 Laura Orsolini
Laura Orsolini Simone Pompili
Simone Pompili Antonella Mauro
Antonella Mauro Virginio Salvi
Virginio Salvi Umberto Volpe
Umberto Volpe- Unit of Clinical Psychiatry, Department of Neurosciences/DIMSC, Polytechnic University of Marche, Ancona, Italy
The COVID-19 pandemic situation significantly affected the mental health of the general and clinical population. However, few studies investigated which COVID-19-related psychopathological determinants may predispose to perinatal depression. We evaluated the impact of COVID-19 related anxiety and fear on perinatal depression in Italy. We retrospectively screened 184 perinatal outpatients afferent to Perinatal Mental Health outpatient service, during March 2020-March 2021, by administering the Edinburgh Postnatal Depression Scale (EPDS), the Fear of COVID-19 (FCV-19-S) and the Coronavirus Anxiety Scale (CAS). Among these, 85 patients agreed to be recruited in the present study. The mean EPDS score was 9.0, experiencing a clinically relevant perinatal depression in 45.7% of the sample. The mean FCV-19-S score was 15.0 and CAS was 1.7. Linear regression analyses demonstrated that FCV-19-S and CAS scores statistically significantly predicted EPDS total scores. A positive significant correlation was reported between FCV-19-S and EPDS and between CAS and EPDS. During the COVID-19 pandemic, women in their perinatal period, independently of previous psychiatric history, experienced increased levels of anxiety, fear and psychological distress, due to subsequent isolation, quarantine, lockdown and deprivation of their normal social support. Further preventive and screening strategies should be implemented in order to early identify at-risk pregnant and puerperal women during the COVID-19 pandemic.
Introduction
The COVID-19 pandemic situation significantly affected the mental health of the general and clinical population (1–5). The COVID-19-related situation determined a significant psychological distress, by determining increased levels of fear, anger and uncertainty, anxiety and depression symptomatology, suicidality, post-traumatic-related symptomatology, sleep disorders, and it facilitated the onset of de novo brief psychotic episodes, and so forth (6–15). Although few studies investigated the impact of COVID-19 pandemic and related restrictive measures on the women's mental health, during the pregnancy and the postpartum period, it was documented an overall increased incidence of anxious and depressive symptomatology in the perinatal period during the COVID-19 pandemic compared to pre-COVID-19 times (16–18).
The perinatal period (i.e., that period including all pregnancy and the first postpartum year) (19), indeed represents a critical vulnerable period for the de novo onset and recurrence of mental conditions, especially among women with a positive psychiatric history or those who experience gestational and/or delivery complications (20, 21). Based on the bio-psycho-social paradigm of mental disorders (22), the perinatal period may predispose women to experience high psychological distress due to physiological, biological, and social changes (17, 23–25). Moreover, within this framework, experiencing stressful and subjectively perceived traumatic events, during the perinatal period, may predispose women to the onset of de novo psychopathological manifestations, also in not predisposed pregnant and puerperal women (26). Therefore, one could argue that the COVID-19 pandemic and related restrictive measurements may have more likely represented a stressful and cumulative traumatic variable which might have modified the psychopathological trajectory in pregnancy and postpartum period, as already reported in the general population (27, 28) and in samples constituted by pregnant and postpartum women (18, 29–31). In fact, the gradual shaping in health care access and services due to the lockdown and restrictive regulations imposed by governments, including limitations in the access to gynecological, obstetrician and perinatal care and the restricted (or interrupted) possibility for partner and/or family member(s) of pregnant and puerperal women to assist them during pregnancy follow-ups, the delivery and postpartum period, significantly determined a psychological distress, an increased uncertainty and indeed fueled feelings of fears, anxiety and worries among pregnant and postpartum women (32–34). Moreover, perinatal women's mental health was also compromised by anxiety levels and worries related to disinformation overflow about COVID-19 pandemic and consequences for pregnant women's health and new-borns' health in case of COVID-19 infection during the pregnancy and/or early postpartum, as well as the uncertainty about the future (24, 35, 36).
Therefore, within the context of a multicenter nationwide population-based naturalistic observational project on perinatal depression, a retrospective chart-review study was carried out at the Unit of Clinical Psychiatry, Department of Neurosciences, University-Hospital “Ospedali Riuniti,” in Ancona, Italy, in collaboration with the Unit of Clinical Gynecology and Obstetrics, University Hospital “Salesi,” in Ancona, Italy. The main purpose of the larger observational protocol was to implement diagnostic and therapeutic interventions for early detection of at-risk women for occurring perinatal mental disorders as well as provide timely treatments. Within this larger project, our study firstly aimed at retrospectively analyzing those data collected during the COVID-19 pandemic, to evaluate the potential impact of COVID-19 related anxiety and fear on perinatal women's mental health, particularly perinatal depression levels. Given the exploratory nature of the study, we had no a priori hypothesis.
Methods
Study design and selection of participants
A retrospective chart-review study was carried out by recruiting all women afferent to the Peripartum Psychiatry Outpatient Service of the Unit of Clinical Psychiatry, at the University Hospital “Ospedali Riuniti,” Polytechnic University of Marche, Ancona, Italy, and/or hospitalized at the Unit of Clinical Gynecology and Obstetrics at the University Hospital “Salesi,” in Ancona, Italy, during the timeframe March 2020 to March 2021. Written informed consent was obtained from the patients after they were informed about the purpose of the study and the related methods. The study was introduced as aiming to assess whether pregnant or puerperal women's mental health changed during the Italian phase I-II-III of the COVID-19 pandemic and whether factors associated with the COVID-19 restrictions affected the course of perinatal symptomatology. Patients were retrospectively included in the study if they met the following inclusion criteria: (a) ≥18 years old; (b) education level not lower than elementary school; (c) absence of linguistic difficulties (i.e., not Italian speaker or foreign without a sufficient ability to understand Italian language); (d) no intellectual disability; (e) absence of severe medical conditions not related to the pregnancy and/or postpartum clinical situation; (f) pregnant women or within their first year of postpartum; (g) signed informed consent for collecting and analyzing clinical data for research purpose, collected during the baseline assessment. Participants were excluded if they met one or more of the following exclusion criteria: (a) intellectual disability or cognitive impairment; (b) diagnosis of organic mental disorder according to the DSM-5 criteria (37); (c) being under the influence of substances and/or alcohol; (d) incomplete filled out questionnaire; (e) refusal to participate to the research study. Recruited patients had also the possibility to withdraw their participation without any kind of clinical and therapeutic consequences. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Institutional Review Board approved our study. This research study was conducted retrospectively from data obtained for clinical purposes. All patients gave written consent to the use of clinical data for research purposes.
Measures
An ad hoc case report form was specifically designed by the researchers to collect sociodemographic data (e.g., age, ethnic, marital status, housing condition, employment status, education level) and clinical data and pregnancy-related correlates (e.g., family context, social support, medical history, psychiatric personal and family history, number of children, obstetric-gynecologic variables, such as last menstruation date [LMD], estimated delivery date [EDD], previous history of miscarriages or induced abortion, delivery course and immediate outcomes).
As a screening tool for diagnosing pregnant and postpartum women who are at risk for perinatal depression, it was used the Edinburgh Postnatal Depression Scale (EPDS) (38–40). EPDS is a 10-items, four-point Likert-type self-assessment questionnaire, which was developed based on the American College of Obstetrics and Gynecology (ACOG) recommendations (41), to assess mood in pregnant women during the past week. The EPDS total score ranges from 0 to 30, with a clinically relevant cut-off ≥12 which indicates a higher risk for perinatal depression in the Italian sample (42, 43).
