Nursing Interventions to Prevent Delirium in Critically Ill Patients in the Intensive Care Unit during the COVID19 Pandemic—Narrative Overview


Abstract
:1. Introduction
2. Non-Modifiable and Potentially Modifiable Risk Factors of Delirium in ICUs
3. Tips for Nurses Managing Delirium
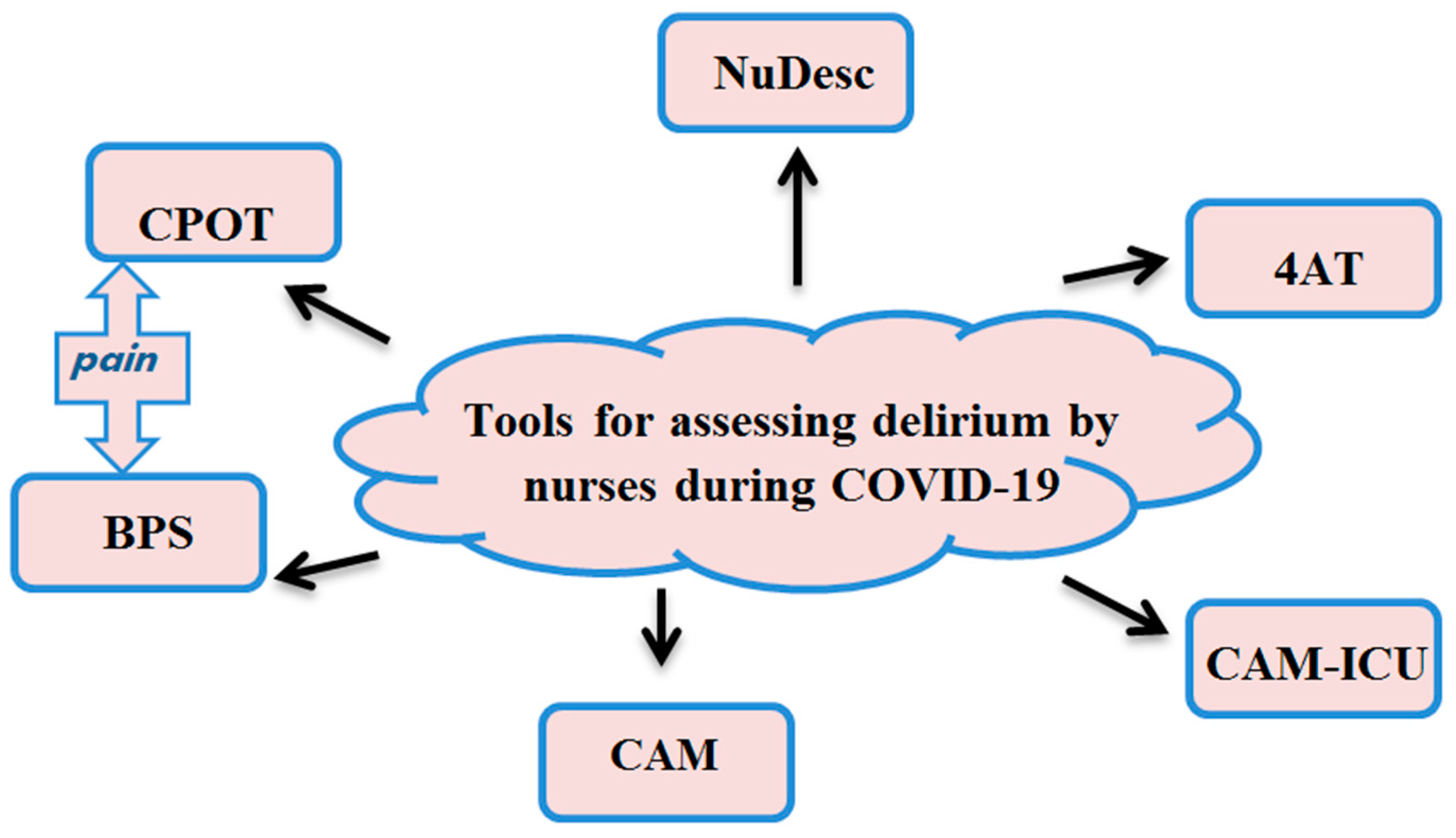
4. Tools Used in the Screening and Diagnostics of Delirium in Patients with COVID-19
5. COVID-19 vs. Delirium in an ICU—What We Know and What We Do
- –
- Assess, prevent and manage pain;
- –
- Both spontaneous awakening trials and spontaneous breathing trials;
- –
- Choice of sedation and analgesia;
- –
- Delirium assessment, prevention and management;
- –
- Early mobility and exercise;
- –
6. “Cooperative Sedation” and the Role of the Nurse
7. ”Understanding Old Age” or Who Is Most at Risk?
