
Impact of Delayed Intravitreal Anti-Vascular Endothelial Growth Factor (VEGF) Therapy Due to the Coronavirus Disease Pandemic on the Prognosis of Patients with Neovascular Age-Related Macular Degeneration


Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kang, K.T.; Kim, Y.C. Dietary patterns and age-related macular degeneration in Korea: The Korea National Health and Nutrition Examination Survey 2010–2011. Sci. Rep. 2019, 9, 8200. [Google Scholar] [CrossRef] [PubMed]
- Keenan, T.D.L.; Cukras, C.A.; Chew, E.Y. Age-related macular degeneration: Epidemiology and clinical aspects. Adv. Exp. Med. Biol. 2021, 1256, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Ricci, F.; Bandello, F.; Navarra, P.; Staurenghi, G.; Stumpp, M.; Zarbin, M. Neovascular age-related macular degeneration: Therapeutic management and new-upcoming approaches. Int. J. Mol. Sci. 2020, 21, 8242. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; Lindsley, K.; Vedula, S.S.; Krzystolik, M.G.; Hawkins, B.S. Anti-vascular endothelial growth factor for neovascular age-related macular degeneration. Cochrane Database Syst. Rev. 2014. Online ahead of print. [Google Scholar] [CrossRef] [Green Version]
- Borrelli, E.; Grosso, D.; Vella, G.; Sacconi, R.; Querques, L.; Zucchiatti, I.; Prascina, F.; Bandello, F.; Querques, G. Impact of COVID-19 on outpatient visits and intravitreal treatments in a referral retina unit: Let’s be ready for a plausible “rebound effect”. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 2655–2660. [Google Scholar] [CrossRef] [PubMed]
- Parravano, M.; Borrelli, E.; Costanzo, E.; Sacconi, R.; Varano, M.; Querques, G. Protect healthcare workers and patients from COVID-19: The experience of two tertiary ophthalmology care referral centers in Italy. Ophthalmol. Ther. 2020, 9, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Sekeroglu, M.A.; Kilinc Hekimsoy, H.; Horozoglu Ceran, T.; Doguizi, S. Treatment of neovascular age related macular degeneration during COVID-19 pandemic: The short term consequences of unintended lapses. Eur. J. Ophthalmol. 2021, 32. [Google Scholar] [CrossRef]
- Yeter, D.Y.; Dursun, D.; Bozali, E.; Ozec, A.V.; Erdogan, H. Effects of the COVID-19 pandemic on neovascular age-related macular degeneration and response to delayed Anti-VEGF treatment. J. Fr. Ophtalmol. 2021, 44, 299–306. [Google Scholar] [CrossRef]
- Borrelli, E.; Battista, M.; Vella, G.; Grosso, D.; Sacconi, R.; Querques, L.; Zucchiatti, I.; Prascina, F.; Bandello, F.; Querques, G. The COVID-19 pandemic has had negative effects on baseline clinical presentation and outcomes of patients with newly diagnosed treatment-naïve exudative AMD. J. Clin. Med. 2021, 10, 1265. [Google Scholar] [CrossRef]