The following scales have been administered to evaluate the following COVID-19-related psychopathological dimensions: i.e., experiences of fear by using the Fear of COVID-19 Scale (FCV-19-S) (44, 45) and anxiety symptomatology by using the Coronavirus Anxiety Scale (CAS) (46–48). The FCV-19-S is a 7-items, 5-point Likert-type questionnaire (1= “strongly disagree”, 5= “strongly agree”), measuring the emotional fear occurring during COVID-19 pandemic. The total score ranged from 7 to 35, with a cut-off≥16.86 that was used to identify a significant risk of fear and other related disorders in the Italian sample (44, 45). The CAS is a 5-item, 5-point Likert-type self-report tool designed to measure the levels of dysfunctional anxiety related to the COVID-19 pandemic over the preceding 2 weeks, with a clinically relevant cut-off ≥9 in the Italian sample (46, 48).
Statistical analysis
Statistical analyses were performed using SPSS (MACOS version 26; IBM Corp, Harmony [NY], 2019). Descriptive statistics were expressed as mean and standard deviation (SD) for the qualitative variables (EPDS, WDEQ, CAS and FCV-19-S), whereas normally distributed; while as median and 95% Confidence Interval (CI) when not normally distributed. After analyzing the continuous variables for skewness, kurtosis, normality distribution through the Shapiro-Wilk test, and the equality of variances by Levene test, parametric or non-parametric statistical tests were used when appropriate. Categorical variables (i.e., socio-demographic features, clinical and pregnancy-related variables) were presented in frequency (n) and percentage (%). Student's t-test for independent data and the non-parametric Mann-Whitney U-test for independent data were used, when appropriate, to compare the mean values of continuous variables among the two groups (pregnant vs. puerperal women) and between two groups (women with a significant EPDS score and women with a not significant EPDS score). The Chi-Square test was used to examine differences in the distribution of all categorical variables between two groups (pregnant vs. puerperal women) and between two groups (women with a significant EPDS score and women with a not significant EPDS score). One-way analysis of variance (ANOVA) or Kruskal-Wallis tests were used, where appropriate, to compare all continuous variables according to all socio-demographic and clinical categorical variables. Bivariate Pearson's correlations were used to investigate potential relationships between EPDS scores and other secondary continuous variables (CAS and FCV-19-S). A linear regression analysis was run to predict EPDS scores (dependent variable) from CAS (independent variable) and EPDS scores (dependent variable) from FCV-19-S (independent), after verifying all socio-demographic variables in both models as well. All the analyses were two-sided with a significance level settled at p < 0.05.
Results
Socio-demographic features of the sample
All socio-demographic characteristics of the included subjects are summarized in Table 1. A total of 184 women were consecutively assessed during the timeframe March 2020-March 2021. Among these, 85 patients gave written informed consent, agreed to provide their data for research purposes, and were recruited in the present study. After excluding those patients who subsequently decided to withdraw from the study (N = 6) and patients who did not fully fill out the questionnaires (N = 9), a final sample consisting of 70 subjects was finally included. The mean age was 34.8 years (SD = 5.8), without any significant differences between pregnant and postpartum women (p = 0.566). All women declared to be married or cohabiting with their partner, while 50% of the sample (N = 35) declared to be full-time employed and with an average middle-level of financial status declared (N = 61; 87.1%) (Table 1). Most women were assessed between January 2021 and March 2021 (N = 60; 85.7%), during the third trimester of their pregnancy (N = 36; 51.4%) and during the first postpartum trimester (N = 24; 34.3%). Most participants had a previous pregnancy (N = 44; 62.9%) and about 20% of participants (N = 14) declared to have experienced at least one miscarriage. Less than half of participants reported a current regular pregnancy course (N = 33; 47.1%) while most participants declared a desired pregnancy (N = 63; 90%) (Table 2).
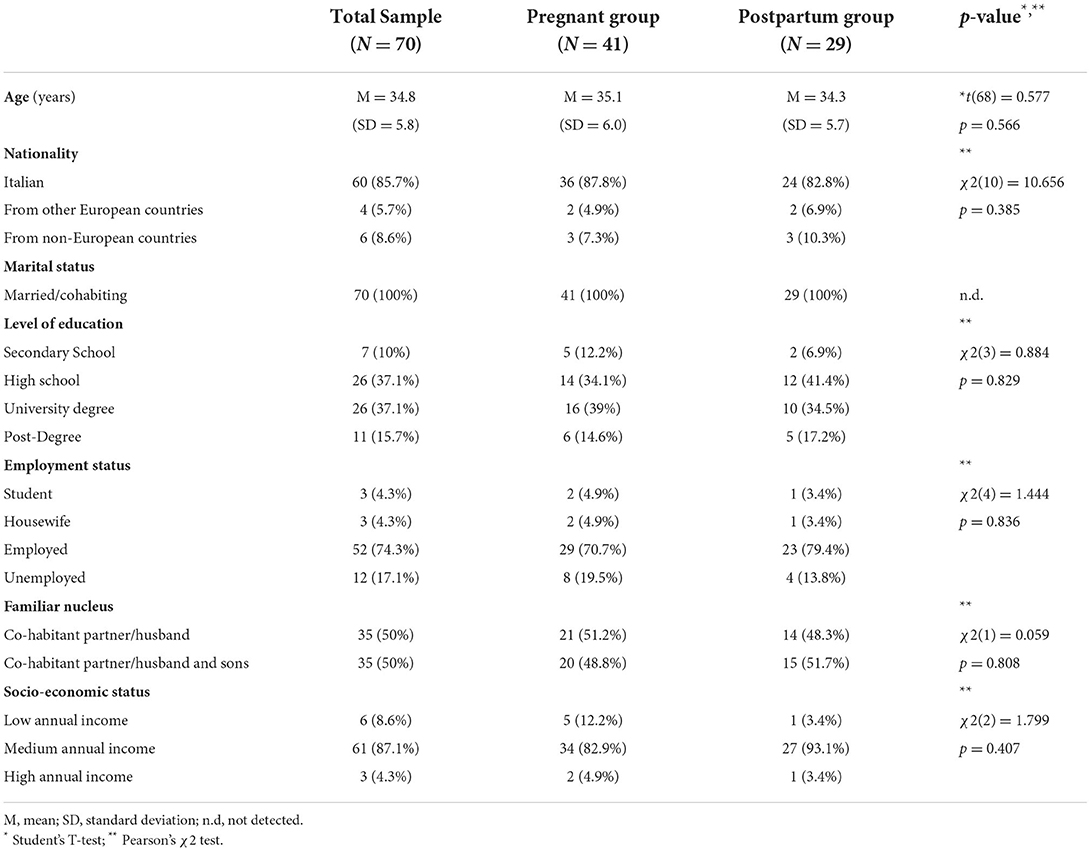
Table 1. Socio-demographic characteristics of the sample.
