

Adolescents’ Opinions on COVID-19 Vaccine Hesitancy: Hints toward Enhancing Pandemic Preparedness in the Future

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
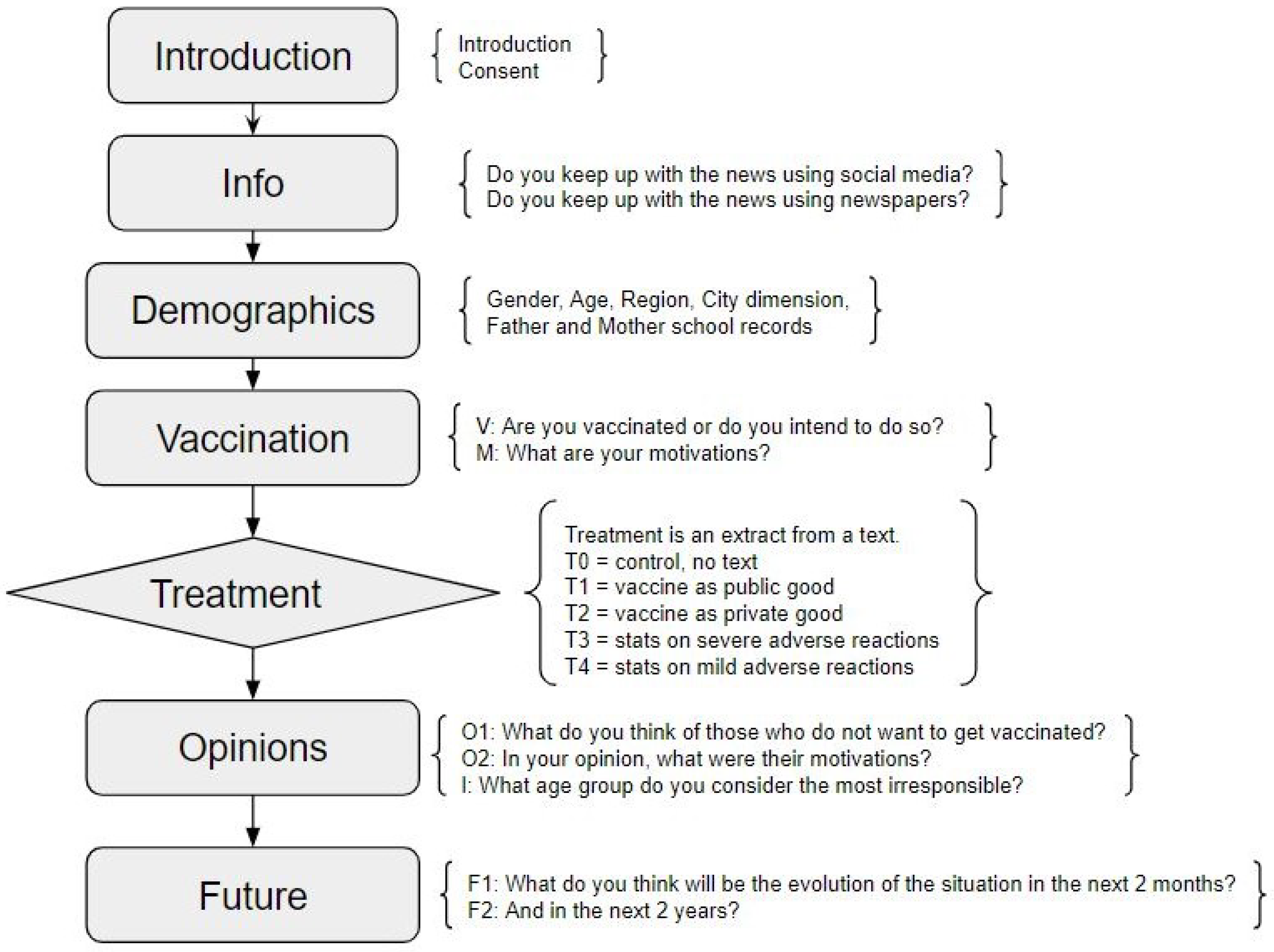
2.1. The Survey
2.2. The Treatments
- T0
- Control group: no treatment, i.e., no text is shown to the subject.
- T1
- The vaccine as a public good.
- “Did you know that:
- according to the Italian Society of Surgery, 400,000 operations were missed in 2020 due to the Coronavirus and that according to the Italian Federation of Medical Doctors in 2020 there were about 30,000 more deaths for “neglected diseases”, i.e., compared to those attributed to Covid and those expected from other pathologies.”
- T2
- The vaccine as a private good.
- “Did you know that:
- estimates of July 2021 from the ISS (Italian National Institute of Health) say that the percentage of Covid cases among the vaccinated is far lower than the percentage of cases among the unvaccinated and that the vaccine prevents very effectively hospitalization and death.
- For example, the effectiveness in preventing hospitalization is 94.6% and in preventing death is 95.8%.”
- T3
- Some statistics about severe adverse effects of the vaccine.
- “Did you know that:
- AIFA (Italian Medicines Agency) reports 0.12% of suspicious events after the administration of an anti-Covid vaccine. 13% of these reports concern serious and potentially fatal events.”
- T4
- Statistics about mild adverse effects of the vaccine.
- “Did you know that:
- Pfizer/BioNTech and AstraZeneca vaccines in their information leaflets declare the incidence of mild side effects (such as fever and nausea) in more than one in 10 people.
- Data on British citizens instead report the appearance of these symptoms in one in 4 people.”
