
Safety of Short-Term Treatments with Oral Chloroquine and Hydroxychloroquine in Patients with and without COVID-19: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Selection Process
2.3. Data Collection and Data Items
2.4. Quality Assessment, Risk of Bias in Individual Studies and across Studies
2.5. Data Synthesis and Summary Measures
2.5.1. Case Series, Case Reports, and Case-Control Studies
2.5.2. Cross-Sectional, Cohort, and Randomised Studies
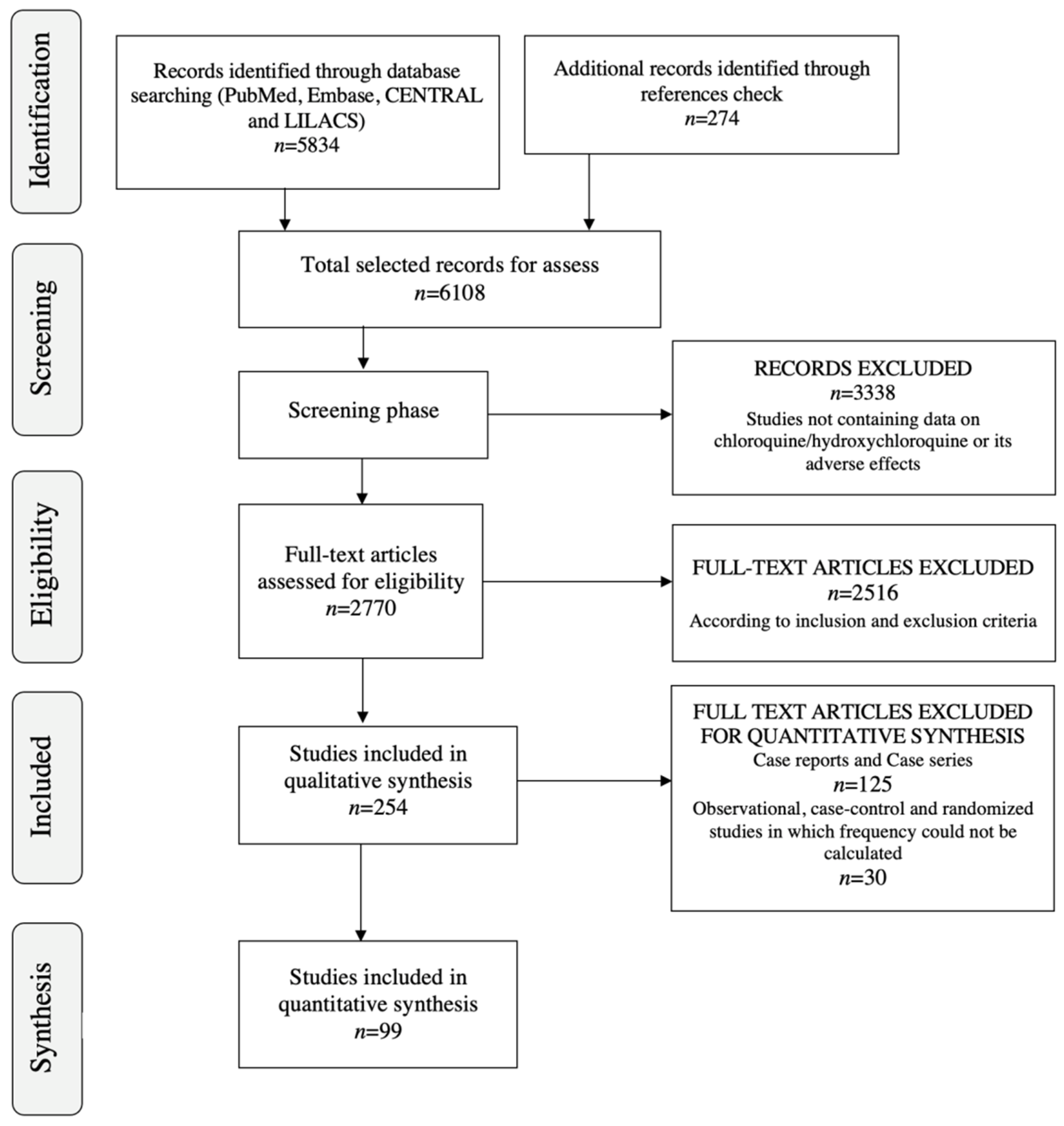
3. Results
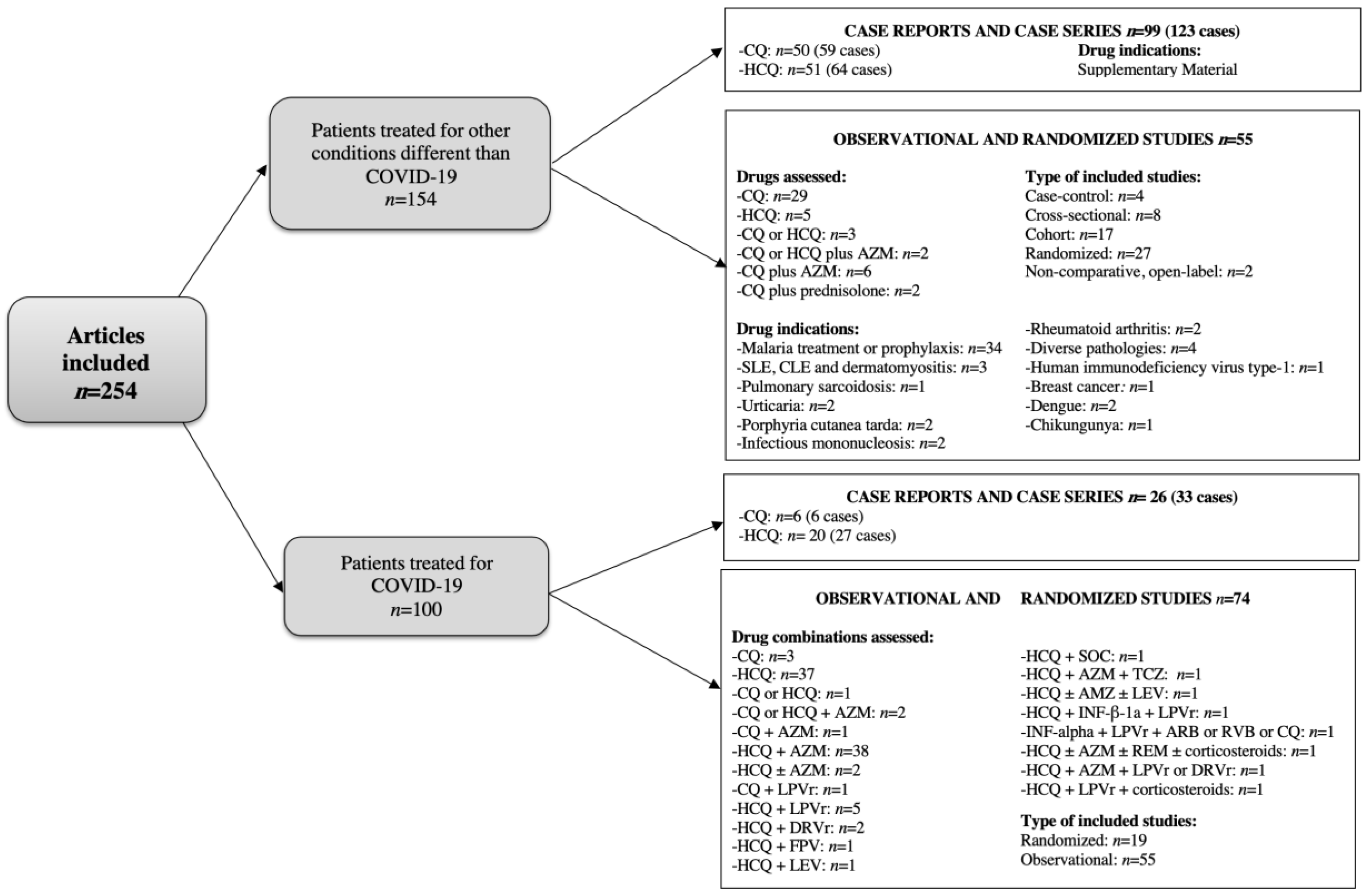
3.1. Study Characteristics and Results of Individual Studies
3.1.1. Patients Treated for Conditions Other Than COVID-19
Case and Case Series Reports
Case-Control, Cross-Sectional, Cohort, and Randomised Studies
3.1.2. Patients Treated for COVID-19
Case and Case Series Reports
Case-Control, Cross-Sectional, Cohort, and Randomised Studies

{kind=link}
{kind=link}
| Organ Affected | N° of Patients (n° of Studies) | Adverse Effect (N° of Patients) (First Author, Year) | Indication of HCQ (n° of Patients) | Long-Term Consequences (n° of Patients) |
|---|---|---|---|---|
| Dermatological | 41 (28) | DRESS (3) (Volpe A et al., 2008, Randhawa A et al., 2018, Girijala RL et al., 2019) [48,60,62] | Seronegative polyarthritis (2) Suspected Sjögren’s like process (1) | Resolution (3) |
| Severe pruritus (1) (Gül U et al., 2006) [45] | Discoid lupus erythematosus (1) | Resolution (1) | ||
| Pemphigus vulgaris (1) (Ghaffarpour G et al., 2006) [44] | Rheumatoid arthritis (1) | After 3 w the lesions cleared with only a mild post-inflammatory hyperpigmentation (1) | ||
| Sweet’s syndrome (1) (Manzo C et al., 2019) [63] | Sjögren syndrome (1) | Resolution (1) | ||
| Inverse psoriasis (1) (Ullah A et al., 2019) [64] | Rheumatoid arthritis (1) | Resolution (1) | ||
| Mild cutaneous eruptions (1) (Matsuda T et al., 2017) [57] | Lupus erythematosus (1) | Resolution (1) | ||
| AGEP (11) (Assier-Bonnet et al., 1996, Evans CC et al., 2004, Atzori L et al., 2007, Bailey K et al., 2013, Soria A et al., 2015, Pearson KC et al., 2016, Mercogliano C et al., 2018, Matsuda-Hirose H et al., 2020) [38,43,47,51,54,55,59,65] | SLE and related disorders (3) NA (1) Erythematous facial dermatitis (1) Photosensitivity (1) Arthritis and related rheumatic disorders (4) Mucinosis (1) | Resolution (10) NA (1) | ||
| Acute pustular psoriasis (1) (Welsch MJ et al., 2003) [42] | Sjögren syndrome (1) | Resolution (1) | ||
| Stevens-Johnson syndrome (1) (Leckie MJ et al., 2002) [41] | Rheumatoid arthritis (1) | The rash improved but persisted (1) | ||
| Erythema multiforme (1) (Abou Assalie N et al., 2017) [56] | SLE (1) | Resolution (1) | ||
| Fatal toxic epidermal necrolysis (2) (Murphy M et al., 2001, Cameron MC et al., 2014) [40,52] | Seropositive nodular rheumatoid disease (1) SLE (1) | Death (2) | ||
| Psoriasis (1) (Gray RG et al., 1985) [34] | Seronegative rheumatoid arthritis (1) | Resolution (1) | ||
| Severe psoriasis exacerbation (1) (Luzar MJ et al., 1982) [31] | Psoriatic arthropathy (1) | Resolution (1) | ||
| Hypersensitivity rash (5) (Mates M et al., 2006, Awad P et al., 2013) [46,50] | Arthritis and related rheumatic disorders (4) Chronic cutaneous lupus (1) | Resolution (1) NA (4) | ||
| Erythema annulare centrifugum (1) (Hudson LD et al., 1985) [35] | Suspected SLE (1) | Resolution (1) | ||
| Pustular eruption (1) (Pastushenko I et al., 2015) [53] | Rheumatoid arthritis (1) | Resolution (1) | ||
| Photosensitivity (2) (Soria A et al., 2015) [54] | Rheumatism (1) Autoimmune bullous skin disease (1) | NA (2) | ||
| AGEP/DRESS (1) (Soria A et al., 2015) [54] | Granuloma annulare (1) | Resolution (1) | ||
| Urticaria (2) (Soria A et al., 2015) [54] | Jessner-Kanof (1) Cutaneous lupus erythematous (1) | Resolution (2) | ||
| MPE (2) (Soria A et al., 2015) [54] | Gougerot-Sjögren syndrome (1) Cutaneous lupus erythematous (1) | Resolution (2) | ||
| Generalised pustular rash (1) (Lotem M et al., 1990) [36] | Pemphigus erythematosus (1) | Resolution (1) | ||
| Psychiatric | 2 (2) | Psychosis (1) (Ward WQ et al., 1985) [74] | Lupus erythematosus (1) | Resolution (1) |
| Auditory and visual hallucination (1) (Ganjei Z et al., 2021) [125] | Discoid lupus erythematosus (1) | Resolution (1) | ||
| Neurologic | 1 (1) | Significant psychomotor agitation (1) (Manzo C et al., 2017) [63] | Rheumatoid arthritis (1) | Resolution (1) |
| Cardiac | 3 (3) | Complete heart block (1) (Comín-Colet J et al., 2001) [96] | SLE (1) | Resolution (1) |
| Implanted pacemaker failure (1) (Huang PH et al., 2003) [97] | Rheumatoid arthritis (1) | Resolution (1) | ||
| QT-interval prolongation (1) Morgan ND et al., 2013 [99] | SLE (1) | QT relatively normal after a year (1) | ||
| Hematologic and metabolic | 4 (4) | Hypoglycaemic coma (1) (Shojania K et al., 1999) [101] | Rheumatoid polyarthritis (1) | Resolution (1) |
| Hypoglycaemia (1) (Winter EM et al., 2011) [102] | Osteoarthritis (1) | Resolution (1) | ||
| Thrombocytopaenia (1) (Demir D et al., 2014) [104] | Used erroneously as a pain killer (1) | Resolution (1) | ||
| Thrombotic thrombocytopaenic purpura (1) (Fromm LM et al., 2017) [105] | Rheumatoid arthritis (1) | Death related to cardiac failure (1) | ||
| Hepatic | 4 (4) | Severe acute hepatitis (1) (Giner Galvañ V et al., 2007) [111] | Arthritis (1) | Resolution (1) |
| Liver injury (1) (Sunkara B et al., 2018) [112] | Subacute cutaneous lupus erythematosus (1) | Resolution (1) | ||
| Fulminant hepatic failure (1) (Makin AJ et al., 1994) [114] | SLE (1) | Death (1) | ||
| Bullous rash and acute hepatitis (1) (Kutz DC et al., 1995) [115] | SLE (1) | Resolution (1) | ||
| Other | 6 (6) | Porphyria variegata precipitation (1) (Baler GR et al., 1976) [116] | SLE (1) | Resolution (1) |
| Severe vacuolar myopathy (1) (Bolaños-Meade J et al., 2005) [119] | cGVHD (1) | Resolution (1) | ||
| Anaphylaxis (1) (Donado CD et al., 2010) [121] | SLE (1) | Resolution (1) | ||
| Two episodes of urinary incontinence (1) (Carnovale C et al., 2013) [122] | Rheumatoid arthritis (1) | Resolution (1) | ||
| Diffuse interstitial lung disease (1) (Català R et al., 2015) [123] | Polymorphic light eruption (1) | Resolution (1) | ||
| Acute eosinophilic pneumonia (1) (Ishiguro Y et al., 2019) [124] | Chilblain lupus erythematosus (1) | Resolution (1) | ||
| Sense organs | 3 (3) | Severe positional vertigo (1) (Prince DS et al., 1975) [107] | Rheumatoid arthritis (1) | Resolution (1) |
| Severe vestibular toxicity (1) (Malik MK et al., 1977) [108] | Malaria (1) | Bilateral complete canal paresis (1) | ||
| Complete ageusia (1) (Fleury O et al., 2009) [110] | SLE (1) | Resolution (1) |
| Organ Affected | N° of Patients (n° of Studies) | Adverse Effect (n° of Patients) (First Author, Year) | Indication of CQ (n° of Patients) | Long-Term Consequences (n° of Patients) |
|---|---|---|---|---|
| Dermatological | 12 (12) | Exacerbation of psoriasis and arthritis (1) (Fisher S, 1961) [27] | Psoriasis (1) | Death due to toxaemia from staphylococcic peritonitis (1) |
| Eczema (1) (Skog E, 1975) [28] | Malaria prophylaxis (1) | NA (1) | ||
| Toxic epidermal necrolysis (1) (Kanwar AJ, 1976) [29] | Suspected malaria (1) | Resolution (1) | ||
| Exacerbation of psoriasis (1) (Olsen TG, 1981) [30] | Malaria (1) | Resolution (1) | ||
| Severe pruritus (1) (Spencer HC, 1982) [32] | Malaria (1) | Resolution (1) | ||
| Pruritus (1) (Bhasin V, 1984) [33] | Malaria (1) | Resolution (1) | ||
| Erythrodermic psoriasis (1) (Vestey JP, 1992) [37] | Psoriasis (1) | Psoriasis remained well controlled with usual treatment (1) | ||
| Pustular eruption (1) (Wilairatana P, 1998) [39] | Malaria (1) | After discontinuation, the eruption quickly resolved with mild desquamation (1) | ||
| Stevens–Johnson syndrome (1) (Das JK, 2011) [49] | Malaria (1) | Resolution (1) | ||
| Photosensitivity (1) (Soria A, 2015) [54] | SLE (1) | NA (1) | ||
| Palmo-plantar exfoliation (1) (Nair PA, 2017) [58] | Malaria (1) | NA (1) | ||
| Urticaria (1) (Balamurugesan K, 2019) [61] | Malaria (1) | Resolution (1) | ||
| Psychiatric | 20 (15) | Psychosis (9) (Burrell Z, 1958; Dornhorst AC, 1963; Rab SM, 1963; Oscar L, 1964; Kabir SM, 1969; Bomb BS, 1975; Ward WQ, 1985; Choughule A, 2019) [66,67,68,69,70,71,74,81] | Acute myocardial infarction (1) Rheumatoid arthritis (1) Hepatic or intestinal amoebiasis (4) Malaria (3) | Resolution (8) NA (1) |
| Moderate to severe depression (2) (Das EM, 1981) [72] | Malaria (2) | Resolution (2) | ||
| Mania (5) (Akhtar S, 1993; Plesnicar BK, 2013) [75,78] | Malaria (4) Rheumathoid arthritis (1) | Resolution (3) Disorder remains beyond 5 months (1) Mild attention deficit and memory difficulties (1) | ||
| Psychotic disorder with symptoms of depersonalization and anxiety (1) (Telgt DS, 2005) [76] | Malaria (1) | Resolution (1) | ||
| Organic delusional (schizophrenia-like) disorder (1) (Sahoo S, 2007) [77] | Malaria (1) | Resolution (1) | ||
| Exacerbation of bipolar disorder (maniac episode with psychotic features) (1) (Bogaczewicz J, 2014) [79] | SLE and arthritis (1) | Resolution (1) | ||
| Paranoid-like disorder (1) (Bogaczewicz A, 2016) [80] | SLE (1) | Resolution (1) | ||
| Neurologic | 15 (11) | Seizures (4), grand mal seizure (1) (Torrey EF, 1968; Martin AN 2016) [82,92] | Hepatic or intestinalamoebiasis (4) Prophylactic treatment of gastrointestinal parasitic infection (1) | Resolution (4) NA (1) |
| Involuntary movements (1) (Umez-Eronini EM, 1977) [83] | Fever (1) | Resolution (1) | ||
| Akathisia and persistent protrusion of the tongue (1) (Singh RP, 1981) [84] | Malaria (1) | Resolution (1) | ||
| Auditory hallucinations, acute psychotic behaviour, difficulty in swallowing, protrusion of the tongue, and marked extrapyramidal rigidity (1) (Singh RP, 1981) [84] | Malaria (1) | Resolution (1) | ||
| Serious tonic-clonic convulsion (1) (Fish DR, 1988) [85] | Malaria prophylaxis (1) | Serious consequences (1) | ||
| Severe cerebral ataxia with extrapyramidal movements (1) (James RF, 1988) [86] | Malaria (1) | Resolution (1) | ||
| Transient global amnesia (1) (Cras P, 1990) [87] | Malaria prophylaxis (1) | Resolution (1) | ||
| Retinopathy and persisting mild ocular myasthenia (1) (De Bleecker J, 1991) [88] | Malaria (1) | Symptoms persisted more than 10 years after drug discontinuation (1) | ||
| Tonic-clonic seizures (2) (Adamolekun B, 1992, Ebenso BE, 1998) [89,91] | Suspected malaria (1) Erythema nodosum leprosum (1) | Resolution (2) | ||
| Non-convulsive status epilepticus (1) (Mülhauser P, 1995) [90] | Malaria prophylaxis (1) | Resolution (1) | ||
| Cardiac | 3 (3) | Cardiovascular collapse (1) (Sogani RK, 1986) [94] | Dermatologic problem (1) | NA (1) |
| Cardiac arrhythmia (1) (Siqueira-Batista R, 1998) [95] | Malaria (1) | Resolution (1) | ||
| Syncopal attacks and torsade de pointes (1) (Yelve K, 2012) [98] | Hepatic and intestinal amoebiasis (1) | Resolution (1) | ||
| Hematologic and metabolic | 2 (2) | Hypoglycaemia (1) (Abu-Shakra M, 1994) [100] | Psoriatic arthritis (1) | Resolution (1) |
| Methaemoglobinaemia (1) (Rizvi I, 2012) [103] | Fever (1) | Resolution (1) | ||
| Sense organs | 3 (3) | Diplopia and persistent blurred near vision (1) (Rubin ML, 1970) [106] | Hypercalcemia associated with sarcoidosis (1) | Resolution (1) |
| Vestibular toxicity (1) (Malik MK, 1977) [108] | Malaria (1) | NA (1) | ||
| Loss of hearing (1) (Dwivedi GS,1978) [109] | Malaria (1) | Tinnitus and hearing loss have so far persisted for 5.5 months without improvement (1) | ||
| Hepatic | 1 (1) | Hepatotoxic reaction (1) (Liu AC, 1995) [113] | Malaria prophylaxis (1) | Resolution (1) |
| Other | 3 (3) | CQ overdose with severe headache, dizziness on standing, nausea and blurred vision (1) (Davis TM, 2003) [117] | Malaria (1) | Resolution (1) |
| Severe myopathy (1) (Richter JG, 2003) [118] | SLE with arthralgia and renal involvement (1) | NA (1) | ||
| Acute eosinophilic pneumonitis (1) (Knudsen L, 2009) [120] | Mild rosacea (1) | NA (1) |
| First Author, Year | Type of Study | Drug, Sample Size | Gastrointestinal Disorders | Hepatobiliary | Neurological | Sense Organs | Dermatological | Other | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Diarrhea | Nausea/Vomiting | Abdominal Pain/Dyspepsia | Bilirubin/GGT Increase | Transaminase Increase | Headache/Dizziness | ||||||
| Malaria treatment and prophylaxis | |||||||||||
| Weinke T, 1992 [126] | OBS | CQ n = 301 | NA | NA | 4.7% | NA | NA | Headache 0.3% Dizziness 0.3% | Tinnitus 0.7% | Exanthema 0% Pruritus 3.3% | Psychosis 0% ECG changes 0% |
| Bussaratid V, 2000 [127] | OBS | CQ n = 1189 | NA | NA | NA | NA | NA | NA | NA | Pruritus 1.9% | NA |
| Olayemi O, 2003 [128] | OBS | CQ n = 200 | NA | NA | NA | NA | NA | NA | NA | Pruritus 64.5% | NA |
| Gama H, 2009 [129] | OBS | CQ n = 542 | NA | NA | NA | NA | NA | NA | NA | Pruritus 30.1% | NA |
| Jeevangi SR, 2010 [130] | OBS | CQ n = 128 | NA | Nausea 9.4% Vomiting 9.4% | NA | NA | NA | NA | Tinnitus 9.4% | NA | Anorexia 9.4% |
| Ballut PC, 2013 [131] | OBS | CQ n = 510 | NA | NA | NA | NA | NA | NA | NA | Pruritus 20.4% | NA |
| Gozal D, 1991 [138] | RAN | CQ n = 78 | 3.8% | Nausea 11.5% Vomiting 8.9% | 24.4% | NA | NA | Headache 10.2% | Visual disturbances 1.3% | Pruritus 1.3% | Anorexia 16.7% Oral ulcers 19.2% |
| McClean K, 1992 [139] | RAN | CQ n = 18 | NA | NA | NA | NA | NA | NA | NA | Pruritus 44.4% | NA |
| Yanze MF, 2001 [171] | RAN | CQ n = 60 | 8.3% | Nausea 10.0% Vomiting 3.3% | 11.7% | NA | NA | Headache 3.3% Dizziness 5.0% | NA | Pruritus 5.0% | NA |
| Dunne MW, 2005 [140] | RAN | CQ n = 102 | NA | Nausea 4.9% Vomiting 7.8% | NA | NA | NA | Headache 1.0% | NA | Cutaneous drug eruption 2.9% Pruritus 7.8% | Myalgia 0% |
| Tagbor H, 2006 [172] | RAN | CQ n = 225 | NA | Nausea 22.2% Vomiting 31.1% | NA | NA | NA | Dizziness 43.1% | NA | Pruritus 39.1% | Weakness 47.1% |
| Ratcliff A, 2007 [141] | RAN | CQ n = 40 | NA | Vomiting 10.0% | NA | NA | NA | NA | NA | NA | NA |
| Massaga JJ, 2008 [142] | RAN | CQ n = 20 | NA | NA | 30% | NA | 0% | Headache 25.0% | NA | NA | Weakness 20.0% Fever 15.0% |
| Dunne MW, 2005 (2) [146] | RAN | CQ n = 16 | 6% | Nausea 0.0% Vomiting 0.0% | NA | NA | NA | Dizziness 19.0% | NA | Pruritus 19.0% | Pharyngitis 6.0% Fatigue 13.9% |
| Poravuth Y, 2011 [149] | RAN | CQ n = 228 | NA | Vomiting 1.8% | NA | 0% | 0.43% | Headache 1.3% Dizziness 2.2% | NA | NA | Fatigue 0.4% Anorexia 0.9% QT prolongation 2.7% |
| Watt G, 1988 [151] | RAN | CQ n = 10 | 20% | Vomiting 10.0% | NA | NA | NA | NA | NA | Pruritus 10.0% | NA |
| Systemic lupus erythematosus and cutaneous lupus erythematosus | |||||||||||
| Kishi CJ, 2018 [13] | OBS | HCQ n = 31 | 6.4% | NA | 3.2% | NA | NA | Dizziness 3.2% | Visual disturbances 3.2% | Erythema 6.4% | NA |
| Gonzalez CD, 2019 [134] | OBS | HCQ/CQ n = 136 | NA | NA | NA | NA | NA | NA | NA | Cutaneous drug eruption 4.0% | NA |
| Chasset F, 2018 [132] | OBS | HCQ/CQ n = 64 | NA | NA | NA | NA | NA | NA | NA | Exanthema 1.6%c | NA |
| Pulmonary sarcoidosis | |||||||||||