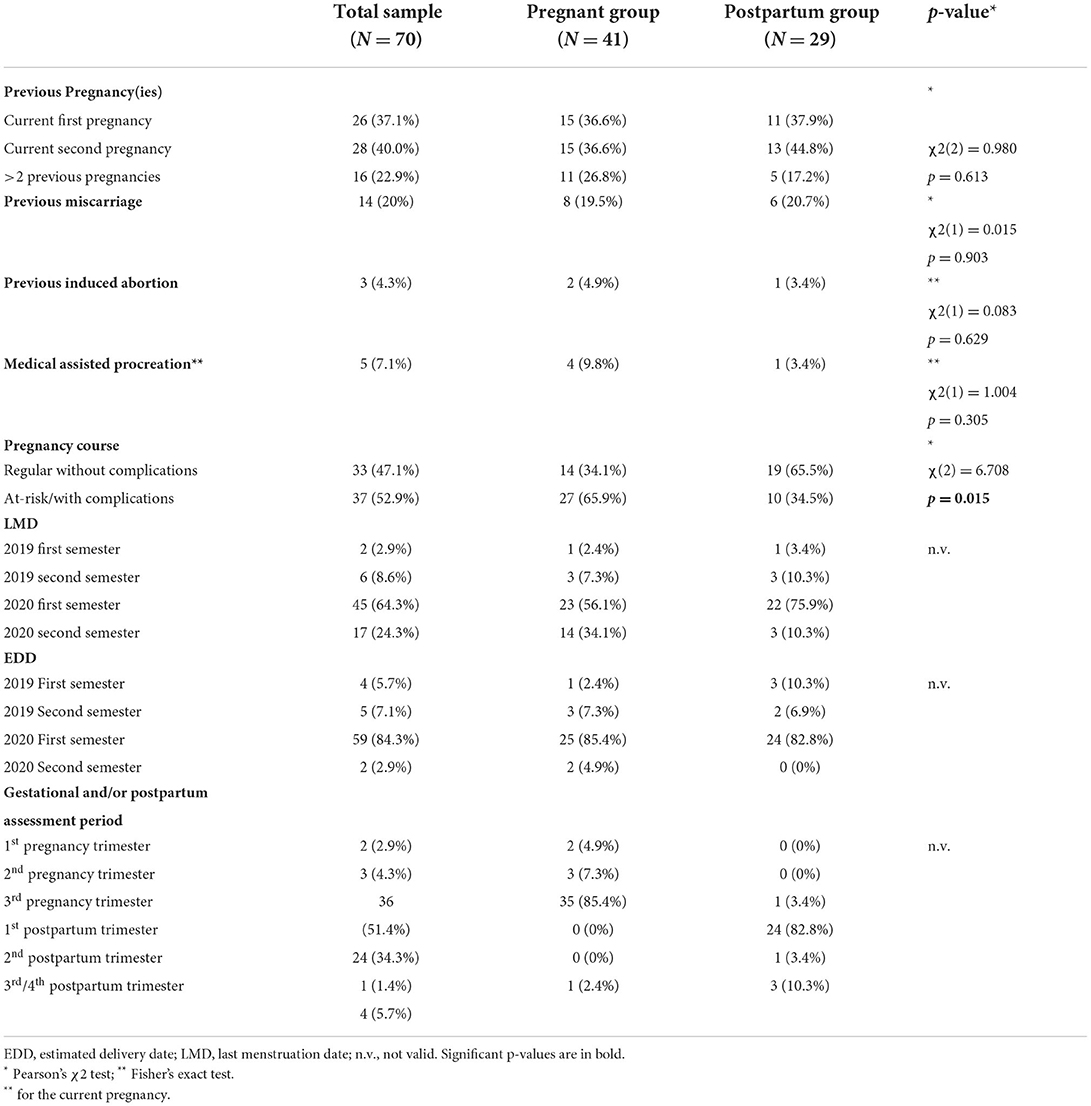
Table 2. Obstetric-gynaecological characteristics of the sample.
Clinical and psychopathological features of participants
Table 3 provides a summary of clinical and psychopathological data. Most of participants did not report any previous psychiatric history (N = 64; 91.4%), any previous psychiatric hospitalization (N = 69; 98.6%), any psychopharmacological therapy before pregnancy (N = 61; 87.1%) and/or during pregnancy (N = 61; 87.1%), either any current psychotherapy (N = 66; 94.3%) (Table 3).
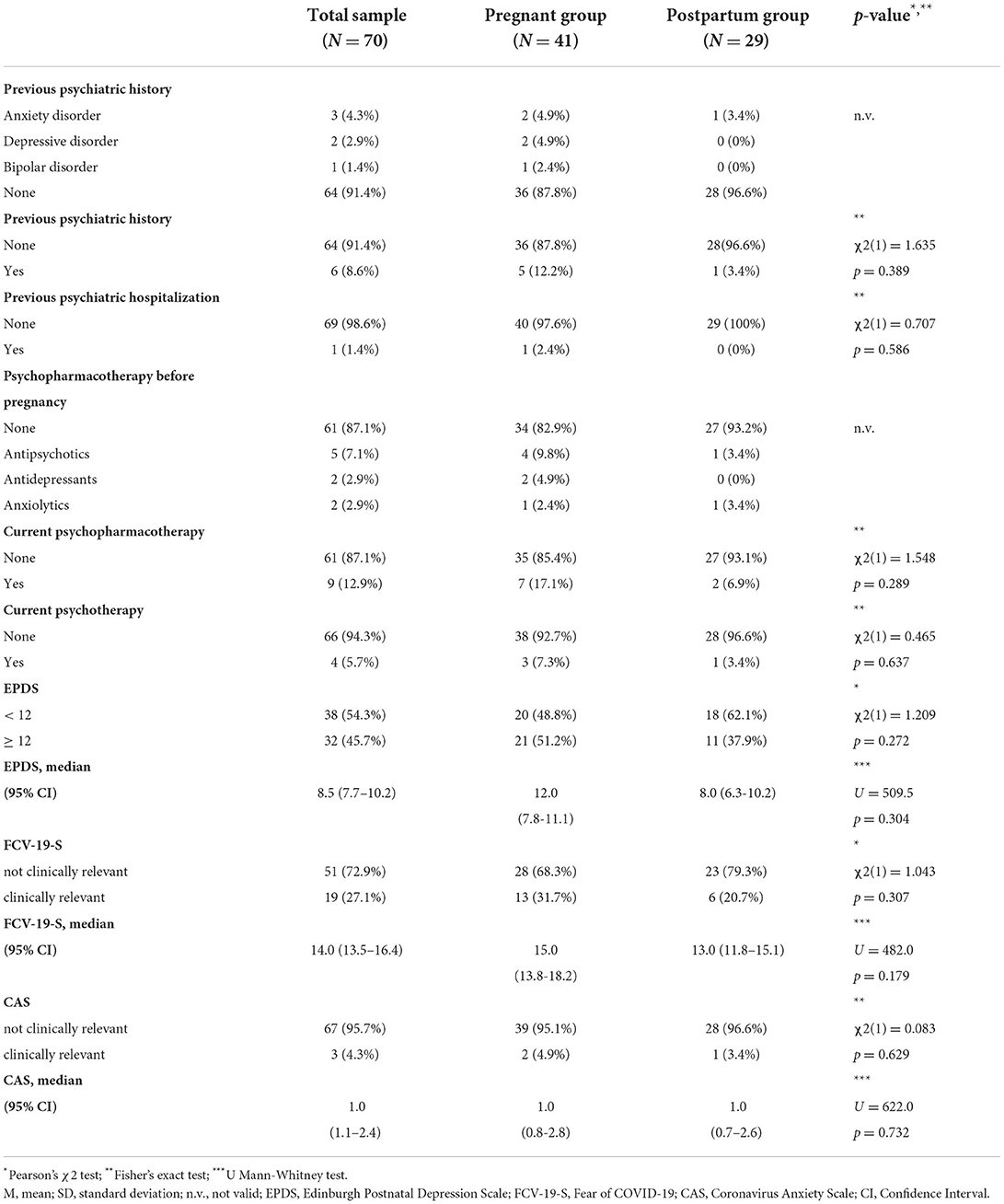
Table 3. Clinical and psychopharmacological characteristics of the sample.
The mean total score at the EPDS was 9.0 (SD = 5.3), being experienced a clinically relevant perinatal depression (EPDS≥12) in 45.7% of the sample, without any significant differences between pregnant and puerperal women (p = 0.304) (Table 3).
The mean total score at FCV-19-S was 15.0 (SD = 6.2), with clinically relevant COVID-19-related fear (FCV-19-S≥16.86) experienced by 27.1% of participants, without any significant differences between pregnant and puerperal women (p = 0.179). Statistically significant higher FCV-19-S scores were found in women who had a previous psychiatric hospitalization (p = 0.029). Significant higher FCV-19-S scores were found in women with clinically relevant CAS total scores (p = 0.001) and clinically relevant EPDS total scores (p = 0.004) (Table 4). A positive correlation was found between FCV-19-S and EPDS (r = 0.390, p < 0.001) (Table 5). Linear regression analysis demonstrated that FCV-19-S scores statistically significantly predicted EPDS total scores [F(1,68) = 12.218, R2 = 0.152, p < 0.001] (Figure 1). No socio-demographic and/or clinical variables included in the regression model demonstrated to be predictive of EPDS scores.
