

Acceptance of COVID-19 Vaccine Booster Doses Using the Health Belief Model: A Cross-Sectional Study in Low-Middle- and High-Income Countries of the East Mediterranean Region

 ,
,  ,
,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
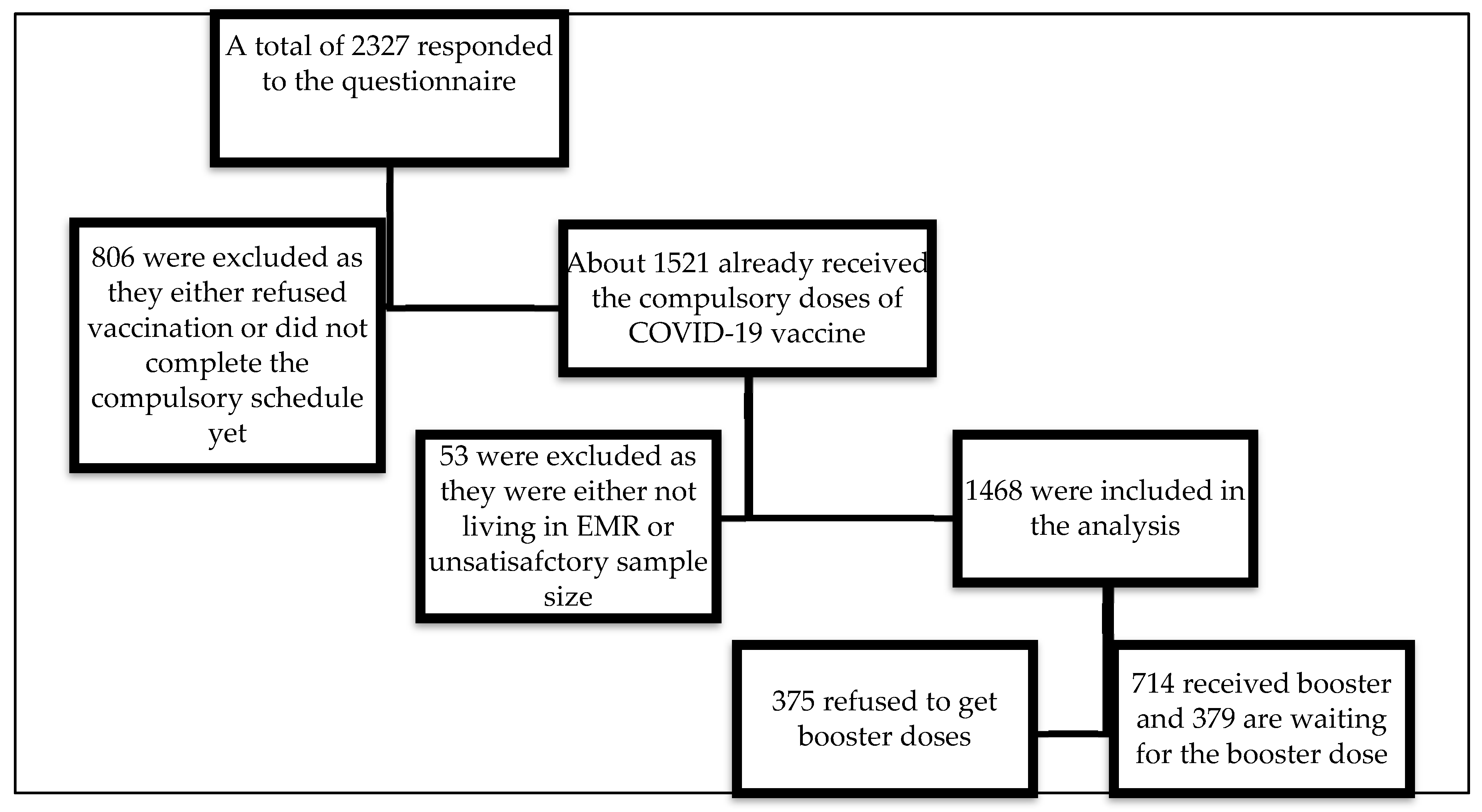
2.2. Study Population and Sampling Methods
2.3. Sample Size
2.4. Tools of Data Collection
2.5. Plan of Data Collection
2.6. Ethical Considerations and Approval
2.7. Statistical Analysis
3. Results
3.1. Respondents’ Sociodemographic Characteristics
