
Incidence of Pneumothorax and Pneumomediastinum in 497 COVID-19 Patients with Moderate–Severe ARDS over a Year of the Pandemic: An Observational Study in an Italian Third Level COVID-19 Hospital

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
- -
- The incidence of PNX/PNM in COVID-19 patients over a year, as the number of patients with PNX/PNM from COVID-19 patients, and as the number of barotrauma events during 1000 days of non-invasive or invasive positive-pressure ventilation;
- -
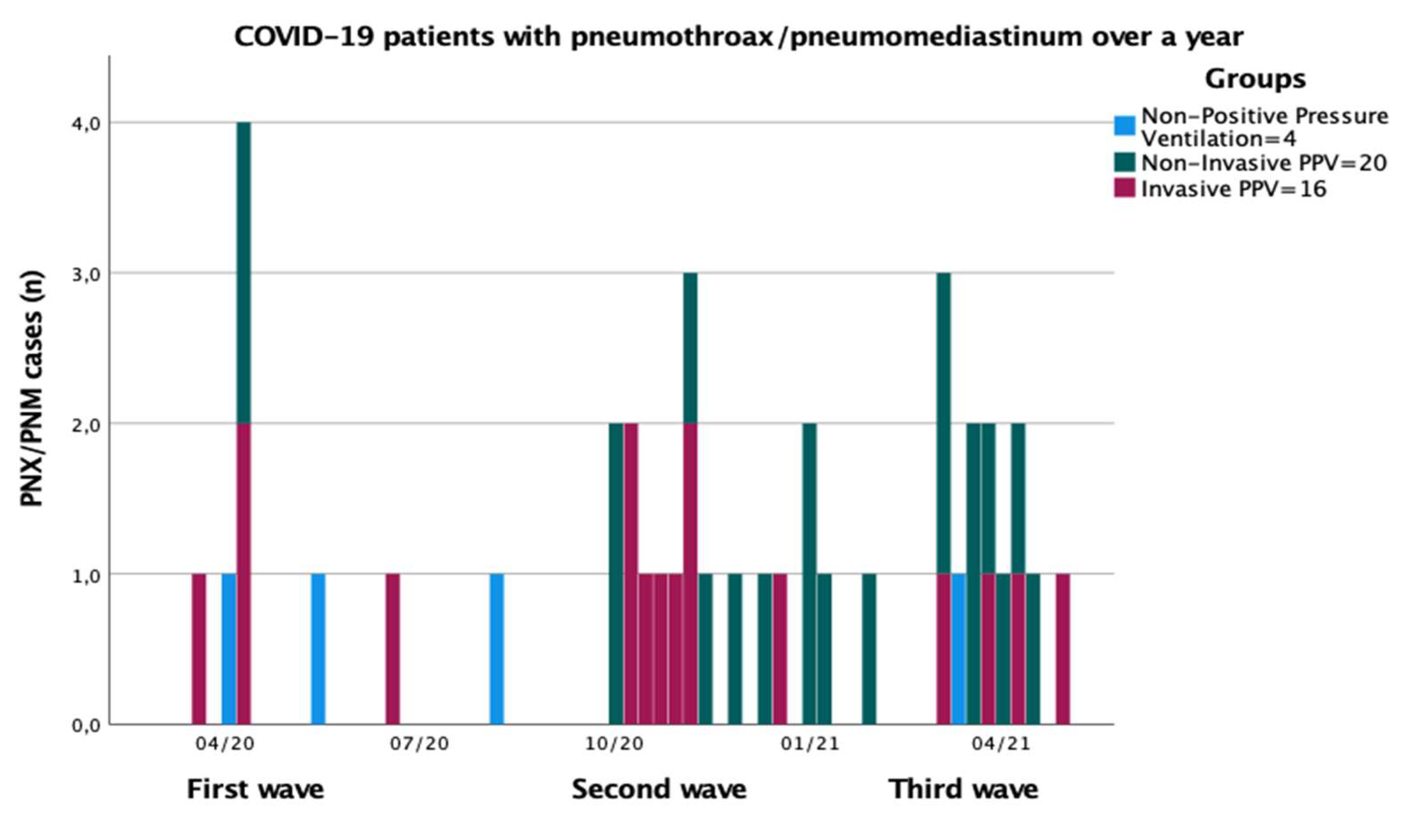
- The incidence between the three waves of COVID-19 during a year of the pandemic;
- -
- The predictive factors associated with the development of PNX/PNM in COVID-19 patients.
