
The Price of Hospital Reshaping: Nasal Myiasis Caused by Flesh Fly (Diptera: Sarcophagidae) in Reallocated COVID-19 Intensive Care Unit
 , , ,
, , ,  and
and 
{kind=link}
Abstract
:1. Introduction
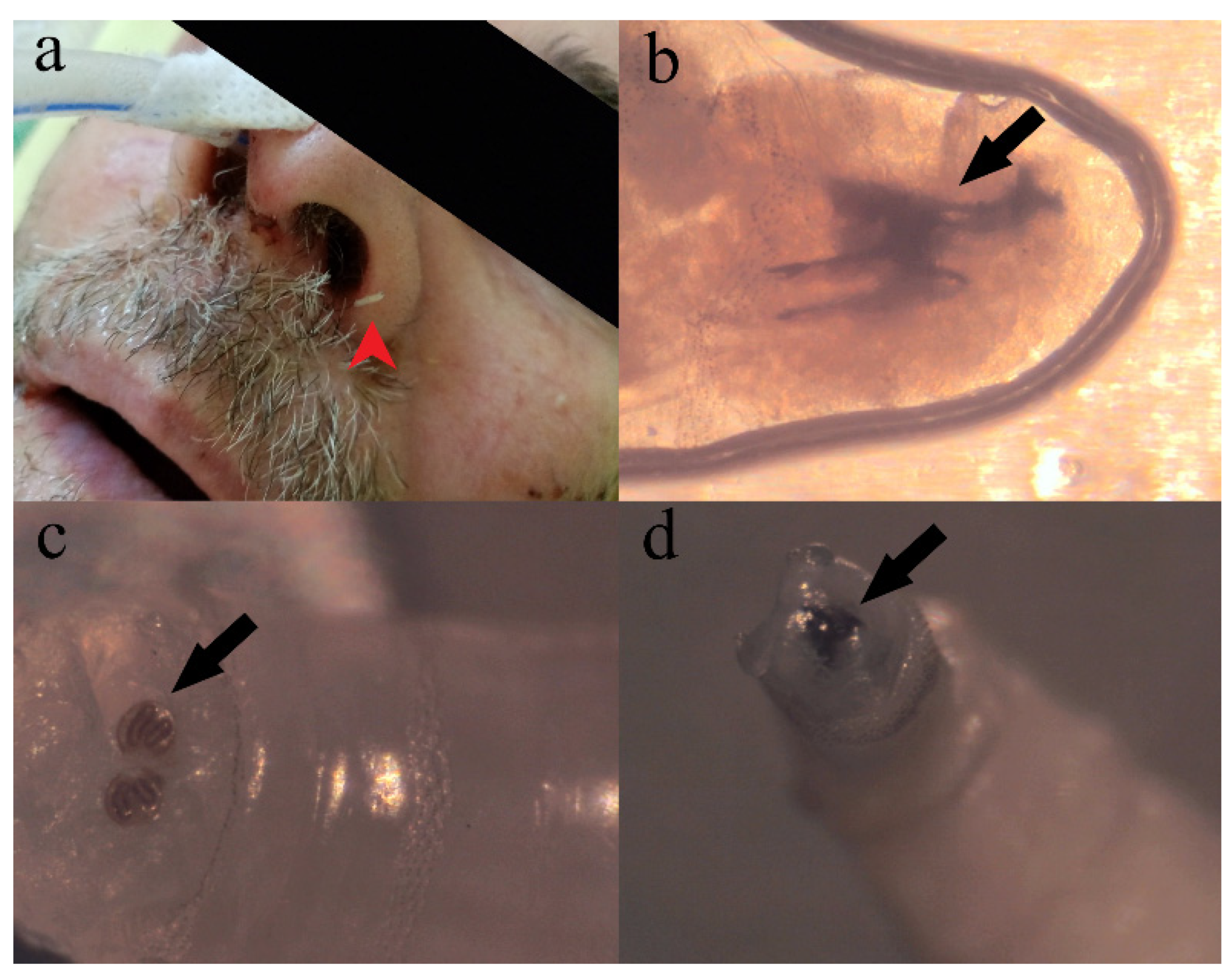
2. Case Presentation
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elhadi, M.; Msherghi, A.; Alkeelani, M.; Alsuyihili, A.; Khaled, A.; Buzreg, A.; Boughididah, T.; Abukhashem, M.; Alhashimi, A.; Khel, S.; et al. Concerns for Low-Resource Countries, with under-Prepared Intensive Care Units, Facing the COVID-19 Pandemic. Infect. Dis. Health 2020, 25, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Frutos, R.; Gavotte, L.; Serra-Cobo, J.; Chen, T.; Devaux, C. COVID-19 and Emerging Infectious Diseases: The Society Is Still Unprepared for the next Pandemic. Environ. Res. 2021, 202, 111676. [Google Scholar] [CrossRef]
- Dutto, M.; Bertero, M. Cutaneous Superficial Myiasis: Report of a Rare Nosocomial Parasitic Disease Caused by Sarcophaga spp. (Diptera, Sarcophagidae). Cent. Eur. J. Public Health 2011, 19, 232–234. [Google Scholar] [CrossRef] [PubMed]
- Fürnkranz, U.; Walochnik, J. Nosocomial Infections: Do Not Forget the Parasites! Pathogens 2021, 10, 238. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.R.J.; Farkas, R. Traumatic Myiasis of Humans and Animals. In Contributions to a Manual of Palaearctic Diptera, General and Applied Dipterology; Papp, L., Darvas, B., Eds.; Science Herald: Budapest, Hungary, 2000; Volume 1, pp. 751–768. [Google Scholar]
- Vincent, J.-L.; Rello, J.; Marshall, J.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. International Study of the Prevalence and Outcomes of Infection in Intensive Care Units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef]
- Dodge, H.R. Diptera: Pictorial Key to Principal Families of Public Health Importance. In Pictorial Keys to Arthropods, Reptiles, Birds, and Mammals of Public Health Significance; U.S. Department of Health, Education and Welfare: Atlanta, GA, USA, 1953. [Google Scholar]
- Phua, J.; Weng, L.; Ling, L.; Egi, M.; Lim, C.-M.; Divatia, J.V.; Shrestha, B.R.; Arabi, Y.M.; Ng, J.; Gomersall, C.D.; et al. Intensive Care Management of Coronavirus Disease 2019 (COVID-19): Challenges and Recommendations. Lancet Respir. Med. 2020, 8, 506–517. [Google Scholar] [CrossRef]
- Fagiuoli, S.; Lorini, F.L.; Remuzzi, G. COVID-19 Bergamo Hospital Crisis Unit. Adaptations and Lessons in the Province of Bergamo. N. Engl. J. Med. 2020, 382, e71. [Google Scholar] [CrossRef]