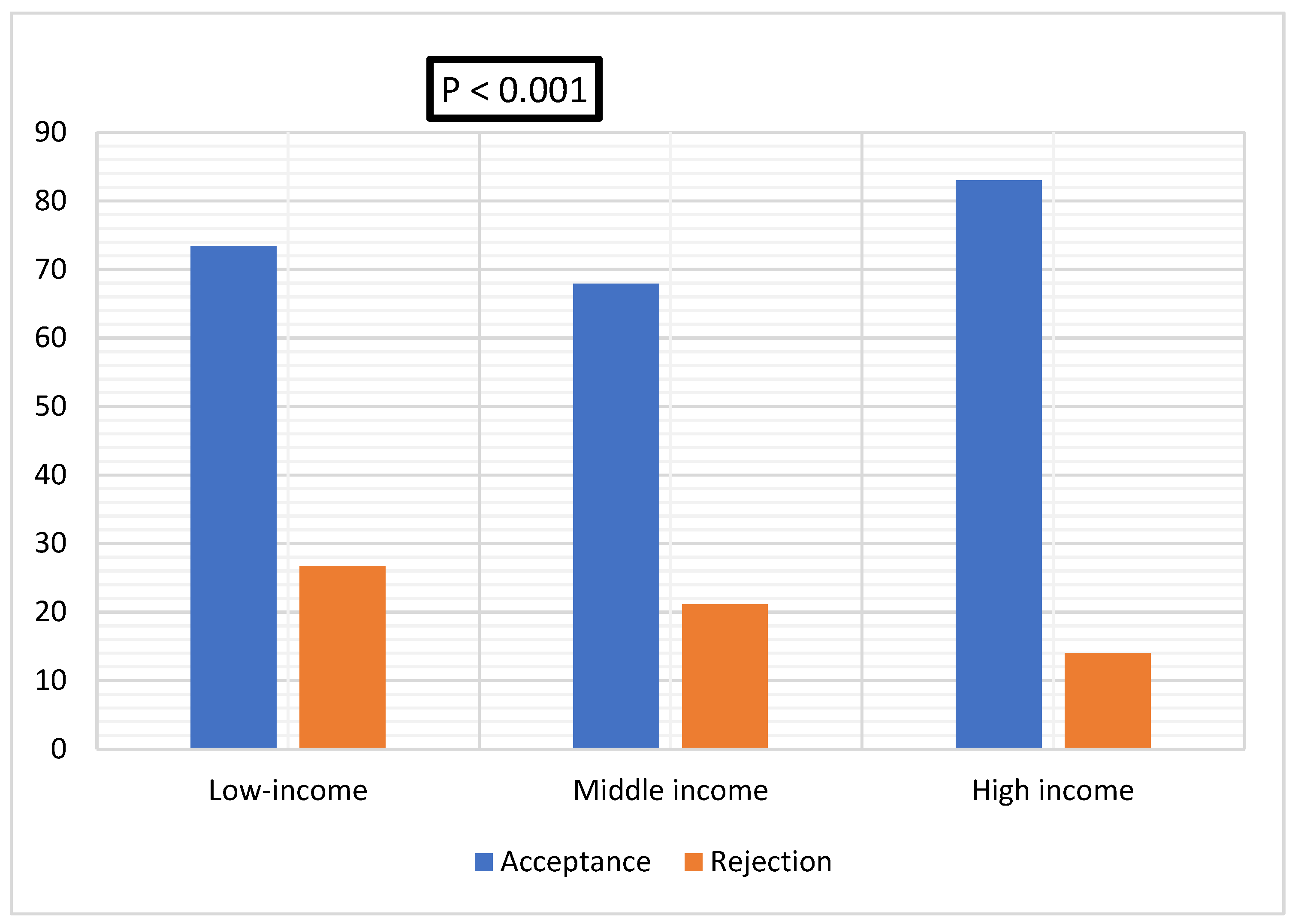
3.2. COVID-19 Booster Dose Acceptance in Low-, Middle, and High-Income Countries
3.3. Characteristics of Vaccinated and Non-Vaccinated Participants
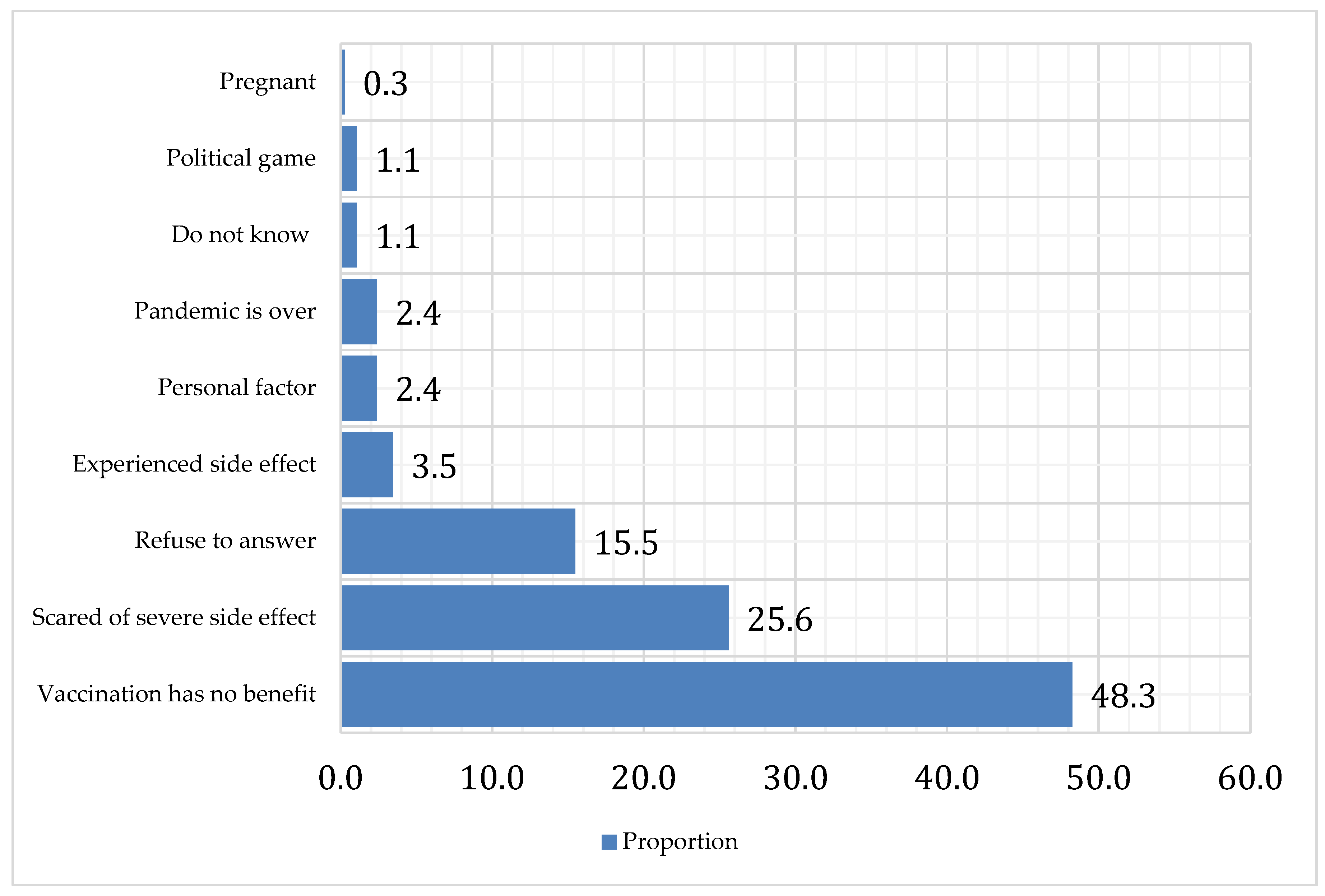
3.4. Leading Causes behind Booster Dose Rejection
3.5. Source of Information about COVID-19
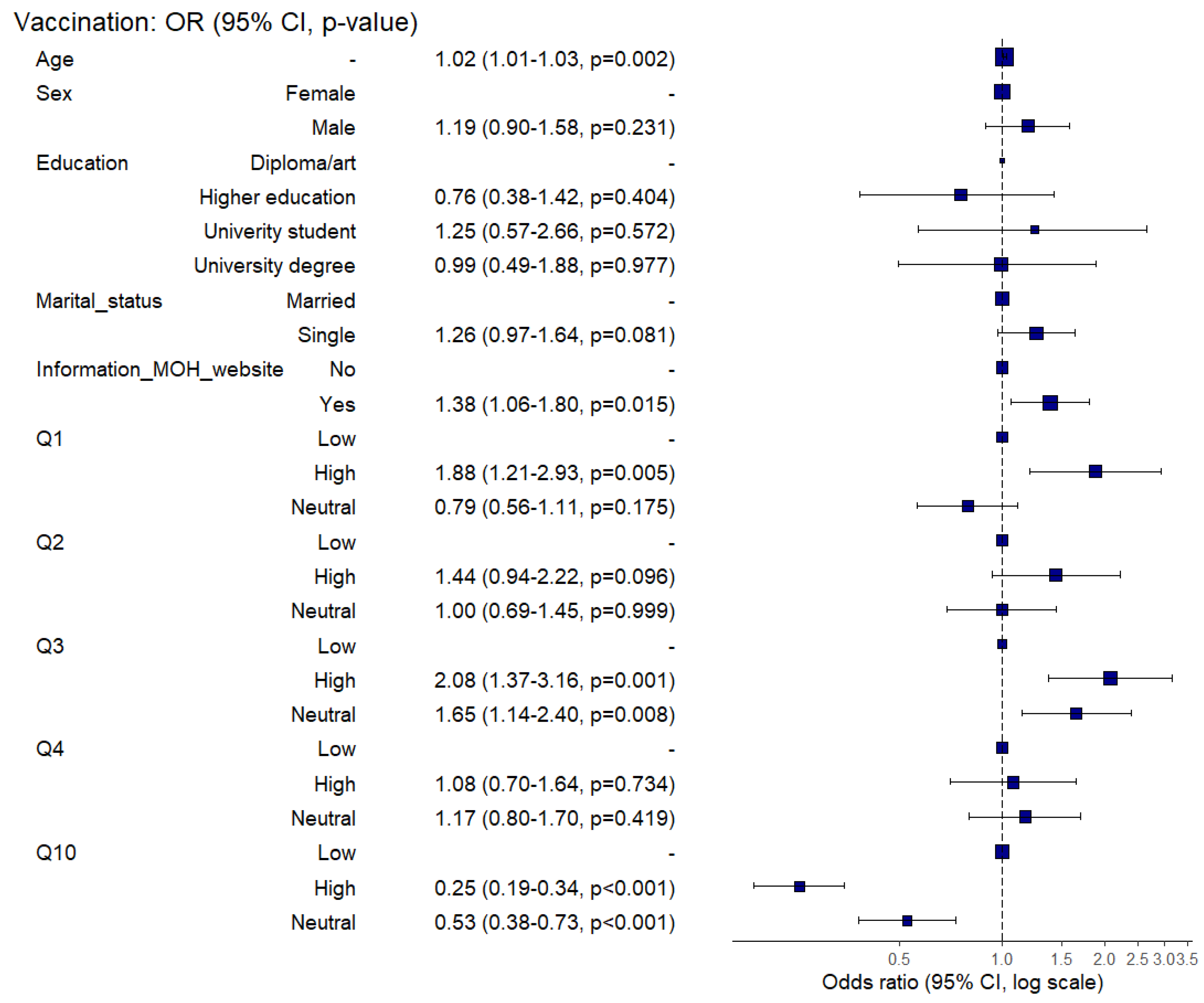
3.6. Determinants of Booster Dose Acceptance
Determinants of Booster Dose Acceptance Using Multivariable Regression Analysis
4. Discussion
4.1. Booster Dose Acceptance
4.2. Acceptance Rate in Low-Middle, and High-Income Countries
4.3. Determinants of Booster Dose Acceptance
4.4. Health Belief Model
4.5. Causes of COVID-19 Vaccine Rejection
4.6. Source of Information about Vaccination
4.7. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hassaan, M.A.; Abdelwahab, R.G.; Elbarky, T.A.; Ghazy, R.M. GIS-based analysis framework to identify the determinants of COVID-19 incidence and fatality in Africa. J. Prim. Care Community Health 2021, 12, 21501327211041208. [Google Scholar] [CrossRef] [PubMed]
- Asem, N.; Ramadan, A.; Hassany, M.; Ghazy, R.M.; Abdallah, M.; Ibrahim, M.; Gamal, E.M.; Hassan, S.; Kamal, N.; Zaid, H. Pattern and determinants of COVID-19 infection and mortality across countries: An ecological study. Heliyon 2021, 7, e07504. [Google Scholar] [CrossRef] [PubMed]
- Lenzen, M.; Li, M.; Malik, A.; Pomponi, F.; Sun, Y.-Y.; Wiedmann, T.; Faturay, F.; Fry, J.; Gallego, B.; Geschke, A. Global socio-economic losses and environmental gains from the Coronavirus pandemic. PLoS ONE 2020, 15, e0235654. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 19 September 2022).