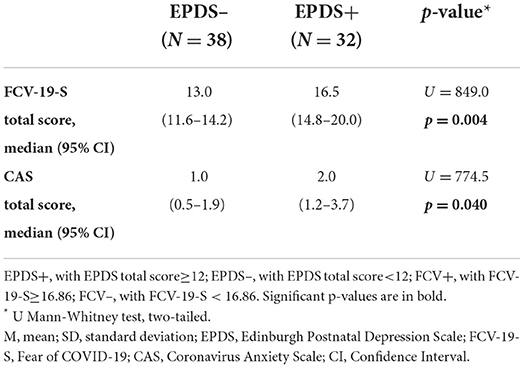
Table 4. Psychopathological differences according to the EPDS screening.
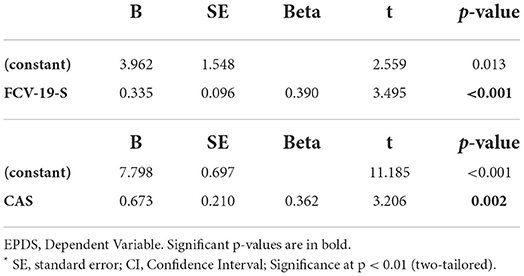
Table 5. Linear regression models.
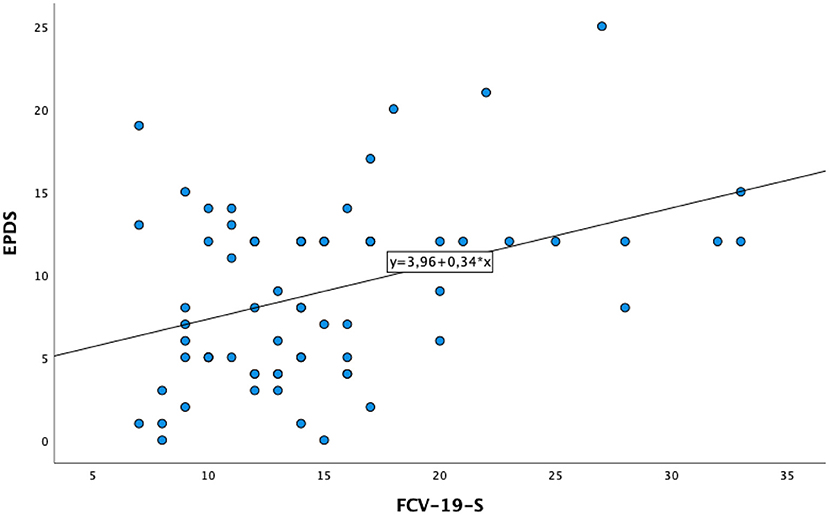
Figure 1. Linear regression model between FCV-19-S and EPDS.
The mean total score at CAS was 1.7 (SD = 2.8), with clinically relevant anxiety related to COVID-19 (CAS≥ 9) experienced by 4.3% of women, without any significant differences between pregnant and puerperal women (p = 0.732). Significant higher CAS scores were found in women who were positive for perinatal depression at EPDS (p = 0.040) (Table 4). A statistical trend with higher CAS scores was observed in those women with a previous psychiatric history of depressive episode(s) and/or major depressive disorder, compared to women without a previous psychiatric history (p = 0.054). A positive correlation was found between CAS and EPDS (r = 0.362, p < 0.001) and between CAS and FCV-19-S (r = 0.641, p < 0.001) (Table 5). Linear regression analysis demonstrated that CAS scores statistically significantly predicted EPDS total scores [F(1,68) = 10.278, R2 = 0.131, p = 0.002] (Figure 2). No socio-demographic and/or clinical variables included in the regression model demonstrated to be predictive of EPDS scores.
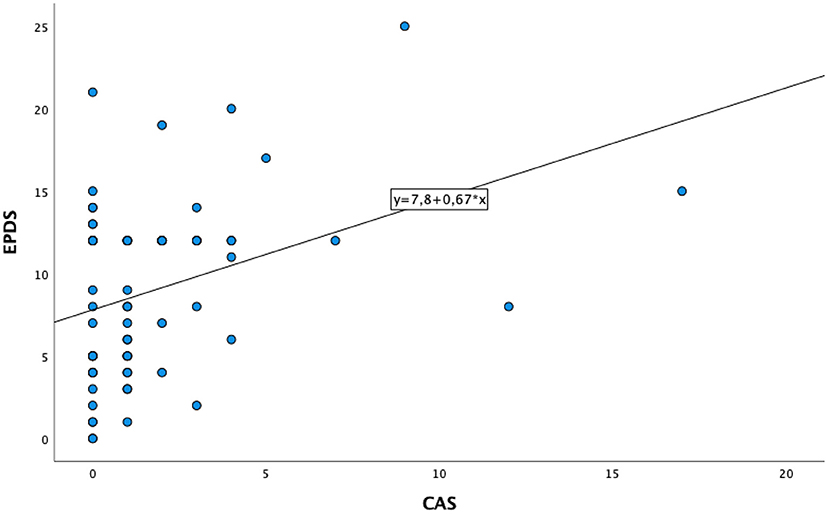
Figure 2. Linear regression model between CAS and EPDS.
Discussion
During the COVID-19 pandemic, pregnant and puerperal women worldwide reported increased levels of mental distress due to lack of access to healthcare, social isolation, sleep loss, feelings of fear and uncertainties (49–55). Overall, our sample reported a clinically relevant perinatal depression, as measured by EPDS, in 45.7% of the sample, with a higher rate, compared to previous international and national studies carried out before the COVID-19 pandemic (56–63). In fact, the prevalence of perinatal depression was estimated between 10–20% in non-Italian samples (59–62). While, in the few studies conducted to assess the Italian prevalence of perinatal depression, a highly variable prevalence was observed ranging from 1.6 to 26.6%, even though all of these studies were carried out before the COVID-19 pandemic indeed (42, 56–58, 64). Our findings are in line with previous published (both international and Italian) studies carried out during the COVID-19 pandemic which reported significantly higher depression rates in pregnant women than studies conducted before the pandemic, with a prevalence ranging from 30 to 43% (16, 18, 29, 31, 53, 65–71).
Although the effects of COVID-19 pandemic on perinatal mental health are still not fully investigated, pregnant and puerperal women represent indeed a particular vulnerable/at-risk population for developing mental health disorders, particularly during stressing situations, such as the current COVID-19 pandemic (72). Accordingly, our findings found that women, who have some mental distress related to the current COVID-19 outbreak, as measured by FCV-19-S and CAS scores, manifested clinically significant scores at EPDS. In particular, significant higher levels of COVID-19 fear were found in women who had a previous psychiatric hospitalization, by suggesting that women with a pre-existing psychiatric history may be more likely vulnerable to manifest fear of COVID-19 and, indirectly, manifest higher perinatal depressive levels compared to those without a previous psychiatric history. However, being our sample more represented by women without a psychiatric diagnosis, further larger studies specifically recruiting and comparing pregnant and postpartum women with and/or without a pre-existing psychiatric diagnosis should be carried out to better investigate this hypothesis. Moreover, our findings reported a significant positive correlation between fear of COVID-19 and COVID-19-related anxiety levels, as well as between fear of COVID-19 and perinatal depression levels, as already documented in previous studies (73–75). Furthermore, our findings documented a significant positive correlation between COVID-19-related anxiety and perinatal depression levels, as already demonstrated in previous studies (76, 77). In fact, the fear of contagion and for the health of the child, the difficulty in promptly accessing to health care system due to the COVID-19 restrictive measures, as well as the poor availability in being supported by own partner and/or family members during the hospitalization for the delivery may represent all factors which may have determined increased depressive and anxious symptoms in women during the peripartum period (67, 70, 72, 78). The increased levels of COVID-19 anxiety seems to be related to specific concerns about the impact of the COVID-19 on maternal health, fetal/neonatal health, vertical transmission of COVID-19 infection from mother to fetus and worries regarding the potential separation and social distancing from family and social relationships during the perinatal period due to quarantine measures (67, 79, 80). In fact, the most critical fears and worries experienced by pregnant and postpartum women regard the possibility of family members to be not present during the perinatal period, during the hospitalization, labor and childbirth while restriction policies in hospital settings are in place (31, 81).