- Muether, P.S.; Hoerster, R.; Hermann, M.M.; Kirchhof, B.; Fauser, S. Long-term effects of ranibizumab treatment delay in neovascular age-related macular degeneration. Graefes Arch. Clin. Exp. Ophthalmol. 2013, 251, 453–458. [Google Scholar] [CrossRef]
- Rauch, R.; Weingessel, B.; Maca, S.M.; Vecsei-Marlovits, P.V. Time to first treatment: The significance of early treatment of exudative age-related macular degeneration. Retina 2012, 32, 1260–1264. [Google Scholar] [CrossRef] [PubMed]
- Sevik, M.O.; Aykut, A.; Özkan, G.; Dericioğlu, V.; Şahin, Ö. The effect of COVID-19 pandemic restrictions on neovascular AMD patients treated with treat-and-extend protocol. Int. Ophthalmol. 2021, 41, 2951–2961. [Google Scholar] [CrossRef] [PubMed]
- Viola, F.; Milella, P.; Pozzo Giuffrida, F.; Ganci, S.; Invernizzi, A. Impact of coronavirus disease pandemic on intravitreal injections treatment for macular diseases: Report from a referral hospital in Milan. Retina 2021, 41, 701–705. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.B.; Feng, H.; Zhang, H. Effects of the COVID-19 pandemic on anti-vascular endothelial growth factor treatment in China. Front. Med. 2020, 7, 576275. [Google Scholar] [CrossRef]
- Elfalah, M.; AlRyalat, S.A.; Toro, M.D.; Rejdak, R.; Zweifel, S.; Nazzal, R.; Abu-Ameerh, M.; Ababneh, O.; Gharaibeh, A.; Sharif, Z.; et al. Delayed intravitreal anti-VEGF therapy for patients during the COVID-19 lockdown: An ethical endeavor. Clin. Ophthalmol. 2021, 15, 661–669. [Google Scholar] [CrossRef]
- Naravane, A.V.; Mundae, R.; Zhou, Y.; Santilli, C.; van Kuijk, F.J.G.M.; Nazari, H.; Yamanuha, J.; Emerson, G.G.; Koozekanani, D.D.; Montezuma, S.R. Short term visual and structural outcomes of anti-vascular endothelial growth factor (anti-VEGF) treatment delay during the first COVID-19 wave: A pilot study. PLoS ONE 2021, 16, e0247161. [Google Scholar] [CrossRef]
- Allegrini, D.; Raimondi, R.; Montesano, G.; Borgia, A.; Sorrentino, T.; Tsoutsanis, P.; Romano, M.R. Short-term outcomes after COVID-19-related treatment interruption among patients with neovascular age-related macular degeneration receiving intravitreal bevacizumab. Clin. Ophthalmol. 2021, 15, 4073–4079. [Google Scholar] [CrossRef]
- Augsburger, M.; Sarra, G.M.; Imesch, P. Treat and extend versus pro re nata regimens of ranibizumab and aflibercept in neovascular age-related macular degeneration: A comparative study. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 1889–1895. [Google Scholar] [CrossRef] [Green Version]
- AlSaad, M.M.; Shatarat, A.T.; AlRyalat, S.A.S. Normative values of the retinal macular thickness in a middle eastern population. BMC Ophthalmol. 2020, 20, 137. [Google Scholar] [CrossRef]