8. Personal Protective Measures versus Management of Patients with Delirium
9. Family, the Last but Not Least Important Element of the ABCDEF Bundle and the Personalised Approach to the Patient
10. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hosie, A.; Agar, M.; Lobb, E.; Davidson, P.M.; Phillips, J. Improving delirium recognition and assessment for people receiving inpatient palliative care: A mixed methods meta-synthesis. Int. J. Nurs. Stud. 2017, 75, 123–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spanakis, M.; Patelarou, A.E.; Patelarou, E. Nursing Personnel in the Era of Personalized Healthcare in Clinical Practice. J. Pers. Med. 2020, 10, 56. [Google Scholar] [CrossRef] [PubMed]
- El-Alti, L.; Sandman, L.; Munthe, C. Person Centered Care and Personalized Medicine: Irreconcilable Opposites or Potential Companions? Health Care Anal. 2019, 27, 45–59. [Google Scholar] [CrossRef] [Green Version]
- Han, C.J. A Concept Analysis of Personalized Health Care in Nursing. Nurs. Forum 2016, 51. [Google Scholar] [CrossRef]
- Wanga, J.; Sai, L.; Yongjun, H.; Ji, M.; Yang, F.; Zhang, Y.; Liu, H.; Li, F.; Wu, W.; Bi, J.; et al. A nurse-administered 3-Minute diagnostic interview for CAM-defined Delirium (3D-CAM Chinese version) in hospitalized elderly patients: A validation study. Int. J. Nurs. Stud. 2020, 110. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Kotfis, K.; Roberson, S.W.; Wilson, J.E.; Dąbrowski, W.; Pun, B.T.; Ely, E.W. COVID-19: ICU delirium management during SARS-CoV-2 pandemic. Crit. Care 2020, 24. [Google Scholar] [CrossRef]
- Fong, T.G.; Tulebaev, S.R.; Inouye, S.K. Delirium in elderly adults: Diagnosis, prevention and treatment. Nat. Rev. Neurol. 2020, 5, 210–220. [Google Scholar] [CrossRef]
- Pandharipande, P.P.; Shintani, A.; Peterson, J.; Ely, E.W. Sedative and analgesic medications are independent risk factors in ICU patients for transitioning into delirium. Crit. Care Med. 2004, 32. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Barr, J.; Fraser, G.L.; Puntillo, K.; Ely, E.W.; Gélinas, C.; Dasta, J.F.; Davidson, J.E.; Devlin, J.W.; John, P.; Kress, J.P.; et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit. Care Med. 2013, 41, 263–306. [Google Scholar] [CrossRef] [PubMed]
- 4AT Rapid Clinical Teat for Delirium. Available online: https://www.the4at.com/ (accessed on 18 September 2020).