Moreover, most participants of our study did not report any previous psychiatric history and/or psychiatric hospitalization and/or any psychopharmacological treatment and/or psychological support before pregnancy. Therefore, our findings suggest that increased levels of perinatal depression may be experienced during the COVID-19 pandemic, more likely due to isolation and quarantine experience, also by pregnant and puerperal women, independently by pre-existing psychiatric disorders. Moreover, our sample is more representative of perinatal period comprising the third trimester of pregnancy and the first postpartum trimester, hence, one could argue that our findings might potentially reflect the effect of the COVID-19 pandemic during this period and that higher levels of perinatal depression observed in our sample might be due an effect dependent on the perinatal stage, as already documented in previous studies (31, 82). In fact, according to these studies, the risk of negative psychological consequences during the COVID-19 pandemic may be increased especially in pregnant women in their third trimester who foresee delivery during the pandemic, as they may experience elevated stress and anxiety due to the potential adverse outcomes on the fetus and the infant (31, 79, 82). Despite a larger longitudinal study by Mei et al. (30) found that the gestational trimester had no correlation with depression, anxiety and stress rates. Therefore, further studies should assess and investigate the perinatal stage variable on perinatal depression, anxiety and stress.
Despite the abovementioned promising findings, the present study has several limitations. Firstly, the cross-sectional study design and the small sample size may limit the generalizability of the findings and may not be fully representative of the full peripartum period, being mainly recruited women at their third trimester of pregnancy and during their first postpartum trimester. The attrition rate between women assessed and women included was indeed mainly due to expressed worry by pregnant and puerperal women recruited during the COVID-19 pandemic to find some relevant COVID-19-related psychopathology and the lack of time to fill out all questionnaires administered (particularly among puerperal women). The lack of a control group constituted by not-pregnant women, coming from both a clinical and not-clinical sample, may not allow the comparability of the findings and may not adequately evaluate the gender-effect on the development of higher depressive scores, independently by the pregnancy and/or postpartum period during the COVID-19 pandemic. Moreover, another issue is the lack of a control group constituted by males, for instance including the partners of recruited women and/o coming from the general population may not allow to discriminate whether the observed effect of COVID-19-related anxiety and fear may really impacting on the perinatal depression due to the gender effect or rather the COVID-19-related psychopathological burden in the vulnerable population of pregnant and/or puerperal women. Secondly, our sample is constituted mainly by women without a previous psychiatric history which may not allow us to completely evaluate the differential impact of the COVID-19 pandemic on pregnant and/or postpartum women with a previous psychiatric disease and compare them with those with a negative psychiatric history. Thirdly, although we collected several socio-demographic and clinical variables in our sample, we did not find that none of these socio-demographic and/or clinical variables demonstrated to be significant predictors of EPDS scores. However, these findings could be mainly due to the small sample size here recruited. Therefore, a larger study recruiting also women with more heterogeneous socio-demographic features could allow researchers to better understand whether a specific socio-demographic and/or clinical profile could represent a predictor of EPDS scores during the COVID-19 pandemic. Moreover, even though the administered assessment tools here chosen, demonstrated to be valid and highly reliable measures of COVID-19-related fear and anxiety symptomatology, some limitations of these self-report questionnaires should be carefully considered and discussed when we interpret our findings. For instance, while some studies reported no gender differences on the FCV-19S (45), other studies reported higher FCV-19S scores in females compared to males (4, 48). Similarly, CAS scores were found to be higher in females compared to males in the development and psychometric study of the tool (48, 83). Finally, our sample is represented by women without a previous and/or a current COVID-19 infection, hence, our findings may not completely evaluate whether the pregnant women with COVID-19 infection may be more or less likely to develop a perinatal depression compared with pregnant women without COVID-19 infection and/or not pregnant women with COVID-19 infection.
Therefore, further research directions performing longitudinal and case-control studies with larger sample sizes, including as potential variables the concomitant COVID-19 infection during pregnancy and/or postpartum period, should be conducted to better evaluate whether the gender-effect might explain the increased levels of depression in pregnant and/or postpartum women during the COVID-19 pandemic, as already reported in previous Italian studies which observed more severe psychological symptoms during the COVID-19 pandemic reported by females compared to males in Italian population (84–86). In fact, “caution is needed when reporting opinions or data coming from cross-sectional studies, especially in the absence of proper controls for lockdown” (87). Moreover, further studies should investigate how experiencing feelings of fear and anxiety related to the COVID-19 might determine increased levels of depression, independently by the pregnancy and/or postpartum period in women compared to men. Moreover, one should better investigate whether women with a previous psychiatry history may be more or less likely to develop increased levels of perinatal depression compared to women without a previous psychiatry history during the COVID-19 pandemic, independently by the variable to be infected with COVID-19 or not. Overall, our findings may indeed address clinicians to better evaluate and early identify those women at high-risk to develop perinatal depression during the COVID-19 pandemic, by investigating their levels of fear and perceived anxiety/distress due to the COVID-19 situation for preventive, screening and monitoring strategies. Finally, one could argue that a possible strategy which may help to improve screening activities could be implementing a smartphone-based screening tool consisting of CAS and FCV-19-S questionnaires which could be periodically and virtually administered to those pregnant and puerperal women to indirectly identify those at-risk to develop a perinatal depression in order to propose a psychological and/or psychiatric support (whereas necessary).
Conclusion
The COVID-19 pandemic and subsequent isolation, quarantine and lockdown represent a risk factor for pregnant and postpartum women who may experience a deprivation of their normal sources of family and social support and, hence, experience increased psychological distress. Our findings might address clinicians and politicians towards tailored clinical and policy implications to be implemented in the perinatal women, such as providing dedicated spaces and/or support figures, trained specifically on perinatal mental health consequences due to the COVID-19 pandemic and related restrictions, if possible. Trained mental health professionals can help women feel less isolated while facing the labor and postpartum period, within hospitals, during the COVID-19 pandemic, by offering psychoeducational interventions on perinatal mental health as well as COVID-19 and perinatal mental health issues. Moreover, implementing public mental health policies to allow a direct and indirect screening for perinatal depression during the COVID-19 pandemic.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Author contributions
LO and UV: conceptualization. LO: methodology, formal analysis, and writing—review and editing. LO, AM, and SP: data curation and collection. SP and LO: writing—original draft preparation. LO, VS, and SP: investigation. VS: visualization. UV: supervision. All authors contributed to the article and approved the submitted version.
Acknowledgments
We would like to acknowledge and thank all women who agreed to participate in the study and Isabella Gargano for partially assisting in data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor MS declared a past co-authorship/collaboration with one of the authors LO.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Holmes EA, O'Connor RC, Perry VH, Tracey I, Wessely S, Arseneault L, et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry. (2020) 7:547–60. doi: 10.1016/S2215-0366(20)30168-1
2. Bassi M, Negri L, Delle Fave A, Accardi R. The relationship between post-traumatic stress and positive mental health symptoms among health workers during COVID-19 pandemic in Lombardy, Italy. J Affect Disord. (2021) 280:1–6. doi: 10.1016/j.jad.2020.11.065
3. Grolli RE, Mingoti MED, Bertollo AG, Luzardo AR, Quevedo J, Réus GZ, et al. Impact of COVID-19 in the mental health in elderly: psychological and biological updates. Mol Neurobiol. (2021) 58:1905–16. doi: 10.1007/s12035-020-02249-x
4. Hossain DA. The Impact of COVID-19 on Accounting Profession by Dewan Azmal Hossain: SSRN. (2021). Available online at: http://dx.doi.org/10.2139/ssrn.3923710 (accessed January 20, 2022).