| Baltzan M, 1999 [145] | RAN | CQ n = 23 | NA | NA | 4.3% | NA | NA | NA | NA | Cutaneous drug eruption 4.3% | Anxiety 4.3% |
| Rheumatoid arthritis | |||||||||||
| Haar D, 1993 [143] | RAN | HCQ n = 28 | NA | NA | 3.6% | NA | NA | NA | NA | NA | NA |
| Dermatomyositis | |||||||||||
| Gonzalez CD, 2019 [134] | OBS | HCQ/CQ n = 44 | NA | NA | NA | NA | NA | NA | NA | Cutaneous drug eruption 5.0% | NA |
| Refractory chronic urticaria and chronic autoimmune urticaria | |||||||||||
| Seth S, 2017 [137] | OBS | HCQ n = 45 | NA | NA | NA | NA | NA | NA | NA | Pruritus 2.2% | NA |
| Reeves GE, 2004 [148] | RAN | HCQ n = 9 | NA | NA | NA | NA | NA | NA | NA | NA | Significant toxicity 0% |
| Porphyria cutanea tarda | |||||||||||
| Petersen CS, 1992 [135] | OBS | HCQ n = 72 | NA | Nausea 20.8% Vomiting 12.5% | 20.8% | Icterus 1.4% | 95.8% | Headache 25.0% | NA | NA | Arthralgia 5.5% Hepatomegaly 2.8% Myalgia 26.4% |
| Rossmann-Ringdahl, 2007 [136] | OBS | CQ n = 57 | NA | NA | NA | NA | 100% | NA | NA | NA | NA |
| Human immunodeficiency virus type 1 | |||||||||||
| Sperber K, 1995 [147] | RAN | HCQ n = 19 | NA | NA | NA | NA | NA | NA | NA | NA | Adverse reactions 0% |
| Breast cancer | |||||||||||
| Arnaout A, 2019 [150] | RAN | CQ n = 46 | 17.4% | Nausea and/or abdominal cramps 23.9% | NA | NA | NA | Dizziness 8.7% | Visual symptoms 8.7% Documented visual changes 0% Auditory symptoms 2.2% | NA | Fatigue 2.2% Muscle weakness 8.7% Dry mouth 4.3% |
| Chikungunya acute infection | |||||||||||
| De Lamballerie X, 2008 [154] | RAN | CQ n = 27 | NA | NA | NA | NA | NA | NA | NA | NA | Mild adverse reactions (mainly nausea and pruritus) 25.9% |
| Dengue | |||||||||||
| Tricou V, 2010 [155] | RAN | CQ n = 153 | NA | Vomiting 4.1% | NA | NA | NA | NA | NA | NA | NA |
| Borges MC, 2013 [156] | RAN | CQ n = 19 | NA | NA | NA | NA | NA | NA | Blurred vision 5.2% | NA | Loss of consciousness 5.2% |
| Infectious mononucleosis | |||||||||||
| Cowley RG, 1962 [152] | OBS | CQ n = 20 | Gastrointestinal complaints (anorexia, nausea, vomiting) 60% | NA | NA | NA | NA | NA | NA | ||
| Schumacher HR, 1963 [153] | OBS | CQ n = 5 | NA | NA | NA | NA | NA | NA | NA | NA | Complications 0% |
| Type of Study, Arm and Sample Size | Randomised AZM Plus CQ n = 114 | Randomised AZM Plus CQ n = 113 | Randomised AZM Plus CQ n = 1446 | Randomised AZM Plus CQ n = 64 | Single-Arm AZM Plus CQ n = 168 | Single-Arm AZM (2 g) Plus CQ n = 110 | Randomised AZM(1 g) Plus CQ n = 197 | Randomised AZM (0.5 g) Plus CQ n = 81 |
|---|---|---|---|---|---|---|---|---|
| Author, year | Sagara I, 2014 [173] | Kimani J, 2016 [179] | Dunne MW, 2005 [146] | Phiri K, 2016 [180] | Kshirsagar NA, 2017 [174] | |||
| Any AEs | 78.1% | 70.8% | 68.9% | 20% | NA | 44% | 26% | 10% |
| Abdominal pain/discomfort | 7.0% | 11.5% | 8.3–8.5% | NA | NA | 0% | 3% | 0% |
| Asthenia | 5.3% | 8.0% | 16.6% | NA | NA | NA | NA | NA |
| Blood/lymphatic disorders | NA | NA | 14.3% | NA | NA | NA | NA | NA |
| Dehydration | NA | NA | NA | NA | NA | 4% | 0% | 0% |
| Diarrhea | 5.3% | 9.7% | 14.2% | 3% | NA | 12% | 4% | 0% |
| Dizziness | 9.6% | 15.9% | 32.0% | 0% | 19.6% | NA | NA | NA |
| Fatigue | 0% | 3.5% | 5.6% | NA | 4.2% | NA | NA | NA |
| Gastritis | NA | NA | NA | NA | NA | 4% | 2% | 1% |
| Headache | 13.2% | 17.7% | 20.7% | NA | 6.0% | 0% | 2% | 0% |
| Infections | NA | NA | 30.1% | Pharyngitis 0% | Parasitic infection 7.1% Upper respiratory infection 4.2% | NA | NA | NA |
| Nausea | 7.9% | 8.8% | 14.9% | 6% | 3.6% | 30% | 0% | 0% |
| Pain | 1.8% | 5.3% | NA | NA | NA | NA | NA | NA |
| Palpitations | 2.6% | 0% | NA | NA | NA | NA | NA | NA |
| Paraesthesia | NA | NA | NA | NA | NA | 0% | 3% | 0% |
| Pruritus | 50.9% | 28.3% | NA | 2% | Pruritus 7.7% Generalised pruritus 5.4% | 4% | 15% | 6% |
| Visual disorders | NA | NA | 10.1% | NA | NA | NA | NA | NA |
| Vomiting | 15.8% | 3.5% | 45.2% | 8% | 20.8% | 18% | 4% | 1% |
| First Author, Year | Drug, Indication | Adverse Effect |
|---|---|---|
| CQ or HCQ alone | ||
| Obasikene G, 2012 [162] | CQ malaria | Ototoxicity |
| Ajayi AA, 1989 [157] | CQ malaria | Pruritus |
| Castro-Cavadía CJ, 2020 [166] | CQ malaria | AEs were confused in frequency and intensity with malaria symptoms and signs |
| Schneider C, 2013 [163] | CQ malaria | Neuropsychiatric disorder |
| Sarathi P, 2014 [165] | CQ malaria | Psychiatric manifestation |
| Dugué A, 2004 [167] | HCQ NA | Muscular adverse events |
| Sidoroff A, 2007 [169] | CQ and HCQ NA | AGEP |
| George AO, 2004 [161] | CQ malaria | Pruritus |
| Patel KJ, 2007 [168] | CQ NA | Gastritis |
| Emerole CG, 2014 [164] | CQ malaria | Loss of visual acuity |
| Ajayi AA, 1998 [175] | CQ malaria | Pruritus |
| Katugampola G,1990 [158] | CQ malaria | Worsening of psoriasis |
| Frías Salcedo JA, 1992 [159] | CQ malaria | Visual and gastrointestinal disturbances or pruritus and headache |
| Yanze MF, 2001 [171] | CQ malaria | Headache, diarrhea, abdominal pain, nausea, pruritus, dizziness, and vomiting |
| Walsh DS, 1999 [170] | CQ malaria | Abdominal discomfort and diarrhea |
| Garcia P, 2020 [280] | HCQ COVID-19 | Psychiatric disorders |
| CQ or HCQ combined with other drug | ||
| Vouri SM, 2020 [177] | CQ and HCQ plus AZM autoimmune disease | Sudden cardiac arrest, ventricular arrhythmias, and cardiac symptoms |
| Sarayani A, 2021 [178] | CQ and HCQ plus AZM NA | CQ and HCQ appeared not to be associated with a safety risk related to torsade de pointes or QT prolongation when used alone, when used with AZM they were associated with a potential safety risk |
| Ajayi AA, 1991 [175] | CQ plus prednisolone malaria | Pruritus |
| Adebayo RA, 1997 [176] | CQ plus prednisolone malaria | Pruritus |
| Organ Affected | Number of Patients | Adverse Effect, Drug Combination If Required (Number of Patients) (First Author, Year) | Long-Term Consequences |
|---|---|---|---|
| CQ | |||
| Cardiac | 2 | Major QT prolongation and recurrent torsade de pointes (1) (Szekely Y, 2020) [188] | ECGs showed gradual normalization of QT interval |
| Wide complex tachycardia, along with AZM (1) (Gracia-Ramos AE, 2021) [189] | Death after cardiac arrest | ||
| Hematologic and metabolic | 1 | G6PD deficiency-associated haemolysis and methaemoglobinaemia (1) (Kuipers MT, 2020) [184] | The patient’s methaemoglobin normalized within 6 days |
| Psychiatric | 3 | Psychotic symptoms, along with AZM (1) (Benjelloun R, 2020) [195] | Resolution after 48 h |
| Acute and intense anxiety, along with AZM (1) (Benjelloun R, 2020) [195] | No | ||
| Psychosis episode (1) (Ambar Akkaoui M, 2021) [193] | NA | ||
| HCQ | |||
| Cardiac | 6 | Right bundle brunch block and critically prolonged QTc (1) (Asli R, 2020) [181] | Resolution |
| QT interval prolongation in a patient on AZM (1) (Mitra RL, 2020) [186] | Death owing to progressive metabolic acidosis and multiorgan system failure | ||
| QTc prolongation and torsade de pointes, along with dexamethasone (1) (Aslam W, 2021) [190] | NA | ||
| Suspected HCQ-induced sinus bradycardia and QTc interval prolongation (1) (Kang Y, 2020) [191] | A temporary pacemaker was implanted | ||
| QTc prolongation, along with AZM (1) (Patel J, 2020) [192] | No | ||
| Sinus bradycardia, along with AZM and corticosteroids (1) (Patel J, 2020) [192] | No | ||
| Dermatological | 12 | Psoriasis exacerbation (1) (Kutlu Ö, 2020) [185] | NA |
| AGEP with erythema multiforme-like lesions (1) (Robustelli Test E, 2020) [187] | Slow but progressive resolution | ||
| Rash (1) (Kurd R, 2020) [202] | NA | ||
| AGEP (1) (Enos T, 2020) [199] | Resolved with prednisone after 38 days | ||
| AGEP (1) (Delaleu J, 2020) [198] | NA | ||
| Erythema multiforme (1) (Monte-Serrano J, 2020) [197] | NA | ||
| Urticaria with maculopapular rash, palmoplantar itching (1) (Sardana K, 2020) [196] | NA | ||
| Urticaria (1) (Sardana K, 2020) [196] | NA | ||
| Palmoplantar itching (1) (Sardana K, 2020) [196] | NA | ||
| DRESS syndrome, along with AZM and LPVr (1) (Castro Jiménez A, 2021) [200] | NA | ||
| Purpuric erythematous rash with non-follicular pustules, on the trunk and limps, with intense involvement of armpits and scalp (1) (Abadías-Granado I, 2021) [201] | No | ||
| Purpuric erythematous rash with non-follicular pustules and targetoid lesions on the back (1) (Abadías-Granado I, 2021) [201] | No | ||
| Hematologic, muscular and metabolic | 6 | Worsening of haemolysis (1) (Beauverd Y, 2020) [183] | NA |
| Haemolysis in a G6DP-deficient patient (1) (Maillart E, 2020) [204] | NA | ||
| Haemolytic anemia in a G6DP-deficient patient (1) (Aguilar J, 2020) [206] | NA | ||
| Acute haemolytic anemia in a G6DP-deficiency patient (1) (Chaney SI, 2020) [205] | NA | ||
| Thrombotic thrombocytopaenic purpura (1) (Arıkan F, 2020) [203] | No | ||
| Hepatic | 1 | Hepatotoxicity (1) (Falcão MB, 2020) [182] | NA |
| Ophthalmology | 1 | Myasthenic syndrome (1) (Koc G, 2020) [194] | No |
| Gastrointestinal | 1 | Nausea, vomiting, diarrhea (1) (Patel J, 2020) [192] | NA |
| First Author, Year | Type of Study, Drug and Sample Size | Cardiac | Gastrointestinal Disorders | Hepatobiliary | Neurological | Sense Organs | Dermatological | Other | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| QT Prolongation | Prolonged QTc ≥ 500 ms | Prolongued QTc ≥ 60 ms | Ventricular Arrythmia | Torsade Depointes | Arrhythmogenic Death | Diarrhea | Nausea/Vomiting | Abdominal Pain/Dyspepsia | Bilirubin/GGT Increase | Transaminase Increase | Headache/Dizziness | |||||
| Seyhan AU, 2020 [241] | OBS HCQ n = 51 | NA | 1.96% | 1.96% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Abella BS, 2021 [270] | RAN HCQ n = 132 | NA | NA | NA | NA | NA | NA | 32% | 9% | 6% | NA | NA | Headache 0% Dizziness 2% | NA | Rash 5% | Paraesthesia 2% |
| Bernardini A, 2021 [246] | OBS HCQ n = 40 | 40% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Furtado RHM, 2020 [247] | RAN HCQ n = 183 | 21% | NA | NA | CRVA 3% | NA | 0% | NA | NA | 24% | 3% | NA | NA | NA | NA | NA |
| Satlin MJ, 2020 [250] | OBS HCQ n = 153 | NA | NA | NA | Monomorphic VT 0.6% | 0% | NA | NA | NA | NA | NA | Grade 3 11% Grade 4 9% | NA | NA | NA | NA |
| Hsia BC, 2020 [253] | OBS HCQ n = 40 | NA | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| OBS CQ n = 5 | NA | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| Skipper CP, 2020 [252] | RAN HCQ n = 212 | NA | NA | NA | NA | NA | NA | 23.6% | 31.1% | NA | NA | NA | Headache 0.9% Dizziness 9.4% | Ringing in ears 3.8% Changes in vision 1.9 Taste, dry mouth 0% | Rash 2.8 | NA |
| Boulware DR, 2020 [271] | RAN HCQ n = 414 | NA | NA | NA | NA | NA | NA | NA | 22.9% | 23.2% | NA | NA | 3.7% | Tinnitus 2.3% Visual changes 0.9% Taste change or dry mouth 0.9% | Skin reaction 1.1% | NA |
| Falcão F, 2020 [239] | OBS HCQ n = 20 | 10% | NA | NA | NA | NA | NA | 5% | Nausea 10% Vomiting 5% | 0% | Liver cholestasis 0% | 10% | NA | Ocular disorders 0% | Skin and subcutaneous disorders 10% | NA |
| Sogut O, 2021 [240] | OBS HCQ n = 152 | 64.5% | 0% | 0% | NA | NA | 0% | 22.3% | NA | NA | 16.4% | NA | Itching and redness 2.6% | NA | ||
| Mitjà O, 2021 [268] | RAN HCQ n = 1116 | NA | NA | NA | NA | NA | NA | 42.6% | NA | NA | 21.7% | NA | NA | General disorder: myalgia, fatigue, malaise 8.6% | ||
| Barnabas RV, 2021 [269] | RAN HCQ n = 407 | NA | NA | NA | NA | NA | NA | NA | 3.4% | 6.1% | NA | NA | Headache 1.2% Dizziness 1.5% | Taste change or dry mouth 0.2% Visual changes 1% Tinnitus 0% | Rash 2.7% | Fatigue 1% |
| Nagaraja BS, 2020 [272] | OBS HCQ n = 156 | NA | NA | NA | NA | NA | NA | 7.22% | Nausea 10.24% Vomiting 1.20% | 7.22% | NA | NA | Headache 6% Dizziness 3.6% | Tinnitus 0.6% Transient visual blurring 2.4% | Hair fall 1.8% Oral ulcer 1.2% Itching 0.6% | Psychiatric 4.8% Nightmare 0.6% Nervousness 1.20% Fatigue, lethargyWeakness 7.2% |
| Özdemir IH, 2020 [256] | OBS HCQ n = 45 | NA | NA | NA | NSVT 0% SVT 0% VF 0% | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Cavalcanti AB, 2021 [257] | RAN HCQ n = 221 | 14.6% | NA | NA | VT 0% | NA | NA | NA | Nausea 4.5% Vomiting 0% | NA | 2.5% | 8.5% | NA | Hypoacusia 0% | Itching 0.5% | Hypoglycaemia 0.5% |
| Çap M, 2020 [258] | OBS HCQ n = 66 | 6% | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Lauriola M, 2020 [259] | OBS HCQ n = 17 | NA | NA | NA | NA | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Ramireddy A, 2020 [264] | OBS HCQ n = 10 | NA | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Tanriverdİ E, 2021 [260] | OBS HCQ n = 30 | NA | NA | NA | 0% | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Arshad S, 2020 [261] | OBS HCQ n = 1202 | NA | NA | NA | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Pereira MR, 2020 [265] | OBS HCQ n = NA | 0% | NA | NA | 0% | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Jain S, 2020 [230] | OBS HCQ n = 415 | 23.6% | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Hor CP, 2020 [228] | OBS HCQ n = 2 | 100% | NA | NA | 0% | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Paccoud O, 2020 [227] | OBS HCQ n = 38 | 5.3% | NA | NA | NA | NA | NA | 2.6% | NA | NA | NA | NA | Headache 2.6% | NA | NA | NA |
| Lagier JC, 2020 [226] | OBS HCQ n = 101 | NA | NA | 2% | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Reis G, 2021 [233] | RAN HCQ n = 207 | NA | NA | NA | NA | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Faruqui AR, 2021 [267] | OBS HCQ n = 1303 (HCQ + AZ: 0.8%; CQ: 0.5%) | NA | NA | NA | NA | NA | NA | NA | Nausea 8.7% Vomiting 1.4% | 7.0% | NA | NA | NA | Photosensitivity 0.5% | NA | NA |
| Eftekhar SP, 2021 [236] | OBS HCQ n = 29 | 10.3% | NA | NA | 0% | 3.4% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Mazzanti A, 2020 [229] | OBS HCQ n = 50 | NA | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Karolyi M, 2021 [231] | OBS CQ n = 20 | NA | NA | NA | NA | NA | NA | 0% | 5% | NA | NA | 10% | NA | NA | NA | NA |
| Mitjà O, 2020 [232] | RAN HCQ n = 136 | NA | NA | NA | NA | NA | 0% | 88.1% | NA | NA | 37.5% | Ear and labyrinth disorders 3% Eye disorders 3% | 6.5% | Psychiatric disorders 1.2% | ||
| Lofgren SM, 2020 [266] | RAN HCQ once-daily n = 576 | NA | NA | NA | NA | NA | 0% | Upset stomach or nausea 25.3% Diarrhea, vomiting, or abdominal pain 22.7% | NA | NA | Headache 2.6% Irritability, dizziness, vertigo 6.8% | Tinnitus 2.8% Visual changes 1.2% Taste change or dry mouth 0.5% | Skin reaction 1.7% | Panic 0% | ||
| RAN HCQ once-weekly n = 473 | NA | NA | NA | NA | NA | 0% | Upset stomach or nausea 17.5% Diarrhea, vomiting, or abdominal pain 12.9% | NA | NA | Irritability, dizziness, vertigo 5.7% | Tinnitus 2.1% Visual changes 1.5% | Skin reaction 2.7% | Sleep disturbance 2.1% | |||
| RAN HCQ twice-weekly n = 463 | NA | NA | NA | NA | NA | 0% | Upset stomach or nausea 19.4% Diarrhea, vomiting, or abdominal pain 17.1% | NA | NA | Irritability, dizziness, vertigo 5.2% | Tinnitus 1.5% Visual changes 0.9% | Skin reaction 5.0% | Sleep disturbance 1.5% | |||