- Dansingani, K.K.; Tan, A.C.S.; Gilani, F.; Phasukkijwatana, N.; Novais, E.; Querques, L.; Waheed, N.K.; Duker, J.S.; Querques, G.; Yannuzzi, L.A.; et al. Subretinal hyperreflective material imaged with optical coherence tomography angiography. Am. J. Ophthalmol. 2016, 169, 235–248. [Google Scholar] [CrossRef]
- Jung, J.J.; Chen, C.Y.; Mrejen, S.; Gallego-Pinazo, R.; Xu, L.; Marsiglia, M.; Boddu, S.; Freund, K.B. The incidence of neovascular subtypes in newly diagnosed neovascular age-related macular degeneration. Am. J. Ophthalmol. 2014, 158, 769–779.e2. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Stetson, P.F.; Ruiz-Garcia, H.; Heussen, F.M.; Sadda, S.R. Automated characterization of pigment epithelial detachment by optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2012, 53, 164–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balaskas, K.; Karampelas, M.; Horani, M.; Hotu, O.; Keane, P.; Aslam, T. Quantitative analysis of pigment epithelial detachment response to different anti-vascular endothelial growth factor agents in wet age-related macular degeneration. Retina 2016, 37, 1297–1304. [Google Scholar] [CrossRef] [PubMed]
- Sridhar, J.; Hsu, J.; Shahlaee, A.; Garg, S.J.; Spirn, M.J.; Fineman, M.S.; Vander, J. Topical dorzolamide-timolol with intravitreous anti-vascular endothelial growth factor for neovascular age-related macular degeneration. JAMA Ophthalmol. 2016, 134, 437–443. [Google Scholar] [CrossRef]
- Ung, C.; Lains, I.; Miller, J.W.; Kim, I.K. Current management of age-related macular degeneration. Adv. Exp. Med. Biol. 2021, 1256, 295–314. [Google Scholar] [CrossRef]
- Li, E.; Donati, S.; Lindsley, K.B.; Krzystolik, M.G.; Virgili, G. Treatment regimens for administration of anti-vascular endothelial growth factor agents for neovascular age-related macular degeneration. Cochrane Database Syst. Rev. 2020, 5, CD012208. [Google Scholar] [CrossRef]
- Kvannli, L.; Krohn, J. Switching from pro re nata to treat-and-extend regimen improves visual acuity in patients with neovascular age-related macular degeneration. Acta Ophthalmol. 2017, 95, 678–682. [Google Scholar] [CrossRef] [Green Version]
- Keane, P.A.; Sadda, S.R. Development of anti-VEGF therapies for intraocular use: A guide for clinicians. J. Ophthalmol. 2012, 2012, 483034. [Google Scholar] [CrossRef] [Green Version]
- Martin, D.F. Evolution of intravitreal therapy for retinal diseases-from CMV to CNV: The LXXIV Edward Jackson Memorial Lecture. Am. J. Ophthalmol. 2018, 191, xli–lviii. [Google Scholar] [CrossRef]
- Borrelli, E.; Grosso, D.; Vella, G.; Sacconi, R.; Battista, M.; Querques, L.; Zucchiatti, I.; Prascina, F.; Bandello, F.; Querques, G. Short-term outcomes of patients with neovascular exudative AMD: The effect of COVID-19 pandemic. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 2621–2628. [Google Scholar] [CrossRef]