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Statistical Analysis
3. Results
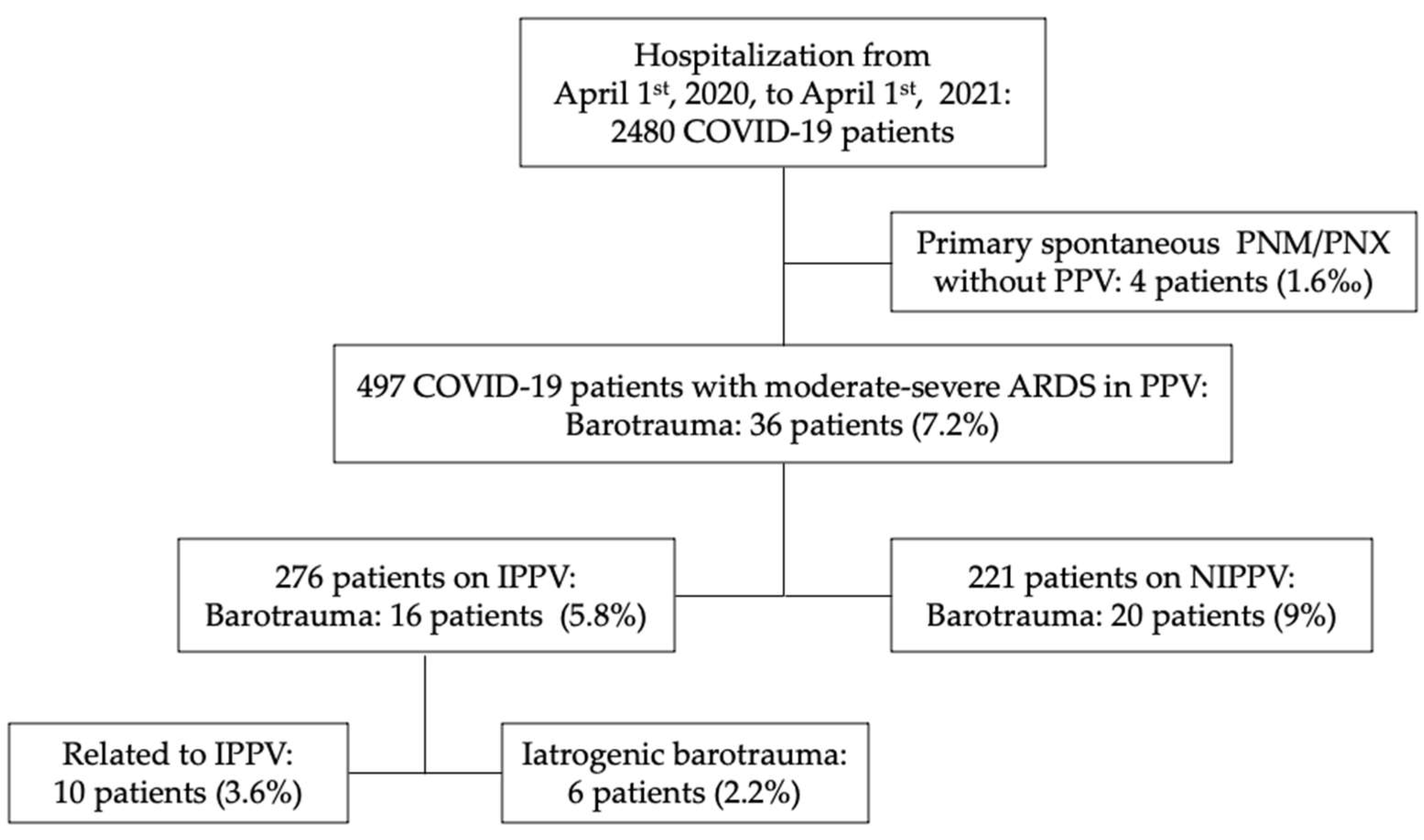
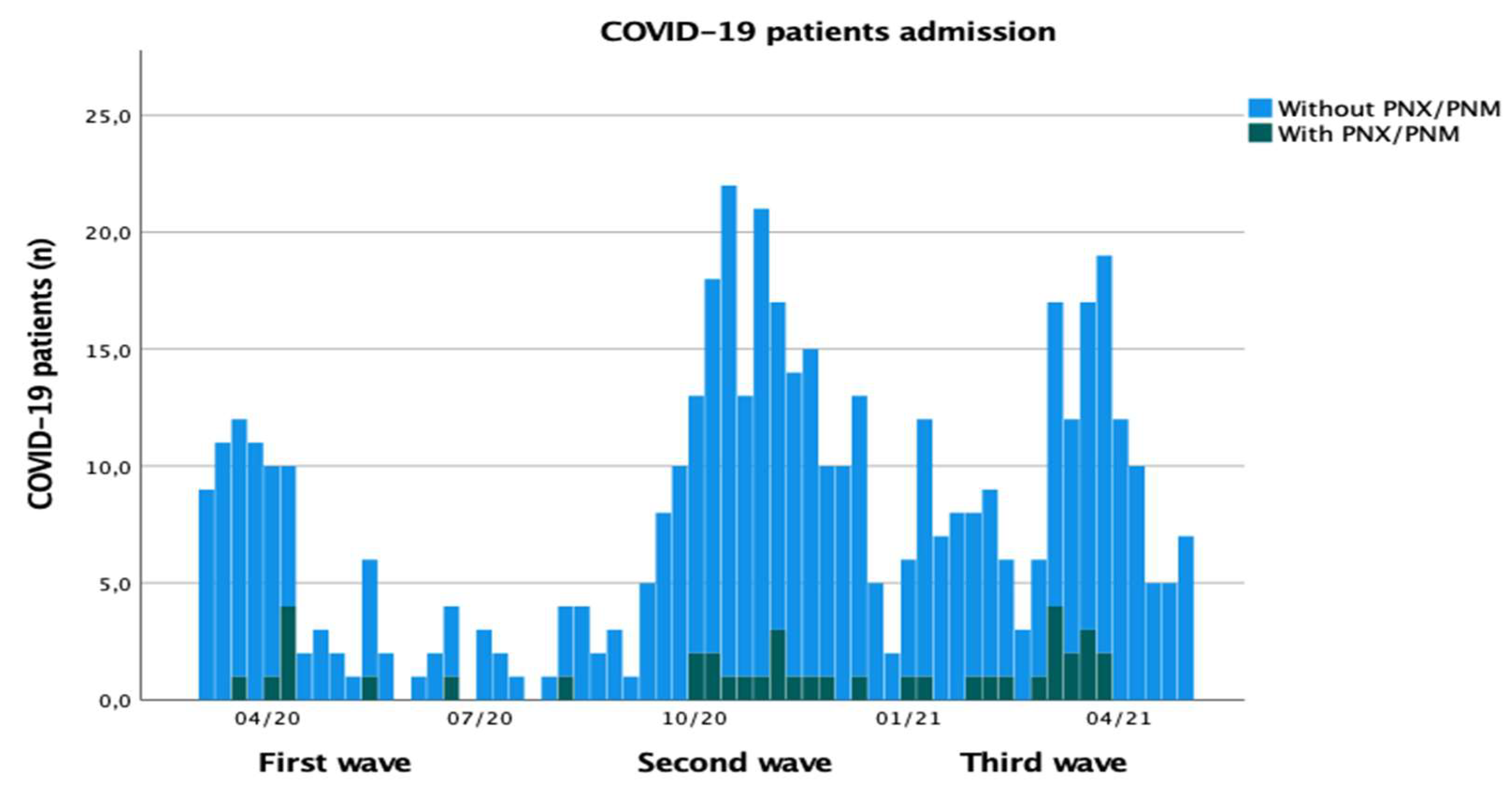
3.1. Incidence of Barotrauma in All COVID-19 Patients Admitted during a Year
3.2. Incidence of Barotrauma in COVID-19 Patients Treated with PPV
3.3. Incidence of Barotrauma Due to Non-Invasive PPV
3.4. Incidence of Barotrauma Due to Invasive PPV
3.5. Barotrauma versus Non-Barotrauma Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Coronavirus Disease (COVID-19) Dashboard; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization (WHO). Infection Prevention and Control Guidance for Long-Term Care Facilities in the Context of COVID-19; World Health Organisation: Geneva, Switzerland, 2020; pp. 1–5. [Google Scholar]
- Privitera, D.; Angaroni, L.; Capsoni, N.; Forni, E.; Pierotti, F.; Vincenti, F.; Bellone, A. Flowchart for Non-Invasive Ventilation Support in COVID-19 Patients from a Northern Italy Emergency Department. Intern. Emerg. Med. 2020, 15, 767–771. [Google Scholar] [CrossRef]
- Kassirian, S.; Taneja, R. Sanjay Mehta Diagnosis and Management of Acute Respiratory Distress Syndrome in a Time of COVID-19. CMAJ 2021, 193, E761–E768. [Google Scholar] [CrossRef]
- Cruz, F.F.; Ball, L.; Rocco, P.R.M.; Pelosi, P. Ventilator-Induced Lung Injury during Controlled Ventilation in Patients with Acute Respiratory Distress Syndrome: Less Is Probably Better. Expert Rev. Respir. Med. 2018, 12, 403–414. [Google Scholar] [CrossRef]
- Alessandri, F.; Pugliese, F.; Ranieri, V.M. The Role of Rescue Therapies in the Treatment of Severe ARDS. Respir. Care 2018, 63, 92–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belletti, A.; Palumbo, D.; Zangrillo, A.; Fominskiy, E.V.; Franchini, S.; Dell’Acqua, A.; Marinosci, A.; Monti, G.; Vitali, G.; Colombo, S.; et al. Predictors of Pneumothorax/Pneumomediastinum in Mechanically Ventilated COVID-19 Patients. J. Cardiothorac. Vasc. Anesth. 2021, 35, 3642–3651. [Google Scholar] [CrossRef]
- Hamouri, S.; Alhazymeh, A.; Syaj, S. Pulmonary Barotrauma in COVID-19 Patients: Invasive versus Noninvasive Positive Pressure Ventilation. Int. J. Gen. Med. 2021, 14, 2017–2032. [Google Scholar] [CrossRef]