| Bessière F, 2020 [207] | OBS HCQ n = 22 | NA | 5% | NA | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Mercuro NJ, 2020 [215] | OBS HCQ n = 37 | NA | 19% | 8% | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Rosenberg ES, 2020 [218] | OBS HCQ n = 271 | 14.4% | NA | NA | NA | NA | NA | 17.0% | NA | NA | NA | NA | NA | NA | NA | NA |
| Saleh M, 2020 [219] | OBS HCQ or CQ n = 82 | NA | 8.5% | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Van den Broek MPH 2020 [220] | RAN CQ n = 95 | NA | 23% | NA | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Chen Z, 2020 [222] | RAN HCQ n = 31 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | Headache 3.2% | NA | 3.2% | NA |
| Huang M, 2020 [223] | RAN CQ n = 10 | NA | NA | NA | NA | NA | NA | 50.0% | Nausea 40% Vomiting 50% | 10% | NA | NA | Headache 0% Dizziness 0% | NA | 10% | Psychosis 0% |
| Fernández-Ruiz M, 2020 [212] | OBS HCQ n = 4 | NA | 25% | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Chen J, 2020 [224] | OBS HCQ n = 15 | NA | NA | NA | NA | NA | NA | 13.3% | NA | NA | 6.66% | NA | NA | NA | NA | Weakness 6.6% |
| First Author, Year | Type of Study, Drug and Sample Size | Cardiac | Gastrointestinal | Hepatobiliary | Neurological | Sense Organs | Dermatological | Other | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| QT Prolongation | Prolonged QTc ≥ 500 ms | Prolongued QTc ≥ 60 ms | Ventricular Arrythmia | Torsade de Pointes | Arrhythmogenic Death | Diarrhea | Nausea/Vomiting | Abdominal Pain/Dyspepsia/Other | Bilirubin Increase/GGT Increase | Transaminase Increase | Headache/Dizziness | |||||
| Gao X, 2020 [273] | OBS INF-alpha + LPVr + arbidol or rivabirin or CQ n = 26 | NA | NA | NA | NA | NA | NA | 11.5% | NA | NA | Abnormal liver function 61.5% | NA | NA | NA | Rash 7.7% | Dyslipidemia 42.3% |
| Seyhan AU, 2020 [241] | OBS HCQ + AZM n = 93 | NA | 1.07% | 2.15% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Lamback EB, 2021 [237] | OBS HCQ + AZM n = 101 | 7.9% | NA | NA | NA | NA | NA | 7.9% | NA | NA | NA | NA | NA | NA | ||
| Saleh M, 2020 [245] | OBS HCQ ± AZM n = 6.476 (HCQ n = 2847 HCQ + AZM n = 3629) | NA | NA | NA | VF 0.06% SMVT 0.08% NSMVT 0.27% SPVT 0.015% NSPVT 0% | 0.015% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Bernardini A, 2021 [246] | OBS HCQ + AZM n = 53 | 70% | 8% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Furtado RHM, 2020 [247] | RAN HCQ + AZM n = 214 | 20% | NA | NA | CRVA 3% | NA | NA | NA | NA | 25% | Bilirrubin increase > 50% 4% | NA | NA | NA | NA | NA |
| Giaime P, 2020 [248] | OBS HCQ + AZM n = 21 | NA | 4.8% | NA | NA | NA | NA | NA | 19% | NA | NA | NA | NA | Visual impairment 0% | Dermatitis 0% | Hypoglicaemia 23.8% |
| Kalligeros M, 2020 [249] | OBS HCQ + AZM n = 32 | 3.1% | 9.4% | NA | VC 0.9% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | Seizure 3.1% |
| Kelly M, 2021 [276] | OBS HCQ + AZM n = 82 | 13.4% | NA | NA | NA | NA | NA | NA | NA | NA | NA | Elevated liver function tests 65% | NA | NA | NA | NA |
| Hsia BC, 2020 [253] | OBS HCQ + AZM n = 33 | NA | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| OBS CQ + AZM n = 4 | NA | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| Moschini L, 2021 [251] | OBS HCQ + AZM n = 52 | NA | 13% (day 3), 20% (day 7) | NA | MVA 1.9% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| OBS HCQ + DRVr n = 61 | NA | NA | NA | MVA 1.6% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| O’Connell TF, 2021 [238] | OBS HCQ + AZM n = 415 | NA | 21% | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Falcão F, 2020 [239] | OBS HCQ + AZM n = 52 | 5.7% | NA | NA | NA | NA | NA | 1.9% | Nausea 3.8% Vomiting 1.9% | 3.8% | Bilirrubin increase 0% GGT increase 1.9% Liver cholestasis 7.7% | 3.84% Hepatotoxicity 7.7% | NA | Ocular disorders 1.9% | Skin and subcutaneous disorders1.9% | NA |
| OBS HCQ + LPVr n = 22 | 0% | NA | NA | NA | NA | NA | 40.9% | Nausea 4.5% Vomiting 4.5% | 4.5% | Bilirrubin increase 13.6% GGT increase 13.6% Liver cholestasis 4.5% | 54.54% Hepatotoxicity 0% | NA | Ocular disorders 4.5% | Skin and subcutaneous disorders 0% | NA | |
| OBS HCQ + AZM + LPVr n = 7 | 14.2% | NA | NA | NA | NA | NA | 71.4% | Nausea 14.2% Vomiting 0% | 0% | Bilirrubin increase 14.3% GGT increase 14.2% Liver cholestasis 14.2% | 42.8% Hepatotoxicity 14.2% | NA | Ocular disorders 0% | Skin and subcutaneous disorders0% | NA | |
| Chen CP, 2020 [274] | RAN HCQ ± AMZ ± OSM ± LEV n = 21 | 0% | NA | NA | NA | NA | NA | 5.3% | 5.3% | Gastritis 5.3% | NA | NA | Headache 21.1% Dizziness 5.3% | Photophobia 5.3% | NA | NA |
| Meriglier E, 2021 [242] | OBS HCQ + LPVr n = 21 | NA | NA | NA | NA | NA | NA | 23.8% | 9.52% | NA | NA | 0% | Headache 0% | NA | 0% | NA |
| OBS HCQ + DRVr n = 25 | NA | NA | NA | NA | NA | NA | 32% | 0% | NA | NA | 4% | Headache 0% | NA | 0% | NA | |
| Self WH, 2020 [275] | RAN HCQ ± AZM ± REM ± corticosteroids n = 242 | NA | 5.9% | NA | 2.1% | NA | NA | NA | NA | NA | NA | 20.7% | NA | NA | NA | Seizure 0.4% Symptomatic hypoglycaemia 4.1% |
| Fteiha B, 2021 [243] | OBS HCQ± AZM n = 90 | NA | 7.8% | 12% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| RECOVERY Collaborative Group, 2020 [244] | RAN HCQ± AZM n = 1561 | NA | NA | NA | VT or fibrillation 0.7% | 0.064% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Nagaraja BS, 2020 [272] | OBS HCQ + AZM n = 7 | NA | NA | NA | NA | NA | NA | 28.6% | NA | NA | NA | NA | NA | NA | ||
| Echarte-Morales J, 2020 [254] | OBS HCQ + AZM n = 54 | 9.3% | 3.7% | 11.1% | NA | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| OBS HCQ + AZM + LPVr n = 114 | 11.4% | 6.1% | 18.4% | NA | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| Jiménez-Jáimez J, 2020 [255] | OBS HCQ + AZM + LPVr or DRVr n = 114 | NA | 1.8% | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| OBS HCQ ± AZM n = 105 | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | ||
| Özdemir IH, 2020 [256] | OBS HCQ + AZM n = 56 | NA | NA | NA | NSVT 0% SVT 0% | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Cavalcanti AB, 2021 [257] | RAN HCQ + AZM n = 217 | 14.7% | NA | NA | VT 0% | NA | NA | NA | Nausea 2.5% Vomiting 0% | NA | Bilirrubin increase 0.4% | 10.9% | NA | Hypoacusia 0% | Itching 0% | Hypoglycaemia 0% |
| Çap M, 2020 [258] | OBS HCQ + FVP n = 66 | 3% | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Rodriguez-Garcia JL, 2020 [277] | OBS HCQ + LPVr + corticosteroids n = 50 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | Delirium 4% Hyperglycemic decompensation 10% |
| Ip A, 2020 [278] | OBS HCQ ± AZM (HCQ: n = 441 HCQ + AZM n = 1473) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Lauriola M, 2020 [259] | OBS HCQ + AZM n = 297 | NA | NA | NA | NA | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Tanriverdİ E, 2021 [260] | OBS HCQ + AZM n = 26 | NA | NA | NA | 0% | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Arshad S, 2020 [261] | OBS HCQ + AZM n = 783 | NA | NA | NA | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Bun SS, 2020 [262] | OBS HCQ + AZM n = 71 | NA | 2.8% | NA | NA | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Dastan F, 2020 [279] | RAN HCQ + INF-β-1a + LPVr n = 20 | NA | NA | NA | NA | NA | 0% | NA | NA | NA | 0% | 0% | NA | NA | NA | NA |
| Maraj I, 2020 [263] | OBS HCQ + AZM n = 91 | 23% | 14% | NA | 2.2% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Ramireddy A, 2020 [264] | OBS HCQ + AZM n = 61 | 11.4% | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Pereira MR, 2020 [265] | OBS HCQ + AZM n = NA | 0% | NA | NA | 0% | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Uğurlu Ilgin B, 2021 [235] | OBS HCQ + OSM + AZM n = 43 | 42.85% | 8.8% | NA | 0% | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| OBS HCQ + OSM + LEV n = 48 | NA | 0% | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | |||
| Hor CP, 2020 [228] | OBS HCQ + AZM n = 11 | NA | NA | 9.1% | 0% | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Lagier JC, 2020 [226] | OBS HCQ + AZM ≥ 3 days n = 3119 HCQ + AZM < 3 days n = 218 | NA | 0.03% | 0.6% | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Dabbous HM, 2021 [234] | OBS HCQ + OSM n = 50 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 0% | NA | NA | NA | NA |
| Eftekhar SP, 2021 [236] | OBS HCQ + AZM n = 143 | 24.5% | NA | NA | 1.4% | 0.7% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Mazzanti A, 2020 [229] | OBS HCQ + AZM n = 39 | NA | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| OBS HCQ + LPVr n = 53 | NA | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| OBS HCQ + LPVr + AZM n = 9 | NA | NA | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| Borba MGS, 2020 [221] | RAN CQ low dose + AZM ± OSM n = 40 | NA | 7.9% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| RAN CQ high dose + AZM ± OSM n = 41 | NA | 21.2% | 5.8% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| Tang W, 2020 [211] | RAN HCQ + SOC n = 70 | NA | NA | NA | NA | NA | NA | 10% | NA | NA | NA | NA | NA | NA | NA | NA |
| Chong VH, 2020 [208] | OBS HCQ + LPVr n = 11 | NA | 18.2% | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Fernández-Ruiz M, 2020 [212] | OBS HCQ + LPVr n = 6 | NA | NA | NA | NA | NA | NA | NA | NA | 16.7% | NA | NA | NA | NA | NA | NA |
| Colaneri M, 2020 [225] | OBS HCQ + AZM + TCZ n = 21 | NA | NA | NA | NA | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Saleh M, 2020 [245] | OBS CQ or HCQ + AZM n = 119 | NA | 9.2% | NA | NA | 0% | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Rosenberg ES, 2020 [218] | OBS HCQ + AZM n = 735 | 11.0% | NA | NA | NA | NA | NA | 11.6% | NA | NA | NA | NA | NA | NA | NA | NA |
| Molina JM, 2020 [217] | OBS HCQ + AZM n = 11 | 9.09% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Million M, 2020 [216] | OBS HCQ + AZM n = 1061 | NA | 0% | 0.8% | NA | 0% | 0% | 1.1% | Nausea 0.2% Vomiting 0.1% | Abdominal pain 0.3% | NA | NA | Headache 0.3% | Transient blurred vision 0.2% | Erythematous and bullous rash 0.1% | Insomnia 0.2% |
| Bessière F, 2020 [207] | OBS HCQ + AZM n = 18 | NA | 33% | NA | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Chorin E, 2020 [209] | OBS HCQ + AZM n = 251 | NA | 13% | NA | NA | 0.4% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Cipriani A, 2020 [210] | OBS HCQ + AZM n = 22 | NA | 4.54% | 18% | 4.54% | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Gautret P, 2020 [213] | OBS HCQ + AZM n = 80 | NA | NA | NA | NA | NA | NA | 5.0% | 2.5% | NA | NA | NA | NA | Blurred vision 1.2% | NA | NA |
| Mahévas M, 2020 [214] | OBS HCQ ± AZM n = 84 | NA | 1.2% | 8.3% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Mercuro NJ, 2020 [215] | OBS HCQ + AZM n = 53 | NA | 21% | 13% | NA | 1.88% | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
3.2. Quality Assessment
3.3. Data Synthesis of the Systematic Review Findings
3.3.1. Patients Treated for Conditions Other Than COVID-19
3.3.2. Patients Treated for COVID-19
| Treatment Indication | Malaria Treatment and Prophylaxis | Autoimmune Diseases | Porphyria Cutanea Tarda | Malaria Treatment and Prophylaxis | COVID-19 Prophylaxis | COVID-19 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Drug | CQ | CQ/HCQ | CQ/HCQ | CQ plus AZM | HCQ | CQ/HCQ | CQ/HCQ + AZM | HCQ + LPVr | HCQ + DRVr | HCQ + AZM + LPVr |
| Cardiac adverse events | ||||||||||
| Arrhythmia | NA | NA | NA | NA | 0–0.2% (1) | 0–16.2% (3) | 0–20.4% (3) | NA | NA | NA |
| Palpitations | NA | NA | NA | 0–2.6% (2) | 0.4–2.4% (3) | NA | NA | NA | NA | NA |
| Cardiac arrest | NA | NA | NA | NA | NA | 0–13.7% (3) | 7–15.5% (2) | NA | NA | NA |
| ECG changes | 0% (1) | NA | NA | NA | NA | 0–27.3% (2) | 0–27.1% (2) | 19.0% (1) | 0–16% (1) | NA |
| Prolonged QTc ≥500 ms | NA | NA | NA | NA | NA | 0–25% (8) | 0–33% (18) | 18.2% (1) | NA | 6.1% (1) |
| QTc change ≥60 ms | NA | NA | NA | NA | NA | 0–8% (4) | 0–18% (9) | NA | NA | 18.4% (1) |
| Torsade de pointes | NA | NA | NA | NA | NA | 0–3.4% (19) | 0–1.88% (19) | 0% (2) | 0% (1) | 0% (2) |
| Arrhythmogenic deaths | NA | NA | NA | NA | 0% (1) | 0% (19) | 0% (18) | 0% (2) | 0% (1) | 0% (3) |
| Dermatological adverse events | ||||||||||
| Cutaneous Drug Eruptions | 2.9% (1) | 4.0–6.4% (4) | NA | NA | 0.6–5% (5) | 0.6–10.0% (9) | 0–1.9% (4) | 0% (2) | 0% (1) | 0% (1) |
| Exanthema | 0% (1) | 1.6% (1) | NA | NA | NA | NA | NA | 0% (1) | 0% (1) | 0% (1) |
| Pruritus | 3.3–64.5% (12) | 2.2% (1) | NA | 2.0–50.9% (6) | NA | NA | NA | 0% (1) | 0% (1) | 0% (1) |
| Gastrointestinal adverse events | ||||||||||
| Diarrhea | 3.8–20.0% (4) | 6.4% (1) | NA | 0–12.0% (6) | 7.2–32% (2) | 0–50% (7) | 1.1–11.6% (4) | 23.8–40.9% (2) | 32% (1) | 71.4% (1) |
| Anorexia | 0.9–16.7% (3) | NA | NA | NA | 4.8% (1) | NA | NA | NA | NA | NA |
| Nausea | 0–22.0% (6) | NA | 20.8% (1) | 0–30.0% (6) | 3.4–25.3% (4) | 4.5–40% (3) | 0.2–3.8% (3) | 4.5–9.5% (2) | 0% (1) | 14.2% (1) |
| Vomiting | 0–31.1% (9) | NA | 12.5% (1) | 1.0–18.0% (6) | 1.2–1.4% (2) | 0–50% (3) | 0–1.9% (3) | 4.5% (1) | 0% (1) | 0% (1) |
| Abdominal pain or discomfort, dyspepsia or GI intolerance | 4.7–30.0% (4) | 3.2–4.3% (3) | 20.8% (1) | 0–11.5% (5) | 6–23.2% (5) | 0–24% (3) | 0.3–25.0% (3) | 4.5–16.7% (2) | NA | 0% (1) |
| Psychiatric and neurological adverse events | ||||||||||
| Anxiety/nervousness | NA | 4.3% (1) | NA | NA | 0.6–1.2% (1) | NA | NA | NA | NA | NA |
| Insomnia/Sleep disturbances | NA | NA | NA | NA | 1.5–2.1% (1) | NA | 0.2% (1) | NA | NA | NA |
| Psychosis | 0% (1) | NA | NA | NA | NA | 0% (1) | NA | NA | NA | NA |
| Dizziness | 0.3–43.1% (5) | 3.2% (1) | NA | 0–15.9% (3) | 1.5–3.6% (3) | 0–9.4% (2) | NA | NA | NA | NA |
| Headache | 0.3–25.0% (6) | NA | 25.0% (1) | 0–17.7% (2) | 0–6% (4) | 0–3.2% (4) | 0.3% (1) | 0% (1) | 0% (1) | NA |
| Paraesthesia | NA | NA | NA | 0–3.0% (3) | 2% (1) | NA | NA | NA | NA | NA |
| Hematologic and metabolic adverse events | ||||||||||
| Thrombocytopaenia | NA | NA | NA | NA | NA | 0–7% (3) | 0–7.1% (3) | 4.5–9.1% (2) | NA | 0% (1) |
| Hypoglycaemia | NA | NA | NA | NA | 1.1% (1) | 0.5% (1) | 0–23.8% (2) | 0 (1) | 0% (1) | NA |
| Sense organs adverse events | ||||||||||
| Blurred vision | NA | NA | NA | NA | NA | NA | 0.2–1.2% (2) | NA | NA | NA |
| Tinnitus | 0.7–9.4% (2) | NA | NA | NA | 0–2.8% (4) | 3.8% (1) | 0% (1) | NA | NA | NA |
| Visual disturbances/ocular disorders | 1.3% (1) | 3.2% (1) | NA | NA | 0.9–2.4% (4) | 0–3% (3) | 0–1.9% (2) | 4.5% (1) | NA | 0% (1) |
| Hepatic adverse events | ||||||||||
| Hepatomegaly | NA | NA | 2.8% (1) | NA | NA | NA | NA | NA | NA | NA |
| Icterus/Bilirubin or GGT increase | 0% (1) | NA | 1.4% (1) | NA | NA | 0–6.6% (4) | 0–4% (3) | NA | NA | 14.3% (1) |
| Transaminase increase | 0–0.43% (2) | NA | 95.8–100.0% (2) | NA | NA | 0–11% (5) | 3.8–10.9% (2) | 0–54.5% (3) | 4% (1) | 42.8% (1) |
| Other adverse events | ||||||||||
| Asthenia/Weakness | 20.0–47.1% (2) | NA | NA | 5.3–8.0% (2) | 7.2% (1) | 6.6% (1) | NA | NA | NA | NA |
| Fatigue | 0.4–1.9% (2) | NA | 13.9% (1) | 0–3.5% (3) | 1% (1) | NA | NA | NA | NA | NA |
| Fever | 15.0% (1) | NA | 37.5–43.8% (2) | NA | NA | NA | NA | NA | NA | NA |
| Myalgia | 0% (1) | NA | 26.4% (1) | NA | NA | NA | NA | NA | NA | NA |
3.4. Summary of the Evidence across Studies
