman, A.S. COVID-19 vaccination in pregnancy: Early experience from a single institution. Am. J. Obstet. Gynecol. MFM 2021, 3, 100464. [Google Scholar] [CrossRef]
- Moradinazar, M.; Najafi, F.; Nazar, Z.M.; Hamzeh, B.; Pasdar, Y.; Shakiba, E. Lifetime Prevalence of Abortion and Risk Factors in Women: Evidence from a Cohort Study. J. Pregnancy 2020, 2020, 1–8. [Google Scholar] [CrossRef]
- Citu, I.M.; Citu, C.; Gorun, F.; Motoc, A.; Gorun, O.M.; Burlea, B.; Bratosin, F.; Tudorache, E.; Margan, M.-M.; Hosin, S.; et al. Determinants of COVID-19 Vaccination Hesitancy among Romanian Pregnant Women. Vaccines 2022, 10, 275. [Google Scholar] [CrossRef]
- Shimabukuro, T.T.; Kim, S.Y.; Myers, T.R.; Moro, P.L.; Oduyebo, T.; Panagiotakopoulos, L.; Marquez, P.L.; Olson, C.K.; Liu, R.; Chang, K.T.; et al. Preliminary findings of mRNA COVID-19 vaccine safety in pregnant persons. N. Engl. J. Med. 2021, 384, 2273–2282. [Google Scholar] [CrossRef]
- Panagiotakopoulos, L.; McCarthy, N.L.; Tepper, N.K.; Kharbanda, E.O.; Lipkind, H.S.; Vazquez-Benitez, G.; McClure, D.L.; Greenberg, V.; Getahun, D.; Glanz, J.M.; et al. Evaluating the Association of Stillbirths After Maternal Vaccination in the Vaccine Safety Datalink. Obstet. Gynecol. 2020, 136, 1086–1094. [Google Scholar] [CrossRef]
- Hu, X.; Miao, M.; Bai, Y.; Cheng, N.; Ren, X. Reproductive Factors and Risk of Spontaneous Abortion in the Jinchang Cohort. Int. J. Environ. Res. Public Health 2018, 15, 2444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pratama, N.R.; Wafa, I.A.; Budi, D.S.; Putra, M.; Wardhana, M.P.; Wungu, C.D.K. mRNA COVID-19 vaccines in pregnancy: A systematic review. PLoS ONE 2022, 17, e0261350. [Google Scholar] [CrossRef] [PubMed]
- Tognon, M.; Tagliapietra, A.; Magagnoli, F.; Mazziotta, C.; Oton-Gonzalez, L.; Lanzillotti, C.; Vesce, F.; Contini, C.; Rotondo, J.C.; Martini, F. Investigation on Spontaneous Abortion and Human Papillomavirus Infection. Vaccines 2020, 8, 473. [Google Scholar] [CrossRef] [PubMed]
- Zauche, L.H.; Wallace, B.; Smoots, A.N.; Olson, C.K.; Oduyebo, T.; Kim, S.Y.; Petersen, E.E.; Ju, J.; Beauregard, J.; Wilcox, A.J.; et al. Receipt of mRNA COVID-19 Vaccines and Risk of Spontaneous Abortion. N. Engl. J. Med. 2021, 385, 1533–1535. [Google Scholar] [CrossRef] [PubMed]
- Kharbanda, E.O.; Haapala, J.; DeSilva, M.; Vazquez-Benitez, G.; Vesco, K.K.; Naleway, A.L.; Lipkind, H.S. Spontaneous Abortion Following COVID-19 Vaccination During Pregnancy. JAMA 2021, 326, 1629–1631. [Google Scholar] [CrossRef]
- Magnus, M.C.; Gjessing, H.K.; Eide, H.N.; Wilcox, A.J.; Fell, D.B.; Håberg, S.E. COVID-19 Vaccination during Pregnancy and First-Trimester Miscarriage. N. Engl. J. Med. 2021, 385, 2008–2010. [Google Scholar] [CrossRef]
- FDA. Vaccines and Related Biological Products Advisory Committee December 17, 2020 Meeting Announcement. 2020. Available online: https://www.fda.gov/advisory-committees/advisory-committee-calendar/vaccines-and-related-biological-products-advisory-committee-december-17-2020-meeting-announcement (accessed on 10 December 2021).
- BioNTech. Pfizer and Biontech Commence Global Clinical Trial to Evaluate COVID-19 Vaccine in Pregnant Women. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-commence-global-clinical-trial-evaluate (accessed on 15 January 2022).