- Jones, E.; Gould, A.; Pillay, T.D.; Khorasanee, R.; Sykes, R.; Bazo-Alvarez, J.C.; Cox, C.; Shurovi, B.; Isted, A.; Simpson, T.; et al. Subcutaneous Emphysema, Pneumomediastinum, and Pneumothorax in Critically Ill Patients with Coronavirus Disease 2019: A Retrospective Cohort Study. Crit. Care Explor. 2020, 2, e0210. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, G.; Zhan, C.; Rosenberg, N.; Azour, L.; Wickstrom, M.; Mason, D.M.; Thomas, K.M.; Moore, W.H. Increased Incidence of Barotrauma in Patients with COVID-19 on Invasive Mechanical Ventilation. Radiology 2020, 297, E252–E262. [Google Scholar] [CrossRef] [PubMed]
- Ojha, V.; Mani, A.; Pandey, N.N.; Sharma, S.; Kumar, S. CT in Coronavirus Disease 2019 (COVID-19): A Systematic Review of Chest CT Findings in 4410 Adult Patients. Eur. Radiol. 2020, 30, 6129–6138. [Google Scholar] [CrossRef]
- Akdogan, R.E.; Mohammed, T.; Syeda, A.; Jiwa, N.; Ibrahim, O.; Mutneja, R. Pneumothorax in Mechanically Ventilated Patients with COVID-19 Infection. Case Rep. Crit. Care 2021, 2021. [Google Scholar] [CrossRef]
- Martinelli, A.W.; Ingle, T.; Newman, J.; Nadeem, I.; Jackson, K.; Lane, N.D.; Melhorn, J.; Davies, H.E.; Rostron, A.J.; Adeni, A.; et al. COVID-19 and Pneumothorax: A Multicentre Retrospective Case Series. Eur. Respir. J. 2020, 56. [Google Scholar] [CrossRef]
- Putukian, M. Pneumothorax and Pneumomediastinum. Clin. Sports Med. 2004, 23, 443–454. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, N.D.; Fan, E.; Camporota, L.; Antonelli, M.; Anzueto, A.; Beale, R.; Brochard, L.; Brower, R.; Esteban, A.; Gattinoni, L.; et al. The Berlin Definition of ARDS: An Expanded Rationale, Justification, and Supplementary Material. Intensive Care Med. 2012, 38, 1573–1582. [Google Scholar] [CrossRef]
- Griffiths, M.J.D.; McAuley, D.F.; Perkins, G.D.; Barrett, N.; Blackwood, B.; Boyle, A.; Chee, N.; Connolly, B.; Dark, P.; Finney, S.; et al. Guidelines on the Management of Acute Respiratory Distress Syndrome. BMJ Open Respir. Res. 2019, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meade, M.O.; Cook, D.J.; Guyatt, G.H.; Slutsky, A.S.; Arabi, Y.M.; Cooper, D.J.; Davies, A.R.; Hand, L.E.; Zhou, Q.; Thabane, L.; et al. Ventilation Strategy Using Low Tidal Volumes, Recruitment Maneuvers, and High Positive End-Expiratory Pressure for Acute Lung Injury and Acute Respiratory Distress Syndrome: A Randomized Controlled Trial. JAMA -J. Am. Med Assoc. 