3.4.1. Cardiac Adverse Drug Reactions
Cases
Observational and Randomised Studies
3.4.2. Dermatological Adverse Drug Reactions
Cases
Observational and Randomised Studies
3.4.3. Neurologic and Psychiatric Adverse Drug Reactions
Cases
Observational and Randomised Studies
3.4.4. Gastrointestinal and Hepatic Adverse Drug Reactions
Cases
Observational and Randomised Studies
3.4.5. Other Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yao, X.; Ye, F.; Zhang, M.; Cui, C.; Huang, B.; Niu, P.; Liu, X.; Zhao, L.; Dong, E.; Song, C.; et al. In Vitro Antiviral Activity and Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2020, 7, 1732–1739. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef] [PubMed]
- Vincent, M.J.; Bergeron, E.; Benjannet, S.; Erickson, B.R.; Rollin, P.E.; Ksiazek, T.G.; Seidah, N.G.; Nichol, S.T. Chloroquine is a potent inhibitor of SARS coronavirus infection and spread. Virol. J. 2005, 2, 69. [Google Scholar] [CrossRef] [PubMed]
- Devaux, C.A.; Rolgin, J.M.; Colson, P.; Raoult, D. New insights on the antiviral effects of chloroquine against coronavirus: What to expect for COVID-19? Int. J. Antimicrob. Agents 2020, 55, 105938. [Google Scholar] [CrossRef]
- Gao, J.; Tian, Z.; Yang, X. Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 asso-ciated pneumonia in clinical studies. Biosci. Trends 2020, 14, 72–73. [Google Scholar] [CrossRef]
- Kang, S.; Peng, W.; Zhu, Y.; Lu, S.; Zhou, M.; Lin, W.; Wu, W.; Huang, S.; Jiang, L.; Luo, X.; et al. Recent progress in understanding 2019 novel coronavirus (SARS-CoV-2) associated with human respiratory disease: Detection, mechanisms and treatment. Int. J. Antimicrob. Agents 2020, 55, 105950. [Google Scholar] [CrossRef]
- Giovane, R.A.; Rezai, S.; Cleland, E.; Henderson, C.E. Current pharmacological modalities for management of novel coronavirus disease 2019 (COVID-19) and the rationale for their utilization: A review. Rev. Med. Virol. 2020, 30, e2136. [Google Scholar] [CrossRef]
- Keshtkar-Jahromi, M.; Bavari, S. A Call for Randomized Controlled Trials to test the Efficacy of Chloroquine and Hy-droxychloroquine as Therapeutics against Novel Coronavirus Disease (COVID-19). Am. J. Trop. Med. Hyg. 2020, 102, 932–933. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Coronavirus (COVID-19) Update: Daily Roundup March 30, 2020. Available online: https://www.fda.gov/news-events/pressannouncements/coronavirus-covid-19-update-dailyroundup-march-30-2020 (accessed on 25 April 2020).
- European Medicines Agency. COVID-19: Chloroquine and Hydroxychloroquine Only to Be Used in Clinical Trials or Emergency Use Programmes. EMA/170590/2020. Available online: https://www.ema.europa.eu/en/news/covid-19-chloroquine-hydroxychloroquine-only-be-used-clinical-trials-emergency-use-programmes (accessed on 25 April 2020).
- Mitjà, O.; Clotet, B. Use of antiviral drugs to reduce COVID-19 transmission. Lancet Glob. Health 2020, 8, e639–e640. [Google Scholar] [CrossRef]
- Revollo, B.; Tebe, C.; Peñafiel, J.; Blanco, I.; Perez-Alvarez, N.; Lopez, R.; Rodriguez, L.; Ferrer, J.; Ricart, P.; Moret, E.; et al. Hydroxychloroquine pre-exposure prophylaxis for COVID-19 in healthcare workers. J. Antimicrob. Chemother. 2020, 76, 827–829. [Google Scholar] [CrossRef]
- Taylor, W.R.; White, N.J. Antimalarial drug toxicity: A review. Drug Saf. 2004, 27, 25–61. [Google Scholar] [CrossRef] [PubMed]
- Chatre, C.; Roubille, F.; Vernhet, H.; Jorgensen, C.; Pers, Y.M. Cardiac Complications Attributed to Chloroquine and Hy-droxychloroquine: A Systematic Review of the Literature. Drug Saf. 2018, 41, 919–931. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Mano, T.; Iwata, A.; Toda, T. Neuropsychiatric adverse events of chloroquine: A real-world pharmacovigilance study using the FDA Adverse Event Reporting System (FAERS) database. Biosci. Trends 2020, 14, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Kashour, Z.; Riaz, M.; Garbati, M.A.; AlDosary, O.; Tlayjeh, H.; Gerberi, D.; Murad, M.H.; Sohail, M.R.; Kashour, T.; Tleyjeh, I.M. Efficacy of chloroquine and hydroxychloroquine in COVID-19 patients: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2021, 71, 30–42. [Google Scholar] [CrossRef]
- Cui, X.; Sun, J.; Minkove, S.J.; Li, Y.; Cooper, D.; Couse, Z.; Eichacker, P.Q.; Torabi-Parizi, P. Effects of chloroquine or hydroxychloroquine treatment on non-SARS-CoV2 viral infections: A systematic review of clinical studies. Rev. Med. Virol. 2021, 31, e2228. [Google Scholar] [CrossRef]
- Fiolet, T.; Guihur, A.; Rebeaud, M.E.; Mulot, M.; Peiffer-Smadja, N.; Mahamat-Saleh, Y. Effect of hydroxychloroquine with or without azithromycin on the mortality of coronavirus disease 2019 (COVID-19) patients: A systematic review and me-ta-analysis. Clin. Microbiol. Infect. 2021, 27, 19–27. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Marin, S.; Martin, A.; Bosch, M.; Rodríguez, C.; Pérez-Ricart, A.; Quiñones, C. A Systematic Review on the Early Toxicity and Its Long-Term Consequences of Oral Chloroquine and Hydroxychloroquine on Patients Suffering from Malaria, Amebiasis, Connective Tissue Diseases, Rheumatoid Conditions, Porphyria Cutanea Tarda and COVID-19. PROSPERO 2020 CRD42020180708. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020180708 (accessed on 30 July 2021).
- World Health Organization. WHO Collaborating Centre for Drug Statistics Methodology [Online]. Available online: http://www.whocc.no/atc_ddd_index (accessed on 1 April 2020).
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D.; CARE Group. The CARE Guidelines: Consensus-Based Clinical Case Reporting Guideline Development. Glob. Adv. Health Med. 2013, 2, 38–43. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Contr. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Naranjo, C.A.; Busto, U.; Sellers, E.M.; Sandor, P.; Ruiz, I.; Roberts, E.A.; Janecek, E.; Domecq, C.; Greenblatt, D.J. A method for estimating the probability of adverse drug reactions. Clin. Pharmacol. Ther. 1981, 30, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [PubMed]
- Fisher, S. Psoriatic erythroderma, rheumatoid arthritis, and death, as a sequence to a drug reaction. J. Maine Med. Assoc. 1961, 52, 57–59. [Google Scholar] [PubMed]
- Skog, E. Systemic eczematous contact-type dermatitis induced by iodochlorhydroxyquin and chloroquine phosphate. Contact Dermat. 1975, 1, 187. [Google Scholar] [CrossRef]
- Kanwar, A.J.; Singh, O.P. Toxic epidermal necrolysis-drug induced. Indian J. Dermatol. 1976, 21, 73–77. [Google Scholar]
- Olsen, T.G. Chloroquine and Psoriasis. Ann. Intern. Med. 1981, 94, 546–547. [Google Scholar] [CrossRef]
- Luzar, M.J. Hydroxychloroquine in psoriatic arthropathy: Exacerbations of psoriatic skin lesions. J. Rheumatol. 1982, 9, 462–464. [Google Scholar]
- Spencer, H.C.; Poulter, N.R.; Lury, J.D.; Poulter, C.J. Chloroquine-associated pruritus in a European. Br. Med. J. (Clin. Res. Ed.) 1982, 285, 1703–1704. [Google Scholar] [CrossRef]
- Bhasin, V.; Goel, S.; Srivastava, V.K. Role of pantothenic acid in chloroquine induced skin toxicity. J. Indian Med. Assoc. 1984, 82, 447–448. [Google Scholar]
- Gray, R.G. Hydroxychloroquine provocation of psoriasis. J. Rheumatol. 1985, 12, 391. [Google Scholar]
- Hudson, L.D. Erythema annulare centrifugum: An unusual case due to hydroxychloroquine sulfate. Cutis 1985, 36, 129–130. [Google Scholar] [PubMed]
- Lotem, M.; Ingber, A.; Segal, R.; Sandbank, M. Generalized pustular drug rash induced by hydroxychloroquine. Acta Derm. Venereol. 1990, 70, 250–251. [Google Scholar] [PubMed]
- Vestey, J.; Savin, J. Psoriasis worsened by antimalarial prophylaxis. J. Infect. 1992, 24, 211–212. [Google Scholar] [CrossRef]
- Assier-Bonnet Saada, V.; Bernier, M.; Clerici, T.; Saïag, P. Acute generalized exanthematous pustulosis induced by hydroxychloroquine. Dermatology 1996, 193, 70–71. [Google Scholar] [CrossRef] [PubMed]
- Wilairatana, P.; Looareesuwan, S.; Riganti, M.; Teja-Isavadharm, P.; Keeratithakul, D.; Eickmeyer, S.; Walsh, D.S. Pustular eruption in a malaria patient treated with chloroquine. Int. J. Dermatol. 1998, 37, 713–714. [Google Scholar]
- Murphy, M.; Carmichael, A.J. Fatal toxic epidermal necrolysis associated with hydroxychloroquine. Clin. Exp. Dermatol. 2001, 26, 457–458. [Google Scholar] [CrossRef]
- Leckie, M.J.; Rees, R.G. Stevens-Johnson syndrome in association with hydroxychloroquine treatment for rheumatoid arthritis. Rheumatology 2002, 41, 473–474. [Google Scholar] [CrossRef]
- Welsch, M.J. Acute pustular psoriasis complicated by leukocytoclastic vasculitis. J. Drugs Dermatol. 2003, 2, 193–197. [Google Scholar]
- Evans, C.C.; Bergstresser, P.R. Acute generalized exanthematous pustulosis precipitated by hydroxychloroquine. J. Am. Acad. Dermatol. 2004, 50, 650–651. [Google Scholar] [CrossRef]
- Ghaffarpour, G.; Jalali, M.H.; Yaghmaii, B.; Mazloomi, S.; Soltani-Arabshahi, R. Chloroquine/hydroxychloroquine-induced pemphigus. Int. J. Dermatol. 2006, 45, 1261–1263. [Google Scholar] [CrossRef]
- Gül, U.; Cakmak, S.K.; Kiliç, A.; Gönül, M.; Bilgili, S. A case of hydroxychloroquine induced pruritus. Eur. J. Dermatol. 2006, 16, 586–587. [Google Scholar] [PubMed]
- Mates, M.; Zevin, S.; Breuer, G.S.; Navon, P.; Nesher, G. Desensitization to hydroxychloroquine--experience of 4 patients. J. Rheumatol. 2006, 33, 814–816. [Google Scholar] [PubMed]
- Atzori, L.; Pinna, A.; Pilloni, L.; Ferreli, C.; Aste, N.; Zucca, M.; Pau, M.; Aste, N. Acute generalized exanthematous pustulosis: The experience of an Italian drug-surveillance centre. G. Ital. Dermatol. Venereol. 2007, 142, 303–310. [Google Scholar]
- Volpe, A.; Marchetta, A.; Caramaschi, P.; Biasi, D.; Bambara, L.M.; Arcaro, G. Hydroxychloroquine-induced DRESS syndrome. Clin. Rheumatol. 2008, 27, 537–539. [Google Scholar] [CrossRef] [PubMed]
- Das, J.K.; Medhi, J.; Chakravarty, R.; Soibam, R. Mucous membrane grafting for the post-Steven-Johnson syndrome symblepharon: A case report. Indian J. Ophthalmol. 2011, 59, 231–233. [Google Scholar] [CrossRef] [PubMed]
- Awad, P.; Wulf, A.; Kawas, D. Reacción adversa a hidroxicloroquina. Rev. Chil. Dermatol. 2013, 29, 197–198. [Google Scholar]
- Bailey, K.; McKee, D.; Wismer, J.; Shear, N. Acute Generalized Exanthematous Pustulosis Induced by Hydroxychloroquine: First Case Report in Canada and Review of the Literature. J. Cutan. Med. Surg. 2013, 17, 414–418. [Google Scholar] [CrossRef]
- Cameron, M.C.; Word, A.P.; Dominguez, A. Hydroxychloroquine-induced fatal toxic epidermal necrolysis complicated by angioinvasive rhizopus. Dermatol. Online J. 2014, 20, 4. [Google Scholar] [CrossRef]
- Pastushenko, I.; Gracia-Cazaña, T.; Morales-Moya, A.L.; Grasa, M.P. Acute cutaneous pustular eruption due to hydroxychloroquine. Med. Clin. 2014, 143, e13. [Google Scholar] [CrossRef]
- Soria, A.; Barbaud, A.; Assier, H.; Avenel-Audran, M.; Tétart, F.; Raison-Peyron, N.; Amarger, S.; Girardin, P.; Francès, C.; FISARD (French Investigators for Skin Adverse Reaction to Drugs). Cutaneous Adverse Drug Reactions with Antimalarials and Allergological Skin Tests. Dermatology 2015, 231, 353–359. [Google Scholar] [CrossRef]
- Pearson, K.C.; Morrell, D.S.; Runge, S.R.; Jolly, P. Prolonged pustular eruption from hydroxychloroquine: An unusual case of acute generalized exanthematous pustulosis. Cutis 2016, 97, 212–216. [Google Scholar] [PubMed]
- Abou Assalie, N.; Durcan, R.; Durcan, L.; Petri, M.A. Hydroxychloroquine-induced erythema multiforme. J. Clin. Rheumatol. 2017, 23, 127–128. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, T.; Ly, N.T.M.; Kambe, N.; Nguyen, C.; Ueda-Hayakawa, I.; Son, Y.; Okamoto, H. Early cutaneous eruptions after oral hydroxychloroquine in a lupus erythematosus patient: A case report and review of the published work. J. Dermatol. 2017, 45, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.A.; Patel, T. Palmoplantar exfoliation due to chloroquine. Indian J. Pharmacol. 2017, 49, 205–207. [Google Scholar] [CrossRef] [PubMed]
- Mercogliano, C.; Khan, M.; Lin, C.; Mohanty, E.; Zimmerman, R. AGEP overlap induced by hydroxychloroquine: A case report and literature review. J. Community Hosp. Intern. Med. Perspect. 2018, 8, 360–362. [Google Scholar] [CrossRef]
- Randhawa, A.; Wylie, G. A case of an acute cutaneous drug reaction with hydroxychloroquine. Scott. Med. J. 2018, 63, 91–94. [Google Scholar] [CrossRef]
- Balamurugesan, K.; Davis, P.; Ponprabha, R.; Sarasveni, M. Chloroquine induced urticaria: A newer adverse effect. J. Fam. Med. Prim. Care 2019, 8, 2545–2547. [Google Scholar] [CrossRef]
- Girijala, R.L.; Siddiqi, I.; Kwak, Y.; Wright, D.; Patel, D.B.; Goldberg, L.H. Pustular DRESS Syndrome Secondary to Hydroxychloroquine with EBV Reactivation. J. Drugs Dermatol. 2019, 18, 207–209. [Google Scholar]
- Manzo, C.; Pollio, N.; Natale, M. Sweet’s Syndrome Following Therapy with Hydroxychloroquine in a Patient Affected with Elderly-Onset Primary Sjogren’s Syndrome. Medicines 2019, 6, 111. [Google Scholar] [CrossRef]
- Ullah, A.; Zeb, H.; Khakwani, Z.; Murphy, F.T. Hydroxychloroquine-induced inverse psoriasis. BMJ Case Rep. 2019, 12, e224619. [Google Scholar] [CrossRef]
- Matsuda-Hirose, H.; Sho, Y.; Yamate, T.; Nakamura, Y.; Saito, K.; Takeo, N.; Nishida, H.; Ishii, K.; Sugiura, K.; Hatano, Y. Acute generalized exanthematous pustulosis induced by hydroxychloroquine successfully treated with etretinate. J. Dermatol. 2019, 47, e53–e54. [Google Scholar] [CrossRef] [PubMed]
- Burrell, Z.L.; Martinez, A.C. Chloroquine and Hydroxychloroquine in the Treatment of Cardiac Arrhythmias. N. Engl. J. Med. 1958, 258, 798–800. [Google Scholar] [CrossRef] [PubMed]
- Dornhorst, A.C.; Robinson, B.J. Chloroquine psychosis? Lancet 1963, 1, 118. [Google Scholar] [CrossRef]
- Rab, S.M. Two Cases of Chloroquine Psychosis. BMJ 1963, 1, 1275. [Google Scholar] [CrossRef] [PubMed]
- Oscar, L. Toxic psychosis due to quinacrine and chloroquine. JAMA 1964, 187, 373–375. [Google Scholar]
- Kabir, S.M. Chloroquine psychosis. Trans. R. Soc. Trop. Med. Hyg. 1969, 63, 549. [Google Scholar] [CrossRef]
- Bomb, B.S.; Bedi, H.K.; Bhatnagar, L.K. Chloroquine psychosis. Trans. R. Soc. Trop. Med. Hyg. 1975, 69, 123. [Google Scholar] [CrossRef]
- Das, E.M.; Mohan, D. Chloroquine-related depression. Indian J. Psychiatry 1981, 23, 184–185. [Google Scholar]
- Mohan, D.; Mohandas, E.; Rajat, R. Chloroquine psychosis: A chemical psychosis? J. Natl. Med. Assoc. 1981, 73, 1073–1076. [Google Scholar]
- Ward, W.Q.; Walter-Ryan, W.G.; Shehi, G.M. Toxic psychosis: A complication of antimalarial therapy. J. Am. Acad. Dermatol. 1985, 12, 863–865. [Google Scholar] [CrossRef]
- Akhtar, S.; Mukherjee, S. Chloroquine Induced Mania. Int. J. Psychiatry Med. 1993, 23, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Telgt, D.S.; van der Ven, A.J.; Schimmer, B.; Droogleever-Fortuyn, H.A. Serious psychiatric symptoms after chloroquine treatment following experi-mental malaria infection. Ann. Pharmacother. 2005, 39, 551–554. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, S.; Kumar, M.; Sinha, V.K. Chloroquine-Induced Recurrent Psychosis. Am. J. Ther. 2007, 14, 406–407. [Google Scholar] [CrossRef] [PubMed]