- Singer, M.A.; Awh, C.C.; Sadda, S.; Freeman, W.R.; Antoszyk, A.N.; Wong, P.; Tuomi, L. HORIZON: An open-label extension trial of ranibizumab for choroidal neovascularization secondary to age-related macular degeneration. Ophthalmology 2012, 119, 1175–1183. [Google Scholar] [CrossRef] [PubMed]
- Beck, R.W.; Moke, P.S.; Turpin, A.H.; Ferris, F.L.; SanGiovanni, J.P.; Johnson, C.A.; Birch, E.E.; Chandler, D.L.; Cox, T.A.; Blair, R.C.; et al. A computerized method of visual acuity testing: Adaptation of the early treatment of diabetic retinopathy study testing protocol. Am. J. Ophthalmol. 2003, 135, 194–205. [Google Scholar] [CrossRef]
- Gillies, M.C.; Campain, A.; Barthelmes, D.; Simpson, J.M.; Arnold, J.J.; Guymer, R.H.; McAllister, I.L.; Essex, R.W.; Morlet, N.; Hunyor, A.P. Long-term outcomes of treatment of neovascular age-related macular degeneration: Data from an observational study. Ophthalmology 2015, 122, 1837–1845. [Google Scholar] [CrossRef] [PubMed]
- Gillies, M.; Arnold, J.; Bhandari, S.; Essex, R.W.; Young, S.; Squirrell, D.; Nguyen, V.; Barthelmes, D. Ten-year treatment outcomes of neovascular age-related macular degeneration from two regions. Am. J. Ophthalmol. 2020, 210, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Wada, I.; Oshima, Y.; Shiose, S.; Kano, K.; Nakao, S.; Kaizu, Y.; Yoshida, S.; Ishibashi, T.; Sonoda, K.H. Five-year treatment outcomes following intravitreal ranibizumab injections for neovascular age-related macular degeneration in Japanese patients. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 1411–1418. [Google Scholar] [CrossRef]
- Sharma, S.; Toth, C.A.; Daniel, E.; Grunwald, J.E.; Maguire, M.G.; Ying, G.S.; Huang, J.; Martin, D.F.; Jaffe, G.J.; Williams, D.F.; et al. Macular morphology and visual acuity in the second year of the comparison of age-related macular degeneration treatments trials. Ophthalmology 2016, 123, 865–875. [Google Scholar] [CrossRef] [Green Version]
- Jaffe, G.J.; Ying, G.S.; Toth, C.A.; Daniel, E.; Grunwald, J.E.; Martin, D.F.; Maguire, M.G. Macular morphology and visual acuity in year five of the comparison of age-related macular degeneration treatments trials. Ophthalmology 2019, 126, 252–260. [Google Scholar] [CrossRef]
- Guymer, R.H.; Markey, C.M.; McAllister, I.L.; Gillies, M.C.; Hunyor, A.P.; Arnold, J.J.; Chang, A.; Syed, A.; Broadhead, G.; Pham, T.; et al. Tolerating subretinal fluid in neovascular age-related macular degeneration treated with ranibizumab using a treat-and-extend regimen: FLUID Study 24-month results. Ophthalmology 2019, 126, 723–734. [Google Scholar] [CrossRef]