2008, 299, 637–645. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, D.A. Lung Ultrasound in the Critically Ill. Ann. Intensive Care 2014, 30, 183–184. [Google Scholar] [CrossRef] [Green Version]
- Falasca, L.; Nardacci, R.; Colombo, D.; Lalle, E.; di Caro, A.; Nicastri, E.; Antinori, A.; Petrosillo, N.; Marchioni, L.; Biava, G.; et al. Postmortem Findings in Italian Patients with COVID-19: A Descriptive Full Autopsy Study of Cases with and without Comorbidities. J. Infect. Dis. 2020, 222, 1807–1815. [Google Scholar] [CrossRef] [PubMed]
- Martines, R.B.; Ritter, J.M.; Matkovic, E.; Gary, J.; Bollweg, B.C.; Bullock, H.; Goldsmith, C.S.; Silva-Flannery, L.; Seixas, J.N.; Reagan-Steiner, S.; et al. Pathology and Pathogenesis of SARS-CoV-2 Associated with Fatal Coronavirus Disease, United States. Emerg. Infect. Dis. 2020, 26, 2005–2015. [Google Scholar] [CrossRef]
- Wintermark, M.; Schnyder, P. The Macklin Effect: A Frequent Etiology for Pneumomediastinum in Severe Blunt Chest Trauma. Chest 2001, 120, 543–547. [Google Scholar] [CrossRef] [Green Version]
- Chassagnon, G.; Favelle, O.; Derogis, V.; Cottier, J.P. Spontaneous Pneumomediastinum Due to the Macklin Effect: Less Is More. Intern. Emerg. Med. 2015, 10, 759–761. [Google Scholar] [CrossRef] [Green Version]
- Miró, Ò. Frequency, Risk Factors, Clinical Characteristics, and Outcomes of Spontaneous Pneumothorax in Patients With Coronavirus Disease 2019. Chest 2021, 159, 1241–1255. [Google Scholar] [CrossRef] [PubMed]
- Lal, A.; Mishra, A.K.; Akhtar, J.; Nabzdyk, C. Pneumothorax and Pneumomediastinum in COVID-19 Acute Respiratory Distress Syndrome. Monaldi Arch. Chest Dis. 2021, 91, 91. [Google Scholar] [CrossRef]
- Grieco, D.L.; Menga, L.S.; Eleuteri, D.; Antonelli, M. Patient Self-Inflicted Lung Injury: Implications for Acute Hypoxemic Respiratory Failure and ARDS Patients on Non-Invasive Support. Minerva Anestesiol. 2019, 85, 1014–1023. [Google Scholar] [CrossRef] [PubMed]