- Zhao, S.; Sha, T.; Xue, Y.; Chen, H. Flattening the Curve: Imperative When China Eases the Severe COVID-19 Control Policy. J. Infect. 2023, 86, e75–e77. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Pesenti, A.; Cecconi, M. Critical Care Utilization for the COVID-19 Outbreak in Lombardy, Italy: Early Experience and Forecast During an Emergency Response. JAMA 2020, 323, 1545–1546. [Google Scholar] [CrossRef]
- Goh, K.J.; Wong, J.; Tien, J.-C.C.; Ng, S.Y.; Wen, S.D.; Phua, G.C.; Leong, C.K.-L. Preparing Your Intensive Care Unit for the COVID-19 Pandemic: Practical Considerations and Strategies. Crit. Care 2020, 24, 215. [Google Scholar] [CrossRef]
- Dondorp, A.M.; Papali, A.C.; Schultz, M.J. Recommendations for the Management of COVID-19 in Low- and Middle-Income Countries. Am. J. Trop. Med. Hyg. 2021, 104, 1. [Google Scholar] [CrossRef] [PubMed]
- Haldane, V.; De Foo, C.; Abdalla, S.M.; Jung, A.-S.; Tan, M.; Wu, S.; Chua, A.; Verma, M.; Shrestha, P.; Singh, S.; et al. Health Systems Resilience in Managing the COVID-19 Pandemic: Lessons from 28 Countries. Nat. Med. 2021, 27, 964–980. [Google Scholar] [CrossRef] [PubMed]
- Condes, E.; Arribas, J.R.; COVID-19 MADRID-S.P.P.M. Group. Impact of COVID-19 on Madrid Hospital System. Enferm. Infecc. Microbiol. Clin. Engl. Ed. 2021, 39, 256–257. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Xu, S. Intensive Care for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in a Makeshift ICU in Wuhan. Crit. Care 2020, 24, 199. [Google Scholar] [CrossRef]
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What Next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Shrestha, G.S.; Lamsal, R.; Tiwari, P.; Acharya, S.P. Anesthesiology and Critical Care Response to COVID-19 in Resource-Limited Settings: Experiences from Nepal. Anesthesiol. Clin. 2021, 39, 285–292. [Google Scholar] [CrossRef]
- Tempe, D.K.; Khilnani, G.C.; Passey, J.C.; Sherwal, B.L. Challenges in Preparing and Managing the Critical Care Services for a Large Urban Area During COVID-19 Outbreak: Perspective from Delhi. J. Cardiothorac. Vasc. Anesth. 2020, 34, 2586–2594. [Google Scholar] [CrossRef]
- Isolation Precautions. Guidelines Library. Infection Control. CDC. Available online: https://www.cdc.gov/infectioncontrol/guidelines/isolation/index.html (accessed on 9 April 2023).
- Lee, J.K.; Jeong, H.W. Rapid Expansion of Temporary, Reliable Airborne-Infection Isolation Rooms with Negative Air Machines for Critical COVID-19 Patients. Am. J. Infect. Control 2020, 48, 822–824. [Google Scholar] [CrossRef]
- CDC Healthcare Workers. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control.html (accessed on 9 April 2023).
