
Safety of Biologic-DMARDs in Rheumatic Musculoskeletal Disorders: A Population-Based Study over the First Two Waves of COVID-19 Outbreak

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Objective
2.2. Study Population, Reference Population, and Procedure to Diagnose COVID-19
2.3. Statistical Analysis
3. Results
3.1. Epidemiologic Data
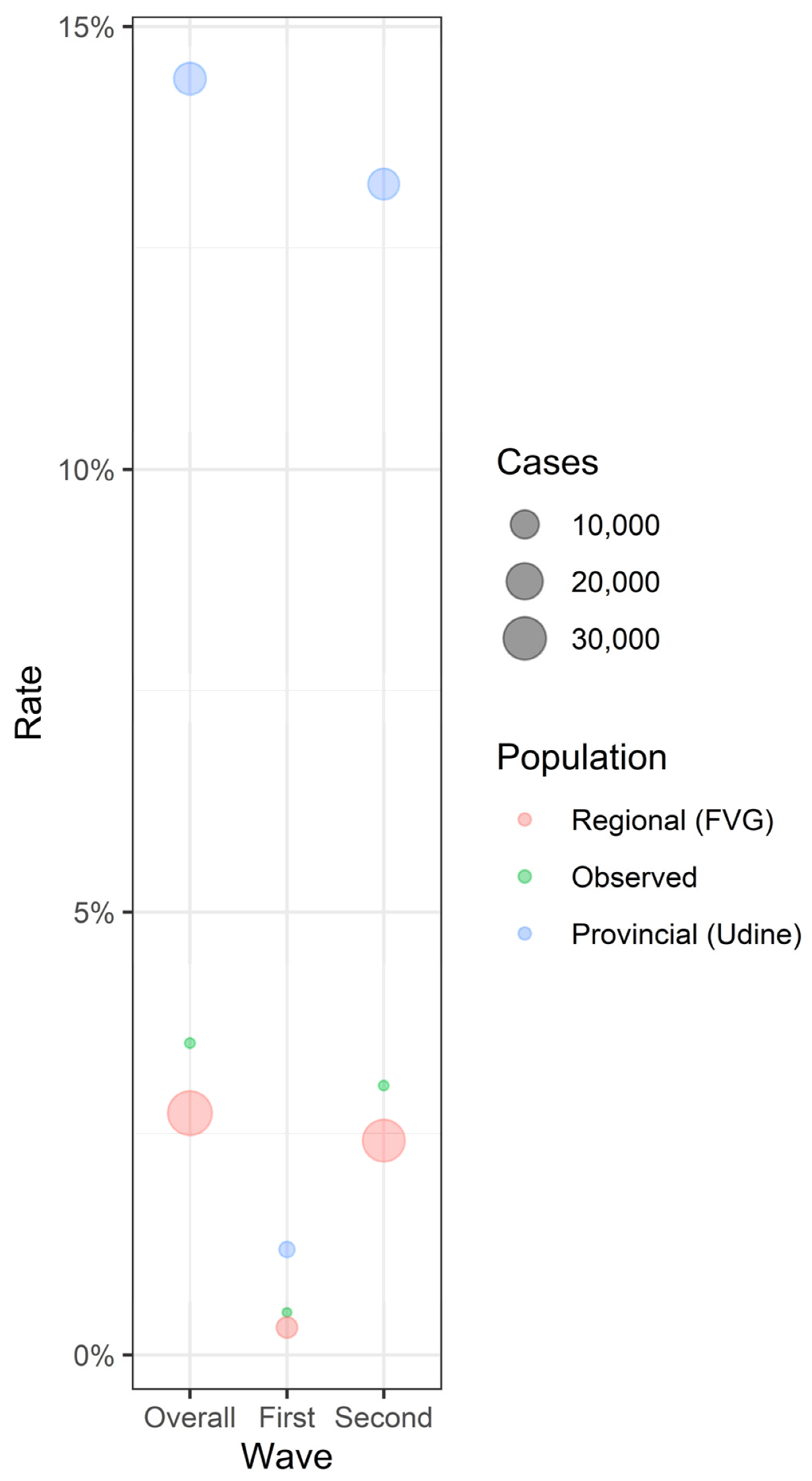
3.2. Comparison with Population Data
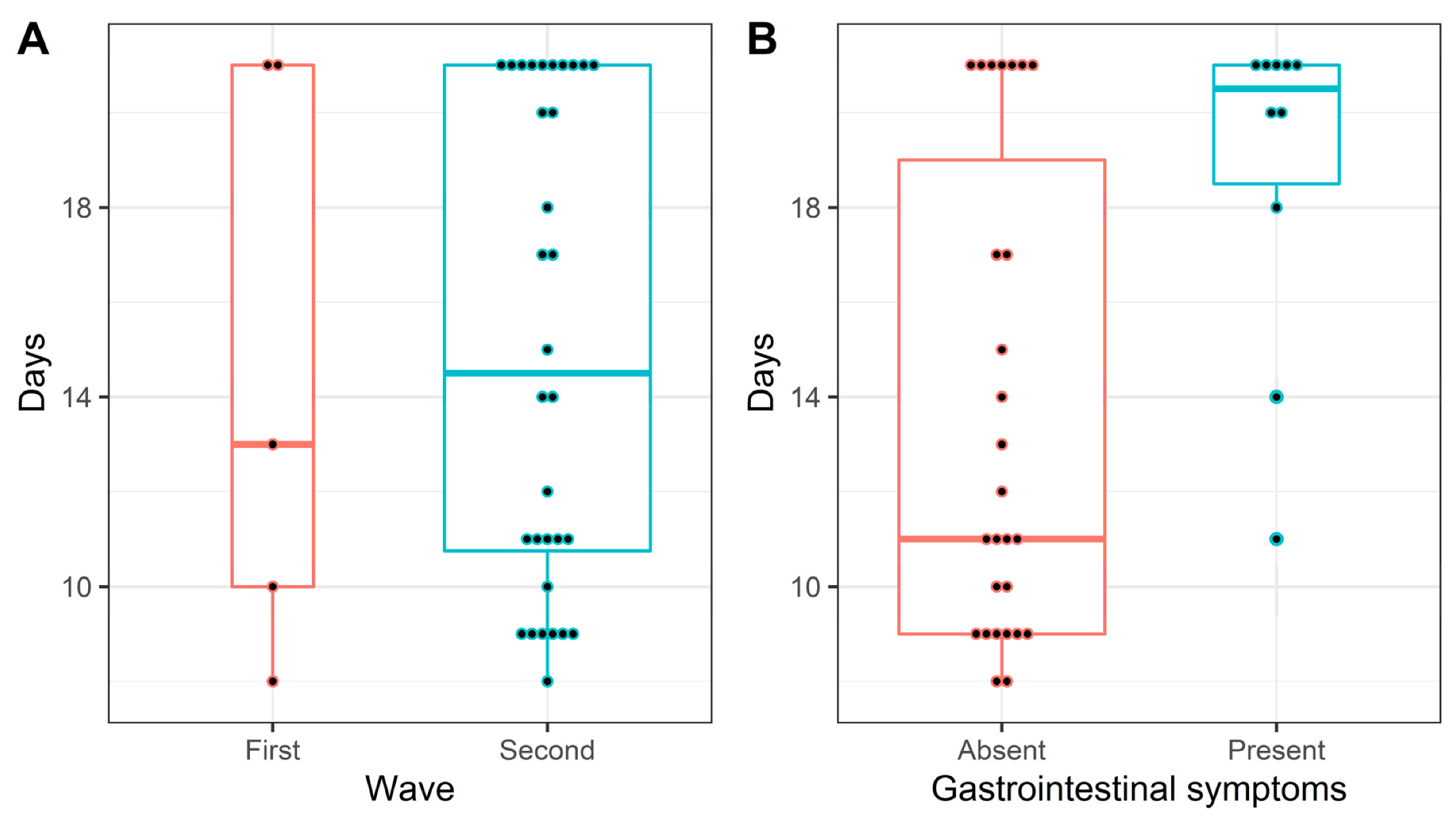
3.3. Characteristics of COVID-19 Patients and Disease Pattern
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baj, J.; Karakuła-Juchnowicz, H.; Teresiński, G.; Buszewicz, G.; Ciesielka, M.; Sitarz, E.; Forma, A.; Karakuła, K.; Flieger, W.; Portincasa, P.; et al. COVID-19: Specific and Non-Specific Clinical Manifestations and Symptoms: The Current State of Knowledge. J. Clin. Med. 2020, 9, 1753. [Google Scholar] [CrossRef] [PubMed]
- Dhar, D.; Mohanty, A. Gut microbiota and COVID-19-possible link and implications. Virus Res. 2020, 285, 198018. [Google Scholar] [CrossRef]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Albini, A.; Di Guardo, G.; Noonan, D.M.; Lombardo, M. The SARS-CoV-2 receptor, ACE-2, is expressed on many different cell types: Implications for ACE-inhibitor- and angiotensin II receptor blocker-based cardiovascular therapies. Intern. Emerg. Med. 2020, 15, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Kamal, M.; Abo Omirah, M.; Hussein, A.; Saeed, H. Assessment and characterisation of post-COVID-19 manifestations. Int. J. Clin. Pract. 2021, 75, e13746. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Davido, B.; Seang, S.; Tubiana, R.; de Truchis, P. Post-COVID-19 chronic symptoms: A postinfectious entity? Clin. Microbiol. Infect. 2020, 26, 1448–1449. [Google Scholar] [CrossRef]
- Gasparotto, M.; Framba, V.; Piovella, C.; Doria, A.; Iaccarino, L. Post-COVID-19 arthritis: A case report and literature review. Clin Rheumatol. 2021, 40, 3357–3362. [Google Scholar] [CrossRef]