- Terzi, E. Acute Respiratory Distress Syndrome and Pneumonia. Jpn. J. Anesthesiol. 2013, 62, 547–556. [Google Scholar] [CrossRef]
- Chopra, A.; Al-Tarbsheh, A.H.; Shah, N.J.; Yaqoob, H.; Hu, K.; Feustel, P.J.; Ortiz-Pacheco, R.; Patel, K.M.; Oweis, J.; Kozlova, N.; et al. Pneumothorax in Critically Ill Patients with COVID-19 Infection: Incidence, Clinical Characteristics and Outcomes in a Case Control Multicenter Study. Respir. Med. 2021, 184, 106464. [Google Scholar] [CrossRef]
- Belletti, A.; Landoni, G.; Zangrillo, A. Pneumothorax and Barotrauma in Invasively Ventilated Patients with COVID-19. Respir. Med. 2021, 187, 106552. [Google Scholar] [CrossRef]
- Chen, K.Y.; Jerng, J.S.; Liao, W.Y.; Ding, L.W.; Kuo, L.C.; Wang, J.Y.; Yang, P.C. Pneumothorax in the ICU: Patient Outcomes and Prognostic Factors. Chest 2002, 122, 678–683. [Google Scholar] [CrossRef]
- Pnömotoraks, Ü.; Yıllık, İ.; Özalp, A.; Sevdi, M.S.; Erkalp, K.; Selcan, A.; Gümü, F.; Win, M. Pneumothorax in the Intensive Care Unit: Retrospective Analysis of Two Years’ Experience. Bagcilar Med Bull. 2019, 5, 1. [Google Scholar]
- Galbois, A.; Zorzi, L.; Meurisse, S.; Kernaéis, S.; Margetis, D.; Alves, M.; Ait-Oufella, H.; Baudel, J.L.; Offenstadt, G.; Maury, E.; et al. Outcome of Spontaneous and Iatrogenic Pneumothoraces Managed with Small-Bore Chest Tubes. Acta Anaesthesiol. Scand. 2012, 56, 507–512. [Google Scholar] [CrossRef]
- Arnaud de Lassence, J.-F.T. Pneumothorax in the Intensive Care Unit: Incidence, Risk Factors, and Outcome. Anesthesiology 2006, 50, 221–222. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PNX/PNM Group (n = 36) | Non-PNX/PNM Group (n = 461) | p-Value a | |
|---|---|---|---|
| Age, median (IQR) | 61.5 (55.7–71.5) | 65 (57–74) | 0.280 |
| Male, n (%) | 29 (80.5%) | 340 (74%) | |
| Female, n (%) | 7 (19.4%) | 121 (26%) | |
| BMI, kg/m2, median (IQR) | 26.9 (26–29.4) | 27.8 (25.4–31.1) | 0.286 |
| SOFA score *, median (IQR) | 5.5 (3–7.7) | 4 (2–7) | 0.209 |
| APACHE II score *, median (IQR) | 11 (8–18) | 9 (7–16) | 0.394 |
| Comorbidities, n (%) | |||
| Arterial hypertension | 23 (64%) | 248 (53.8%) | 0.423 |
| Other cardiopathies | 7 (19.4%) | 106 (23%) | 0.949 |
| Diabetes | 5 (13.8%) | 74 (16%) | 0.271 |