- Garg, I.; Shekhar, R.; Sheikh, A.; Pal, S. COVID-19 Vaccine in Pregnant and Lactating Women: A Review of Existing Evidence and Practice Guidelines. Infect. Dis. Rep. 2021, 13, 685–699. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables * | Total (n = 3094) | Vaccine (n = 927) | No Vaccine (n = 2167) | p-Value |
|---|---|---|---|---|
| Age, years (mean ± SD) | 30.7 ± 6.1 | 29.5 ± 7.3 | 31.6 ± 5.6 | <0.001 t |
| Weight, BMI (mean ± SD) | 23.9 ± 5.4 | 24.1 ± 5.2 | 23.8 ± 5.4 | 0.152 t |
| Previous SARS-CoV-2 infection | 341 (11.0%) | 148 (15.9%) | 193 (8.9%) | <0.001 |
| Nulliparous | 1973 (63.8%) | 584 (62.9%) | 1389 (64.1%) | 0.560 |
| Infertility treatment | 106 (3.4%) | 30 (3.2%) | 76 (3.5%) | 0.704 |
| Spontaneous abortion | 395 (12.8%) | 124 (13.4%) | 271 (12.5%) | 0.506 |
| Abnormal karyotype | 30 (0.9%) | 11 (1.2%) | 19 (0.9%) | 0.420 |
| Pregnancy complications ** | 229 (7.4%) | 64 (6.9%) | 165 (7.6%) | 0.489 |
| Chronic conditions *** | 199 (6.4%) | 63 (6.8%) | 136 (6.3%) | 0.589 |
| Frequent smoking | 394 (12.7%) | 110 (11.9%) | 284 (13.1%) | 0.343 |
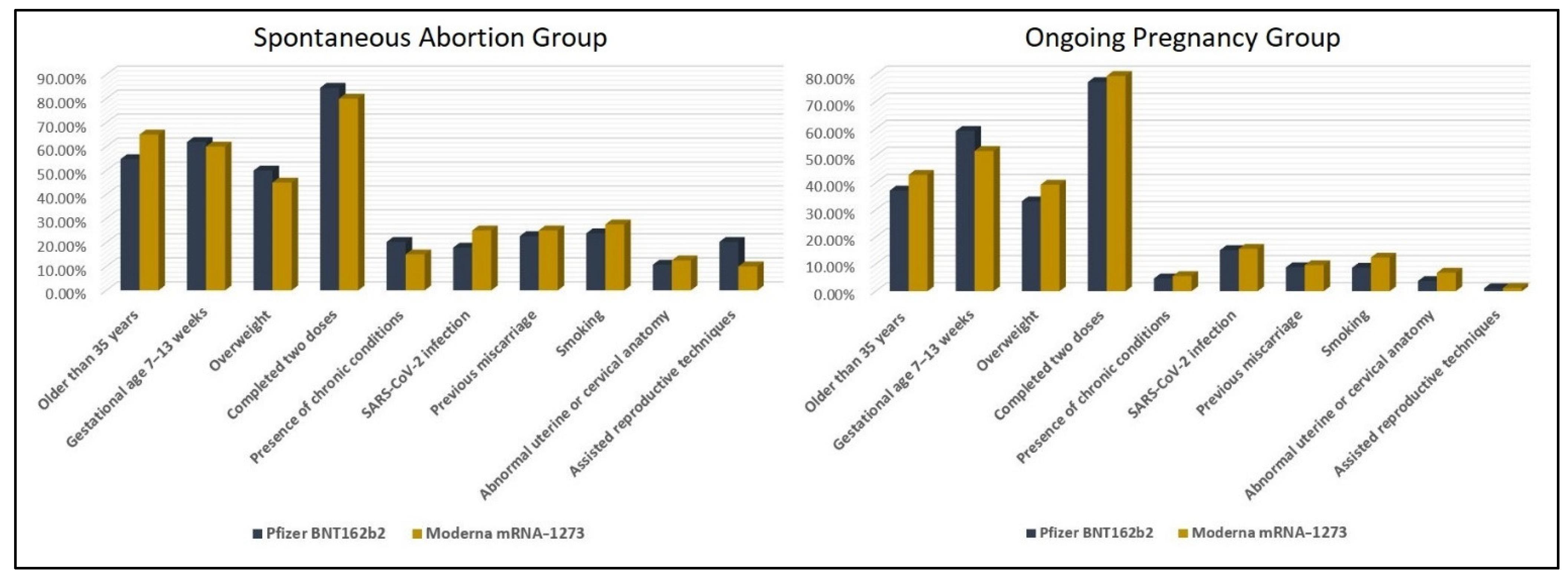
| Characteristics * | Spontaneous Abortion (n = 124) | Ongoing Pregnancy (n = 803) | p-Value |
|---|---|---|---|
| Age | <0.001 | ||
| <35 | 52 (41.9%) | 490 (61.0%) | |
| ≥35 | 72 (58.1%) | 313 (39.0%) | |
| Weight ** | 0.004 | ||
| Normal (<25 kg/m2) | 64 (51.6%) | 521 (64.9%) | |
| Overweight (≥25 kg/m2) | 60 (48.4%) | 282 (35.1%) | |
| Gestational age | 0.358 | ||
| 1–6 weeks | 48 (38.7%) | 346 (43.1%) | |