- Moore, S.; Hill, E.M.; Tildesley, M.J.; Dyson, L.; Keeling, M.J. Vaccination and non-pharmaceutical interventions for COVID-19: A mathematical modelling study. Lancet Infect. Dis. 2021, 21, 793–802. [Google Scholar] [CrossRef]
- Lang, R.; Atabati, O.; Oxoby, R.J.; Mourali, M.; Shaffer, B.; Sheikh, H.; Fullerton, M.M.; Tang, T.; Leigh, J.P.; Manns, B.J.; et al. Characterization of non-adopters of COVID-19 non-pharmaceutical interventions through a national cross-sectional survey to assess attitudes and behaviours. Sci. Rep. 2021, 11, 21751. [Google Scholar] [CrossRef]
- Ghazy, R.M.; Taha, S.H.N.; Elhadi, Y.A.M. Letter from Egypt. Respirology 2022, 27, 242–244. [Google Scholar] [CrossRef]
- Bo, Y.; Guo, C.; Lin, C.; Zeng, Y.; Li, H.B.; Zhang, Y.; Hossain, M.S.; Chan, J.W.M.; Yeung, D.W.; Kwok, K.O.; et al. Effectiveness of non-pharmaceutical interventions on COVID-19 transmission in 190 countries from 23 January to 13 April 2020. Int. J. Infect. Dis. 2021, 102, 247–253. [Google Scholar] [CrossRef]
- Galanis, G.; Di Guilmi, C.; Bennett, D.L.; Baskozos, G. The effectiveness of Non-pharmaceutical interventions in reducing the COVID-19 contagion in the UK, an observational and modelling study. PLoS ONE 2021, 16, e0260364. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/?mapFilter=vaccinations (accessed on 14 September 2022).
- Song, F.; Bachmann, M.O. Vaccination against COVID-19 and society’s return to normality in England: A modelling study of impacts of different types of naturally acquired and vaccine-induced immunity. BMJ Open 2021, 11, e053507. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V. Covid-19 breakthrough infections in vaccinated health care workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Kuhlmann, C.; Mayer, C.K.; Claassen, M.; Maponga, T.; Burgers, W.A.; Keeton, R.; Riou, C.; Sutherland, A.D.; Suliman, T.; Shaw, M.L. Breakthrough infections with SARS-CoV-2 omicron despite mRNA vaccine booster dose. Lancet 2022, 399, 625–626. [Google Scholar] [CrossRef]
- Alishaq, M.; Nafady-Hego, H.; Jeremijenko, A.; Al Ajmi, J.A.; Elgendy, M.; Vinoy, S.; Fareh, S.B.; Veronica Plaatjies, J.; Nooh, M.; Alanzi, N. Risk factors for breakthrough SARS-CoV-2 infection in vaccinated healthcare workers. PLoS ONE 2021, 16, e0258820. [Google Scholar] [CrossRef] [PubMed]
- Vicenti, I.; Basso, M.; Gatti, F.; Scaggiante, R.; Boccuto, A.; Zago, D.; Modolo, E.; Dragoni, F.; Parisi, S.G.; Zazzi, M. Faster decay of neutralizing antibodies in never infected than previously infected healthcare workers three months after the second BNT162b2 mRNA COVID-19 vaccine dose. Int. J. Infect. Dis. 2021, 112, 40–44. [Google Scholar] [CrossRef]
- Lucas, C.; Vogels, C.B.; Yildirim, I.; Rothman, J.E.; Lu, P.; Monteiro, V.; Gehlhausen, J.R.; Campbell, M.; Silva, J.; Tabachnikova, A. Impact of circulating SARS-CoV-2 variants on mRNA vaccine-induced immunity. Nature 2021, 600, 523–529. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R. Protection of BNT162b2 vaccine booster against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Choi, A.; Koch, M.; Wu, K.; Chu, L.; Ma, L.; Hill, A.; Nunna, N.; Huang, W.; Oestreicher, J.; Colpitts, T. Safety and immunogenicity of SARS-CoV-2 variant mRNA vaccine boosters in healthy adults: An interim analysis. Nat. Med. 2021, 27, 2025–2031. [Google Scholar] [CrossRef]