2.3. Description of the Sample
2.4. The Variables Not Analyzed
2.5. Empirical Strategy
3. Results
3.1. Opinions Concerning Anti-Vaxxers
3.2. Feelings about the Evolution of the COVID-19 Pandemic
4. Discussion
4.1. Key General Findings
4.2. Findings about Individual Characteristics
4.3. Opinions about Anti-Vaxxers’ Motivations
4.4. Opinions about the Evolution of the COVID-19 Pandemic
4.5. Limitations of This Study and Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| FMD | Fondazione Mondo Digitale |
| PC | Principal component |
| VAF | Variance accounted for |
| PRINCALS | Categorical principal component analysis |
| CAREUS | Ethical committee of the University of Siena |
| WHO | World Health Organization |
Appendix A. More Information about the Variables Not Analyzed



Appendix B. Principal Component Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question O1: What do you think about those who do not want to get vaccinated? | |||
| Scale: From 1 (Strongly Agree) to 5 (Strongly Disagree) | |||
| Answer | a.PC1: Generic Distrust | a.PC2: Distrust of Vaccines | a.PC3: Self-Thinkers |
| They are selfish. | −0.685 | 0.402 | 0.158 |
| They are not brave. | −0.611 | 0.462 | 0.152 |
| They are very brave. | −0.601 | 0.133 | −0.277 |
| They are easily influenced by other people. | −0.635 | - | 0.377 |
| They never listen to others. | −0.669 | - | 0.207 |
| They do not trust science and vaccines. | −0.710 | −0.538 | - |
| They do not trust COVID-19 vaccine. | −0.647 | −0.595 | −0.196 |
| They do not want to limit individual freedom. | −0.426 | 0.245 | −0.757 |
| Eigenvalues | 3.158 | 1.100 | 0.924 |
| VAF | 39.477 | 13.752 | 11.547 |
| Cumulative VAF | 39.480 | 53.230 | 64.780 |
| Question O2: What do you think was the motivation for those people who do not want to get vaccinated? | |||
| Scale: From 1 (Strongly Agree) to 5 (Strongly Disagree) | |||
| Answer | b.PC1: Generic Distrust | b.PC2: Distrust of COVID-19 Vaccine | b.PC3: COVID-19 Deniers |
| They do not trust COVID-19 vaccine. | −0.710 | −0.198 | −0.410 |
| They think COVID-19 vaccine is not adequately tested. | −0.709 | −0.338 | −0.156 |
| They think COVID-19 vaccine long-term effects are not known enough. | −0.685 | −0.400 | −0.187 |
| They do not trust science and vaccines. | −0.660 | 0.249 | −0.414 |
| They do not trust politician, executives and managers of the pandemics. | −0.622 | −0.107 | - |
| They do not believe COVID-19 is a dangerous disease. | −0.474 | 0.639 | - |
| They believe COVID-19 is dangerous, but they do not trust vaccines. | −0.577 | −0.272 | 0.422 |
| They need more info about possible side effects. | −0.478 | −0.337 | 0.607 |
| They cannot accept each drug has possible side effects. | −0.614 | 0.481 | 0.209 |
| They think vaccine side effects are riskier than the chances of getting sick. | −0.678 | 0.407 | 0.207 |
| Eigenvalues | 3.922 | 1.381 | 1.025 |
| VAF | 39.218 | 13.813 | 10.250 |
| Cumulative VAF | 39.220 | 53.030 | 62.280 |
| Question F1: How do you think the pandemic situation will evolve in Italy in the next two months? | |||
| Scale: From 1 (Strongly Agree) to 5 (Strongly Disagree) | |||
| Answer | c.PC1: Generic Pessimism | c.PC2: Optimism toward COVID-19 Vaccine | c.PC3: Pessimism toward Others’ Behavior |
| COVID-19 will not be dangerous anymore, because everyone will be vaccinated. | −0.553 | −0.654 | 0.111 |
| COVID-19 will be still dangerous, because of the new variants. | −0.654 | 0.185 | 0.664 |
| COVID-19 will be still dangerous, because of many people not vaccinated. | −0.609 | 0.475 | −0.411 |
| COVID-19 will not be dangerous anymore, because the virus will become weaker. | −0.638 | −0.461 | −0.345 |
| COVID-19 will be still dangerous, because of many people not respecting social distancing. | −0.672 | 0.365 | - |
| Eigenvalues | 1.963 | 1.033 | 0.742 |
| VAF | 39.266 | 20.665 | 14.840 |
| Cumulative VAF | 39.270 | 59.930 | 74.770 |
| Question F2: How do you think the pandemic situation will evolve in Italy in the next two years? | |||
| Scale: From 1 (Strongly Agree) to 5 (Strongly Disagree) | |||
| Answer | d.PC1: Generic Pessimism | d.PC2: Optimism toward COVID-19 Vaccine | d.PC3: Uncertainty Virus vs. Vaccine Campaign |
| COVID-19 will not be dangerous anymore, because everyone will be vaccinated. | −0.329 | −0.777 | −0.439 |
| COVID-19 will be still dangerous, because of the new variants. | −0.740 | −0.317 | 0.324 |
| COVID-19 will be still dangerous, because of many people not vaccinated. | −0.726 | −0.342 | −0.391 |
| COVID-19 will not be dangerous anymore, because the virus will become weaker. | −0.459 | 0.692 | 0.445 |
| COVID-19 will be still dangerous, because of many people not respecting social distancing. | −0.821 | −0.109 | - |
| Eigenvalues | 2.067 | 1.311 | 0.648 |
| VAF | 41.341 | 26.220 | 12.963 |
| Cumulative VAF | 41.340 | 67.560 | 80.520 |
Appendix C. Variables Selection
| Regression | Model | Includes Treatments | R-Squared | Adj. R-Squared | Pred. R-Squared | AIC | SBC |
|---|---|---|---|---|---|---|---|
| 5 | No | 0.111 | 0.090 | 0.063 | 1096.44 | 1140.21 | |
| a.PC1 | 6 | Yes | 0.117 | 0.087 | 0.050 | 1101.87 | 1161.55 |