- Mohapatra, R.K.; Pintilie, L.; Kandi, V.; Sarangi, A.K.; Das, D.; Sahu, R.; Perekhoda, L. The Recent Challenges of Highly Contagious COVID-19, Causing Respiratory Infections: Symptoms, Diagnosis, Transmission, Possible Vaccines, Animal Models, and Immunotherapy. Chem. Biol. Drug Des. 2020, 96, 1187–1208. [Google Scholar] [CrossRef]
- Caumes, E.; Carrière, J.; Guermonprez, G.; Bricaire, F.; Danis, M.; Gentilini, M. Dermatoses Associated with Travel to Tropical Countries: A Prospective Study of the Diagnosis and Management of 269 Patients Presenting to a Tropical Disease Unit. Clin. Infect. Dis. 1995, 20, 542–548. [Google Scholar] [CrossRef]
- Rana, A.; Sharma, R.; Sharma, V.; Mehrotra, A.; Singh, R. Otorhinolaryngological Myiasis: The Problem and Its Presentations in the Weak and Forgotten. GMJ 2020, 54, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Singh, Z. Incidence of Myiasis among Humans—A Review. Parasitol. Res. 2015, 114, 3183–3199. [Google Scholar] [CrossRef] [PubMed]
- El Haj Chehade, A.; Metcalf, J.; Jacobs, B. Nasal Myiasis under Direct Bronchoscopic Visualization. Respirol. Case Rep. 2022, 10, e0892. [Google Scholar] [CrossRef] [PubMed]
- Giangaspero, A.; Barlaam, A.; Pane, S.; Marchili, M.R.; Muda, A.O.; Putignani, L.; Hall, M.J.R. Accidental Nasal Myiasis Caused by Megaselia rufipes (Diptera: Phoridae) in a Child. J. Med. Entomol. 2021, 58, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.; Meng, X.; Huang, X.; Wu, A.; Long, L. Nasal Myiasis in Patients with Disturbance of Consciousness: A Case Report and Literature Review. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2021, 46, 1442–1446. [Google Scholar] [CrossRef]
- Jang, M.; Ryu, S.-M.; Kwon, S.-C.; Ha, J.-O.; Kim, Y.-H.; Kim, D.-H.; Jung, S.-M.; Lee, S.-I.; Sohn, W.-M.; Cha, H.-J.; et al. A Case of Oral Myiasis Caused by Lucilia sericata (Diptera: Calliphoridae) in Korea. Korean J. Parasitol. 2013, 51, 119–123. [Google Scholar] [CrossRef]
- Kalezic, T.; Stojkovic, M.; Vukovic, I.; Spasic, R.; Andjelkovic, M.; Stanojlovic, S.; Bozic, M.; Dzamic, A. Human External Ophthalmomyiasis Caused by Lucilia sericata Meigen (Diptera: Calliphoridae)—A Green Bottle Fly. J. Infect. Dev. Ctries. 2014, 8, 925–928. [Google Scholar] [CrossRef]
- Nazni, W.A.; Jeffery, J.; Lee, H.L.; Lailatul, A.M.N.; Chew, W.K.; Heo, C.C.; Sadiyah, I.; Khairul, A.M.; Heah, S.K.; Mohd, H.H. Nosocomial Nasal Myiasis in an Intensive Care Unit. Malays. J. Pathol. 2011, 33, 53–56. [Google Scholar]