- Plesnicar, B.; Velikonja, I.; Vitorovic, S. Two Challenge and Rechallenge Episodes of Chloroquine-Induced Psychotic Mania in a Patient with Rheumatoid Arthritis. Aktuel. Rheumatol. 2013, 38, 177–179. [Google Scholar] [CrossRef]
- Bogaczewicz, J.; Sobów, T.; Robak, E.; Bienkowski, P.; Sysa-Jędrzejowska, A.; Woźniacka, A. Exacerbations of bipolar disorder triggered by chloroquine in systemic lupus erythematosus—A case report. Lupus 2014, 23, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Bogaczewicz, A.; Sobów, T.; Bienkowski, P.; Kowalski, J.; Wozniacka, A. Chloroquine-induced subacute paranoid-like disorder as a complication of dermatological treatment. Int. J. Dermatol. 2016, 55, 1378–1380. [Google Scholar] [CrossRef]
- Choughule, A.; Salunkhe, R. Chloroquine induced psychosis in an adult patient with amoebic liver abscess: A case report. Indian J. Ment. Health 2019, 6, 115–118. [Google Scholar]
- Torrey, E.F. Chloroquine seizures. JAMA 1968, 204, 867–870. [Google Scholar] [CrossRef]
- Umez-Eronini, E.M.; Eronini, E.A. Chloroquine induced involuntary movements. BMJ 1977, 1, 945–946. [Google Scholar] [CrossRef]
- Singh, R.P.; Sinha, A.K. Neuropsychiatric toxicity of chloroquine. J. Indian Med. Assoc. 1981, 77, 133–134. [Google Scholar]
- Fish, D.R.; Espir, M.L. Convulsions associated with prophylactic antimalarial drugs: Implications for people with epilepsy. BMJ 1988, 297, 526–527. [Google Scholar] [CrossRef] [PubMed]
- James, R.F. Cerebellar ataxia in patients with malaria treated with chloroquine. Postgrad. Med. J. 1988, 64, 167. [Google Scholar] [CrossRef] [PubMed]
- Cras, P.; Martin, J.J. Transient global amnesia following ingestion of chloroquine. J. Neurol. Neurosurg. Psychiatry 1990, 53, 926. [Google Scholar] [CrossRef] [PubMed]
- De Bleecker, J.; De Reuck, J.; Quatacker, J.; Meire, F. Persisting chloroquine-induced myasthenia? Acta Clin. Belg. 1991, 46, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Adamolekun, B. Seizures associated with chloroquine therapy. Cent. Afr. J. Med. 1992, 38, 350–352. [Google Scholar]
- Mulhauser, P.; Allemann, Y.; Regamey, C. Chloroquine and Nonconvulsive Status Epilepticus. Ann. Intern. Med. 1995, 123, 76. [Google Scholar] [CrossRef]
- Ebenso, B.E. Seizures following chloroquine treatment of type II lepra reaction: A case report. Lepr. Rev. 1998, 69, 178–181. [Google Scholar] [CrossRef]
- Martin, A.N.; Tsekes, D.; White, W.J.; Rossouw, D. Chloroquine-induced bilateral anterior shoulder dislocation: A unique aetiology for a rare clinical problem. BMJ Case Rep. 2016, 2016, bcr2015214292. [Google Scholar] [CrossRef]
- Manzo, C.; Gareri, P.; Castagna, A. Psychomotor Agitation Following Treatment with Hydroxychloroquine. Drug Saf. Case Rep. 2017, 4, 6. [Google Scholar] [CrossRef]
- Sogani, R.K.; Sharma, D.K.; Gupta, V. Cardiovascular collapse following small dose of chloroquin in healthy young adult. J. Assoc. Physicians India 1986, 34, 534. [Google Scholar]
- Siqueira-Batista, R.; Ramos Júnior, A.N.; Pessanha, B.S.; Sforza-de-Almeida, M.P.; Potsch, D.F. Chloroquine and cardiac arrhythmia: Case report. East Afr. Med. J. 1998, 75, 117–119. [Google Scholar] [PubMed]
- Comín-Colet, J.; Sánchez-Corral, M.A.; Alegre-Sancho, J.J.; Valverde, J.; López-Gómez, D.; Sabaté, X.; Juan-Mas, A.; Esplugas, E. Complete heart block in an adult with systemic lupus erythe-matosus and recent onset of hydroxychloroquine therapy. Lupus 2001, 10, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.H.; Tuan, T.C.; Lin, Y.J.; Ding, Y.A.; Kong, C.W. Implanted pacemaker failure caused by the antirheumatic drug hydroxychloroquine. Lupus 2003, 12, 725–727. [Google Scholar] [CrossRef] [PubMed]
- Yelve, K.; Phatak, S.; Patil, M.A.; Pazare, A.R. Syncope in a patient being treated for hepatic and intestinal amoebiasis. BMJ Case Rep. 2012, 2012, bcr2012006687. [Google Scholar] [CrossRef] [PubMed]
- Morgan, N.D.; Patel, S.V.; Dvorkina, O. Suspected Hydroxychloroquine-Associated QT-Interval Prolongation in a Patient with Systemic Lupus Erythematosus. J. Clin. Rheumatol. 2013, 19, 286–288. [Google Scholar] [CrossRef] [PubMed]
- Abu-Shakra, M.; Lee, P. Hypoglycemia: An unusual adverse reaction to chloroquine. Clin. Exp. Rheumatol. 1994, 12, 95. [Google Scholar]
- Shojania, K.; Koehler, B.E.; Elliott, T. Hypoglycemia induced by hydroxychloroquine in a type II diabetic treated for polyarthritis. J. Rheumatol. 1999, 26, 195–196. [Google Scholar]
- Winter, E.M.; van der Meer, A.S.; Eustatia-Rutten, C.; Janssen, M.; Shawkat, E.; Hussain, N.; Myers, J.E.; Gillham, J.; Helbert, M. Hydroxychloroquine as a glucose lowering drug. BMJ Case Rep. 2011, 2011, bcr0620114393. [Google Scholar] [CrossRef]
- Rizvi, I.; Zaman, S.; Zaidi, N.; Asif, M.S.; Abdali, N. Acute life-threatening methaemoglobinaemia following ingestion of chloroquine. BMJ Case Rep. 2012, 2012, bcr1220115383. [Google Scholar] [CrossRef]
- Demir, D.; Öcal, F.; Abanoz, M.; Dermenci, H. A case of thrombocytopenia associated with the use of hydroxychloroquine following open heart surgery. Int. J. Surg. Case Rep. 2014, 5, 1282–1284. [Google Scholar] [CrossRef]
- Fromm, L.M. Suspected hydroxychloroquine-induced thrombotic thrombocytopaenic purpura. J. Pharm. Pract. Res. 2018, 48, 72–75. [Google Scholar] [CrossRef]
- Rubin, M.L.; Thomas, W.C., Jr. Diplopia and loss of accommodation due to chloroquine. Arthritis Rheum. 1970, 13, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Prince, D.S.; Hardin, J.G. Hydroxychloroquine-induced vertigo. JAMA 1975, 233, 984. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.K.; Bhatia, B.P.R.; Malik, G.K. Chloroquine causing vestibular toxicity. Indian J. Otolaryngol. Head Neck Surg. 1977, 29, 191. [Google Scholar] [CrossRef]
- Dwivedi, G.S.; Mehra, Y.N. Ototoxicity of Chloroquine Phosphate. A case report. J. Laryngol. Otol. 1978, 92, 701–703. [Google Scholar] [CrossRef]
- Fleury, O.; Droitcourt, C.; Polard, E.; Chevrant-Breton, J. Reversible ageusia as an adverse effect of hydroxychloroquine treatment. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 604–605. [Google Scholar] [CrossRef]
- Giner Galvañ, V.; Oltra, M.R.; Rueda, D.; Esteban, M.J.; Redón, J. Severe acute hepatitis related to hydroxychloroquine in a woman with mixed connective tissue disease. Clin. Rheumatol. 2007, 26, 971–972. [Google Scholar] [CrossRef]
- Sunkara, B.; Roofeh, D.; Silver, S.; Pearson, T.L.; Ettel, M.; McCune, W.J. The devil’s in the dosing: Severe drug-induced liver injury in a hydroxychloroquine-naive patient with subacute cutaneous lupus erythematosus and porphyria cutanea tarda. Lupus 2018, 27, 1383–1386. [Google Scholar] [CrossRef]
- Liu, A.C. Hepatotoxic reaction to chloroquine phosphate in a patient with previously unrecognized porphyria cutanea tarda. West. J. Med. 1995, 162, 548–551. [Google Scholar]
- Makin, A.J.; Wendon, J.; Fitt, S.; Portmann, B.C.; Williams, R. Fulminant hepatic failure secondary to hydroxychloroquine. Gut 1994, 35, 569–570. [Google Scholar] [CrossRef]
- Kutz, D.C.; Bridges, A.J. Bullous rash and brown urine in a systemic lupus erythematosus patient treated with hydroxychlo-roquine. Arthritis Rheum. 1995, 38, 440–443. [Google Scholar] [CrossRef] [PubMed]
- Baler, G.R. Porphyria precipitated by hydroxychloroquine treatment of systemic lupus erythematosus. Cutis 1976, 17, 96–98. [Google Scholar] [PubMed]
- Davis, T.M.E.; Syed, D.A.; Ilett, K.F.; Barrett, P.H.R. Toxicity Related to Chloroquine Treatment of Resistant Vivax Malaria. Ann. Pharmacother. 2003, 37, 526–529. [Google Scholar] [CrossRef] [PubMed]
- Richter, J.G.; Becker, A.; Ostendorf, B.; Specker, C.; Stoll, G.; Neuen-Jacob, E.; Schneider, M. Differential diagnosis of high serum creatine kinase levels in systemic lupus ery-thematosus. Rheumatol. Int. 2003, 23, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Bolaños-Meade, J.; Zhou, L.; Hoke, A.; Corse, A.; Vogelsang, G.; Wagner, K.R. Hydroxychloroquine causes severe vacuolar myopathy in a patient with chronic graft-versus-host disease. Am. J. Hematol. 2005, 78, 306–309. [Google Scholar] [CrossRef]
- Knudsen, L.; Gugger, M.; Dumont, P.; Nicod, L.; von Garnier, C. A Rare Cause of Acute Respiratory Failure and Elevated Eosinophils in Broncho-Alveolar Lavage Fluid. Respiration 2009, 77, 224–228. [Google Scholar] [CrossRef]
- Donado, C.D.; Díez, E.M. Successful Desensitization for Hydroxychloroquine Anaphylaxis. J. Rheumatol. 2010, 37, 1975–1976. [Google Scholar] [CrossRef]
- Carnovale, C.; Perrone, V.; Borsadoli, C.; Mambrini, A.; Speziali, A.; Froldi, G.; Antoniazzi, S.; Magistro, L.; Clementi, E.; Radice, S. A case of urinary incontinence by hydroxychloroquine in a geriatric patient. J. Clin. Pharm. Ther. 2013, 38, 169–171. [Google Scholar] [CrossRef]
- Català, R.; Azón Masoliver, A. Hernández Flix SInterstitial lung disease induced by hydroxychloroquine. Med. Clin. 2015, 145, 415–416. [Google Scholar] [CrossRef]
- Ishiguro, Y.; Muro, Y.; Murase, C.; Takeichi, T.; Kono, M.; Adachi, R.; Takahashi, K.; Akiyama, M. Drug-induced acute eosinophilic pneumonia due to hydroxychloroquine in a chilblain lupus patient. J. Dermatol. 2019, 46, e356–e357. [Google Scholar] [CrossRef]
- Ganjei, Z.; Bahmani, K. A case report of hydroxychloroquine-induced auditory and visual hallucination. Int. J. Clin. Pharmacol. Ther. 2021, 59, 254–256. [Google Scholar] [CrossRef] [PubMed]
- Weinke, T.; Held, T.; Trautmann, M.; Rögler, G.; Mravak, S.; Alexander, M.; Pohle, H.D. Malaria therapy in 452 patients, with special reference to the use of quinine. J. Infect. 1992, 25, 173–180. [Google Scholar] [CrossRef]
- Bussaratid, V.; Walsh, D.S.; Wilairatana, P.; Krudsood, S.; Silachamroon, U.; Looareesuwan, S. Frequency of pruritus in Plasmodium vivax malaria patients treated with chloroquine in Thailand. Trop. Dr. 2000, 30, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Olayemi, O.; Fehintola, F.; Osungbade, A.; Aimakhu, C.; Udoh, E.; Adeniji, A. Pattern of chloroquine-induced pruritus in antenatal patients at the University College Hospital, Ibadan. J. Obstet. Gynaecol. 2003, 23, 490–495. [Google Scholar] [CrossRef]
- Gama, H.; Ismael, A.; Sitoi, F.; Matola, A.; Barros, H.; Lunet, N. Factors associated with chloroquine-induced pruritus during malaria treatment in Mozam-bican university students. Gac. Sanit. 2009, 23, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Jeevangi, S.R.; Manjunath, S.; Awanti, S.M. Prescription pattern of anti-malarial drugs in a tertiary care hospital. Asian Pac. J. Trop. Med. 2010, 3, 337–420. [Google Scholar]
- Ballut, P.C.; Siqueira, A.M.; Orlando, A.C.; Alexandre, M.A.; Alecrim, M.G.C.; Lacerda, M.V. Prevalence and risk factors associated to pruritus in Plasmodium vivax patients using chloroquine in the Brazilian Amazon. Acta Trop. 2013, 128, 504–508. [Google Scholar] [CrossRef]
- Chasset, F.; Arnaud, L.; Jachiet, M.; Monfort, J.-B.; Bouaziz, J.-D.; Cordoliani, F.; Bagot, M.; Barbaud, A.; Francès, C. Changing antimalarial agents after inefficacy or intolerance in patients with cutaneous lupus erythematosus: A multicenter observational study. J. Am. Acad. Dermatol. 2018, 78, 107–114.e1. [Google Scholar] [CrossRef]
- Kishi, C.; Motegi, S.I.; Yasuda, M.; Ishikawa, O. Therapeutic efficacy and adverse events of hydroxychloroquine administration in Jap-anese systemic/cutaneous lupus erythematosus patients. J. Dermatol. 2018, 45, 1020–1022. [Google Scholar] [CrossRef]
- Gonzalez, C.D.; Hansen, C.; Clarke, J.T. Adverse cutaneous drug reactions with antimalarials in cutaneous lupus and derma-tomyositis: A retrospective cohort study. J. Am. Acad. Dermatol. 2019, 81, 859–860. [Google Scholar] [CrossRef]
- Petersen, C.S.; Thomsen, K. High dose hydroxychloroquine treatment of porphyria cutanea tarda. J. Am. Acad. Dermatol. 1992, 26, 614–619. [Google Scholar] [CrossRef]
- Rossmann-Ringdahl, I.; Olsson, R. Porphyria cutanea tarda: Effects and risk factors for hepatotoxicity from high-dose chlo-roquine treatment. Acta Derm. Venereol. 2007, 87, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Seth, S.; Khan, D.A. The Comparative Safety of Multiple Alternative Agents in Refractory Chronic Urticaria Patients. J. Allergy Clin. Immunol. Pract. 2016, 5, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Gozal, D.; Hengy, C.; Fadat, G. Prolonged malaria prophylaxis with chloroquine and proguanil (chloroguanide) in a nonim-mune resident population of an endemic area with a high prevalence of chloroquine resistance. Antimicrob. Agent Chemother. 1991, 35, 373–376. [Google Scholar] [CrossRef] [PubMed]
- McClean, K.L.; Hitchman, D.; Shafran, S.D. Norfloxacin Is Inferior to Chloroquine for Falciparum Malaria in Northwestern Zambia: A Comparative Clinical Trial. J. Infect. Dis. 1992, 165, 904–907. [Google Scholar] [CrossRef]
- Dunne, M.W.; Dev, V.; Valecha, N.; Singh, N.; Shukla, M.; Devi, C.U.; Patki, K.; Yadav, R.S.; Bhattacharyya, P.C.; Mohapatra, M.K.; et al. A Double-blind, randomized study of azithromycin compared to chloroquine for the treatment of plasmodium vivax malaria in india. Am. J. Trop. Med. Hyg. 2005, 73, 1108–1111. [Google Scholar] [CrossRef]
- Ratcliff, A.; Siswantoro, H.; Kenangalem, E.; Wuwung, M.; Brockman, A.; Edstein, M.; Laihad, F.; Ebsworth, E.; Anstey, N.; Tjitra, E.; et al. Therapeutic response of multidrug-resistant Plasmodium falciparum and P. vivax to chloroquine and sulfadoxine–pyrimethamine in southern Papua, Indonesia. Trans. R. Soc. Trop. Med. Hyg. 2007, 101, 351–359. [Google Scholar] [CrossRef]
- Massaga, J.J.; Lusingu, J.P.; Makunde, R.; Malebo, H.M.; Chile, M.M.; Akida, J.A.; Lemnge, M.M.; Rønn, A.M.; Theander, T.G.; Bygbjerg, I.C.; et al. Biological and haematological safety profile of oral amodiaquine and chloroquine in healthy volunteers with or without Plasmodium falciparum infection in northeast Tanzania. Tanzan. J. Health Res. 2008, 10, 144–150. [Google Scholar] [CrossRef]
- Haar, D.; Sølvkjær, M.; Unger, B.; Rasmussen, K.-J.E.; Christensen, L.; Hansen, T.M. A Double-blind Comparative Study of Hydroxychloroquine and Dapsone, Alone and in Combination, in Rheumatoid Arthritis. Scand. J. Rheumatol. 1993, 22, 113–118. [Google Scholar] [CrossRef]
- Van Schaardenburg, D.; Vlkema, R.; Dijkmans, B.A.; Papapoulos, S.; Zwinderman, A.H.; Han, K.H.; Pauwels, E.K.; Breedveld, F.C. Prednisone treatment of elderly-onset rheumatoid arthritis. Disease activity and bone mass in comparison with chloroquine treatment. Arthritis Rheumatol. 1995, 38, 334–342. [Google Scholar] [CrossRef]
- Baltzan, M.; Mehta, S.; Kirkham, T.H.; Cosio, M.G. Randomized Trial of Prolonged Chloroquine Therapy in Advanced Pulmonary Sarcoidosis. Am. J. Respir. Crit. Care Med. 1999, 160, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Dunne, M.W.; Singh, N.; Shukla, M.; Valecha, N.; Bhattacharyya, P.C.; Dev, V.; Patel, K.; Mohapatra, M.K.; Lakhani, J.; Benner, R.; et al. A multicenter study of azithromycin, alone and in combination with chloroquine, for the treatment of acute uncomplicated Plasmodium falciparum malaria in India. J. Infect. Dis. 2005, 191, 1582–1588. [Google Scholar] [CrossRef] [PubMed]