| 7 | Yes | 0.119 | 0.084 | 0.042 | 1104.94 | 1172.58 | |
| 6 | Yes | 0.069 | 0.037 | 0.005 | 1122.71 | 1182.39 | |
| a.PC2 | 7 | Yes | 0.072 | 0.038 | 0.004 | 1123.29 | 1186.95 |
| 8 | Yes | 0.075 | 0.036 | −0.005 | 1126.14 | 1197.76 | |
| 5 | Yes | 0.053 | 0.025 | −0.007 | 1125.60 | 1177.33 | |
| a.PC3 | 6 | Yes | 0.059 | 0.027 | −0.011 | 1126.98 | 1186.67 |
| 7 | Yes | 0.062 | 0.028 | −0.013 | 1127.60 | 1191.27 | |
| 3 | Yes | 0.044 | 0.024 | −0.002 | 1123.09 | 1162.88 | |
| b.PC1 | 4 | Yes | 0.050 | 0.025 | −0.008 | 1124.85 | 1172.60 |
| 5 | Yes | 0.054 | 0.024 | −0.015 | 1127.21 | 1182.92 | |
| 3 | Yes | 0.056 | 0.039 | 0.018 | 1116.21 | 1152.02 | |
| b.PC2 | 4 | Yes | 0.065 | 0.043 | 0.016 | 1116.38 | 1160.15 |
| 5 | Yes | 0.067 | 0.011 | 0.042 | 1118.39 | 1170.11 | |
| 6 | Yes | 0.059 | 0.027 | 0.005 | 1120.95 | 1156.76 | |
| b.PC3 | 7 | Yes | 0.062 | 0.028 | −0.013 | 1127.60 | 1191.27 |
| 8 | Yes | 0.064 | 0.027 | −0.015 | 1128.73 | 1196.37 | |
| 3 | Yes | 0.044 | 0.026 | 0.002 | 1121.41 | 1157.22 | |
| c.PC1 | 4 | Yes | 0.054 | 0.032 | 0.002 | 1121.03 | 1164.80 |
| 5 | Yes | 0.063 | 0.036 | 0.000 | 1121.42 | 1173.14 | |
| 5 | No | 0.064 | 0.045 | 0.013 | 1114.81 | 1154.60 | |
| c.PC2 | 6 | Yes | 0.069 | 0.040 | −0.002 | 1120.64 | 1176.34 |
| 7 | Yes | 0.071 | 0.037 | −0.012 | 1123.86 | 1187.53 | |
| 5 | Yes | 0.042 | 0.017 | −0.013 | 1127.94 | 1175.69 | |
| c.PC3 | 6 | Yes | 0.046 | 0.018 | −0.015 | 1128.52 | 1180.25 |
| 7 | Yes | 0.048 | 0.016 | −0.021 | 1131.36 | 1191.04 | |
| 4 | Yes | 0.061 | 0.039 | 0.010 | 1118.11 | 1161.87 | |
| d.PC1 | 5 | Yes | 0.066 | 0.041 | 0.009 | 1118.22 | 1165.97 |
| 6 | Yes | 0.070 | 0.041 | 0.003 | 1120.33 | 1176.03 | |
| 4 | No | 0.030 | 0.012 | −0.013 | 1126.95 | 1162.76 | |
| d.PC2 | 5 | Yes | 0.032 | 0.004 | −0.032 | 1134.07 | 1185.80 |
| 6 | Yes | 0.034 | 0.001 | −0.041 | 1137.27 | 1196.95 | |
| 3 | Yes | 0.033 | 0.015 | −0.007 | 1125.80 | 1161.61 | |
| d.PC3 | 4 | Yes | 0.037 | 0.017 | −0.008 | 1125.93 | 1165.72 |
| 5 | Yes | 0.041 | 0.016 | −0.014 | 1128.48 | 1176.23 |
References
- Mattiuzzi, C.; Lippi, G. Primary COVID-19 vaccine cycle and booster doses efficacy: Analysis of Italian nationwide vaccination campaign. Eur. J. Public Health 2022, 32, 328–330. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Vaccine Effectiveness. 2021. Available online: https://covid.cdc.gov/covid-data-tracker/#vaccine-effectiveness (accessed on 14 February 2023).
- Rates of COVID-19bcases and Deaths by Vaccination Status. 2021. Available online: https://covid.cdc.gov/covid-data-tracker/#rates-by-vaccine-status (accessed on 14 February 2023).
- Johnson, A.G. COVID-19 incidence and death rates among unvaccinated and fully vaccinated adults with and without booster doses during periods of Delta and Omicron variant emergence—25 US Jurisdictions, April 4–December 25, 2021. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Megget, K. Even covid-19 can’t kill the anti-vaccination movement. BMJ 2020, 369, m2184. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Jones, A.; Daly, M. International estimates of intended uptake and refusal of COVID-19 vaccines: A rapid systematic review and meta-analysis of large nationally representative samples. Vaccine 2021, 39, 2024–2034. [Google Scholar] [CrossRef]
- Wang, C.; Han, B.; Zhao, T.; Liu, H.; Liu, B.; Chen, L.; Xie, M.; Liu, J.; Zheng, H.; Zhang, S.; et al. Vaccination willingness, vaccine hesitancy, and estimated coverage at the first round of COVID-19 vaccination in China: A national cross-sectional study. Vaccine 2021, 39, 2833–2842. [Google Scholar] [CrossRef]
- Waszkiewicz, P.; Lewulis, P.; Górski, M.; Czarnecki, A.; Feleszko, W. Public vaccination reluctance: What makes us change our minds? Results of a longitudinal cohort survey. Vaccines 2022, 10, 1081. [Google Scholar] [CrossRef]
- Larson, H.J.; Gakidou, E.; Murray, C.J. The vaccine-hesitant moment. N. Engl. J. Med. 2022, 387, 58–65. [Google Scholar] [CrossRef]
- Zarbo, C.; Candini, V.; Ferrari, C.; d’Addazio, M.; Calamandrei, G.; Starace, F.; Caserotti, M.; Gavaruzzi, T.; Lotto, L.; Tasso, A.; et al. COVID-19 Vaccine Hesitancy in Italy: Predictors of acceptance, fence sitting and refusal of the COVID-19 vaccination. Front. Public Health 2022, 10, 873098. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Parimi, K.; Gilkeson, K.; Creamer, B.A. COVID-19 vaccine hesitancy: Considerations for reluctance and improving vaccine uptake. Hum. Vaccines Immunother. 2022, 18, 2062972. [Google Scholar] [CrossRef]
- World Health Organization. Ten Threats to Global Health in 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Razai, M.S.; Chaudhry, U.A.; Doerholt, K.; Bauld, L.; Majeed, A. Covid-19 vaccination hesitancy. BMJ 2021, 373, 160. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K.; Sun, J.; Jang, S.; Connelly, S. Misinformation of COVID-19 vaccines and vaccine hesitancy. Sci. Rep. 2022, 12, 13681. [Google Scholar] [CrossRef] [PubMed]
- Chadwick, A.; Kaiser, J.; Vaccari, C.; Freeman, D.; Lambe, S.; Loe, B.S.; Vanderslott, S.; Lewandowsky, S.; Conroy, M.; Ross, A.R.; et al. Online social endorsement and Covid-19 vaccine hesitancy in the United Kingdom. Soc. Media Soc. 2021, 7, 20563051211008817. [Google Scholar] [CrossRef]