- Quartuccio, L.; Sonaglia, A.; Pecori, D.; Peghin, M.; Fabris, M.; Tascini, C.; De Vita, S. Higher levels of IL-6 early after tocilizumab distinguish survivors from nonsurvivors in COVID-19 pneumonia: A possible indication for deeper targeting of IL-6. J. Med. Virol. 2020, 92, 2852–2856. [Google Scholar] [CrossRef]
- Birra, D.; Benucci, M.; Landolfi, L.; Merchionda, A.; Loi, G.; Amato, P.; Licata, G.; Quartuccio, L.; Triggiani, M.; Moscato, P. COVID 19: A clue from innate immunity. Immunol. Res. 2020, 68, 161–168. [Google Scholar] [CrossRef]
- Quartuccio, L.; Fabris, M.; Sonaglia, A.; Peghin, M.; Domenis, R.; Cifù, A.; Curcio, F.; Tascini, C. Interleukin 6, soluble interleukin 2 receptor alpha (CD25), monocyte colony-stimulating factor, and hepatocyte growth factor linked with systemic hyperinflammation, innate immunity hyperactivation, and organ damage in COVID-19 pneumonia. Cytokine 2021, 140, 155438. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Zimba, O.; Gasparyan, A.Y. COVID-19 and the clinical course of rheumatic manifestations. Clin. Rheumatol. 2021, 40, 2611–2619. [Google Scholar] [CrossRef] [PubMed]
- Schett, G.; Manger, B.; Simon, D.; Caporali, R. COVID-19 revisiting inflammatory pathways of arthritis. Nat. Rev. Rheumatol. 2020, 16, 465–470. [Google Scholar] [CrossRef]
- Alunno, A.; Najm, A.; Machado, P.M.; Bertheussen, H.; Burmester, G.R.; Carubbi, F.; de Marco, G.; Giacomelli, R.; Hermine, O.; Isaacs, J.D.; et al. EULAR points to consider on pathophysiology and use of immunomodulatory therapies in COVID-19. Ann. Rheum. Dis. 2021, 80, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Quartuccio, L.; Sonaglia, A.; McGonagle, D.; Fabris, M.; Peghin, M.; Pecori, D.; de Monte, A.; Bove, T.; Curcio, F.; Bassi, F.; et al. Profiling COVID-19 pneumonia progressing into the cytokine storm syndrome: Results from a single Italian Centre study on tocilizumab versus standard of care. J. Clin. Virol. 2020, 129, 104444. [Google Scholar] [CrossRef] [PubMed]