5. Murata S, Rezeppa T, Thoma B, Marengo L, Krancevich K, Chiyka E, et al. The psychiatric sequelae of the COVID-19 pandemic in adolescents, adults, and health care workers. Depress Anxiety. (2021) 38:233–46. doi: 10.1002/da.23120
6. Ho CS, Chee CY, Ho RC. Mental health strategies to combat the psychological impact of coronavirus disease 2019 (COVID-19) beyond paranoia and panic. Ann Acad Med Singapore. (2020) 49:155–60. doi: 10.47102/annals-acadmedsg.202043
7. Czeisler MÉ, Lane RI, Petrosky E, Wiley JF, Christensen A, Njai R. Mental Health, Substance Use, Suicidal Ideation During the COVID-19 Pandemic — United States. Centers for Disease Control Prevention. (2020). Available online at: https://archive.hshsl.umaryland.edu/handle/10713/19199 (accessed January 20, 2022).
8. Cénat JM, Blais-Rochette C, Kokou-Kpolou CK, Noorishad PG, Mukunzi JN, McIntee SE, et al. Prevalence of symptoms of depression, anxiety, insomnia, posttraumatic stress disorder, and psychological distress among populations affected by the COVID-19 pandemic: a systematic review and meta-analysis. Psychiatry Res. (2021) 295:113599. doi: 10.1016/j.psychres.2020.113599
9. Deng J, Zhou F, Hou W, Silver Z, Wong CY, Chang O, et al. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: a meta-analysis. Ann N Y Acad Sci. (2021) 1486:90–111. doi: 10.1111/nyas.14506
10. Doufik J, Ouhmou M, Bouraoua I, Laaraj H, Mouhadi K, Rammouz I. Acute psychotic episodes related to the COVID-19 pandemic. Ann Med Psychol (Paris). (2022) 180:410–1. doi: 10.1016/j.amp.2021.03.008
11. Jahrami H, BaHammam AS, Bragazzi NL, Saif Z, Faris M, Vitiello MV. Sleep problems during the COVID-19 pandemic by population: a systematic review and meta-analysis. J Clin Sleep Med JCSM Off Publ Am Acad Sleep Med. (2021) 17:299–313. doi: 10.5664/jcsm.8930
12. Mortier P, Vilagut G, Ferrer M, Alayo I, Bruffaerts R, Cristóbal-Narváez P, et al. Thirty-day suicidal thoughts and behaviours in the Spanish adult general population during the first wave of the Spain COVID-19 pandemic. Epidemiol Psychiatr Sci. (2021) 30:e19. doi: 10.1017/S2045796021000093
13. Oloniniyi IO, Ibigbami OI, Amiola A, Esan OA, Esan OO. First episode psychosis during COVID-19 pandemic: a case series. West Afr J Med. (2021) 38:599–603.
14. Silva Junior FJG, Miranda PIG, Sales JCES, Parente A da CM, Monteiro CF de S, Costa APC, et al. Suicidal behaviour in adults during the COVID-19 pandemic: protocol for systematic review of observational studies. BMJ Open. (2021) 11:e045313. doi: 10.1136/bmjopen-2020-045313
15. Smith LE, Duffy B, Moxham-Hall V, Strang L, Wessely S, Rubin GJ. Anger and confrontation during the COVID-19 pandemic: a national cross-sectional survey in the UK. J R Soc Med. (2021) 114:77–90. doi: 10.1177/0141076820962068
16. Sun G, Wang Q, Lin Y, Li R, Yang L, Liu X, et al. Perinatal depression of exposed maternal women in the COVID-19 pandemic in Wuhan, China. Front Psychiatry. (2020) 11:551812 doi: 10.3389/fpsyt.2020.551812
17. Baran J, Leszczak J, Baran R, Biesiadecka A, Weres A, Czenczek-Lewandowska E, et al. Prenatal and postnatal anxiety and depression in mothers during the COVID-19 pandemic. J Clin Med. (2021) 10:3193. doi: 10.3390/jcm10143193
18. Dong H, Hu R, Lu C, Huang D, Cui D, Huang G, et al. Investigation on the mental health status of pregnant women in China during the pandemic of COVID-19. Arch Gynecol Obstet. (2021) 303:463–9. doi: 10.1007/s00404-020-05805-x
19. Austin MP. Antenatal screening and early intervention for ≪perinatal≫ distress, depression and anxiety: where to from here? Arch Womens Ment Health. (2004) 7:1–6. doi: 10.1007/s00737-003-0034-4
20. Howard LM, Khalifeh H. Perinatal mental health: a review of progress and challenges. World Psychiatry. (2020) 19:313–27. doi: 10.1002/wps.20769
21. Sommer JL, Shamblaw A, Mota N, Reynolds K, El-Gabalawy R. Mental disorders during the perinatal period: results from a nationally representative study. Gen Hosp Psychiatry. (2021) 73:71–7. doi: 10.1016/j.genhosppsych.2021.09.011
22. Chen X, Hong F, Wang D, Bai B, Xia Y, Wang C. Related psychosocial factors and delivery mode of depression and anxiety in primipara in late pregnancy. Evid-Based Complement Altern Med ECAM. (2021) 2021:3254707. doi: 10.1155/2021/3254707
23. Bjelica A, Cetkovic N, Trninic-Pjevic A, Mladenovic-Segedi L. The phenomenon of pregnancy - a psychological view. Ginekol Pol. (2018) 89:102–6. doi: 10.5603/GP.a2018.0017
24. Diamond RM, Brown KS, Miranda J. Impact of COVID-19 on the perinatal period through a biopsychosocial systemic framework. Contemp Fam Ther. (2020) 42:205–16. doi: 10.1007/s10591-020-09544-8
25. Duberstein ZT, Brunner J, Panisch LS, Bandyopadhyay S, Irvine C, Macri JA, et al. The biopsychosocial model and perinatal health care: determinants of perinatal care in a community sample. Front Psychiatry. (2021) 12:746803. doi: 10.3389/fpsyt.2021.746803
26. Chen H, Selix N, Nosek M. Perinatal anxiety and depression during COVID-19. J Nurse Pract. (2021) 17:26–31. doi: 10.1016/j.nurpra.2020.09.014
27. Fiorillo A, Sampogna G, Giallonardo V, Del Vecchio V, Luciano M, Albert U, et al. Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: results from the COMET collaborative network. Eur Psychiatry. (2020) 63:e87. doi: 10.1192/j.eurpsy.2020.89
28. Sampogna G, Pompili M, Fiorillo A. Mental health in the time of COVID-19 pandemic: a worldwide perspective. Int J Environ Res Public Health. (2021) 19:161. doi: 10.3390/ijerph19010161
29. Denizli R, Sakin Ö, Koyuncu K, Çiçekli N, Farisogullari N, Özdemir M. The impact of the COVID-19 pandemic on depression and sexual function: are pregnant women affected more adversely? Rev Bras Ginecol Obstet. (2021) 43:765–74. doi: 10.1055/s-0041-1736174
30. Mei H, Li N, Li J, Zhang D, Cao Z, Zhou Y, et al. Depression, anxiety, and stress symptoms in pregnant women before and during the COVID-19 pandemic. J Psychosom Res. (2021) 149:110586. doi: 10.1016/j.jpsychores.2021.110586
31. Smorti M, Ponti L, Ionio C, Gallese M, Andreol A, Bonassi L. Becoming a mother during the COVID-19 national lockdown in Italy: issues linked to the wellbeing of pregnant women. Int J Psychol J Int Psychol. (2022) 57:146–52. doi: 10.1002/ijop.12806
32. Corbett GA, Milne SJ, Hehir MP, Lindow SW. O'connell MP. Health anxiety and behavioural changes of pregnant women during the COVID-19 pandemic. Eur J Obstet Gynecol Reprod Biol. (2020) 249:96–7. doi: 10.1016/j.ejogrb.2020.04.022
33. Thapa SB, Mainali A, Schwank SE, Acharya G. Maternal mental health in the time of the COVID-19 pandemic. Acta Obstet Gynecol Scand. (2020) 99:817–8. doi: 10.1111/aogs.13894
34. Jiang H, Jin L, Qian X, Xiong X, La X, Chen W, et al. Maternal mental health status and approaches for accessing antenatal care information during the COVID-19 epidemic in China: cross-sectional study. J Med Internet Res. (2021) 23:e18722. doi: 10.2196/18722
35. Yakovi Gan-Or N. Going solo: the law and ethics of childbirth during the COVID-19 pandemic. J Law Biosci. (2020) 7:lsaa079. doi: 10.1093/jlb/lsaa079
36. Rudrum S. Pregnancy during the global COVID-19 pandemic: Canadian experiences of care. Front Sociol. (2021) 6:611324. doi: 10.3389/fsoc.2021.611324