- Sperber, K.; Louie, M.; Kraus, T.; Proner, J.; Sapira, E.; Lin, S.; Stecher, V.; Mayer, L. Hydroxychloroquine treatment of patients with human immunodeficiency virus type 1. Clin. Ther. 1995, 17, 622–636. [Google Scholar] [CrossRef]
- Reeves, G.E.M.; Boyle, M.J.; Bonfield, J.; Dobson, P.; Loewenthal, M. Impact of hydroxychloroquine therapy on chronic urticaria: Chronic autoimmune urticaria study and evaluation. Intern. Med. J. 2004, 34, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Poravuth, Y.; Socheat, D.; Rueangweerayut, R.; Uthaisin, C.; Pyae Phyo, A.; Valecha, N.; Rao, B.H.; Tjitra, E.; Purnama, A.; Borghini-Fuhrer, I.; et al. Pyronaridine-artesunate versus chloroquine in patients with acute Plas-modium vivax malaria: A randomized, double-blind, non-inferiority trial. PLoS ONE 2011, 6, e14501. [Google Scholar] [CrossRef]
- Arnaout, A.; Robertson, S.J.; Pond, G.R.; Lee, H.; Jeong, A.; Ianni, L.; Kroeger, L.; Hilton, J.; Coupland, S.; Gottlieb, C.; et al. A randomized, double-blind, window of opportunity trial evaluating the effects of chloroquine in breast cancer patients. Breast Cancer Res. Treat. 2019, 178, 327–335. [Google Scholar] [CrossRef]
- Watt, G.; Long, G.W.; Padre, L.P.; Alban, P.; Sangalang, R.; Ranoa, C.P. Chloroquine and quinine: A randomized, double-blind comparison of efficacy and side effects in the treatment of Plasmodium falciparum malaria in the Philippines. Trans. R. Soc. Trop. Med. Hyg. 1988, 82, 205–208. [Google Scholar] [CrossRef]
- Cowley, R.G.; Myers, J.E., Jr. Chloroquine in the treatment of infectious mononucleosis. Ann. Intern. Med. 1962, 57, 937–945. [Google Scholar] [CrossRef]
- Schumacher, H.R.; Jacobson, W.A.; BeMiller, C.R. Treatment of Infectious Mononucleosis. Ann. Intern. Med. 1963, 58, 217–228. [Google Scholar] [CrossRef]
- De Lamballerie, X.; Boisson, V.; Reynier, J.C.; Enault, S.; Charrel, R.N.; Flahault, A.; Roques, P.; Le Grand, R. On chikungunya acute infection and chloroquine treatment. Vector Borne Zoonotic Dis. 2008, 8, 837–839. [Google Scholar] [CrossRef]
- Tricou, V.; Minh, N.N.; VAN, T.P.; Lee, S.J.; Farrar, J.; Wills, B.; Tran, H.T.; Simmons, C.P. A Randomized Controlled Trial of Chloroquine for the Treatment of Dengue in Vietnamese Adults. PLoS Negl. Trop. Dis. 2010, 4, e785. [Google Scholar] [CrossRef] [PubMed]
- Borges, M.C.; Castro, L.A.; da Fonseca, B.A.L. Chloroquine use improves dengue-related symptoms. Mem. Inst. Oswaldo Cruz 2013, 108, 596–599. [Google Scholar] [CrossRef] [PubMed]
- Ajayi, A.A.; Oluokun, A.; Sofowora, O.; Akinleye, A. Epidemiology of antimalarial-induced pruritus in Africans. Eur. J. Clin. Pharmacol. 1989, 37, 539–540. [Google Scholar] [CrossRef] [PubMed]
- Katugampola, G.; Katugampola, S. Chloroquine and Psoriasis. Int. J. Dermatol. 1990, 29, 153–154. [Google Scholar] [CrossRef] [PubMed]
- Frías Salcedo, J.A.; Flores Vargas, D. Acute reactions to chloroquine phosphate at the beginning of antimalaria chemopro-phylaxis. Rev. Sanid Mil. 1992, 46, 1–3. [Google Scholar]
- Ajayi, A.A.; Olotu, T.C.; Sofowora, G.G. Knowledge, attitude and practice of prednisolone prevention of chloroquine induced pruritus among Nigerian health workers. Trop. Dr. 1998, 28, 210–211. [Google Scholar] [CrossRef]
- George, A.O. Chloroquine induced pruritus--questionnaire based epidemiological study. Afr. J. Health Sci. 2005, 11, 87–92. [Google Scholar] [CrossRef]
- Obasikene, G.; Adobamen, P.; Okundia, P.; Ogusi, F.O. Prevalence of ototoxicity in University of Benin Teaching Hospital, Benin city: A 5-year review. Niger. J. Clin. Pract. 2012, 15, 453–457. [Google Scholar] [CrossRef]
- Schneider, C.; Adamcova, M.; Jick, S.S.; Schlagenhauf, P.; Miller, M.K.; Rhein, H.-G.; Meier, C.R. Antimalarial chemoprophylaxis and the risk of neuropsychiatric disorders. Travel Med. Infect. Dis. 2013, 11, 71–80. [Google Scholar] [CrossRef]
- Emerole, C.G.; Nneli, R.O.; Osim, E.E. Gender and environmental influences on visual acuity in Owerri, Nigeria. Niger. J. Physiol. Sci. 2014, 29, 17–22. [Google Scholar]
- Sarathi, P.; Sen, D.; Majumdar, R. Psychosis following chloroquine ingestion: A 10-year comparative study from a malar-ia-hyperendemic district of India. Gen. Hosp. Psychiatry 2014, 36, 181–186. [Google Scholar]
- Castro-Cavadía, C.J.; Carmona-Fonseca, J. Assessment of the efficacy and safety of chloroquine monotherapy for the treatment of acute uncomplicated gestational malaria caused by P. vivax, Cordoba, Colombia, 2015–2017. Rev. Colomb. Obstet. Ginecol. 2020, 71, 21–33. [Google Scholar] [PubMed]
- Dugué, A.; Bagheri, H.; Lapeyre-Mestre, M.; Tournamille, J.F.; Sailler, L.; Dedieu, G.; Salvayre, R.; Thouvenot, J.P.; Massip, P.; Montastruc, J.L. Detection and incidence of muscular adverse drug reactions: A prospective analysis from laboratory signals. Eur. J. Clin. Pharmacol. 2004, 60, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.J.; Kedia, M.Ş.; Bajpai, D.; Mehta, S.S.; Kshirsagar, N.A.; Gogtay, N.J. Evaluation of the prevalence and economic burden of adverse drug reactions presenting to the medical emergency department of a tertiary referral centre: A prospective study. BMC Clin. Pharmacol. 2007, 7, 8. [Google Scholar] [CrossRef]
- Sidoroff, A.; Dunant, A.; Viboud, C.; Halevy, S.; Bavinck, J.B.; Naldi, L.; Mockenhaupt, M.; Fagot, J.-P.; Roujeau, J.-C. Risk factors for acute generalized exanthematous pustulosis (AGEP)—results of a multinational case–control study (EuroSCAR). Br. J. Dermatol. 2007, 157, 989–996. [Google Scholar] [CrossRef]
- Walsh, D.S.; Looareesuwan, S.; Wilairatana, P.; Heppner, J.D.G.; Tang, D.B.; Brewer, T.G.; Chokejindachai, W.; Viriyavejakul, P.; Kyle, D.E.; Milhous, W.K.; et al. Randomized Dose-Ranging Study of the Safety and Efficacy of WR 238605 (Tafenoquine) in the Prevention of Relapse of Plasmodium vivax Malaria in Thailand. J. Infect. Dis. 1999, 180, 1282–1287. [Google Scholar] [CrossRef]
- Yanze, M.F.; Duru, C.; Jacob, M.; Bastide, J.M.; Lankeuh, M. Rapid therapeutic response onset of a new pharmaceutical form of chloroquine phosphate 300 mg: Effervescent tablets. Trop. Med. Int. Health 2001, 6, 196–201. [Google Scholar] [CrossRef]
- Tagbor, H.; Bruce, J.; Browne, E.; Randal, A.; Greenwood, B.; Chandramohan, D. Efficacy, safety, and tolerability of amodiaquine plus sulphadoxine-pyrimethamine used alone or in combination for malaria treatment in pregnancy: A randomised trial. Lancet 2006, 368, 1349–1356. [Google Scholar] [CrossRef]
- Sagara, I.; Oduro, A.R.; Mulenga, M.; Dieng, Y.; Ogutu, B.; Tiono, A.B.; Mugyenyi, P.; Sie, A.; Wasunna, M.; Kain, K.C.; et al. Efficacy and safety of a combination of azithromycin and chloroquine for the treatment of uncomplicated Plasmodium falciparum malaria in two multi-country randomized clinical trials in African adults. Malar. J. 2014, 13, 458. [Google Scholar] [CrossRef]
- Kshirsagar, N.A.; Gogtay, N.J.; Moran, D.; Utz, G.; Sethia, A.; Sarkar, S.; Vandenbroucke, P. Treatment of adults with acute uncomplicated malaria with azithromycin and chloroquine in India, Colombia, and Suriname. Res. Rep. Trop. Med. 2017, 8, 85–104. [Google Scholar] [CrossRef]
- Ajayi, A.A.; Akinleye, A.O.; Udoh, S.J.; Ajayi, O.O.; Oyelese, O.; Ijaware, C.O. The effects of prednisolone and niacin on chloroquine-induced pruritus in malaria. Eur. J. Clin. Pharmacol. 1991, 41, 383–385. [Google Scholar] [CrossRef] [PubMed]
- Adebayo, R.A.; Sofowora, G.G.; Onayemi, O.; Udoh, S.J.; Ajayi, A.A. Chloroquine-induced pruritus in malaria fever: Contribution of malaria para-sitemia and the effects of prednisolone, niacin, and their combination, compared with antihistamine. Br. J. Clin. Pharmacol. 1997, 44, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Vouri, S.M.; Thai, T.N.; Winterstein, A.G. An evaluation of co-use of chloroquine or hydroxychloroquine plus azithromycin on cardiac outcomes: A pharmacoepidemiological study to inform use during the COVID19 pandemic. Res. Soc. Adm. Pharm. 2020, 17, 2012–2017. [Google Scholar] [CrossRef] [PubMed]
- Sarayani, A.; Cicali, B.; Henriksen, C.H.; Brown, J.D. Safety signals for QT prolongation or Torsades de Pointes associated with azithromycin with or without chloroquine or hydroxychloroquine. Res. Soc. Adm. Pharm. 2021, 17, 483–486. [Google Scholar] [CrossRef]
- Kimani, J.; Phiri, K.; Kamiza, S.; Duparc, S.; Ayoub, A.; Rojo, R.; Robbins, J.; Orrico, R.; Vandenbroucke, P. Efficacy and Safety of Azithromycin-Chloroquine versus Sulfadoxine-Pyrimethamine for Intermittent Preventive Treatment of Plasmodium falciparum Malaria Infection in Pregnant Women in Africa: An Open-Label, Randomized Trial. PLoS ONE 2016, 11, e0157045. [Google Scholar] [CrossRef]
- Phiri, K.; Kimani, J.; Mtove, G.A.; Zhao, Q.; Rojo, R.; Robbins, J.; Duparc, S.; Ayoub, A.; Vandenbroucke, P. Parasitological Clearance Rates and Drug Concentrations of a Fixed Dose Combination of Azithromycin-Chloroquine in Asymptomatic Pregnant Women with Plasmodium Falciparum Parasitemia: An Open-Label, Non-Comparative Study in Sub-Saharan Africa. PLoS ONE 2016, 11, e0165692. [Google Scholar] [CrossRef]
- Asli, R.; Abdullah, M.S.; Chong, P.L.; Metussin, D.; Momin, R.N.; Mani, B.I.; Chong, V.H. Case report: Right bundle brunch block and QTc prolongation in a patient with novel coronavirus disease (COVID-19) treated with hydroxychloroquine. Am. J. Trop. Med. Hyg. 2020, 103, 79–82. [Google Scholar] [CrossRef]
- Falcão, M.B.; Pamplona de Góes Cavalcanti, L.; Filgueiras Filho, N.M.; de Brito, C.A.A. Case Report: Hepatotoxicity Associated with the Use of Hydroxychloroquine in a Patient with COVID-19. Am. J. Trop. Med. Hyg. 2020, 102, 1214–1216. [Google Scholar] [CrossRef]
- Beauverd, Y.; Adam, Y.; Assouline, B.; Samii, K. COVID-19 infection and treatment with hydroxychloroquine cause severe hae-molysis crisis in a patient with glucose-6-posphate dehydrogenase deficiency. Eur. J. Haematol. 2020, 105, 357–359. [Google Scholar] [CrossRef]
- Kuipers, M.T.; van Zwieten, R.; Heijmans, J.; Rutten, C.E.; de Heer, K.; Kater, A.P.; Nur, E. G6PD deficiency-associated hemolysis and methemoglobinemia in a COVID-19 patient treated with chloroquine. Am. J. Hematol. 2020, 95, E194–E196. [Google Scholar] [CrossRef]
- Kutlu, Ö.; Metin, A. A case of exacerbation of psoriasis after oseltamivir and hydroxychloroquine in a patient with COVID-19: Will cases of psoriasis increase after COVID-19 pandemic? Dermatol. Ther. 2020, 33, e13383. [Google Scholar] [CrossRef] [PubMed]
- Mitra, R.L.; Greenstein, S.A.; Epstein, L.M. An algorithm for managing QT prolongation in coronavirus disease 2019 (COVID 2019) patients treated with either chloroquine or hydroxychloroquine in conjunction with azithromycin: Possible benefits of in-travenous lidocaine. Heart Rhythm. Case Rep. 2020, 6, 244–248. [Google Scholar]
- Robustelli Test, E.; Vezzoli, P.; Carugno, A.; Raponi, F.; Gianatti, A.; Rongioletti, F.; Sena, P. Acute generalized exanthematous pustulosis with erythema multiforme-like lesions in a COVID-19 woman. Eur. Acad. Dermatol. Venereol. 2020, 12, 475–478. [Google Scholar]
- Szekely, Y.; Lichter, Y.; Abu Shrkihe, B.; Bruck, H.; Oster, H.S.; Viskin, S. Chloroquine-induced torsades de pointes in a patient with coronavirus disease 2019. Heart Rhythm 2020, 17, 1452–1455. [Google Scholar] [CrossRef] [PubMed]
- Gracia-Ramos, A.E.; Cortes-Ortiz, A. Wide complex tachycardia in a patient with COVID-19 treated with chloro-quine/azithromycin. Oxf. Med. Case Rep. 2021, 1, omaa124. [Google Scholar] [CrossRef]
- Aslam, W.; Lamb, C.R.; Ali, N. Torsades de pointes in SARS-CoV-2 (COVID-19) pneumonia: Medicine reconciliation and careful monitoring of QTc interval may help prevent cardiac complications. BMJ Case Rep. 2021, 14, e239963. [Google Scholar] [CrossRef]
- Kang, Y.; Wang, H.; Chen, H.; Wang, B.; Yang, Y.; Zhao, X.; Ran, Q.; Wei, J. Suspected Hydroxychloroquine-Induced Sinus Bradycardia and QTc Prolongation in a Patient with COVID-19. Int. Heart J. 2020, 61, 1056–1058. [Google Scholar] [CrossRef]
- Patel, J.; Patel, R.; Rodriguez, L.-M.; Blanco, A.; Hamza, A. Cardiovascular Considerations of Experimental Hydroxychloroquine Therapy on Patients Diagnosed with COVID-19: A Case Series Review. Cureus 2020, 12, e9151. [Google Scholar] [CrossRef]
- Ambar Akkaoui, M.; Lejoyeux, M.; Geoffroy, P.A. Chloroquine-Induced First-Episode Psychosis in a Patient Self-medicated for COVID-19. Biol. Psychiatry 2021, 89, e9. [Google Scholar] [CrossRef]
- Koc, G.; Odabasi, Z.; Tan, E. Myasthenic Syndrome Caused by Hydroxychloroquine Used for COVID-19 Prophylaxis. J. Clin. Neuromuscul. Dis. 2020, 22, 60–62. [Google Scholar] [CrossRef]
- Benjelloun, R.; Otheman, Y.; El Kettani, C. Psychiatric side effects of chloroquine in COVID-19 patients: Two case reports. Pan Afr. Med. J. 2020, 35, 83. [Google Scholar] [CrossRef] [PubMed]
- Sardana, K.; Mathachan, S.R.; Deepak, D.; Khurana, A.; Sinha, S. Cutaneous side effects of hydroxychloroquine in health care workers in a COVID referral hospital—Implications for clinical practice. J. Dermatolog. Treat. 2020, 22, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Monte-Serrano, J.; Cruañes-Monferrer, J.; García-García, M.; García-Gil, M.F. Hydroxychloroquine-induced erythema multiforme in a patient with COVID-19. Med. Clin. (Engl. Ed.) 2020, 155, 231. [Google Scholar] [CrossRef] [PubMed]
- Delaleu, J.; Deniau, B.; Battistella, M.; de Masson, A.; Bensaid, B.; Jachiet, M.; Lazaridou, I.; Bagot, M.; Bouaziz, J.D.; Saint-Louis CORE (COVID Research) Group. Acute generalized exanthematous pustulosis induced by hydroxychloroquine prescribed for COVID-19. J. Allergy Clin. Immunol. Pract. 2020, 8, 2777–2779. [Google Scholar] [CrossRef] [PubMed]
- Enos, T.; Jeong, H.S.; Vandergriff, T.; Jacobe, H.T.; Chong, B.F. Acute generalized exanthematous pustulosis induced by empiric hydroxychloroquine for presumed COVID-19. Dermatol. Ther. 2020, 33, e13834. [Google Scholar] [CrossRef]
- Castro Jiménez, A.; Navarrete Navarrete, N.; Gratacós Gómez, A.R.; Florido López, F.; García Rodríguez, R.; Gómez Torrijos, E. First case of DRESS syndrome caused by hydroxychloroquine with a positive patch test. Contact Dermat. 2021, 84, 50–51. [Google Scholar] [CrossRef]
- Abadías-Granado, I.; Palma-Ruiz, A.; Cerro, P.; Morales-Callaghan, A.; Gómez-Mateo, M.; Gilaberte, Y.; Schwartz, R. Generalized pustular figurate erythema first report in two COVID-19 patients on hydroxychloroquine. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e5–e7. [Google Scholar] [CrossRef]
- Kurd, R.; Zuckerman, M.; Ben-Chetrit, E. Hydroxychloroquine-related Rash in COVID-19 Infected Patient. Isr. Med. Assoc. J. 2020, 22, 525. [Google Scholar]
- Arıkan, F.; Yıldız, Y.; Ercan, T.; Oruç, Ö.; Akçay, S.; Yılmaz, F.; Toptaş, T.; Tuğlular, T. Hydroxychloroquine-Associated Thrombotic Thrombocytopenic Purpura. Turk. J. Hematol. 2020, 37, 302–304. [Google Scholar] [CrossRef]