- Lewandowska, K.; Małkiewicz, M.A.; Siemiński, M.; Cubała, W.J.; Winklewski, P.J.; Mędrzycka-Dąbrowska, W.A. The role of melatonin and melatonin receptor agonist in the prevention of sleep disturbances and delirium in intensive care unit—A clinical review. Sleep Med. 2020, 69, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Cudak, E.; Dyk, D.; Gutysz-Wojnicka, A.; Nowaczyk, B.; Glaza, C.; Kazimierska, D.; Miętkiewicz, S. Behawioralna ocena bólu u pacjentów na Oddziale Intensywnej Terapii—Wyniki wstępne. Pol. Nurs. 2018, 68, 152–157. [Google Scholar] [CrossRef] [Green Version]
- Helms, J.; Kremer, S.; Merdji, H.; Schenck, M.; Severac, F.; Clere-Jehl, R.; Studer, A.; Radosavljevic, M.; Kummerlen, C.; Monnier, A.; et al. Delirium and encephalopathy in severe COVID-19: A cohort analysis of ICU patients. Crit. Care 2020, 24. [Google Scholar] [CrossRef]
- Hägi-Pedersen, D.; Thybo, K.H.; Holgersen, T.H.; Jensen, J.J.; Gaudreau, J.D.; Radtke, F.M. Nu-DESC DK: The Danish version of the nursing delirium screening scale (nu-DESC). BMC Nurs. 2017, 16. [Google Scholar] [CrossRef]
- Carrillo, G.; Rubiano, Y. Research in validation of nursing diagnoses. Rev. Cubana Enfermer. 2007, 23, 24–29. [Google Scholar]
- Bellelli, G.; Morandi, A.; Davis, D.H.; Mazzola, P.; Turco, R.; Gentile, S.; Ryan, T.; Cash, H.; Guerini, F.; Torpilliesi, T.; et al. Validation of the 4AT, a new instrument for rapid delirium screening: A study in 234 hospitalised older people. Age Ageing 2014, 43, 496–502. [Google Scholar] [CrossRef] [Green Version]
- Schuurmans, M.J.; Shortridge Baggett, L.M.; Luursma, S.A. The Delirium Observation Screening Scale: A screening instrument for delirium. Res. Theory Nurs. Pract. 2003, 17, 31–50. [Google Scholar] [CrossRef]
- Van den Boogaard, M.; Pickkers, P.; Slooter, A.J.C.; Kuiper, M.A.; Spronk, P.E.; van der Voort, P.H.J.; van der Hoeven, J.G.; Donders, R.; van Achterberg, T.; Schoonhoven, L. Development and validation of PRE-DELIRIC (Prediction of Delirium in ICU patients) delirium prediction model for intensive care patients: Observational multicentre study. BMJ 2012, 344. [Google Scholar] [CrossRef] [Green Version]
- Chanques, G.; Pohlman, A.; Kress, J.P.; Molinari, N.; de Jong, A.; Jaber, S.; Jesse, B.; Hall, J.B. Psychometric comparison of three behavioural scales for the assessment of pain in critically ill patients unable to self-report. Crit. Care 2014, 18. [Google Scholar] [CrossRef] [Green Version]
- Gutysz-Wojnicka, A.; Ozga, D.; Mayzner-Zawadzka, E.; Dyk, D.; Majewski, M.; Doboszyńska, A. Psychometric Assessment of Physiologic and Behavioral Pain Indicators in Polish Versions of the Pain Assessment Scales. Pain Manag. Nurs. 2019, 20, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Kotfis, K.; Strzelbicka, M.; Zegan-Barańska, M.; Safranow, K.; Brykczyński, M.; Żukowski, M.; Ely, E.W.; POL-BPS Study Group. Validation of the behavioral pain scale to assess pain intensity in adult, intubated post cardiac surgery patients: A cohort observational study—POL-BPS. Medicine (Baltimore) 2018, 97. [Google Scholar] [CrossRef]
- Piastra, M.; Pizza, A.; Gaddi, S.; Luca, E.; Genovese, O.; Picconi, E.; Luca, D.D.; Conti, G. Dexmedetomidine is effective and safe during NIV in infants and young children with acute respiratory failure. BMC Pediatr. 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Sessler, C.N.; Gosnell, M.S.; Grap, M.J.; Brophy, G.M.; O’Neal, P.V.; Kimberly, A.; Keane, K.A.; Tesoro, E.P.; Elswick, R.K. The Richmond agitation-sedation scale: Validity and reliability in adult intensive care unit patients. Am. J. Respir. Crit. Care Med. 2002, 166, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Krupa, S.; Ozga, D. Review of the Literature on the Occurrence of Delirium after Veno-Venous and Veno-Arterial Extracorporeal Membrane Oxygenation: A Systematic Review. Dement. Geriatr. Cogn. Disord. Extra 2019, 9, 374–380. [Google Scholar] [CrossRef]
- Marra, A.; Frimpong, K.; Wesley, E. The ABCDEF Implementation Bundle. Korean J. Crit. Care Med. 2016, 31, 181–193. [Google Scholar] [CrossRef]
- Balas, M.C.; Burke, W.J.; Gannon, D.; Cohen, M.Z.; Colburn, L.; Bevil, C.; Franz, D.; Olsen, K.M.; Ely, E.W.; Vasilevskis, E.E. Implementing the awakening and breathing coordination, delirium monitoring/management, and early exercise/mobility bundle into everyday care: Opportunities, challenges, and lessons learned for implementing the ICU Pain, Agitation, and Delirium Guidelines. Crit. Care Med. 2013, 41, S116–S127. [Google Scholar] [CrossRef]
- Vasilevskis, E.E.; Ely, E.W.; Speroff, T.; Pun, B.T.; Boehm, L.; Dittus, R.S. Reducing iatrogenic risks: ICU-acquired delirium and weakness—Crossing the quality chasm. Chest 2010, 138, 1224–1233. [Google Scholar] [CrossRef] [Green Version]
- Girard, T.D.; Kress, J.P.; Fuchs, B.D.; Thomason, J.W.W.; Schweickert, W.D.; Pun, B.T.; Taichman, D.B.; Dunn, J.G.; Pohlman, A.S.; Kinniry, P.A.; et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): A randomised controlled trial. Lancet 2008, 371, 126–134. [Google Scholar] [CrossRef]
- ICU Delirium. Nashville, VUMC Center for Health Services Research. Available online: www.ICUdelirium.org (accessed on 8 September 2020).