- Amoaku, W.M.; Chakravarthy, U.; Gale, R.; Gavin, M.; Ghanchi, F.; Gibson, J.; Harding, S.; Johnston, R.L.; Kelly, S.P.; Kelly, S.; et al. Defining response to anti-VEGF therapies in neovascular AMD. Eye 2015, 29, 721–731. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number or Interval (Range) | |
|---|---|---|
| Total number of eyes enrolled (patients) | 57 | |
| Age (years) | 71.6 ± 7.6 (57–85) | |
| Sex (male-to-female) | 42:15 | |
| Laterality (right-to-left) | 38:19 | |
| Previous anti-VEGF injection (number of times) | 14.7 ± 10.3 (3–51) | |
| Delayed injection interval (months) | 1.46 ± 1.24 (0.4–9) | |
| Interval from diagnosis to delayed injection (months) | 46.23 ± 34.02 (6–164) | |
| Interval from baseline to delayed injection (months) | 3.32 ± 1.21 (1.6–9.8) | |
| Injection interval (months, before delayed injection vs. after delayed injection) | 3.05 ± 1.45 (1–8.6) vs. 2.41 ± 1.46, (1–11.5), p = 0.002 a * | |
| Treatment regimen at baseline (PRN-to-T&E) | 21:36 | |
| Treatment regimen after delayed injection (PRN-to-T&E) | 9:48, p < 0.001 b * | |
| Type of injection drug (including duplicates) # | Bevacizumab | 23 |
| Aflibercept | 45 | |
| Ranibizumab | 29 | |
| Baseline (N = 57) | Delayed Injection (N = 57) | 2 Months Later (N = 40) | 4 Months Later (N = 55) | 6 Months Later (N = 56) | |
|---|---|---|---|---|---|
| OCT evidence of SRF, n (%) | 33 (57.9) | 44 (77.2), p = 0.027 a * | 27 (67.5), p = 0.549 a | 39 (70.9), p = 0.096 a | 43 (76.8), p = 0.021 a * |
| OCT evidence of PED, n (%) | 50 (87.7) | 51 (89.5), p = 1.000 a | 34 (85.0), p = 1.000 a | 49 (89.1), p = 1.000 a | 52 (92.9), p = 0.500 a |
| OCT evidence of SHRM, n (%) | 11 (19.3) | 14 (24.6), p = 0.250 a | 12 (30.0), p = 0.250 a | 17 (30.9), p = 0.016 a * | 18 (32.1), p = 0.016 a * |
| OCT evidence of IRF, n (%) | 9 (15.8) | 13 (22.8), p = 0.125 a | 10 (25.0), p = 0.375 a | 11 (20.0), p = 0.625 a | 13 (23.2), p = 0.219 a |
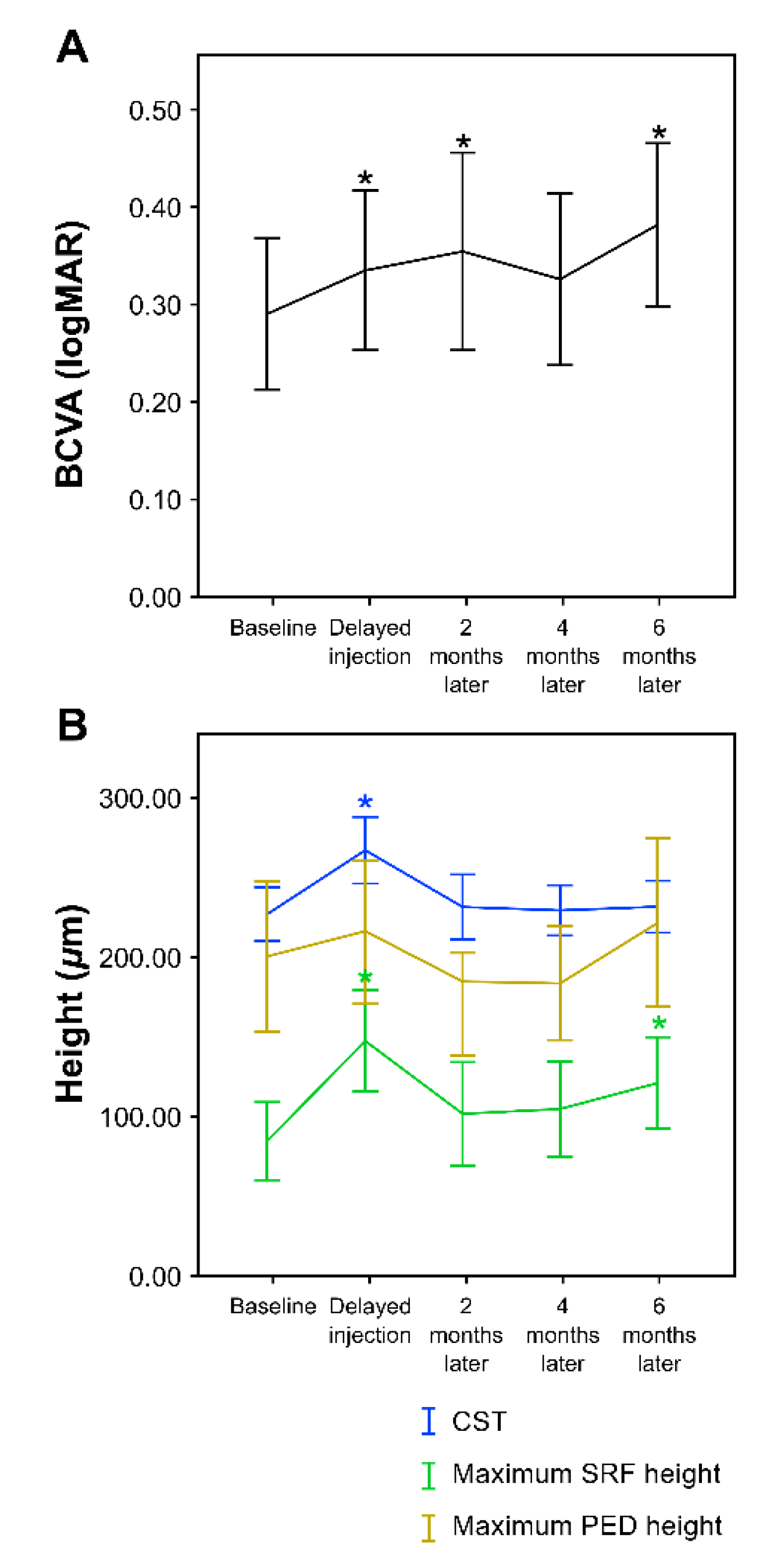
| Baseline (N = 57) | Delayed Injection (N = 57) | 2 Months Later (N = 40) | 4 Months Later (N = 55) | 6 Months Later (N = 56) | |
|---|---|---|---|---|---|
| BCVA (by logMAR) | 0.29 ± 0.29 | 0.34 ± 0.31, p = 0.044 a * | 0.36 ± 0.32, p = 0.038 a * | 0.33 ± 0.33, p = 0.141 a | 0.38 ± 0.31, p = 0.001 a * |
| CST (µm) | 227.82 ± 62.46 | 267.26 ± 77.74, p < 0.001 a * | 231.83 ± 64.52, p = 0.708 a | 229.47 ± 58.16, p = 0.926 a | 231.80 ± 61.15, p = 0.757 a |
| Maximum SRF height (µm) | 84.32 ± 89.33 | 147.51 ± 113.94, p < 0.001 a * | 101.64 ± 101.20, p = 0.677 a | 104.41 ± 107.50, p = 0.260 a | 121.38 ± 103.36, p = 0.027 a * |
| Maximum PED height (µm) | 200.42 ± 169.98 | 215.71 ± 161.11, p = 0.347 a | 184.05 ± 141.78, p = 0.286 a | 184.10 ± 126.56, p = 0.373 a | 222.00 ± 190.64, p = 0.292 a |