- Maillart, E.; Leemans, S.; Van Noten, H.; Vandergraesen, T.; Mahadeb, B.; Salaouatchi, M.T.; De Bels, D.; Clevenbergh, P. A case report of serious haemolysis in a glucose-6-phosphate dehydrogenase-deficient COVID-19 patient receiving hydroxychloroquine. Infect. Dis. (Lond.) 2020, 52, 659–661. [Google Scholar] [CrossRef]
- Chaney, S.; Basirat, A.; McDermott, R.; Keenan, N.; Moloney, E. COVID-19 and hydroxychloroquine side-effects: Glucose 6-phosphate dehydrogenase deficiency (G6PD) and acute haemolytic anaemia. QJM 2020, 113, 890–891. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, J.; Averbukh, Y. Hemolytic Anemia in a Glucose-6-Phosphate Dehydrogenase-Deficient Patient Receiving Hy-droxychloroquine for COVID-19: A Case Report. Perm. J. 2020, 24, 158. [Google Scholar] [CrossRef] [PubMed]
- Bessière, F.; Roccia, H.; Delinière, A.; Charrière, R.; Chevalier, P.; Argaud, L.; Cour, M. Assessment of QT Intervals in a Case Series of Patients with Coronavirus Disease 2019 (COVID-19) Infection Treated with Hydroxychloroquine Alone or in Combination with Azithromycin in an Intensive Care Unit. JAMA Cardiol. 2020, 5, 1067–1069. [Google Scholar] [CrossRef] [PubMed]
- Chong, V.H.; Chong, P.L.; Metussin, D.; Asli, R.; Momin, R.N.; Mani, B.I.; Abdullah, M.S. Conduction abnormalities in hydroxychloroquine add on therapy to lop-inavir/ritonavir in COVID-19. J. Med. Virol. 2020, 92, 2322–2324. [Google Scholar] [CrossRef]
- Chorin, E.; Wadhwani, L.; Magnani, S.; Dai, M.; Shulman, E.; Nadeau-Routhier, C.; Knotts, R.; Bar-Cohen, R.; Kogan, E.; Barbhaiya, C.; et al. QT interval prolongation and torsade de pointes in patients with COVID-19 treated with hydroxychloroquine/azithromycin. Heart Rhythm 2020, 17, 1425–1433. [Google Scholar] [CrossRef]
- Cipriani, A.; Zorzi, A.; Ceccato, D.; Capone, F.; Parolin, M.; Donato, F.; Fioretto, P.; Pesavento, R.; Previato, L.; Maffei, P.; et al. Arrhythmic profile and 24-hour QT interval variability in COVID-19 patients treated with hydroxychloroquine and azithromycin. Int. J. Cardiol. 2020, 316, 280–284. [Google Scholar] [CrossRef]
- Tang, W.; Cao, Z.; Han, M.; Wang, Z.; Chen, J.; Sun, W.; Wu, Y.; Xiao, W.; Liu, S.; Chen, E.; et al. Hydroxychloroquine in patients with mainly mild to moderate coronavirus disease 2019: Open label, randomised controlled trial. BMJ 2020, 369, m1849. [Google Scholar] [CrossRef]
- Fernández-Ruiz, M.; Andrés, A.; Loinaz, C.; Delgado, J.F.; López-Medrano, F.; Juan, R.S.; González, E.; Polanco, N.; Folgueira, M.D.; Lalueza, A.; et al. COVID-19 in solid organ transplant recipients: A single-center case series from Spain. Am. J. Transplant. 2020, 20, 1849–1858. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.-C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Sevestre, J.; Mailhe, M.; Doudier, B.; Aubry, C.; Amrane, S.; et al. Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: A pilot observational study. Travel Med. Infect. Dis. 2020, 34, 101663. [Google Scholar] [CrossRef]
- Mahévas, M.; Tran, V.-T.; Roumier, M.; Chabrol, A.; Paule, R.; Guillaud, C.; Fois, E.; Lepeule, R.; Szwebel, T.-A.; Lescure, X.; et al. Clinical efficacy of hydroxychloroquine in patients with COVID-19 pneumonia who require oxygen: Observational comparative study using routine care data. BMJ 2020, 369, m1844. [Google Scholar] [CrossRef]
- Mercuro, N.J.; Yen, C.F.; Shim, D.J.; Maher, T.R.; McCoy, C.M.; Zimetbaum, P.J.; Gold, H.S. Risk of QT interval prolongation associated with use of hydroxychloroquine with or without concomitant azithromycin among hospitalized patients testing postivie for coronavirus disease 2019 (COVID-2019). JAMA Cardiol. 2020, 5, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Million, M.; Lagier, J.-C.; Gautret, P.; Colson, P.; Fournier, P.-E.; Amrane, S.; Hocquart, M.; Mailhe, M.; Esteves-Vieira, V.; Doudier, B.; et al. Early treatment of COVID-19 patients with hydroxychloroquine and azithromycin: A retrospective analysis of 1061 cases in Marseille, France. Travel Med. Infect. Dis. 2020, 35, 101738. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.; Delaugerre, C.; Le Goff, J.; Mela-Lima, B.; Ponscarme, D.; Goldwirt, L.; de Castro, N. No evidence of rapid antiviral clearance or clinical benefit with the combination of hydroxychloroquine and azithromycin in patients with severe COVID-19 infection. Med. Mal. Infect. 2020, 50, 384. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, E.S.; Dufort, E.M.; Udo, T.; Wilberschied, L.A.; Kumar, J.; Tesoriero, J.; Weinberg, P.; Kirkwood, J.; Muse, A.; DeHovitz, J.; et al. Association of Treatment with Hydroxychloroquine or Azithromycin with In-Hospital Mortality in Patients with COVID-19 in New York State. JAMA 2020, 323, 2493–2502. [Google Scholar] [CrossRef] [PubMed]
- Saleh, M.; Gabriels, J.; Chang, D.; Soo Kim, B.; Mansoor, A.; Mahmood, E.; Makker, P.; Ismail, H.; Goldner, B.; Willner, J.; et al. Effect of chloroquine, hydroxychloroquine and azithromycin on the corrected QT interval in patients with SARS-CoV-2 infection. Circ. Arrhythmia Electrophysiol. 2020, 13, e008662. [Google Scholar] [CrossRef]
- Van den Broek, M.P.H.; Möhlmann, J.E.; Abeln, B.G.S.; Liebregts, M.; van Dijk, V.F.; van de Garde, E.M.W. Chloroquine-induced QTc prolongation in COVID-19 patients. Neth. Heart J. 2020, 28, 406–409. [Google Scholar] [CrossRef]
- Borba, M.G.S.; Val, F.F.A.; Sampaio, V.S.; Alexandre, M.A.A.; Melo, G.C.; Brito, M.; Mourão, M.P.G.; Brito-Sousa, J.D.; Baía-da-Silva, D.; Guerra, M.V.F.; et al. Effect of high vs low doses of chloroquine diphosphate as adjunctive therapy for patients hospitalized with severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) infection: A randomized clinical Trial. JAMA Netw. Open 2020, 3, e208857. [Google Scholar] [CrossRef]
- Chen, Z.; Hu, J.; Zhang, Z.; Jiang, S.; Han, S.; Yan, D.; Zhuang, R.; Hu, B.; Zhang, Z. Efficacy of hydroxychloroquine in patients with COVID-19: Results of a randomized clinical trial. MedRxiv 2020. [Google Scholar] [CrossRef]
- Huang, M.; Tang, T.; Pang, P.; Li, M.; Ma, R.; Lu, J.; Shu, J.; You, Y.; Chen, B.; Liang, J.; et al. Treating COVID-19 with Chloroquine. J. Mol. Cell Biol. 2020, 12, 322–325. [Google Scholar] [CrossRef]
- Chen, J.; Liu, D.; Liu, L.; Liu, P.; Xu, Q.; Xia, L.; Ling, Y.; Huang, D.; Song, S.; Zhang, D.; et al. A pilot study of hydroxychloroquine in treatment of patients with common coronavirus disease-19 (COVID-19). J. Zhejiang Univ. 2020, 49, 215–219. [Google Scholar]
- Colaneri, M.; Bogliolo, L.; Valsecchi, P.; Sacchi, P.; Zuccaro, V.; Brandolino, F.; Montecucco, C.; Mojoli, F.; Giusti, E.M.; Bruno, R.; et al. Tocilizumab for Treatment of Severe COVID-19 Patients: Preliminary Results from SMAtteo COvid19 REgistry (SMACORE). Microorganisms 2020, 8, 695. [Google Scholar] [CrossRef] [PubMed]
- Lagier, J.-C.; Million, M.; Gautret, P.; Colson, P.; Cortaredona, S.; Giraud-Gatineau, A.; Honoré, S.; Gaubert, J.-Y.; Fournier, P.-E.; Tissot-Dupont, H.; et al. Outcomes of 3,737 COVID-19 patients treated with hydroxychloroquine/azithromycin and other regimens in Marseille, France: A retrospective analysis. Travel Med. Infect. Dis. 2020, 36, 101791. [Google Scholar] [CrossRef] [PubMed]
- Paccoud, O.; Tubach, F.; Baptiste, A.; Bleibtreu, A.; Hajage, D.; Monsel, G.; Tebano, G.; Boutolleau, D.; Klement, E.; Godefroy, N.; et al. Compassionate Use of Hydroxychloroquine in Clinical Practice for Patients with Mild to Severe COVID-19 in a French University Hospital. Clin. Infect. Dis. 2020, 73, e4064–e4072. [Google Scholar] [CrossRef] [PubMed]
- Hor, C.P.; Hussin, N.; Nalliah, S.; Ooi, W.T.; Tang, X.Y.; Zachariah, S.; Singh, G.P.S.J.; Rani, R.A.; Perumal, K.; Cheah, W.K. Experience of short-term hydroxychloroquine and azithromycin in COVID-19 patients and effect on QTc trend. J. Infect. 2020, 81, e117–e119. [Google Scholar] [CrossRef] [PubMed]
- Mazzanti, A.; Briani, M.; Kukavica, D.; Bulian, F.; Marelli, S.; Trancuccio, A.; Monteforte, N.; Manciulli, T.; Morini, M.; Carlucci, A.; et al. Association of Hydroxychloroquine with QTc Interval in Patients with COVID-19. Circulation 2020, 142, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Workman, V.; Ganeshan, R.; Obasare, E.R.; Burr, A.; DeBiasi, R.M.; Freeman, J.V.; Akar, J.; Lampert, R.; Rosenfeld, L.E. Enhanced electrocardiographic monitoring of patients with Coronavirus Disease 2019. Heart Rhythm 2020, 17, 1417–1422. [Google Scholar] [CrossRef]
- Karolyi, M.; Pawelka, E.; Mader, T.; Omid, S.; Kelani, H.; Ely, S.; Jilma, B.; Baumgartner, S.; Laferl, H.; Ott, C.; et al. Hydroxychloroquine versus lopinavir/ritonavir in severe COVID-19 patients: Results from a real-life patient cohort. Wien Klin. Wochenschr. 2021, 133, 284–291. [Google Scholar] [CrossRef]
- Mitjà, O.; Corbacho-Monné, M.; Ubals, M.; Tebé, C.; Peñafiel, J.; Tobias, A.; Ballana, E.; Alemany, A.; Riera-Martí, N.; Pérez, C.A.; et al. Hydroxychloroquine for Early Treatment of Adults with Mild Covid-19: A Randomized-Controlled Trial. Clin. Infect. Dis. 2021, 73, e4073–e4081. [Google Scholar] [CrossRef]
- Reis, G.; Moreira Silva, E.A.D.S.; Medeiros Silva, D.C.; Thabane, L.; Singh, G.; Park, J.J.H.; Forrest, J.I.; Harari, O.; Quirino Dos Santos, C.V.; Guimarães de Almeida, A.P.F.; et al. Effect of Early Treatment with Hydroxychloroquine or Lopinavir and Ritonavir on Risk of Hospitalization Among Patients with COVID-19: The TOGETHER Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e216468. [Google Scholar] [CrossRef]
- Dabbous, H.M.; El-Sayed, M.H.; El Assal, G.; Elghazaly, H.; Ebeid, F.F.S.; Sherief, A.F.; Elgaafary, M.; Fawzy, E.; Hassany, S.M.; Riad, A.R.; et al. Safety and efficacy of favipiravir versus hydroxychloroquine in management of COVID-19: A randomised controlled trial. Sci. Rep. 2021, 11, 7282. [Google Scholar] [CrossRef]
- Uğurlu Ilgın, B.; Akbulut Koyuncu, İ.M.; Kızıltunç, E. Effect of triple antimicrobial therapy on electrocardiography parameters in patients with mild-to-moderate coronavirus disease 2019. Anatol. J. Cardiol. 2021, 25, 184–190. [Google Scholar] [PubMed]
- Eftekhar, S.P.; Kazemi, S.; Barary, M.; Javanian, M.; Ebrahimpour, S.; Ziaei, N. Effect of Hydroxychloroquine and Azithromycin on QT Interval Prolongation and Other Cardiac Arrhythmias in COVID-19 Confirmed Patients. Cardiovasc. Ther. 2021, 2021, 6683098. [Google Scholar] [CrossRef] [PubMed]
- Lamback, E.B.; de Oliveira, M.A.; Haddad, A.F.; Vieira, A.F.M.; Neto, A.L.F.; Maia, T.d.S.; Chrisman, J.D.R.; Spineti, P.P.D.M.; de Mattos, M.A.; Costa, E. Hydroxychloroquine with azithromycin in patients hospitalized for mild and moderate COVID-19. Braz. J. Infect. Dis. 2021, 25, 101549. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, T.F.; Bradley, C.J.; Abbas, A.E.; Williamson, B.D.; Rusia, A.; Tawney, A.M.; Gaines, R.; Schott, J.; Dmitrienko, A.; Haines, D.E. Hydroxychloroquine/Azithromycin Therapy and QT Prolongation in Hospitalized Patients with COVID-19. JACC Clin. Electrophysiol. 2021, 7, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Falcão, F.; Viegas, E.; Carmo, I.; Soares, J.; Falcao, M.; Solano, M.; Cavaco, P.; Mendes, D.; Rijo, J.; Povoa, P.; et al. A prospective, observational study to evaluate adverse drug reactions in patients with COVID-19 treated with remdesivir or hydroxychloroquine: A preliminary report. Eur. J. Hosp. Pharm. 2021, 28, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Sogut, O.; Can, M.M.; Guven, R.; Kaplan, O.; Ergenc, H.; Umit, T.B.; Demir, O.; Kaya, M.; Akdemir, T.; Cakmak, S. Safety and efficacy of hydroxychloroquine in 152 outpatients with confirmed COVID-19: A pilot observational study. Am. J. Emerg. Med. 2020, 40, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Seyhan, A.U.; Doganay, F.; Yilmaz, E.; Topal, N.P.; Ak, R. Investigation of QT Prolongation with Hydroxychloroquine and Azithromycin for the Treatment of COVID-19. J. Coll. Physicians Surg. Pak. 2020, 30, 153–157. [Google Scholar] [CrossRef]
- Meriglier, E.; Rivoisy, C.; Hessamfar, M.; Bernard, N.; Aureau, I.; Lapoirie, J.; Contis, A.; Sacher, F.; Sacristan, B.; Lahouati, M.; et al. Safety of hydroxychloroquine and darunavir or lopinavir in COVID-19 infection. J. Antimicrob. Chemother. 2020, 76, 482–486. [Google Scholar] [CrossRef]
- Fteiha, B.; Karameh, H.; Kurd, R.; Ziff-Werman, B.; Feldman, I.; Bnaya, A.; Einav, S.; Orlev, A.; Ben-Chetrit, E. QTc prolongation among hydroxychloroquine sulphate-treated COVID-19 patients: An observational study. Int. J. Clin. Pract. 2021, 75, e13767. [Google Scholar] [CrossRef]
- Recovery Collaborative Group. Effect of Hydroxychloroquine in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2020, 383, 2030–2040. [Google Scholar] [CrossRef]
- Saleh, M.; Gabriels, J.; Chang, D.; Fishbein, J.; Qiu, M.; Mountantonakis, S.E.; Epstein, L.M.; Northwell COVID-19 Research Consortium. Safely Administering Potential QTc Prolonging Therapy Across a Large Health Care System in the COVID-19 Era. Circ. Arrhythm. Electrophysiol. 2020, 13, e008937. [Google Scholar] [CrossRef] [PubMed]
- Bernardini, A.; Ciconte, G.; Negro, G.; Rondine, R.; Mecarocci, V.; Viva, T.; Santini, F.; de Innocentiis, C.; Gianelli, L.; Witkowska, E.; et al. Assessing QT interval in COVID-19 patients:safety of hydroxychloro-quine-azithromycin combination regimen. Int. J. Cardiol. 2021, 324, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Furtado, R.H.M.; Berwanger, O.; Fonseca, H.A.; Corrêa, T.D.; Ferraz, L.R.; Lapa, M.G.; Zampieri, F.G.; Veiga, V.C.; Azevedo, L.C.P.; Rosa, R.G.; et al. Azithromycin in addition to standard of care versus standard of care alone in the treatment of patients admitted to the hospital with severe COVID-19 in Brazil (COALITION II): A randomised clinical trial. Lancet 2020, 396, 959–967. [Google Scholar] [CrossRef]
- Giaime, P.; Guenoun, M.; Pedinielli, N.; Narbonne, H.; Bergounioux, J.-P.; Solas, C.; Guilhaumou, R.; Sampol, J.; Ollier, J.; Sichez, H.; et al. Hydroxychloroquine and azithromycin tolerance in haemodialysis patients during COVID-19 infection. Nephrol. Dial. Transplant. 2020, 35, 1346–1353. [Google Scholar] [CrossRef]
- Kalligeros, M.; Shehadeh, F.; Atalla, E.; Mylona, E.K.; Aung, S.; Pandita, A.; Larkin, J.; Sanchez, M.; Touzard-Romo, F.; Brotherton, A.; et al. Hydroxychloroquine use in hospitalised patients with COVID-19: An observational matched cohort study. J. Glob. Antimicrob. Resist. 2020, 22, 842–844. [Google Scholar] [CrossRef]
- Satlin, M.J.; Goyal, P.; Magleby, R.; Maldarelli, G.A.; Pham, K.; Kondo, M.; Schenck, E.J.; Rennert, H.; Westblade, L.F.; Choi, J.J.; et al. Safety, tolerability, and clinical outcomes of hydroxychloroquine for hospitalized patients with coronavirus 2019 disease. PLoS ONE 2020, 15, e0236778. [Google Scholar] [CrossRef]
- Moschini, L.; Loffi, M.; Regazzoni, V.; Di Tano, G.; Gherbesi, E.; Danzi, G.B. Effects on QT interval of hydroxychloroquine associated with ritonavir/darunavir or azithromycin in patients with SARS-CoV-2 infection. Heart Vessels 2021, 36, 115–120. [Google Scholar] [CrossRef]
- Skipper, C.P.; Pastick, K.A.; Engen, N.W.; Bangdiwala, A.S.; Abassi, M.; Lofgren, S.M.; Williams, D.A.; Okafor, E.C.; Pullen, M.F.; Nicol, M.R.; et al. Hydroxychloroquine in Nonhospitalized Adults with Early COVID-19: A Randomized Trial. Ann. Intern. Med. 2020, 173, 623–631. [Google Scholar] [CrossRef]