- Mircheraghi, S.F.; Mircheraghi, S.F.; Ramezani, H.; Riabi, A.; Parsapour, A. Nasal Nosocomial Myiasis Infection Caused by Chrysomya bezziana (Diptera: Calliphoridae) Following the Septicemia: A Case Report. Iran J. Parasitol. 2016, 11, 284. [Google Scholar]
- Wakid, M.H. A Laboratory-Based Study for First Documented Case of Urinary Myiasis Caused by Larvae of Megaselia scalaris (Diptera: Phoridae) in Saudi Arabia. Korean J. Parasitol. 2008, 46, 33–36. [Google Scholar] [CrossRef]
- Alizadeh, M.; Mowlavi, G.; Kargar, F.; Nateghpour, M.; Akbarzadeh, K.; Hajenorouzali-Tehrani, M. A Review of Myiasis in Iran and a New Nosocomial Case from Tehran, Iran. J. Arthropod Borne Dis. 2014, 8, 124–131. [Google Scholar] [PubMed]
- Chigusa, Y.; Kawakami, K.; Shimada, M.; Kurahashi, H.; Matsuda, H. Hospital-Acquired Oral Myiasis Due to Boettcherisca septentrionalis (Diptera: Sarcophagidae) in Shimane Prefecture, Japan. Med. Entomol. Zool. 2006, 57, 139–143. [Google Scholar] [CrossRef]
- Dutto, M.; Bertero, M. Traumatic Myiasis from Sarcophaga (Bercaea) cruentata Meigen, 1826 (Diptera, Sarcophagidae) in a Hospital Environment: Reporting of a Clinical Case Following Polytrauma. J. Prev. Med. Hyg. 2010, 51, 50–52. [Google Scholar] [PubMed]
- Giangaspero, A.; Marangi, M.; Balotta, A.; Venturelli, C.; Szpila, K.; Di Palma, A. Wound Myiasis Caused by Sarcophaga (Liopygia) argyrostoma (Robineau-Desvoidy) (Diptera: Sarcophagidae): Additional Evidences of the Morphological Identification Dilemma and Molecular Investigation. Sci. World J. 2017, 2017, 9064531. [Google Scholar] [CrossRef] [PubMed]
- Suwannayod, S.; Sanit, S.; Sukontason, K.; Sukontason, K.L. Parasarcophaga (Liopygia) ruficornis (Diptera: Sarcophagidae): A Flesh Fly Species of Medical Importance. Trop. Biomed. 2013, 30, 174–180. [Google Scholar]
- Uni, S.; Shinonaga, S.; Nishio, Y.; Fukunaga, A.; Iseki, M.; Okamoto, T.; Ueda, N.; Miki, T. Ophthalmomyiasis Caused by Sarcophaga crassipalpis (Diptera: Sarcophagidae) in a Hospital Patient. J. Med. Entomol. 1999, 36, 906–908. [Google Scholar] [CrossRef]
- Serafim, R.A.; do Espírito Santo, R.B.; de Mello, R.A.F.; Collin, S.M.; Deps, P.D. Case Report: Nasal Myiasis in an Elderly Patient with Atrophic Rhinitis and Facial Sequelae of Leprosy. Am. J. Trop. Med. Hyg. 2020, 102, 448–450. [Google Scholar] [CrossRef]
- Surayya, R.; Parwati, D.R. Management of Nasal Myiasis and Type 2 Diabetes Mellitus: A Rare Case and Review Article. Int. J. Surg. Case Rep. 2021, 85, 106244. [Google Scholar] [CrossRef]
- Szakacs, T.A.; MacPherson, P.; Sinclair, B.J.; Gill, B.D.; McCarthy, A.E. Nosocomial Myiasis in a Canadian Intensive Care Unit. CMAJ 2007, 177, 719–720. [Google Scholar] [CrossRef]