| Change in BCVA | Change in Maximum SRF Height | |||
|---|---|---|---|---|
| Standardized Beta Coefficient (SE) | p-Value | Standardized Beta Coefficient (SE) | p-Value | |
| Age (years) | −0.017 | 0.918 | −0.038 | 0.764 |
| Sex | −0.106 | 0.499 | 0.135 | 0.274 |
| Previous anti-VEGF injection (number of times) | −0.361 | 0.107 | −0.238 | 0.171 |
| Delayed injection time (months) | −0.431 | 0.187 | −0.146 | 0.562 |
| Injection interval before delayed injected (months) | −0.081 | 0.679 | −0.246 | 0.111 |
| Injection interval after delayed injected (months) | −0.238 | 0.201 | −0.181 | 0.212 |
| Interval from diagnosis to delayed injection (months) | 0.197 | 0.356 | 0.132 | 0.428 |
| Interval from last follow-up to delayed injection (months) | 0.428 | 0.201 | −0.089 | 0.731 |
| Baseline BCVA (logMAR) | −0.293 | 0.073 | −0.064 | 0.609 |
| Baseline CST (µm) | −0.106 | 0.544 | −0.264 | 0.059 |
| Baseline maximum SRF height (µm) | 0.318 | 0.184 | −0.716 | <0.001 * |
| Baseline maximum PED height (µm) | −0.282 | 0.138 | 0.238 | 0.110 |
| Change in BCVA | Change in Maximum SRF Height | |||
|---|---|---|---|---|
| Standardized Beta Coefficient (SE) | p-Value | Standardized Beta Coefficient (SE) | p-Value | |
| SRF+ | 0.158 | 0.274 | −0.351 | 0.015 * |
| PED+ | 0.179 | 0.230 | 0.058 | 0.678 |
| SHRM+ | 0.150 | 0.304 | −0.104 | 0.458 |
| IRF+ | −0.017 | 0.907 | −0.168 | 0.220 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-G.; Kim, Y.C.; Kang, K.T. Impact of Delayed Intravitreal Anti-Vascular Endothelial Growth Factor (VEGF) Therapy Due to the Coronavirus Disease Pandemic on the Prognosis of Patients with Neovascular Age-Related Macular Degeneration. J. Clin. Med. 2022, 11, 2321. https://doi.org/10.3390/jcm11092321
Kim J-G, Kim YC, Kang KT. Impact of Delayed Intravitreal Anti-Vascular Endothelial Growth Factor (VEGF) Therapy Due to the Coronavirus Disease Pandemic on the Prognosis of Patients with Neovascular Age-Related Macular Degeneration. Journal of Clinical Medicine. 2022; 11(9):2321. https://doi.org/10.3390/jcm11092321
Chicago/Turabian StyleKim, Jae-Gon, Yu Cheol Kim, and Kyung Tae Kang. 2022. "Impact of Delayed Intravitreal Anti-Vascular Endothelial Growth Factor (VEGF) Therapy Due to the Coronavirus Disease Pandemic on the Prognosis of Patients with Neovascular Age-Related Macular Degeneration" Journal of Clinical Medicine 11, no. 9: 2321. https://doi.org/10.3390/jcm11092321
APA StyleKim, J.-G., Kim, Y. C., & Kang, K. T. (2022). Impact of Delayed Intravitreal Anti-Vascular Endothelial Growth Factor (VEGF) Therapy Due to the Coronavirus Disease Pandemic on the Prognosis of Patients with Neovascular Age-Related Macular Degeneration. Journal of Clinical Medicine, 11(9), 2321. https://doi.org/10.3390/jcm11092321