- Benucci, M.; Damiani, A.; Infantino, M.; Manfredi, M.; Quartuccio, L. Old and new antirheumatic drugs for the treatment of COVID-19. Joint Bone Spine 2020, 87, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Favalli, E.G.; Ingegnoli, F.; De Lucia, O.; Cincinelli, G.; Cimaz, R.; Caporali, R. COVID-19 infection and rheumatoid arthritis: Faraway, so close! Autoimmun. Rev. 2020, 19, 102523. [Google Scholar] [CrossRef]
- Scirè, C.A.; Carrara, G.; Zanetti, A.; Landolfi, G.; Chighizola, C.; Alunno, A.; Andreoli, L.; Caporali, R.; Gerli, R.; Sebastiani, G.D.; et al. COVID-19 in rheumatic diseases in Italy: First results from the Italian registry of the Italian Society for Rheumatology (CONTROL-19). Clin. Exp. Rheumatol. 2020, 38, 748–753. [Google Scholar]
- Saadoun, D.; Vieira, M.; Vautier, M.; Baraliakos, X.; Andreica, I.; da Silva, J.A.P.; Sousa, M.; Luis, M.; Khmelinskii, N.; Gracía, J.M.A.; et al. SARS-CoV-2 outbreak in immune-mediated inflammatory diseases: The Euro-COVIMID multicentre cross-sectional study. Lancet Rheumatol. 2021, 3, e481–e488. [Google Scholar] [CrossRef]
- Sanchez-Piedra, C.; Diaz-Torne, C.; Manero, J.; Pego-Reigosa, J.M.; Rúa-Figueroa, Í.; Gonzalez-Gay, M.A.; Gomez-Reino, J.; Alvaro-Gracia, J.M. Clinical features and outcomes of COVID-19 in patients with rheumatic diseases treated with biological and synthetic targeted therapies. Ann. Rheum. Dis. 2020, 79, 988–990. [Google Scholar] [CrossRef]
- Gianfrancesco, M.; Hyrich, K.L.; Al-Adely, S.; Carmona, L.; Danila, M.I.; Gossec, L.; Izadi, Z.; Jacobsohn, L.; Katz, P.; Lawson-Tovey, S.; et al. Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: Data from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann. Rheum. Dis. 2020, 79, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Murtas, R.; Andreano, A.; Gervasi, F.; Guido, D.; Consolazio, D.; Tunesi, S.; Andreoni, L.; Greco, M.T.; Gattoni, M.E.; Sandrini, M.; et al. Association between autoimmune diseases and COVID-19 as assessed in both a test-negative case-control and population case-control design. Autoimmun. Highlights 2020, 11, 15. [Google Scholar] [CrossRef] [PubMed]