- Stoddard, S.A.; Pierce, J. Promoting positive future expectations during adolescence: The role of assets. Am. J. Community Psychol. 2015, 56, 332–341. [Google Scholar] [CrossRef] [PubMed]
- Aschwanden, C. Five reasons why COVID herd immunity is probably impossible. Nature 2021, 591, 520–522. [Google Scholar] [CrossRef]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J.A. Vaccine hesitancy: An overview. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef]
- Cadeddu, C.; Castagna, C.; Sapienza, M.; Lanza, T.E.; Messina, R.; Chiavarini, M.; Ricciardi, W.; De Waure, C. Understanding the determinants of vaccine hesitancy and vaccine confidence among adolescents: A systematic review. Hum. Vaccines Immunother. 2021, 17, 4470–4486. [Google Scholar] [CrossRef]
- Bianchi, F.P.; Tafuri, S.; Migliore, G.; Vimercati, L.; Martinelli, A.; Lobifaro, A.; Diella, G.; Stefanizzi, P.; Control Room Working Group. BNT162b2 mRNA COVID-19 vaccine effectiveness in the prevention of SARS-CoV-2 infection and symptomatic disease in five-month follow-up: A retrospective cohort study. Vaccines 2021, 9, 1143. [Google Scholar] [CrossRef]
- Zhang, P.; Li, Y.; Wang, H.; Luo, L.; Wang, P.; Wang, H.; Li, Q.; Meng, Z.; Yang, H.; Liu, Y.; et al. COVID-19 Vaccine Hesitancy Among Older Adolescents and Young Adults: A National Cross-Sectional Study in China. Front. Public Health 2022, 10, 877668. [Google Scholar] [CrossRef]
- Sisto, A.; Quintiliani, L.; Vicinanza, F.; Fabris, S.; Campanozzi, L.L.; Curcio, G.; Michilli, M.; Molina, A.; Ghilardi, G.; Manazza, A.; et al. Personal attitudes and denialist views about the COVID-19 pandemic in Italy: A national survey. Med. Morale 2022, 71, 143–156. [Google Scholar] [CrossRef]
- Bianchi, F.P.; Stefanizzi, P.; Cuscianna, E.; Riformato, G.; Di Lorenzo, A.; Giordano, P.; Germinario, C.A.; Tafuri, S. COVID-19 vaccination hesitancy among Italian parents: A systematic review and meta-analysis. Hum. Vaccines Immunother. 2023, 19, 2171185. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.; Leung, D.; Chua, G.; Duque, J.; Peare, S.; So, H.; Chan, S.; Kwan, M.; Ip, P.; Lau, Y. Adolescents’ attitudes to the COVID-19 vaccination. Vaccine 2022, 40, 967–969. [Google Scholar] [CrossRef] [PubMed]
- Middleman, A.B.; Klein, J.; Quinn, J. Vaccine hesitancy in the time of COVID-19: Attitudes and intentions of teens and parents regarding the COVID-19 vaccine. Vaccines 2021, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Herman, R.; McNutt, L.A.; Mehta, M.; Salmon, D.A.; Bednarczyk, R.A.; Shaw, J. Vaccination perspectives among adolescents and their desired role in the decision-making process. Hum. Vaccines Immunother. 2019, 15, 1752–1759. [Google Scholar] [CrossRef]
- Slater, J.A.; Katharine, A. Child, Adolescent, and Adult Development. In Psychiatry, 3rd ed.; Cutler, J., Ed.; Oxford Academic: New York, NY, USA, 2014; pp. 418–447. [Google Scholar]
- Fazel, M.; Puntis, S.; White, S.R.; Townsend, A.; Mansfield, K.L.; Viner, R.; Herring, J.; Pollard, A.J.; Freeman, D. Willingness of children and adolescents to have a COVID-19 vaccination: Results of a large whole schools survey in England. EClinicalMedicine 2021, 40, 101144. [Google Scholar] [CrossRef]
- Hunter, D.J.; Abdool Karim, S.S.; Baden, L.R.; Farrar, J.J.; Hamel, M.B.; Longo, D.L.; Morrissey, S.; Rubin, E.J. Addressing vaccine inequity—Covid-19 vaccines as a global public good. N. Engl. J. Med. 2022, 386, 1176–1179. [Google Scholar] [CrossRef]
- Card, K.G. Collectivism, individualism and COVID-19 prevention: A cross sectional study of personality, culture and behavior among Canadians. Health Psychol. Behav. Med. 2022, 10, 415–438. [Google Scholar] [CrossRef]
- Ibuka, Y.; Li, M.; Vietri, J.; Chapman, G.B.; Galvani, A.P. Free-riding behavior in vaccination decisions: An experimental study. PLoS ONE 2014, 9, e87164. [Google Scholar] [CrossRef]
- Peacock, S.J. Vaccine nationalism will persist: Global public goods need effective engagement of global citizens. Glob. Health 2022, 18, 1–11. [Google Scholar] [CrossRef]
- Radic, A.; Koo, B.; Kim, J.J.; Ariza-Montes, A.; Vega-Muñoz, A.; Han, H. The Effects of Media Encouragements on Coronavirus Vaccination Decision and Public Interest in Traveling Abroad. Information 2022, 13, 157. [Google Scholar] [CrossRef]
- Medina, L.M.; Rodriguez, J.R.; Sarmiento, P.J.D. Shaping public opinion through the lens of agenda setting in rolling out COVID-19 vaccination program. J. Public Health 2021, 43, e389–e390. [Google Scholar] [CrossRef] [PubMed]
- Holt, L.J.; Anselmi, D.; Gasataya, S.A. Predictors of Vaccine Hesitancy in College-Attending Emerging Adults: Implications for Public Health Outreach. Am. J. Health Educ. 2022, 53, 186–195. [Google Scholar] [CrossRef]
- Sylvester, S.M. COVID-19 and motivated reasoning: The influence of knowledge on COVID-related policy and health behavior. Soc. Sci. Q. 2021, 102, 2341–2359. [Google Scholar] [CrossRef]
- Vu, T.V. Long-Term Cultural Barriers to Sustaining Collective Effort in Vaccination Against COVID-19. 2021. Available online: https://ssrn.com/abstract=3943011 (accessed on 18 March 2023).