- Hsia, B.C.; Greige, N.; Quiroz, J.A.; Khokhar, A.S.; Daily, J.; Di Biase, L.; Ferrick, K.J.; Fisher, J.D.; Krumerman, A. QT prolongation in a diverse, urban population of COVID-19 patients treated with hydroxychloroquine, chloroquine, or azithromycin. J. Interv. Card Electrophysiol. 2020, 59, 337–345. [Google Scholar] [CrossRef]
- Echarte-Morales, J.; Minguito-Carazo, C.; Del Castillo-García, S.; Borrego-Rodríguez, J.; Rodríguez-Santamarta, M.; Sánchez-Muñoz, E.; Bergel-García, R.; González-Maniega, C.; Prieto-González, S.; Menéndez-Suarez, P.; et al. Effect of hydroxychloroquine, azithromycin and lop-inavir/ritonavir on the QT corrected interval in patients with COVID-19. J. Electrocardiol. 2021, 64, 30–35. [Google Scholar] [CrossRef]
- Jiménez-Jáimez, J.; Macías-Ruiz, R.; Bermúdez-Jiménez, F.; Rubini-Costa, R.; Ramírez-Taboada, J.; Flores, P.I.G.; Gallo-Padilla, L.; García, J.D.M.; García, C.M.; Suárez, S.M.; et al. Absence of relevant QT interval prolongation in not critically ill COVID-19 patients. Sci. Rep. 2020, 10, 21417. [Google Scholar] [CrossRef] [PubMed]
- Zdemir, İ.H.; Özlek, B.; Özen, M.B.; Gündüz, R.; Çetin, N.; Bilge, A.R. Hydroxychloroquine/azithromycin treatment, QT interval and ventricular arrhythmias in hospitalised patients with COVID-19. Int. J. Clin. Pract. 2021, 75, e13896. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, A.B.; Zampieri, F.G.; Rosa, R.G.; Azevedo, L.C.; Veiga, V.C.; Avezum, A.; Damiani, L.P.; Marcadenti, A.; Kawano-Dourado, L.; Lisboa, T.; et al. Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate Covid-19. N. Engl. J. Med. 2020, 383, 2041–2052. [Google Scholar] [CrossRef] [PubMed]
- Çap, M.; Bilge, Ö.; Işık, F.; Burak, C.; Karagöz, A.; İnci, Ü.; Akyüz, A.; Aslan, B.; Altıntaş, B.; Altındağ, R.; et al. The effect of favipiravir on QTc interval in patients hospitalized with coronavirus disease 2019. J. Electrocardiol. 2020, 63, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Lauriola, M.; Pani, A.; Ippoliti, G.; Mortara, A.; Milighetti, S.; Mazen, M.; Perseghin, G.; Pastori, D.; Grosso, P.; Scaglione, F. Effect of Combination Therapy of Hydroxychloroquine and Azithromycin on Mortality in Patients with COVID-19. Clin. Transl. Sci. 2020, 13, 1071–1076. [Google Scholar] [CrossRef]
- Tanriverdİ, E.; Çörtük, M.; Yildirim, B.Z.; Uğur Chousein, E.G.; Turan, D.; Çinarka, H.; Özgül, M.A.; Çetinkaya, E. Hydroxychloroquine plus azithromycin and early hospital admission are benefi-cial in COVID-19 patients: Turkish experience with real-life data. Turk. J. Med. Sci. 2021, 51, 10–15. [Google Scholar] [CrossRef]
- Arshad, S.; Kilgore, P.; Chaudhry, Z.S.; Jacobsen, G.; Wang, D.D.; Huitsing, K.; Brar, I.; Alangaden, G.J.; Ramesh, M.S.; McKinnon, J.E.; et al. Treatment with hydroxychloroquine, azithromycin, and combination in patients hospitalized with COVID-19. Int. J. Infect. Dis. 2020, 97, 396–403. [Google Scholar] [CrossRef]
- Bun, S.S.; Taghji, P.; Courjon, J.; Squara, F.; Scarlatti, D.; Theodore, G.; Baudouy, D.; Sartre, B.; Labbaoui, M.; Dellamonica, J.; et al. QT Interval Prolongation Under Hydroxychloroquine/Azithromycin Association for Inpa-tients with SARS-CoV-2 Lower Respiratory Tract Infection. Clin. Pharmacol. Ther. 2020, 108, 1090–1097. [Google Scholar] [CrossRef]
- Maraj, I.; Hummel, J.P.; Taoutel, R.; Chamoun, R.; Workman, V.; Li, C.; Tran, L.; DelVecchio, A.; Howes, C.; Akar, J.G. Incidence and determinants of QT interval prolongation in COVID-19 patients treated with hydroxychloroquine and azithromycin. J. Cardiovasc. Electrophysiol. 2020, 31, 1904–1907. [Google Scholar] [CrossRef]
- Ramireddy, A.; Chugh, H.; Reinier, K.; Ebinger, J.; Park, E.; Thompson, M.; Cingolani, E.; Cheng, S.; Marban, E.; Albert, C.M.; et al. Experience with Hydroxychloroquine and Azithromycin in the Coronavirus Dis-ease 2019 Pandemic: Implications for QT Interval Monitoring. J. Am. Heart Assoc. 2020, 9, e017144. [Google Scholar] [CrossRef]
- Pereira, M.R.; Mohan, S.; Cohen, D.J.; Husain, S.A.; Dube, G.K.; Ratner, L.E.; Arcasoy, S.; Aversa, M.M.; Benvenuto, L.J.; Dadhania, D.M.; et al. COVID-19 in solid organ transplant recipients: Initial report from the US epicenter. Am. J. Transplant. 2020, 20, 1800–1808. [Google Scholar] [CrossRef] [PubMed]
- Lofgren, S.M.; Nicol, M.R.; Bangdiwala, A.S.; Pastick, K.A.; Okafor, E.C.; Skipper, C.P.; Pullen, M.F.; Engen, N.W.; Abassi, M.; Williams, D.A.; et al. Safety of Hydroxychloroquine Among Outpatient Clinical Trial Participants for COVID-19. Open Forum Infect. Dis. 2020, 7, ofaa500. [Google Scholar] [CrossRef] [PubMed]
- Kshirsagar, N.; Faruqui, A.R.; Xavier, D.; Kamat, S.; Chandy, S.; Medhi, B.; Tripathi, R.; Shetty, Y.; Raj, J.; Kaushal, S.; et al. Safety of hydroxychloroquine in healthcare workers for COVID-19 prophylaxis. Indian J. Med. Res. 2021, 153, 219–226. [Google Scholar] [CrossRef]
- Mitjà, O.; Corbacho-Monné, M.; Ubals, M.; Alemany, A.; Suñer, C.; Tebé, C.; Tobias, A.; Peñafiel, J.; Ballana, E.; Pérez, C.A.; et al. A Cluster-Randomized Trial of Hydroxychloroquine for Prevention of Covid-19. N. Engl. J. Med. 2021, 384, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Barnabas, R.V.; Brown, E.R.; Bershteyn, A.; Stankiewicz Karita, H.C.; Johnston, C.; Thorpe, L.E.; Kottkamp, A.; Neuzil, K.M.; Laufer, M.K.; Deming, M.; et al. Hydroxychloroquine as Postexposure Prophylaxis to Prevent Severe Acute Respiratory Syndrome Coronavirus 2 Infection: A Randomized Trial. Ann. Intern. Med. 2021, 174, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Abella, B.S.; Jolkovsky, E.L.; Biney, B.T.; Uspal, J.E.; Hyman, M.C.; Frank, I.; Hensley, S.E.; Gill, S.; Vogl, D.T.; Maillard, I.; et al. Efficacy and Safety of Hydroxychloroquine vs Placebo for Pre-exposure SARS-CoV-2 Prophylaxis Among Health Care Workers: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Boulware, D.R.; Pullen, M.F.; Bangdiwala, A.S.; Pastick, K.A.; Lofgren, S.M.; Okafor, E.C.; Skipper, C.P.; Nascene, A.A.; Nicol, M.R.; Abassi, M.; et al. A Randomized Trial of Hydroxychloroquine as Postexposure Prophylaxis for Covid-19. N. Engl. J. Med. 2020, 383, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Nagaraja, B.S.; Ramesh, K.N.; Dhar, D.; Mondal, M.S.; Dey, T.; Saha, S.; Khan, M.A.; Rutul, S.D.; Pratik, K.; Manjula, J.; et al. HyPE study: Hydroxychloroquine prophylaxis-related adverse events’ analysis among healthcare workers during COVID-19 pandemic: A rising public health concern. J. Public Health 2020, 42, 493–503. [Google Scholar] [CrossRef]
- Gao, X.; Ma, C.; Ma, Y.; Wang, X.; Wei, J.; Feng, T.; Zhao, G.; Xu, L.; Zhou, W.; Zheng, X.; et al. Clinical efficacy and safety of different antiviral regimens in patients with coronavirus disease 2019. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2020, 32, 1423–1427. [Google Scholar]
- Chen, C.P.; Lin, Y.C.; Chen, T.C.; Tseng, T.Y.; Wong, H.L.; Kuo, C.Y.; Lin, W.P.; Huang, S.R.; Wang, W.Y.; Liao, J.H.; et al. A multicenter, randomized, open-label, controlled trial to evaluate the efficacy and tol-erability of hydroxychloroquine and a retrospective study in adult patients with mild to moderate coronavirus disease 2019 (COVID-19). PLoS ONE 2020, 15, e0242763. [Google Scholar]
- Self, W.H.; Semler, M.W.; Leither, L.M.; Casey, J.D.; Angus, D.C.; Brower, R.G.; Chang, S.Y.; Collins, S.P.; Eppensteiner, J.C.; Filbin, M.R.; et al. Effect of Hydroxychloroquine on Clinical Status at 14 Days in Hospitalized Patients with COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 2165–2176. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.; O’Connor, R.; Townsend, L.; Coghlan, M.; Relihan, E.; Moriarty, M.; Carr, B.; Melanophy, G.; Doyle, C.; Bannan, C.; et al. Clinical outcomes and adverse events in patients hospitalised with COVID-19, treated with off-label hydroxychloroquine and azithromycin. Br. J. Clin. Pharmacol. 2021, 87, 1150–1154. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Garcia, J.L.; Sanchez-Nievas, G.; Arevalo-Serrano, J.; Garcia-Gomez, C.; Jimenez-Vizuete, J.M.; Martinez-Alfaro, E. Bari-citinib improves respiratory function in patients treated with corticosteroids for SARS-CoV-2 pneumonia: An observational cohort study. Rheumatology (Oxford) 2021, 60, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Ip, A.; Berry, D.A.; Hansen, E.; Goy, A.H.; Pecora, A.L.; Sinclaire, B.A.; Bednarz, U.; Marafelias, M.; Berry, S.M.; Berry, N.S.; et al. Hydroxychloroquine and tocilizumab therapy in COVID-19 patients—An observational study. PLoS ONE 2020, 15, e0237693. [Google Scholar] [CrossRef] [PubMed]
- Dastan, F.; Nadji, S.A.; Saffaei, A.; Marjani, M.; Moniri, A.; Jamaati, H.; Hashemian, S.M.; Baghaei, P.; Abedini, A.; Varahram, M.; et al. Subcutaneous administration of interferon beta-1a for COVID-19: A non-controlled prospective trial. Int. Immunopharmacol. 2020, 85, 106688. [Google Scholar] [CrossRef] [PubMed]
- Garcia, P.; Revet, A.; Yrondi, A.; Rousseau, V.; Degboe, Y.; Montastruc, F. Psychiatric Disorders and Hydroxychloroquine for Coronavirus Disease 2019 (COVID-19): A VigiBase Study. Drug Saf. 2020, 43, 1315–1322. [Google Scholar] [CrossRef]
- Lewis, K.; Chaudhuri, D.; Alshamsi, F.; Carayannopoulos, L.; Dearness, K.; Chagla, Z.; Alhazzani, W.; GUIDE Group. The efficacy and safety of hydroxychloroquine for COVID-19 prophylaxis: A systematic review and meta-analysis of randomized trials. PLoS ONE 2021, 16, e0244778. [Google Scholar] [CrossRef]
- ElSawah, H.K.; Elsokary, M.A.; Elrazzaz, M.G.; Elshafie, A.H. Hydroxychloroquine for treatment of nonsevere COVID-19 patients: Systematic review and meta-analysis of controlled clinical trials. J. Med. Virol. 2020, 93, 1265–1275. [Google Scholar] [CrossRef]
- Chen, C.; Pan, K.; Wu, B.; Li, X.; Chen, Z.; Xu, Q.; Li, X.; Lv, Q. Safety of hydroxychloroquine in COVID-19 and other diseases: A systematic review and meta-analysis of 53 randomized trials. Eur. J. Clin. Pharmacol. 2021, 77, 13–24. [Google Scholar] [CrossRef]
- Yam, J.C.; Kwok, A.K.H. Ocular toxicity of hydroxychloroquine. Hong Kong Med. J. 2006, 12, 294–304. [Google Scholar]
- Kumar, J.; Jain, S.; Meena, J.; Yadav, A. Efficacy and safety of hydroxychloroquine/chloroquine against SARS-CoV-2 infection: A systematic review and meta-analysis. J. Infect. Chemother. 2021, 27, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Tleyjeh, I.M.; Kashour, Z.; AlDosary, O.; Riaz, M.; Tlayjeh, H.; Garbati, M.A.; Tleyjeh, R.; Al-Mallah, M.H.; Sohail, M.R.; Gerberi, D.; et al. Cardiac Toxicity of Chloroquine or Hydroxychloroquine in Patients with COVID-19: A Systematic Review and Meta-regression Analysis. Mayo Clin. Proc. Innov. Qual. Outcomes 2021, 5, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Virani, S.S.; Alam, M.; Denktas, A.E.; Hamzeh, I.; Khalid, U. Coronavirus disease-19 and cardiovascular disease: A risk factor or a risk marker? Rev. Med. Virol. 2021, 31, e2172. [Google Scholar] [CrossRef] [PubMed]
- Gori, T.; Lelieveld, J.; Münzel, T. Perspective: Cardiovascular disease and the Covid-19 pandemic. Basic Res. Cardiol. 2020, 115, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Ray, W.A.; Murray, K.T.; Hall, K.; Arbogast, P.G.; Stein, C.M. Azithromycin and the Risk of Cardiovascular Death. New Engl. J. Med. 2012, 366, 1881–1890. [Google Scholar] [CrossRef] [PubMed]
- Gourieux, B.; Reisz, F.; Belmas, A.S.; Danion, F.; Fourtage, M.; Nai, T.; Reiter-Schatz, A.; Ruch, Y.; Walther, J.; Nivoix, Y.; et al. Prescribing practices of lopinavir/ritonavir, hydroxychloroquine and azithromycin during the COVID-19 epidemic crisis and pharmaceutical interventions in a French teaching hospital. Eur. J. Hosp. Pharm. 2021, 28, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Kelleci Cakir, B.; Bayraktar-Ekincioglu, A.; Demirkan, K. Benefit versus toxicity risk of digoxin in patients with COVID-19. Eur. J. Hosp. Pharm. 2021, 1. [Google Scholar] [CrossRef]
- White, N.J. Cardiotoxicity of antimalarial drugs. Lancet Infect. Dis. 2007, 7, 549–558. [Google Scholar] [CrossRef]
- Zequn, Z.; Yujia, W.; Dingding, Q.; Jiangfang, L. Off-label use of chloroquine, hydroxychloroquine, azithromycin and lop-inavir/ritonavir in COVID-19 risks prolonging the QT interval by targeting the hERG channel. Eur. J. Pharmacol. 2021, 893, 173813. [Google Scholar] [CrossRef]
- Li, W.; Luo, X.; Poetsch, M.S.; Oertel, R.; Nichani, K.; Schneider, M.; Strano, A.; Hasse, M.; Steiner, R.P.; Cyganek, L.; et al. Synergistic Adverse Effects of Azithromycin and Hydroxychloroquine on Human Cardio-myocytes at a Clinically Relevant Treatment Duratio n. Pharmaceuticals 2022, 15, 220. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, J.; Zheng, K.; Thai, S.; Simpson, R.J.; Kinlaw, A.C.; Xu, Y.; Wei, J.; Cui, X.; Buse, J.B.; et al. Serious Cardiovascular Adverse Events Associated with Hydroxychloroquine/Chloroquine Alone or with Azithromycin in Patients with COVID-19: A Pharmacovigilance Analysis of the FDA Adverse Event Reporting System (FAERS). Drugs Real World Outcomes 2022, 9, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Marcianò, G.; Roberti, R.; Palleria, C.; Mirra, D.; Rania, V.; Casarella, A.; De Sarro, G.; Gallelli, L. SARS-CoV-2 Treatment: Current Therapeutic Options and the Pursuit of Tailored Therapy. Appl. Sci. 2021, 11, 7457. [Google Scholar] [CrossRef]
- Ross, S.B.; Wilson, M.G.; Papillon-Ferland, L.; Elsayed, S.; Wu, P.E.; Battu, K.; Porter, S.; Rashidi, B.; Tamblyn, R.; Pilote, L.; et al. COVID-SAFER: Deprescribing Guidance for Hydroxychloroquine Drug Interactions in Older Adults. J. Am. Geriatr. Soc. 2020, 68, 1636–1646. [Google Scholar] [CrossRef] [PubMed]
- Das, P.; Rai, A.; Chopra, A.; Philbrick, K. Psychosis Likely Induced by Hydroxychloroquine in a Patient with Chronic Q Fever: A Case Report and Clinically Relevant Review of Pharmacology. Psychosomatics 2014, 55, 409–413. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marin, S.; Martin Val, A.; Bosch Peligero, M.; Rodríguez-Bernuz, C.; Pérez-Ricart, A.; Vilaró Jaques, L.; Paredes, R.; Roca, J.; Quiñones, C. Safety of Short-Term Treatments with Oral Chloroquine and Hydroxychloroquine in Patients with and without COVID-19: A Systematic Review. Pharmaceuticals 2022, 15, 634. https://doi.org/10.3390/ph15050634
Marin S, Martin Val A, Bosch Peligero M, Rodríguez-Bernuz C, Pérez-Ricart A, Vilaró Jaques L, Paredes R, Roca J, Quiñones C. Safety of Short-Term Treatments with Oral Chloroquine and Hydroxychloroquine in Patients with and without COVID-19: A Systematic Review. Pharmaceuticals. 2022; 15(5):634. https://doi.org/10.3390/ph15050634
Chicago/Turabian StyleMarin, Sergio, Alba Martin Val, Maite Bosch Peligero, Cristina Rodríguez-Bernuz, Ariadna Pérez-Ricart, Laia Vilaró Jaques, Roger Paredes, Josep Roca, and Carles Quiñones. 2022. "Safety of Short-Term Treatments with Oral Chloroquine and Hydroxychloroquine in Patients with and without COVID-19: A Systematic Review" Pharmaceuticals 15, no. 5: 634. https://doi.org/10.3390/ph15050634