- Zen, M.; Fuzzi, E.; Astorri, D.; Saccon, F.; Padoan, R.; Ienna, L.; Cozzi, G.; Depascale, R.; Zanatta, E.; Gasparotto, M.; et al. SARS-CoV-2 infection in patients with autoimmune rheumatic diseases in northeast Italy: A cross-sectional study on 916 patients. J. Autoimmun. 2020, 112, 102502. [Google Scholar] [CrossRef] [PubMed]
- Kow, C.S.; Hasan, S.S. Use of rituximab and the risk of adverse clinical outcomes in COVID-19 patients with systemic rheumatic disease. Rheumatol. Int. 2020, 40, 2117–2118. [Google Scholar] [CrossRef]
- Quartuccio, L.; Treppo, E.; Binutti, M.; Del Frate, G.; De Vita, S. Timing of Rituximab and Immunoglobulin Level Influence the Risk of Death for COVID-19 in ANCA-Associated Vasculitis. Rheumatology 2021, 60, 3476–3477. Available online: https://pubmed.ncbi.nlm.nih.gov/33609106/ (accessed on 4 January 2022). [CrossRef]
- Strangfeld, A.; Schäfer, M.; Gianfrancesco, M.A.; Lawson-Tovey, S.; Liew, J.W.; Ljung, L.; Mateus, E.F.; Richez, C.; Santos, M.J.; Schmajuk, G.; et al. Factors associated with COVID-19-related death in people with rheumatic diseases: Results from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann. Rheum. Dis. 2021, 80, 930–942. [Google Scholar] [CrossRef]
- Quartuccio, L.; Valent, F.; Pasut, E.; Tascini, C.; De Vita, S. Prevalence of COVID-19 among patients with chronic inflammatory rheumatic diseases treated with biologic agents or small molecules: A population-based study in the first two months of COVID-19 outbreak in Italy. Jt. Bone Spine 2020, 87, 439–443. [Google Scholar] [CrossRef]
- I.STAT. Available online: http://dati.istat.it/ (accessed on 23 December 2021).
- Kruskal, W.H.; Wallis, W.A. Use of Ranks in One-Criterion Variance Analysis. J. Am. Stat. Assoc. 1952, 47, 583–621. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 23 December 2021).