- Betsch, C.; Böhm, R.; Korn, L. Inviting free-riders or appealing to prosocial behavior? game-theoretical reflections on communicating herd immunity in vaccine advocacy. Health Psychol. 2013, 32, 978. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Böhm, R.; Korn, L.; Holtmann, C. On the benefits of explaining herd immunity in vaccine advocacy. Nat. Hum. Behav. 2017, 1, 1–6. [Google Scholar] [CrossRef]
- Benin, A.L.; Wisler-Scher, D.J.; Colson, E.; Shapiro, E.D.; Holmboe, E.S. Qualitative analysis of mothers’ decision-making about vaccines for infants: The importance of trust. Pediatrics 2006, 117, 1532–1541. [Google Scholar] [CrossRef]
- Joshi, A.; Kale, S.; Chandel, S.; Pal, D.K. Likert scale: Explored and explained. Br. J. Appl. Sci. Technol. 2015, 7, 396. [Google Scholar] [CrossRef]
- Gifi, A. Nonlinear Multivariate Analysis; Wiley-Blackwell: Hoboken, NJ, USA, 1990. [Google Scholar]
- Saukani, N.; Ismail, N.A. Identifying the components of social capital by categorical principal component analysis (CATPCA). Soc. Indic. Res. 2019, 141, 631–655. [Google Scholar] [CrossRef]
- Linting, M.; van der Kooij, A. Nonlinear principal components analysis with CATPCA: A tutorial. J. Personal. Assess. 2012, 94, 12–25. [Google Scholar] [CrossRef]
- Neter, J.; Kutner, M.H.; Nachtsheim, C.J.; Wasserman, W. Applied Linear Statistical Models, 4th ed.; WCB McGraw-Hill: New York, NY, USA, 1996. [Google Scholar]
- Report Settimanale, 2021. 29 Ottobre 2021. Available online: http://www.quotidianosanita.it/allegati/allegato6443%633.pdf (accessed on 14 February 2023).
- Cupertino, V.; Bozzola, E.; De Luca, G.; Del Giudice, E.; De Martino, G.; Cannataro, P.; Tozzi, A.E.; Corsello, G. The awareness and acceptance of anti-COVID 19 vaccination in adolescence. Ital. J. Pediatr. 2022, 48, 1–6. [Google Scholar] [CrossRef]
- Rehati, P.; Amaerjiang, N.; Yang, L.; Xiao, H.; Li, M.; Zunong, J.; Wang, L.; Vermund, S.H.; Hu, Y. COVID-19 vaccine hesitancy among adolescents: Cross-sectional school survey in four Chinese cities prior to vaccine availability. Vaccines 2022, 10, 452. [Google Scholar] [CrossRef] [PubMed]
- Zintel, S.; Flock, C.; Arbogast, A.L.; Forster, A.; von Wagner, C.; Sieverding, M. Gender differences in the intention to get vaccinated against COVID-19: A systematic review and meta-analysis. J. Public Health 2022, 1–25, ahead of print. [Google Scholar] [CrossRef]
- Kretchmar, J. Gender socialization. In Sociology Reference Guide. Gender Roles & Equality; Salem Press: Hackensack, NJ, USA, 2011; pp. 41–52. [Google Scholar]
- Bandura, A. Perceived self-efficacy in the exercise of personal agency. J. Appl. Sport Psychol. 1990, 2, 128–163. [Google Scholar] [CrossRef]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.A.; Failla, G.; Puleo, V.; Melnyk, A.; Lontano, A.; Ricciardi, W. Social media and attitudes towards a COVID-19 vaccination: A systematic review of the literature. EClinicalMedicine 2022, 48, 101454. [Google Scholar] [CrossRef] [PubMed]
- Campanozzi, L.L.; Tambone, V.; Ciccozzi, M. A Lesson from the Green Pass Experience in Italy: A Narrative Review. Vaccines 2022, 10, 1483. [Google Scholar] [CrossRef] [PubMed]
- Petersen, M.B.; Bor, A.; Jørgensen, F.; Lindholt, M.F. Transparent communication about negative features of COVID-19 vaccines decreases acceptance but increases trust. Proc. Natl. Acad. Sci. USA 2021, 118, e2024597118. [Google Scholar] [CrossRef] [PubMed]
- Jennings, W.; Stoker, G.; Bunting, H.; Valgarðsson, V.O.; Gaskell, J.; Devine, D.; McKay, L.; Mills, M.C. Lack of trust, conspiracy beliefs, and social media use predict COVID-19 vaccine hesitancy. Vaccines 2021, 9, 593. [Google Scholar] [CrossRef]