37. American Psychiatic Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 7th eds. Washington, DC (2013).
38. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry J Ment Sci. (1987) 150:782–6. doi: 10.1192/bjp.150.6.782
39. Gibson J McKenzie-McHarg K Shakespeare J Price J Gray R A A systematic review of studies validating the Edinburgh postnatal depression scale in antepartum and postpartum women. Acta Psychiatr Scand. (2009) 119:350–64. doi: 10.1111/j.1600-0447.2009.01363.x
40. O'Connor E, Rossom RC, Henninger M, Groom HC, Burda BU. primary care screening for and treatment of depression in pregnant and postpartum women: evidence report and systematic review for the US preventive services task force. JAMA. (2016) 315:388–406. doi: 10.1001/jama.2015.18948
41. McKinney J, Keyser L, Clinton S, Pagliano C, ACOG. Committee opinion no. 736: optimizing postpartum care. Obstet Gynecol. (2018) 132:784–5. doi: 10.1097/AOG.0000000000002849
42. Balestrieri M, Matteo B, Isola M, Miriam I, Bisoffi G, Giulia B, et al. Determinants of ante-partum depression: a multicenter study. Soc Psychiatry Psychiatr Epidemiol. (2012) 47:1959–65. doi: 10.1007/s00127-012-0511-z
43. Levis B, Negeri Z, Sun Y, Benedetti A, Thombs BD. Depression Screening Data (DEPRESSD) EPDS Group. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: systematic review and meta-analysis of individual participant data. BMJ. (2020) 371:m4022. doi: 10.1136/bmj.m4022
44. Soraci P, Ferrari A, Abbiati FA, Del Fante E, De Pace R, Urso A, et al. Validation and psychometric evaluation of the Italian version of the fear of COVID-19 scale. Int J Ment Health Addict. (2020) 1–10. doi: 10.1007/s11469-020-00277-1
45. Ahorsu DK, Lin CY, Imani V, Saffari M, Griffiths MD, Pakpour AH. The fear of COVID-19 scale: development and initial validation. Int J Ment Health Addict. (2022) 20:1537–45. doi: 10.1007/s11469-020-00270-8
46. Lee SA. Coronavirus anxiety scale: a brief mental health screener for COVID-19 related anxiety. Death Stud. (2020) 44:393–401. doi: 10.1080/07481187.2020.1748481
47. Mozzoni M, Franzot E. Coronavirus Anxiety Scale (CAS). Department of Psychology, Christopher Newport University (Virginia, USA). (2020)
48. Orrù G, Bertelloni D, Diolaiuti F, Conversano C, Ciacchini R, Gemignani A, et al. Psychometric examination of the coronavirus anxiety scale and the fear of coronavirus disease 2019 scale in the Italian population. Front Psychol. (2021) 12:669384. doi: 10.3389/fpsyg.2021.669384
49. Berthelot N, Lemieux R, Garon-Bissonnette J, Drouin-Maziade C, Martel É, Maziade M. Uptrend in distress and psychiatric symptomatology in pregnant women during the coronavirus disease 2019 pandemic. Acta Obstet Gynecol Scand. (2020) 99:848–55. doi: 10.1111/aogs.13925
50. Lebel C, MacKinnon A, Bagshawe M, Tomfohr-Madsen L, Giesbrecht G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J Affect Disord. (2020) 277:5–13. doi: 10.1016/j.jad.2020.07.126
51. Teng YM, Wu KS, Lin KL. Life or livelihood? Mental health concerns for quarantine hotel workers during the COVID-19 pandemic. Front Psychol. (2020) 11:2168. doi: 10.3389/fpsyg.2020.02168
52. Teng YM, Wu KS, Lin KL, Xu D. Mental health impact of COVID-19 on quarantine hotel employees in China. Risk Manag Healthc Policy. (2020) 13:2743–51. doi: 10.2147/RMHP.S286171
53. Wu Y, Zhang C, Liu H, Duan C, Li C, Fan J, et al. Perinatal depressive and anxiety symptoms of pregnant women during the coronavirus disease 2019 outbreak in China. Am J Obstet Gynecol. (2020) 223:240.e1-e9. doi: 10.1016/j.ajog.2020.05.009
54. Papadopoulos A, Nichols ES, Mohsenzadeh Y, Giroux I, Mottola MF, Van Lieshout RJ, et al. Depression in pregnant women with and without COVID-19. BJPsych Open. (2021) 7:e173. doi: 10.1192/bjo.2021.1010
55. Teng YM, Wu KS, Xu D. The association between fear of coronavirus disease 2019, mental health, and turnover intention among quarantine hotel employees in China. Front Public Health. (2021) 9:668774. Available online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.668774 doi: 10.3389/fpubh.2021.668774
56. Mauri M, Oppo A, Montagnani MS, Borri C, Banti S, Camilleri V, et al. Beyond “postpartum depressions”: specific anxiety diagnoses during pregnancy predict different outcomes: results from PND-ReScU. J Affect Disord. (2010) 127:177–84. doi: 10.1016/j.jad.2010.05.015
57. Palumbo G, Mirabella F, Cascavilla Del Re D, Romano G, Gigantesco A. Prevenzione e intervento precoce per il rischio di depressione post partum. Rapporti Istasan. (2016) 16:31.
58. Clavenna A, Seletti E, Cartabia M, Didoni A, Fortinguerra F, Sciascia T, et al. Postnatal depression screening in a paediatric primary care setting in Italy. BMC Psychiatry. (2017) 17:42. doi: 10.1186/s12888-017-1205-6
59. Woody CA Ferrari AJ Siskind DJ Whiteford HA Harris MG A A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J Affect Disord. (2017) 219:86–92. doi: 10.1016/j.jad.2017.05.003
60. Shorey S, Chee CYI, Ng ED, Chan YH, Tam WWS, Chong YS. Prevalence and incidence of postpartum depression among healthy mothers: a systematic review and meta-analysis. J Psychiatr Res. (2018) 104:235–48. doi: 10.1016/j.jpsychires.2018.08.001
61. Okagbue HI, Adamu PI, Bishop SA, Oguntunde PE, Opanuga AA, Akhmetshin EM. Systematic review of prevalence of antepartum depression during the trimesters of pregnancy. Open Access Maced J Med Sci. (2019) 7:1555–60. doi: 10.3889/oamjms.2019.270
62. Camoni L, Mirabella F, Palumbo G, Del Re D, Gigantesco A, Calamandrei G, et al. A screening and treatment programme to deal with perinatal anxiety and depression during the COVID-19 pandemic. Epidemiol Prev. (2020) 44:369–73.