- Goodwin, H.; Lewin, J.J.; Mirski, M.A. Cooperative sedation: Optimizing comfort while maximizing systemic and neurological function. Crit. Care 2012, 16. [Google Scholar] [CrossRef] [Green Version]
- Ely, E.W.; Truman, B.; Shintani, A.; Thomason, J.W.W.; Wheeler, A.P.; Gordon, S.; Francis, J.; Speroff, T.; Gautam, S.; Margolin, R.; et al. Monitoring sedation status over time in ICU patients: Reliability and validity of the Richmond Agitation-Sedation Scale (RASS). JAMA 2003, 16, 2983–2991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riker, R.R.; Picard, J.T.; Fraser, G.L. Prospective evaluation of the Sedation-Agitation Scale for the adult critically ill patients. Crit. Care Med. 1999, 16, 1325–1329. [Google Scholar] [CrossRef] [PubMed]
- Devlin, J.W.; Boleski, G.; Mlynarek, M.; Nerenz, D.R.; Peterson, E.; Jankowski, M.; Horst, H.M.; Zarowitz, B.J. Motor Activity Assessment Scale: Avalid and reliable sedation scale for use with mechanically ventilated patients in an adult surgical intensive care unit. Crit. Care Med. 1999, 16, 1271–1275. [Google Scholar] [CrossRef] [PubMed]
- De Jonghe, B.; Cook, D.; Griffith, L.; Appere-de-Vecchi, C.; Guyatt, G.; Théron, V.; Vagnerre, A.; Outin, H. Adaptation to the intensive care environment (ATICE): Development and validation of a new sedation assessment instrument. Crit. Care Med. 2003, 16, 2344–2354. [Google Scholar] [CrossRef] [PubMed]
- Mirski, M.A.; Le Droux, S.N.; Lewin, J.J.; Thompson, C.B.; Mirski, K.T.; Griswold, M. Validity and reliability of an intuitive conscious sedation scoring tool: The nursing instrument for the communication of sedation. Crit. Care Med. 2010, 16, 1674–1684. [Google Scholar] [CrossRef]
- Myles, P.S.; Leslie, K.; McNeil, J.; Forbes, A.; Chan, M.T.V. Bispectral index monitoring to prevent awareness during anaesthesia: The B-Aware randomized controlled trial. Lancet 2004, 16, 1757–1763. [Google Scholar] [CrossRef]
- Guttormson, J.L.; Chlan, L.; Weinert, C.; Savik, K. Factors influencing nurse sedation practices with mechanically ventilated patients: A US national survey. Int. Crit. Care Nurs. 2010, 16, 44–50. [Google Scholar] [CrossRef]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic features in severe SARS-CoV-2 infection. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- O’Hanlon, S.; Inouye, S.K. Delirium: A missing piece in the COVID-19 pandemic puzzle. Age Ageing 2020, 49, 497–498. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When COVID-19 Is Suspected (v1.2). Available online: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected (accessed on 19 April 2020).