- Larson, H.J.; Clarke, R.M.; Jarrett, C.; Eckersberger, E.; Levine, Z.; Schulz, W.S.; Paterson, P. Measuring trust in vaccination: A systematic review. Hum. Vaccines Immunother. 2018, 14, 1599–1609. [Google Scholar] [CrossRef]
- Sisto, A.; Vicinanza, F.; Campanozzi, L.L.; Ricci, G.; Tartaglini, D.; Tambone, V. Towards a transversal definition of psychological resilience: A literature review. Medicina 2019, 55, 745. [Google Scholar] [CrossRef]

| Full Sample | T0 | T1 | T2 | T3 | T4 | |
|---|---|---|---|---|---|---|
| (%) | (%) | (%) | (%) | (%) | (%) | |
| Independent variables | ||||||
| Gender: Females | 65.82 | 66.67 | 58.54 | 73.33 | 67.11 | 64.20 |
| Gender: Males | 27.34 | 22.22 | 36.59 | 24.00 | 26.32 | 27.16 |
| Gender: Other | 6.84 | 11.11 | 4.88 | 2.67 | 6.58 | 8.64 |
| Age: 12–15 | 23.80 | 24.69 | 26.83 | 20.00 | 23.68 | 23.46 |
| Age: 16–17 | 48.86 | 45.68 | 50.00 | 50.67 | 47.37 | 50.62 |
| Age: 18–19 | 27.34 | 29.63 | 23.17 | 29.33 | 28.95 | 25.93 |
| Mother’s ed.: Uni | 25.57 | 17.28 | 34.15 | 26.67 | 28.95 | 20.99 |
| Mother’s ed.: HS | 39.75 | 43.21 | 35.37 | 45.33 | 38.16 | 37.04 |
| Mother’s ed.: No HS | 34.68 | 39.51 | 30.49 | 28.00 | 32.89 | 41.98 |
| No lyceum HS | 26.08 | 25.93 | 24.39 | 24.00 | 30.26 | 25.93 |
| Lyceum (ref: other HS) | 73.92 | 74.07 | 75.61 | 76.00 | 69.74 | 74.07 |
| Big city (>20,000 inhabitants) | 65.57 | 59.26 | 65.85 | 68.00 | 65.79 | 69.14 |
| Small city (<20,000 inhabitants) | 34.43 | 40.74 | 34.15 | 32.00 | 34.21 | 30.86 |
| North/center | 85.32 | 87.65 | 84.15 | 88.00 | 80.26 | 86.42 |
| South/islands | 14.68 | 12.35 | 15.85 | 12.00 | 19.74 | 13.58 |
| Social: Rarely | 4.30 | 3.70 | 7.32 | 2.67 | 1.32 | 6.17 |
| Social: Sometimes | 25.06 | 22.22 | 26.83 | 25.33 | 21.05 | 29.63 |
| Social: Often | 70.63 | 74.07 | 65.85 | 72.00 | 77.63 | 64.20 |
| News: Rarely | 40.00 | 32.10 | 43.90 | 33.33 | 47.37 | 43.21 |
| News: Sometimes | 42.53 | 49.38 | 42.68 | 48.00 | 35.53 | 37.04 |
| News: Often | 17.47 | 18.52 | 13.41 | 18.67 | 17.11 | 19.75 |
| Vaccinated: No | 7.59 | 7.41 | 7.32 | 2.67 | 13.16 | 7.41 |
| Vaccinated: Yes | 92.41 | 92.59 | 92.68 | 97.33 | 86.84 | 92.60 |
| T0: Control group | 20.51 | - | - | - | - | - |
| T1: Public good | 20.76 | - | - | - | - | - |
| T2: Private good | 18.99 | - | - | - | - | - |
| T3: Severe adverse effects | 19.24 | - | - | - | - | - |
| T4: Mild adverse effects | 20.51 | - | - | - | - | - |
| Mean | Mean | Mean | Mean | Mean | Mean | |
| Dependent variables | ||||||
| a.PC1 | 0.000 | 0.101 | −0.253 | 0.054 | 0.031 | 0.076 |
| a.PC2 | 0.000 | 0.104 | −0.192 | −0.061 | 0.007 | 0.173 |
| a.PC3 | 0.000 | 0.223 | −0.035 | −0.089 | −0.019 | −0.087 |
| b.PC1 | 0.000 | −0.196 | 0.048 | −0.079 | 0.157 | 0.073 |
| b.PC2 | 0.000 | −0.072 | 0.192 | 0.061 | −0.007 | −0.173 |
| b.PC3 | 0.000 | −0.054 | 0.108 | 0.017 | −0.125 | 0.047 |
| c.PC1 | 0.000 | −0.096 | 0.217 | −0.038 | −0.001 | −0.088 |
| c.PC2 | 0.000 | −0.016 | 0.005 | −0.148 | 0.013 | 0.135 |
| c.PC3 | 0.000 | −0.036 | −0.160 | 0.119 | 0.067 | 0.026 |
| d.PC1 | 0.000 | −0.101 | 0.253 | −0.054 | −0.031 | −0.076 |
| d.PC2 | 0.000 | 0.111 | −0.006 | −0.026 | −0.114 | 0.027 |
| d.PC3 | 0.000 | −0.223 | 0.035 | 0.089 | 0.019 | 0.087 |
| No. observations | 395 | 81 | 82 | 75 | 76 | 81 |
| a.PC1: Generic Distrust | a.PC2: Distrust of Vaccines | a.PC3: Self-Thinkers | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Coeff. | St. Dev. | p-Value | Coeff. | St. Dev. | p-Value | Coeff. | St. Dev. | p-Value | |
| Gender: Males | 0.259 | 0.111 | 0.020 | 0.004 | 0.115 | 0.973 | −0.239 | 0.115 | 0.038 |
| Gender: Other | −0.143 | 0.195 | 0.466 | −0.062 | 0.203 | 0.759 | −0.115 | 0.202 | 0.569 |
| Age: 16–17 | −0.186 | 0.122 | 0.129 | 0.116 | 0.126 | 0.358 | 0.280 | 0.126 | 0.026 |