63. Cena L, Mirabella F, Palumbo G, Gigantesco A, Trainini A, Stefana A. Prevalence of maternal antenatal and postnatal depression and their association with sociodemographic and socioeconomic factors: a multicentre study in Italy. J Affect Disord. (2021) 279:217–21. doi: 10.1016/j.jad.2020.09.136
64. Cena L, Palumbo G, Mirabella F, Gigantesco A, Stefana A, Trainini A, et al. Perspectives on early screening and prompt intervention to identify and treat maternal perinatal mental health. Protocol for a prospective multicenter study in Italy. Front Psychol. (2020) 11:365. doi: 10.3389/fpsyg.2020.00365
65. Durankuş F, Aksu E. Effects of the COVID-19 pandemic on anxiety and depressive symptoms in pregnant women: a preliminary study. J Matern-Fetal Neonatal Med. (2022) 35:205–11. doi: 10.1080/14767058.2020.1763946
66. Ostacoli L, Cosma S, Bevilacqua F, Berchialla P, Bovetti M, Carosso AR, et al. Psychosocial factors associated with postpartum psychological distress during the COVID-19 pandemic: a cross-sectional study. BMC Pregnancy Childbirth. (2020) 20:703. doi: 10.1186/s12884-020-03399-5
67. Saccone G, Florio A, Aiello F, Venturella R, De Angelis MC, Locci M, et al. Psychological impact of coronavirus disease 2019 in pregnant women. Am J Obstet Gynecol. (2020) 223:293–5. doi: 10.1016/j.ajog.2020.05.003
68. Zanardo V, Manghina V, Giliberti L, Vettore M, Severino L, Straface G. Psychological impact of COVID-19 quarantine measures in northeastern Italy on mothers in the immediate postpartum period. Int J Gynaecol Obstet. (2020) 150:184–8. doi: 10.1002/ijgo.13249
69. Perzow SED, Hennessey EMP, Hoffman MC, Grote NK, Davis EP, Hankin BL. Mental health of pregnant and postpartum women in response to the COVID-19 pandemic. J Affect Disord Rep. (2021) 4:100123. doi: 10.1016/j.jadr.2021.100123
70. Ravaldi C, Wilson A, Ricca V, Homer C, Vannacci A. Pregnant women voice their concerns and birth expectations during the COVID-19 pandemic in Italy. Women Birth J Aust Coll Midwives. (2021) 34:335–43. doi: 10.1016/j.wombi.2020.07.002
71. Suwalska J, Napierała M, Bogdański P, Łojko D, Wszołek K, Suchowiak S, et al. Perinatal mental health during COVID-19 pandemic: an integrative review and implications for clinical practice. J Clin Med. (2021) 10:2406. doi: 10.3390/jcm10112406
72. Hessami K, Romanelli C, Chiurazzi M, Cozzolino M. COVID-19 pandemic and maternal mental health: a systematic review and meta-analysis. J Matern-Fetal Neonatal Med. (2020) 1–8. doi: 10.1080/14767058.2020.1843155
73. Asai K, Wakashima K, Toda S, Koiwa K. Fear of novel coronavirus disease (COVID-19) among pregnant and infertile women in Japan. J Affect Disord Rep. (2021) 4:100104. doi: 10.1016/j.jadr.2021.100104
74. Dymecka J, Gerymski R, Iszczuk A, Bidzan M. Fear of coronavirus, stress and fear of childbirth in Polish pregnant women during the COVID-19 pandemic. Int J Environ Res Public Health. (2021) 18:13111. doi: 10.3390/ijerph182413111
75. Giesbrecht GF, Rojas L, Patel S, Kuret V, MacKinnon AL, Tomfohr-Madsen L, et al. Fear of COVID-19, mental health, and pregnancy outcomes in the pregnancy during the COVID-19 pandemic study: fear of COVID-19 and pregnancy outcomes. J Affect Disord. (2022) 299:483–91. doi: 10.1016/j.jad.2021.12.057
76. Janik K, Cwalina U, Iwanowicz-Palus G, Cybulski M. An assessment of the level of COVID-19 anxiety among pregnant women in Poland: a cross-sectional study. J Clin Med. (2021) 10:5869. doi: 10.3390/jcm10245869
77. Luo Z, Xue L, Ma L, Liu Z. Comorbid anxiety and depression and related factors among pregnant and postpartum Chinese women during the coronavirus disease 2019 pandemic. Front Psychol. (2021) 4419. doi: 10.3389/fpsyg.2021.701629
78. Fan HSL, Choi EPH, Ko RWT, Kwok JYY, Wong JYH, Fong DYT, et al. COVID-19 related fear and depression of pregnant women and new mothers. Public Health Nurs Boston Mass. (2022) 39:562–71. doi: 10.1111/phn.13035
79. Rashidi Fakari F, Simbar M. Coronavirus pandemic and worries during pregnancy; a letter to editor. Arch Acad Emerg Med. (2020) 8:e21.
80. Grumi S, Provenzi L, Accorsi P, Biasucci G, Cavallini A, Decembrino L, et al. Depression and anxiety in mothers who were pregnant during the COVID-19 outbreak in Northern Italy: the role of pandemic-related emotional stress and perceived social support. Front Psychiatry. (2021) 12:716488. doi: 10.3389/fpsyt.2021.716488
81. Vacaru S, Beijers R, Browne PD, Cloin M, van Bakel H, van den Heuvel MI, et al. The risk and protective factors of heightened prenatal anxiety and depression during the COVID-19 lockdown. Sci Rep. (2021) 11:20261. doi: 10.1038/s41598-021-99662-6
82. Schwartz DA, Graham AL. Potential maternal and infant outcomes from coronavirus 2019-nCoV (SARS-CoV-2) infecting pregnant women: lessons from SARS, MERS, and other human coronavirus infections. Viruses. (2020) 12:194. doi: 10.3390/v12020194
83. Silva WAD, de Sampaio Brito TR, Pereira CR. COVID-19 anxiety scale (CAS): Development and psychometric properties. Curr Psychol. (2020) 1–10. doi: 10.1007/s12144-020-01195-0
84. Mazza MG, Palladini M, De Lorenzo R, Magnaghi C, Poletti S, Furlan R, et al. Persistent psychopathology and neurocognitive impairment in COVID-19 survivors: effect of inflammatory biomarkers at three-month follow-up. Brain Behav Immun. (2021) 94:138–47. doi: 10.1016/j.bbi.2021.02.021
85. Salfi F, Lauriola M, D'Atri A, Amicucci G, Viselli L, Tempesta D, et al. Demographic, psychological, chronobiological, and work-related predictors of sleep disturbances during the COVID-19 lockdown in Italy. Sci Rep. (2021) 11:11416. doi: 10.1038/s41598-021-90993-y
86. Maggi G, Baldassarre I, Barbaro A, Cavallo ND, Cropano M, Nappo R, et al. Age- and gender-related differences in the evolution of psychological and cognitive status after the lockdown for the COVID-19 outbreak: a follow-up study. Ital J Neurol Sci. (2022) 43:1521–32. doi: 10.1007/s10072-021-05768-0
Keywords: COVID-19, depression, peripartum, perinatal mental health, postpartum, pregnancy, women's mental health
Citation: Orsolini L, Pompili S, Mauro A, Salvi V and Volpe U (2022) Fear and anxiety related to COVID-19 pandemic may predispose to perinatal depression in Italy. Front. Psychiatry 13:977681. doi: 10.3389/fpsyt.2022.977681
Received: 24 June 2022; Accepted: 07 July 2022;
Published: 03 August 2022.
Edited by:
Mohammadreza Shalbafan, Iran University of Medical Sciences, IranReviewed by:
Rubia Carla Formighieri Giordani, Federal University of Paraná, BrazilGaia Sampogna, University of Campania Luigi Vanvitelli, Italy
Kun-Shan Wu, Tamkang University, Taiwan
Copyright © 2022 Orsolini, Pompili, Mauro, Salvi and Volpe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laura Orsolini, l.orsolini@staff.univpm.it