| 7–13 weeks | 76 (61.3%) | 457 (56.9%) | |
| Vaccine | 0.779 | ||
| Pfizer BNT162b2 | 84 (67.7%) | 554 (68.9%) | |
| Moderna mRNA-1273 | 40 (32.3%) | 249 (31.1%) | |
| Number of doses | 0.232 | ||
| 1 | 17 (13.7%) | 120 (14.9%) | |
| 2 | 103 (83.1%) | 626 (77.9%) | |
| 3 | 4 (3.2%) | 57 (7.2%) | |
| Other vaccines given during 1st trimester | |||
| Tdap | 83 (66.9%) | 519 (64.6%) | 0.619 |
| HPV | 7 (5.6%) | 62 (7.7%) | 0.412 |
| Influenza | 42 (33.9%) | 271 (33.7%) | 0.978 |
| Chronic conditions *** | <0.001 | ||
| Yes | 23 (18.5%) | 40 (4.9%) | |
| No | 101 (81.5%) | 763 (95.1%) | |
| SARS-CoV-2 infection | 0.175 | ||
| Yes | 25 (20.1%) | 123 (15.3%) | |
| No | 99 (79.9%) | 680 (84.7%) | |
| Previous miscarriage | <0.001 | ||
| Yes | 29 (23.3%) | 73 (9.1%) | |
| No | 95 (76.7%) | 730 (90.9%) | |
| Smoking status | <0.001 | ||
| Smoker | 31 (25.0%) | 79 (9.8%) | |
| Non-smoker | 93 (75.0%) | 724 (90.2%) | |
| Abnormal uterine or cervical anatomy | 0.003 | ||
| Yes | 14 (11.3%) | 38 (4.7%) | |
| No | 110 (88.7%) | 765 (95.3%) | |
| Karyotype analysis (n = 37) | |||
| Normal | 26 (70.3%) | - | |
| Abnormal | 11 (29.7%) | - | |
| Assisted reproductive techniques | <0.001 | ||
| Yes | 21 (16.9%) | 9 (1.1%) | |
| No | 103 (83.1%) | 794 (98.9%) |
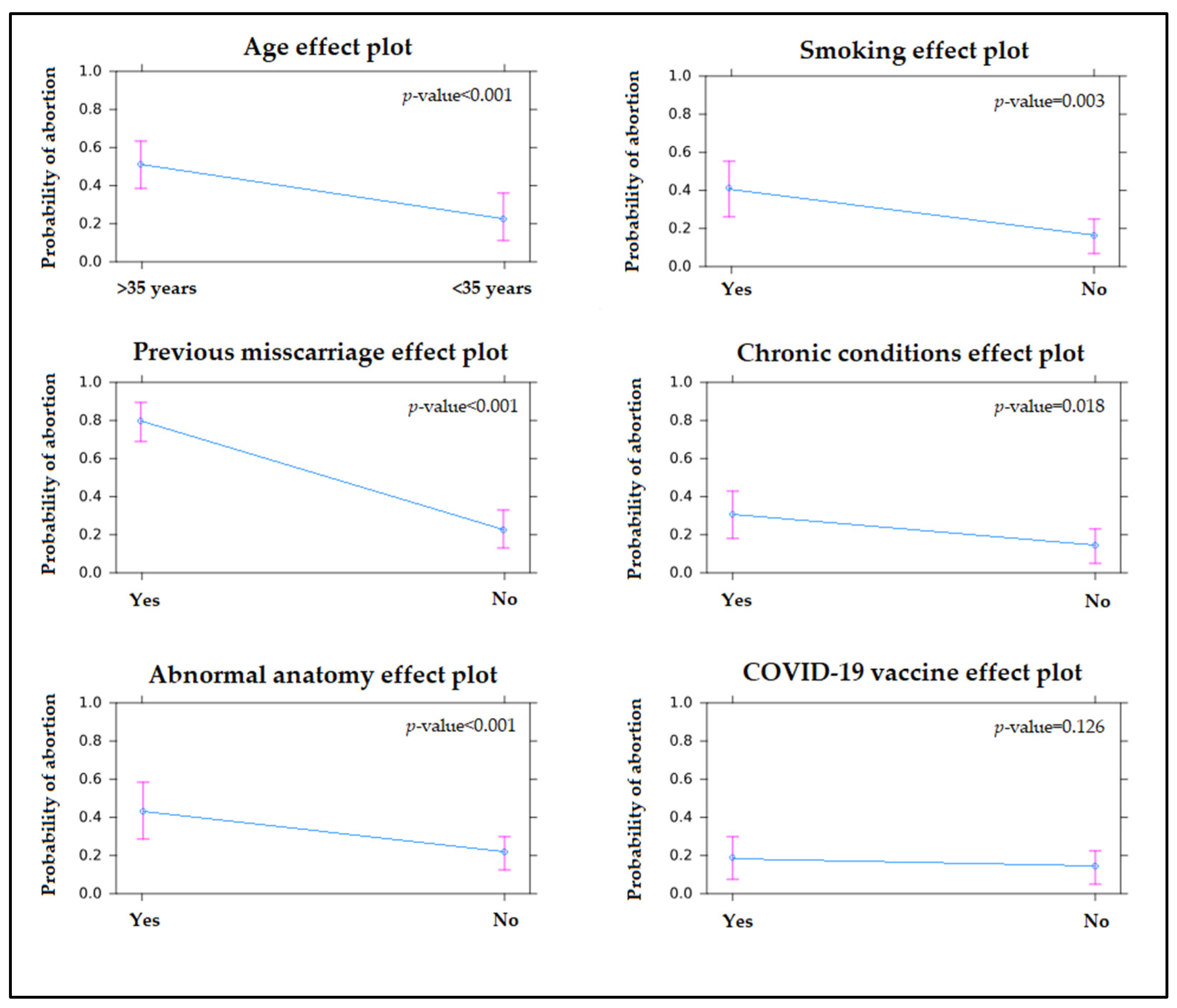
| Factors | Adjusted OR | 95% CI | p-Value |
|---|---|---|---|
| Maternal age (>35 years) | 1.81 | 1.48–2.15 | <0.001 |
| Overweight status (≥25 kg/m2) | 1.03 | 0.86–1.19 | 0.192 |
| Smoker | 1.22 | 1.03–1.36 | 0.003 |