| Age: 18–19 | −0.012 | 0.139 | 0.929 | 0.119 | 0.144 | 0.409 | 0.178 | 0.144 | 0.217 |
| Mother’s ed.: HS | −0.272 | 0.124 | 0.029 | −0.180 | 0.129 | 0.163 | −0.091 | 0.128 | 0.480 |
| Mother’s ed.: No HS | −0.423 | 0.130 | 0.001 | −0.395 | 0.136 | 0.004 | −0.209 | 0.134 | 0.119 |
| Lyceum (ref: other HS) | - | - | - | −0.041 | 0.118 | 0.731 | - | - | - |
| Social: Sometimes | −0.133 | 0.336 | 0.600 | −0.372 | 0.263 | 0.158 | −0.055 | 0.261 | 0.036 |
| Social: Often | 0.101 | 0.243 | 0.677 | −0.255 | 0.252 | 0.312 | −0.443 | 0.251 | 0.078 |
| Vaccinated: Yes | 0.698 | 0.185 | 0.000 | 0.357 | 0.192 | 0.064 | −0.502 | 0.191 | 0.009 |
| T1: Public good | 0.132 | 0.153 | 0.388 | 0.230 | 0.158 | 0.146 | −0.019 | 0.157 | 0.905 |
| T2: Private good | 0.112 | 0.155 | 0.471 | 0.072 | 0.161 | 0.652 | 0.108 | 0.160 | 0.500 |
| T3: Severe adverse effects | 0.220 | 0.154 | 0.155 | 0.308 | 0.160 | 0.055 | −0.094 | 0.159 | 0.557 |
| T4: Mild adverse effects | 0.035 | 0.151 | 0.817 | 0.319 | 0.156 | 0.042 | 0.171 | 0.156 | 0.273 |
| Intercept | −0.493 | 0.336 | 0.142 | −0.091 | 0.353 | 0.798 | 0.876 | 0.346 | 0.012 |
| No. obs. | 395 | 395 | 395 | ||||||
| R-squared | 0.117 | 0.057 | 0.059 | ||||||
| Adj. R-squared | 0.087 | 0.022 | 0.027 | ||||||
| F-test | 3.879 *** | 1.632 * | 1.834 ** | ||||||
| b.PC1: Generic Distrust | b.PC2: Distrust of COVID-19 Vaccine | b.PC3: COVID-19 Deniers | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Coeff. | St. Dev. | p-Value | Coeff. | St. Dev. | p-Value | Coeff. | St. Dev. | p-Value | |
| Gender: Males | - | - | - | - | - | - | 0.064 | 0.114 | 0.579 |
| Gender: Other | - | - | - | - | - | - | −0.108 | 0.201 | 0.591 |
| Age: 16–17 | −0.026 | 0.126 | 0.834 | - | - | - | 0.193 | 0.125 | 0.123 |
| Age: 18–19 | 0.148 | 0.143 | 0.302 | - | - | - | 0.056 | 0.143 | 0.696 |
| Mother’s ed.: HS | −0.102 | 0.128 | 0.428 | - | - | - | −0.054 | 0.128 | 0.671 |
| Mother’s ed.: No HS | −0.337 | 0.132 | 0.011 | - | - | - | −0.292 | 0.135 | 0.031 |
| Lyceum (ref: other HS) | - | - | - | - | - | - | 0.153 | 0.117 | 0.190 |
| Social: Sometimes | −0.430 | 0.261 | 0.099 | −0.432 | 0.259 | 0.059 | −0.175 | 0.261 | 0.503 |
| Social: Often | −0.229 | 0.250 | 0.361 | −0.264 | 0.247 | 0.285 | 0.147 | 0.250 | 0.556 |
| News: Sometimes | - | - | - | −0.115 | 0.110 | 0.296 | - | - | - |
| News: Often | - | - | - | −0.299 | 0.142 | 0.036 | - | - | - |
| Vaccinated: Yes | - | - | - | −0.661 | 0.189 | 0.001 | 0.672 | 0.191 | 0.000 |
| T1: Public good | 0.217 | 0.157 | 0.166 | 0.055 | 0.154 | 0.720 | 0.104 | 0.156 | 0.507 |
| T2: Private good | 0.090 | 0.159 | 0.572 | −0.093 | 0.157 | 0.555 | −0.014 | 0.159 | 0.931 |
| T3: Severe adverse effects | 0.329 | 0.159 | 0.039 | 0.163 | 0.158 | 0.303 | −0.055 | 0.158 | 0.730 |
| T4: Mild adverse effects | 0.287 | 0.156 | 0.067 | 0.177 | 0.155 | 0.254 | 0.090 | 0.155 | 0.561 |
| Intercept | 0.215 | 0.286 | 0.454 | 0.946 | 0.329 | 0.004 | −0.610 | 0.350 | 0.082 |
| No. obs. | 395 | 395 | 395 | ||||||
| R-squared | 0.050 | 0.065 | 0.073 | ||||||
| Adj. R-squared | 0.025 | 0.043 | 0.039 | ||||||
| F-test | 2.006 ** | 2.978 *** | 2.138 *** | ||||||
| c.PC1: Generic Pessimism | c.PC2: Optimism toward Vaccines | c.PC3: Pessimism toward Others’ Behavior | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Coeff. | St. Dev. | p-Value | Coeff. | St. Dev. | p-Value | Coeff. | St. Dev. | p-Value | |
| Gender: Males | - | - | - | 0.096 | 0.114 | 0.402 | 0.153 | 0.115 | 0.182 |
| Gender: Other | - | - | - | 0.398 | 0.201 | 0.048 | 0.050 | 0.204 | 0.808 |
| Mother’s ed.: HS | - | - | - | −0.248 | 0.127 | 0.051 | - | - | - |
| Mother’s ed.: No HS | - | - | - | −0.129 | 0.131 | 0.327 | - | - | - |