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goh, G.K.; Dunker, A.K.; Foster, J.A.; Uversky, V.N. Shell disorder analysis predicts greater resilience of the SARS-CoV-2 (COVID-19) outside the body and in body fluids. Microb. Pathog. 2020, 144. [Google Scholar] [CrossRef] [PubMed]
- Goh, G.K.; Dunker, A.K.; Foster, J.A.; Uversky, V.N. Shell Disorder Analysis Suggests That Pangolins Offered a Window for a Silent Spread of an Attenuated SARS-CoV-2 Precursor among Humans. J. Proteome Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Phipps, L.M.; Bartke, C.N.; Spear, D.A.; Jones, L.F.; Foerster, C.P.; Killian, M.E.; Hughes, J.R.; Hess, J.C.; Johnson, D.R.; Thomas, N.J. Assessment of parental presence during bedside pediatric intensive care unit rounds: Effect on duration, teaching, and privacy. Pediatr. Crit. Care Med. 2007, 8, 220–224. [Google Scholar] [CrossRef]
- Tan, Z.; Khoo, D.W.S.; Zeng, L.A.; Tien, J.-C.C.; Lee, A.K.Y.; Ong, Y.Y.; Teo, M.M.; Abdullah, H.R. Protecting health care workers in the front line: Innovation in COVID-19 pandemic. J. Glob. Health 2020, 10. [Google Scholar] [CrossRef]
- Massimo, R. Facilitating supportive care in cardiac intensive care units. Curr. Opin. Supportive Palliat. Care 2020, 14, 19–24. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-Modifiable | Potentially Modifiable |
|---|---|
| Dementia and cognitive disturbances | Immobilisation (catheters, probes, tubes, intravenous infusions, restraint straps) |
| History of delirium | Medication (sedatives, narcotics, anticholinergics, corticosteroids, complex pharmacotherapy, sudden discontinuation of certain drugs and benzodiazepines) |
| History of stroke and neurological disease | Acute neurological diseases (acute stroke, especially within the right parietal region, intracranial bleeding, meningitis, encephalitis) |
| Falls and gait disturbances | Comorbidities (infections, acute diseases, anaemia, dehydration, undernutrition, fracture, and trauma) |
| Advanced age | Vision and hearing impairment |
| Complex multimorbidity | Metabolic disturbances (hypoglycaemia, hyperglycaemia, hyponatremia, hypernatremia, etc.) |
| Male gender | Surgeries |
| Chronic renal or liver disease | Environmental (e.g., admission to the ICU) |
| Pain | |
| Stress, long-lasting insomnia |
| SAT Safety Screen | SBT Safety Screen |
| No active seizures No alcohol withdrawal No agitation No paralytics No myocardial ischemia Normal intracranial pressure | No agitation Oxygen saturation ≥ 88% FiO2 ≤ 50% PEEP ≤ 7.5 cm H2O No myocardial ischemia No vasopressor use Inspiratory efforts |
| SAT Failure | SBT Failure |
| Anxiety, agitation, pain Respiratory rate > 35/min Oxygen saturation < 88% Respiratory distress Acute cardiac arrhythmia | Respiratory rate > 35/min Respiratory rate < 8/min Oxygen saturation < 88% Respiratory distress Mental status change Acute cardiac arrhythmia |
| Non-pharmacological interventions. Orientations Provide visual and hearing aids. Encourage communication and orientation to the day/time/location by nurses and family. Have familiar objects from the patients’ home in the room. Attempt consistency in nursing staff. Allow television during the day with daily news. Non-verbal music. Environment Sleep hygiene: lights off at night, on during the day. Consider sleep aids (zolpidem, mirtazapine). Control excess noise (staff, equipment, visitors) at night. Ambulate or mobilize patients. Clinical parameters Maintain systolic blood pressure >90 mmHg. Maintain saturations >90%. Treat underlying metabolic derangements and infections. Discontinue any unnecessary and potentially deliriogenic medications. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ozga, D.; Krupa, S.; Witt, P.; Mędrzycka-Dąbrowska, W. Nursing Interventions to Prevent Delirium in Critically Ill Patients in the Intensive Care Unit during the COVID19 Pandemic—Narrative Overview. Healthcare 2020, 8, 578. https://doi.org/10.3390/healthcare8040578
Ozga D, Krupa S, Witt P, Mędrzycka-Dąbrowska W. Nursing Interventions to Prevent Delirium in Critically Ill Patients in the Intensive Care Unit during the COVID19 Pandemic—Narrative Overview. Healthcare. 2020; 8(4):578. https://doi.org/10.3390/healthcare8040578
Chicago/Turabian StyleOzga, Dorota, Sabina Krupa, Paweł Witt, and Wioletta Mędrzycka-Dąbrowska. 2020. "Nursing Interventions to Prevent Delirium in Critically Ill Patients in the Intensive Care Unit during the COVID19 Pandemic—Narrative Overview" Healthcare 8, no. 4: 578. https://doi.org/10.3390/healthcare8040578