| Kidney disease (stage 3–5 of CKD) | 1 (2.8%) | 21 (4.5%) | 0.438 |
| Moderate to severe chronic liver disease | 0 (0.0%) | 5 (1.1%) | 0.485 |
| Chronic pulmonary diseases ** | 6 (16.7%) | 58 (12.5%) | 0.582 |
| Neoplasm *** | 3 (8.3%) | 29 (6.3%) | 0.974 |
| Previous surgery in last month | 2 (5.5%) | 12 (2.6%) | 0.396 |
| Previous hospitalization in last six months | 3 (8.3%) | 24 (5.2%) | 0.932 |
| Obesity **** | 11 (30.5%) | 163 (35.4%) | 0.147 |
| Chronic neurological disorders | 0 (0.0%) | 38 (8.2%) | 0.446 |
| Autoimmune disease | 3 (8.3%) | 49 (10.7%) | 0.508 |
| Other chronic disease | 7 (19.4%) | 61 (13.2%) | 0.436 |
| Outcome at 30 days from barotrauma | |||
| Discharged, patients (%) | 19 (52.8%) | 289 (62.6%) | |
| Mortality, patients (%) | 17 (47.2%) | 172 (37.3%) | 0.429 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tetaj, N.; Garotto, G.; Albarello, F.; Mastrobattista, A.; Maritti, M.; Stazi, G.V.; Marini, M.C.; Caravella, I.; Macchione, M.; De Angelis, G.; et al. Incidence of Pneumothorax and Pneumomediastinum in 497 COVID-19 Patients with Moderate–Severe ARDS over a Year of the Pandemic: An Observational Study in an Italian Third Level COVID-19 Hospital. J. Clin. Med. 2021, 10, 5608. https://doi.org/10.3390/jcm10235608
Tetaj N, Garotto G, Albarello F, Mastrobattista A, Maritti M, Stazi GV, Marini MC, Caravella I, Macchione M, De Angelis G, et al. Incidence of Pneumothorax and Pneumomediastinum in 497 COVID-19 Patients with Moderate–Severe ARDS over a Year of the Pandemic: An Observational Study in an Italian Third Level COVID-19 Hospital. Journal of Clinical Medicine. 2021; 10(23):5608. https://doi.org/10.3390/jcm10235608
Chicago/Turabian StyleTetaj, Nardi, Gabriele Garotto, Fabrizio Albarello, Annelisa Mastrobattista, Micaela Maritti, Giulia Valeria Stazi, Maria Cristina Marini, Ilaria Caravella, Manuela Macchione, Giada De Angelis, and et al. 2021. "Incidence of Pneumothorax and Pneumomediastinum in 497 COVID-19 Patients with Moderate–Severe ARDS over a Year of the Pandemic: An Observational Study in an Italian Third Level COVID-19 Hospital" Journal of Clinical Medicine 10, no. 23: 5608. https://doi.org/10.3390/jcm10235608