- Regression Modeling Strategies Short Course 2021. Available online: https://hbiostat.org/doc/rms/4day.html (accessed on 23 December 2021).
- Landewé, R.B.; Machado, P.M.; Kroon, F.; Bijlsma, H.W.; Burmester, G.R.; Carmona, L.; Combe, B.; Galli, M.; Gossec, L.; Iagnocco, A.; et al. EULAR provisional recommendations for the management of rheumatic and musculoskeletal diseases in the context of SARS-CoV-2. Ann. Rheum. Dis. 2020, 79, 851–858. [Google Scholar] [CrossRef]
- Sarzi-Puttini, P.; Marotto, D.; Caporali, R.; Montecucco, C.M.; Favalli, E.G.; Franceschini, F.; Fredi, M.; Balduzzi, S.; Bazzani, C.; Bongiovanni, S.; et al. Prevalence of COVID infections in a population of rheumatic patients from Lombardy and Marche treated with biological drugs or small molecules: A multicentre retrospective study. J. Autoimmun. 2021, 116, 102545. [Google Scholar] [CrossRef] [PubMed]
- Ruscitti, P.; Conforti, A.; Cipriani, P.; Giacomelli, R.; Tasso, M.; Costa, L.; Caso, F. Pathogenic implications, incidence, and outcomes of COVID-19 in autoimmune inflammatory joint diseases and autoinflammatory disorders. Adv. Rheumatol. 2021, 61, 45. [Google Scholar] [CrossRef] [PubMed]
- Brito, C.A.; Paiva, J.G.; Pimentel, F.N.; Guimarães, R.S.; Moreira, M.R. COVID-19 in patients with rheumatological diseases treated with anti-TNF. Ann. Rheum. Dis. 2021, 80, e62. [Google Scholar] [CrossRef]
- Zhang, M.; Bai, X.; Cao, W.; Ji, J.; Wang, L.; Yang, Y.; Yang, H. The Influence of Corticosteroids, Immunosuppressants and Biologics on Patients With Inflammatory Bowel Diseases, Psoriasis and Rheumatic Diseases in the Era of COVID-19: A Review of Current Evidence. Front Immunol. 2021, 12, 677957. [Google Scholar] [CrossRef]
- Clemente, J.C.; Manasson, J.; Scher, J.U. The role of the gut microbiome in systemic inflammatory disease. BMJ 2018, 360, j5145. [Google Scholar] [CrossRef] [PubMed]
- Manasson, J.; Shen, N.; Garcia Ferrer, H.R.; Ubeda, C.; Iraheta, I.; Heguy, A.; Von Feldt, J.M.; Espinoza, L.R.; Kutzbach, A.G.; Segal, L.N.; et al. Gut Microbiota Perturbations in Reactive Arthritis and Postinfectious Spondyloarthritis. Arthritis Rheumatol. 2018, 70, 242–254. [Google Scholar] [CrossRef] [Green Version]
- Han, C.; Duan, C.; Zhang, S.; Spiegel, B.; Shi, H.; Wang, W.; Zhang, L.; Lin, R.; Liu, J.; Ding, Z.; et al. Digestive Symptoms in COVID-19 Patients With Mild Disease Severity: Clinical Presentation, Stool Viral RNA Testing, and Outcomes. Am. J. Gastroenterol. 2020, 115, 916–923. [Google Scholar] [CrossRef] [PubMed]
- Schettino, M.; Pellegrini, L.; Picascia, D.; Saibeni, S.; Bezzio, C.; Bini, F.; Omazzi, B.F.; Devani, M.; Arena, I.; Bongiovanni, M.; et al. Clinical Characteristics of COVID-19 Patients With Gastrointestinal Symptoms in Northern Italy: A Single-Center Cohort Study. Am. J. Gastroenterol. 2021, 116, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Wang, B.; Zhang, T.; Xu, J.; Shang, S. The mechanism and treatment of gastrointestinal symptoms in patients with COVID-19. Am. J. Physiol. Gastrointest. Liver Physiol. 2020, 319, G245–G252. [Google Scholar] [CrossRef]