- Teah, M.K.; Chu, Y.M.; Shanmuganathan, S.D.; Yeap, T.B. Massive Airway Myiasis: An Extreme Rarity. BMJ Case Rep. 2020, 13, e237764. [Google Scholar] [CrossRef]
- Hall, R.D.; Gerhardt, R.R. Flies (Diptera). In Medical and Veterinary Entomology; Mullen, G., Durden, L., Eds.; Academic Press: San Diego, CA, USA, 2002; pp. 127–145. ISBN 978-0-12-510451-7. [Google Scholar]
- Francesconi, F.; Lupi, O. Myiasis. Clin. Microbiol. Rev. 2012, 25, 79–105. [Google Scholar] [CrossRef] [PubMed]
- Barazi, R.; Dabbous, H. Nasal Myiasis in Pediatric Age Group: Case Report and Review of the Literature. Ann. Clin. Otolaryngol. 2020, 5, 1040. [Google Scholar]
- Sherman, R.A.; Roselle, G.; Bills, C.; Danko, L.H.; Eldridge, N. Healthcare-Associated Myiasis: Prevention and Intervention. Infect. Control Hosp. Epidemiol. 2005, 26, 828–832. [Google Scholar] [CrossRef] [PubMed]
- White, Z.L.; Chu, M.W.; Hood, R.J. Nasal Myiasis: A Case Report. Ear Nose Throat J. 2015, 94, E24–E25. [Google Scholar] [CrossRef]
- Barlaam, A.; Puccini, A.; Caiaffa, M.F.; Di Bona, D.; Macchia, L.; Giangaspero, A. Dermanyssosis in the Urban Context: When the One Health Paradigm Is Put into Practice. Pathogens 2022, 11, 1396. [Google Scholar] [CrossRef]
- Bellanger, A.P.; Bories, C.; Foulet, F.; Bretagne, S.; Botterel, F. Nosocomial Dermatitis Caused by Dermanyssus gallinae. Infect. Control Hosp. Epidemiol. 2008, 29, 282–283. [Google Scholar] [CrossRef]
- Flamm, H.; Rotter, M. Angewandte Hygiene im Krankenhaus und Arztpraxis, 4th ed.; Wilhelm Maudrich: Vienna, Austria, 1999. [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dolinaj, V.; Grujić, J.; Križanović, D.; Potkonjak, A.; Pape, T.; Banović, P. The Price of Hospital Reshaping: Nasal Myiasis Caused by Flesh Fly (Diptera: Sarcophagidae) in Reallocated COVID-19 Intensive Care Unit. Healthcare 2023, 11, 1533. https://doi.org/10.3390/healthcare11111533
Dolinaj V, Grujić J, Križanović D, Potkonjak A, Pape T, Banović P. The Price of Hospital Reshaping: Nasal Myiasis Caused by Flesh Fly (Diptera: Sarcophagidae) in Reallocated COVID-19 Intensive Care Unit. Healthcare. 2023; 11(11):1533. https://doi.org/10.3390/healthcare11111533
Chicago/Turabian StyleDolinaj, Vladimir, Jasmina Grujić, Davor Križanović, Aleksandar Potkonjak, Thomas Pape, and Pavle Banović. 2023. "The Price of Hospital Reshaping: Nasal Myiasis Caused by Flesh Fly (Diptera: Sarcophagidae) in Reallocated COVID-19 Intensive Care Unit" Healthcare 11, no. 11: 1533. https://doi.org/10.3390/healthcare11111533