| Presence of chronic conditions | 1.18 | 1.06–1.35 | 0.018 |
| Previous SARS-CoV-2 infection | 0.94 | 0.72–1.14 | 0.149 |
| Abnormal uterine or cervical anatomy | 1.33 | 1.10–1.68 | <0.001 |
| Previous miscarriage | 2.02 | 1.54–2.61 | <0.001 |
| Assisted reproductive techniques | 1.09 | 0.94–1.15 | 0.042 |
| Vaccine type | |||
| Pfizer BNT162b2 | 1.04 | 0.91–1.12 | 0.086 |
| Moderna mRNA-1273 ^ | 1.02 | 0.89–1.08 | 0.175 |
| Number of doses | |||
| 1 dose ^ | 0.91 | 0.69–1.08 | 0.338 |
| 2 doses | 0.94 | 0.66–1.05 | 0.247 |
| 3 doses | 0.77 | 0.60–1.01 | 0.590 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Citu, I.M.; Citu, C.; Gorun, F.; Sas, I.; Bratosin, F.; Motoc, A.; Burlea, B.; Rosca, O.; Malita, D.; Gorun, O.M. The Risk of Spontaneous Abortion Does Not Increase Following First Trimester mRNA COVID-19 Vaccination. J. Clin. Med. 2022, 11, 1698. https://doi.org/10.3390/jcm11061698
Citu IM, Citu C, Gorun F, Sas I, Bratosin F, Motoc A, Burlea B, Rosca O, Malita D, Gorun OM. The Risk of Spontaneous Abortion Does Not Increase Following First Trimester mRNA COVID-19 Vaccination. Journal of Clinical Medicine. 2022; 11(6):1698. https://doi.org/10.3390/jcm11061698
Chicago/Turabian StyleCitu, Ioana Mihaela, Cosmin Citu, Florin Gorun, Ioan Sas, Felix Bratosin, Andrei Motoc, Bogdan Burlea, Ovidiu Rosca, Daniel Malita, and Oana Maria Gorun. 2022. "The Risk of Spontaneous Abortion Does Not Increase Following First Trimester mRNA COVID-19 Vaccination" Journal of Clinical Medicine 11, no. 6: 1698. https://doi.org/10.3390/jcm11061698