- Yeoh, Y.K.; Zuo, T.; Lui, G.C.-Y.; Zhang, F.; Liu, Q.; Li, A.Y.; Chung, A.C.; Cheung, C.P.; Tso, E.Y.; Fung, K.S.; et al. Gut microbiota composition reflects disease severity and dysfunctional immune responses in patients with COVID-19. Gut 2021, 70, 698–706. [Google Scholar] [CrossRef]
- Zuo, T.; Zhang, F.; Lui, G.C.Y.; Yeoh, Y.K.; Li, A.Y.L.; Zhan, H.; Wan, Y.; Chung, A.C.K.; Cheung, C.P.; Chen, N.; et al. Alterations in Gut Microbiota of Patients With COVID-19 During Time of Hospitalization. Gastroenterology 2020, 159, 944–955.e8. [Google Scholar] [CrossRef] [PubMed]
- Ahlawat, S.; Asha; Sharma, K.K. Immunological co-ordination between gut and lungs in SARS-CoV-2 infection. Virus Res. 2020, 286, 198103. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, V.; Capurso, G.; Ianiro, G.; Gasbarrini, A.; Arcidiacono, P.G.; Alvaro, D. Intestinal permeability changes with bacterial translocation as key events modulating systemic host immune response to SARS-CoV-2: A working hypothesis. Dig. Liver Dis. 2020, 52, 1383–1389. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Hall, S.; Vitetta, L. Altered gut microbial metabolites could mediate the effects of risk factors in COVID-19. Rev. Med. Virol. 2021, 31, 1–13. [Google Scholar] [CrossRef]
- Chen, Z.-R.; Liu, J.; Liao, Z.-G.; Zhou, J.; Peng, H.-W.; Gong, F.; Hu, J.-F.; Zhou, Y. COVID-19 and gastroenteric manifestations. World J. Clin. Cases 2021, 9, 4990–4997. [Google Scholar] [CrossRef]
- Katz-Agranov, N.; Zandman-Goddard, G. Autoimmunity and COVID-19—The microbiotal connection. Autoimmun. Rev. 2021, 20, 102865. [Google Scholar] [CrossRef]
- Segal, J.P.; Mak, J.W.Y.; Mullish, B.H.; Alexander, J.L.; Ng, S.C.; Marchesi, J.R. The gut microbiome: An under-recognised contributor to the COVID-19 pandemic? Ther. Adv. Gastroenterol. 2020, 13, 1756284820974914. [Google Scholar] [CrossRef]
- Glintborg, B.; Jensen, D.V.; Engel, S.; Terslev, L.; Pfeiffer Jensen, M.; Hendricks, O.; Østergaard, M.; Rasmussen, S.H.; Adelsten, T.; Colic, A.; et al. Self-protection strategies and health behaviour in patients with inflammatory rheumatic diseases during the COVID-19 pandemic: Results and predictors in more than 12,000 patients with inflammatory rheumatic diseases followed in the Danish DANBIO registry. RMD Open 2021, 7, e001505. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | N. of Observations | Negative (N = 1014) | Positive (N = 37) | Combined (N = 1051) | p-Value |
|---|---|---|---|---|---|
| Age | 1051 | 59 (48–70) | 60 (49–69) | 59 (48–70) | 0.99 |
| Sex (Male) | 1051 | 330 (33%) | 18 (49%) | 348 (33%) | 0.47 |
| RMD | |||||
| RA | 936 | 354 (39%) | 16 (43%) | 370 (40%) | 0.89 |
| PsA | 937 | 269 (30%) | 10 (27%) | 279 (30%) | 0.99 |
| SpA | 934 | 167 (19%) | 9 (24%) | 176 (19%) | 0.73 |
| SLE | 934 | 39 (4%) | 0 (0%) | 39 (4%) | 0.73 |
| Vasculitis | 934 | 73 (8%) | 2 (5%) | 75 (8%) | 0.87 |
| Other | 928 | 19 (2%) | 0 (0%) | 19 (2%) | 0.73 |
| b- or ts-DMARD | 1051 | 0.45 | |||
| Anti-TNF | 611 (60%) | 24 (65%) | 635 (60%) | ||
| JAK inhibitors | 69 (7%) | 4 (11%) | 73 (7%) | ||
| Anti-B cells | 66 (7%) | 1 (3%) | 67 (6%) | ||
| Anti-IL17/23 | 96 (10%) | 6 (16%) | 102 (10%) | ||