| Lyceum (ref: other HS) | −0.280 | 0.115 | 0.015 | - | - | - | 0.162 | 0.115 | 0.161 |
| Small City (<20,000 inhabitants) | - | - | - | 0.177 | 0.106 | 0.095 | −0.126 | 0.107 | 0.241 |
| Social: Sometimes | −0.530 | 0.261 | 0.043 | −0.724 | 0.259 | 0.005 | −0.503 | 0.264 | 0.057 |
| Social: Often | −0.406 | 0.249 | 0.103 | −0.581 | 0.248 | 0.020 | −0.447 | 0.252 | 0.077 |
| News: Sometimes | 0.052 | 0.110 | 0.636 | - | - | - | - | - | - |
| News: Often | 0.341 | 0.144 | 0.035 | - | - | - | - | - | - |
| Vaccinated: Yes | - | - | - | −0.581 | 0.248 | 0.020 | 0.412 | 0.192 | 0.032 |
| T1: Public good | 0.329 | 0.155 | 0.035 | −0.001 | 0.156 | 0.993 | −0.168 | 0.157 | 0.287 |
| T2: Private good | 0.071 | 0.158 | 0.651 | −0.060 | 0.159 | 0.707 | 0.129 | 0.161 | 0.421 |
| T3: Severe adverse effects | 0.103 | 0.158 | 0.516 | 0.017 | 0.158 | 0.915 | 0.131 | 0.159 | 0.411 |
| T4: Mild adverse effects | 0.009 | 0.156 | 0.951 | 0.157 | 0.155 | 0.313 | 0.036 | 0.157 | 0.817 |
| Intercept | 0.441 | 0.278 | 0.113 | 1.060 | 0.349 | 0.003 | −0.083 | 0.340 | 0.806 |
| No. obs. | 395 | 395 | 395 | ||||||
| R-squared | 0.054 | 0.069 | 0.046 | ||||||
| Adj. R-squared | 0.032 | 0.040 | 0.018 | ||||||
| F-test | 2.442 ** | 2.366 *** | 1.664 * | ||||||
| d.PC1: Generic Pessimism | d.PC2: Optimism toward COVID-19 Vaccine | d.PC3: Uncertainty (Virus vs. Vaccine Campaign) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Coeff. | St. Dev. | p-Value | Coeff. | St. Dev. | p-Value | Coeff. | St. Dev. | p-Value | |
| Mother’s ed.: HS | −0.375 | 0.126 | 0.003 | 0.267 | 0.130 | 0.041 | −0.043 | 0.130 | 0.742 |
| Mother’s ed.: No HS | −0.336 | 0.132 | 0.011 | 0.297 | 0.135 | 0.028 | 0.138 | 0.135 | 0.307 |
| Lyceum (ref: other HS) | −0.294 | 0.114 | 0.011 | - | - | - | - | - | - |
| Small City (<20,000 inhabitants) | −0.152 | 0.104 | 0.146 | - | - | - | - | - | - |
| South/islands (ref: north/center) | - | - | - | - | - | - | 0.199 | 0.146 | 0.176 |
| News: Sometimes | - | - | - | 0.142 | 0.113 | 0.210 | - | - | - |
| News: Often | - | - | - | 0.095 | 0.148 | 0.521 | - | - | - |
| Vaccinated: Yes | - | - | - | 0.277 | 0.192 | 0.151 | 0.438 | 0.191 | 0.022 |
| T1: Public good | 0.289 | 0.155 | 0.063 | −0.056 | 0.159 | 0.724 | 0.259 | 0.157 | 0.022 |
| T2: Private good | 0.009 | 0.158 | 0.953 | −0.121 | 0.161 | 0.454 | 0.308 | 0.160 | 0.055 |
| T3: Severe adverse effects | 0.006 | 0.157 | 0.969 | −0.156 | 0.162 | 0.336 | 0.259 | 0.160 | 0.105 |
| T4: Mild adverse effects | −0.005 | 0.155 | 0.974 | −0.059 | 0.158 | 0.707 | 0.301 | 0.156 | 0.054 |
| Intercept | 0.473 | 0.178 | 0.008 | −0.465 | 0.249 | 0.062 | −0.083 | 0.340 | 0.806 |
| No. obs. | 395 | 395 | 395 | ||||||
| R-squared | 0.060 | 0.027 | 0.037 | ||||||
| Adj. R-squared | 0.040 | 0.004 | 0.017 | ||||||
| F-test | 3.074 *** | 1.181 | 1.872 * | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muscillo, A.; Lombardi, G.; Sestini, E.; Garbin, F.; Tambone, V.; Campanozzi, L.L.; Pin, P. Adolescents’ Opinions on COVID-19 Vaccine Hesitancy: Hints toward Enhancing Pandemic Preparedness in the Future. Vaccines 2023, 11, 967. https://doi.org/10.3390/vaccines11050967
Muscillo A, Lombardi G, Sestini E, Garbin F, Tambone V, Campanozzi LL, Pin P. Adolescents’ Opinions on COVID-19 Vaccine Hesitancy: Hints toward Enhancing Pandemic Preparedness in the Future. Vaccines. 2023; 11(5):967. https://doi.org/10.3390/vaccines11050967
Chicago/Turabian StyleMuscillo, Alessio, Gabriele Lombardi, Elena Sestini, Francesca Garbin, Vittoradolfo Tambone, Laura Leondina Campanozzi, and Paolo Pin. 2023. "Adolescents’ Opinions on COVID-19 Vaccine Hesitancy: Hints toward Enhancing Pandemic Preparedness in the Future" Vaccines 11, no. 5: 967. https://doi.org/10.3390/vaccines11050967