| Anti-IL6 | 102 (10%) | 2 (5%) | 104 (10%) | ||
| Other therapies | 70 (7%) | 0 (0%) | 70 (7%) | ||
| Comorbidities | |||||
| Hypertension | 914 | 268 (30%) | 11 (32%) | 279 (31%) | 0.99 |
| Diabetes | 914 | 61 (7%) | 4 (12%) | 65 (7%) | 0.73 |
| Chronic heart disease | 915 | 105 (12%) | 4 (12%) | 109 (12%) | 0.99 |
| History of cancer | 913 | 81 (9%) | 5 (15%) | 86 (9%) | 0.73 |
| Obesity | 896 | 103 (12%) | 6 (19%) | 109 (12%) | 0.73 |
| Duration of last b- or ts-DMARD (months) | 878 | 24 (8–60) | 12 (6–36) | 24 (8–58) | 0.47 |
| Concomitant treatment | |||||
| Methotrexate | 906 | 248 (28%) | 11 (33%) | 259 (29%) | 0.87 |
| Corticosteroids | 911 | 143 (16%) | 3 (9%) | 146 (16%) | 0.73 |
| Hydroxychloroquine | 910 | 69 (8%) | 1 (3%) | 70 (8%) | 0.73 |
| Smoke | 643 | 90 (15%) | 4 (15%) | 94 (15%) | 0.99 |
| Cases (Proportions) | |||
|---|---|---|---|
| Periods | RMD Patients | Province Population | Region Population |
| Overall wave | 37 (0.0352) * | 14,437 (0.1441) | 32,970 (0.0273) |
| First wave | 5 (0.0048) ° | 1190 (0.0119) | 3769 (0.0031) |
| Second wave | 32 (0.0304) * | 13,247 (0.1322) | 29,201 (0.0242) |
| Characteristics | N = 37 |
|---|---|
| Sex (Male) | 18 (49%) |
| Age | 60 (49–69) |
| RMD | |
| Rheumatoid Arthritis | 16 (43%) |
| Psoriatic Arthritis | 10 (27%) |
| Other Seronegative Spondyloarthritis | 9 (24%) |
| Other | 2 (5%) |
| RMD duration (years) | 6 (3–15) |
| Therapy | |
| Corticosteroids | 3 (9%) |
| cs-DMARDs | 15 (39%) |
| Anti-TNF | 24 (65%) |
| Anti-IL17/23 | 6 (16%) |
| JAK-inhibitors | 4 (11%) |
| Anti-IL6 | 2 (5%) |
| Rituximab | 1 (3%) |
| Charlson Comorbidity Index | 0 (0–1) |
| Wave of COVID-19 | |
| First | 5 (14%) |
| Second | 32 (86%) |
| Symptoms | |
| Fever | 26 (70%) |
| Fatigue | 22 (59%) |
| Myalgia | 18 (49%) |
| Arthralgia | 20 (54%) |
| Cough | 13 (35%) |
| Dyspnoea | 7 (19%) |
| GI symptoms | 10 (27%) |
| Anosmia | 10 (27%) |
| Ageusia | 10 (27%) |
| Disease course | |
| Hospitalization | 9 (24%) |
| ICU admission | 2 (5%) |
| Disease flare after COVID-19 | 12 (32%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sonaglia, A.; Comoretto, R.; Pasut, E.; Treppo, E.; Del Frate, G.; Colatutto, D.; Zabotti, A.; De Vita, S.; Quartuccio, L. Safety of Biologic-DMARDs in Rheumatic Musculoskeletal Disorders: A Population-Based Study over the First Two Waves of COVID-19 Outbreak. Viruses 2022, 14, 1462. https://doi.org/10.3390/v14071462
Sonaglia A, Comoretto R, Pasut E, Treppo E, Del Frate G, Colatutto D, Zabotti A, De Vita S, Quartuccio L. Safety of Biologic-DMARDs in Rheumatic Musculoskeletal Disorders: A Population-Based Study over the First Two Waves of COVID-19 Outbreak. Viruses. 2022; 14(7):1462. https://doi.org/10.3390/v14071462
Chicago/Turabian StyleSonaglia, Arianna, Rosanna Comoretto, Enrico Pasut, Elena Treppo, Giulia Del Frate, Donatella Colatutto, Alen Zabotti, Salvatore De Vita, and Luca Quartuccio. 2022. "Safety of Biologic-DMARDs in Rheumatic Musculoskeletal Disorders: A Population-Based Study over the First Two Waves of COVID-19 Outbreak" Viruses 14, no. 7: 1462. https://doi.org/10.3390/v14071462