- Yue, L.; Zhou, J.; Zhou, Y.; Yang, X.; Xie, T.; Yang, M.; Zhao, H.; Zhao, Y.; Yang, T.; Li, H. Antibody response elicited by a third boost dose of inactivated SARS-CoV-2 vaccine can neutralize SARS-CoV-2 variants of concern. Emerg. Microbes Infect. 2021, 10, 2125–2127. [Google Scholar] [CrossRef]
- Goren, A.; Cadegiani, F.A.; Warmbier, C.G.; Vano-Galvan, S.; Tosti, A.; Shapiro, J.; Mesinkovska, N.A.; Ramos, P.M.; Sinclair, R.; Lupi, O. Androgenetic alopecia may be associated with weaker COVID-19 T-cell immune response: An insight into a potential COVID-19 vaccine booster. Med. Hypotheses 2021, 146, 110439. [Google Scholar] [CrossRef]
- Shmueli, L. Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model. BMC Public Health 2021, 21, 804. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Sanofi, M.; Sallam, M. A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. J. Multidiscip. Healthc. 2022, 15, 21–45. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Fajar, J.K.; Sallam, M.; Soegiarto, G.; Sugiri, Y.J.; Anshory, M.; Wulandari, L.; Kosasih, S.A.P.; Ilmawan, M.; Kusnaeni, K.; Fikri, M.; et al. Global Prevalence and Potential Influencing Factors of COVID-19 Vaccination Hesitancy: A Meta-Analysis. Vaccines 2022, 10, 1356. [Google Scholar] [CrossRef] [PubMed]
- ElSayed, D.A.; Bou Raad, E.; Bekhit, S.A.; Sallam, M.; Ibrahim, N.M.; Soliman, S.; Abdullah, R.; Farag, S.; Ghazy, R.M. Validation and Cultural Adaptation of the Parent Attitudes about Childhood Vaccines (PACV) Questionnaire in Arabic Language Widely Spoken in a Region with a High Prevalence of COVID-19 Vaccine Hesitancy. Trop. Med. Infect. Dis. 2022, 7, 234. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 14 September 2022).
- World Health Organization. Health Inequities in the Eastern Mediterranean Region: Selected Country Case Studies. Available online: https://apps.who.int/iris/handle/10665/204666 (accessed on 16 September 2022).
- Abdou, M.S.; Kheirallah, K.A.; Aly, M.O.; Ramadan, A.; Elhadi, Y.A.M.; Elbarazi, I.; Deghidy, E.A.; El Saeh, H.M.; Salem, K.M.; Ghazy, R.M. The coronavirus disease 2019 (COVID-19) vaccination psychological antecedent assessment using the Arabic 5c validated tool: An online survey in 13 Arab countries. PLoS ONE 2021, 16, e0260321. [Google Scholar] [CrossRef]
- Rababa’h, A.; Abedalqader, N.; Ababneh, M. Jordanians’ willingness to receive heterologous prime-boost COVID-19 vaccination and vaccine boosters. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 7516–7525. [Google Scholar]
- Alobaidi, S.; Hashim, A. Predictors of the Third (Booster) Dose of COVID-19 Vaccine Intention among the Healthcare Workers in Saudi Arabia: An Online Cross-Sectional Survey. Vaccines 2022, 10, 987. [Google Scholar] [CrossRef]
- Patwary, M.M.; Bardhan, M.; Disha, A.S.; Hasan, M.; Haque, M.Z.; Sultana, R.; Hossain, M.R.; Browning, M.H.E.M.; Alam, M.A.; Sallam, M. Determinants of COVID-19 Vaccine Acceptance among the Adult Population of Bangladesh Using the Health Belief Model and the Theory of Planned Behavior Model. Vaccines 2021, 9, 1393. [Google Scholar] [CrossRef]
- Limbu, Y.B.; Gautam, R.K.; Pham, L. The Health Belief Model Applied to COVID-19 Vaccine Hesitancy: A Systematic Review. Vaccines 2022, 10, 973. [Google Scholar] [CrossRef]
- Bandura, A.; Freeman, W.H.; Lightsey, R. Self-Efficacy: The Exercise of Control. J. Cogn. Psychother. 1999, 13. [Google Scholar] [CrossRef]
- Al-Metwali, B.Z.; Al-Jumaili, A.A.; Al-Alag, Z.A.; Sorofman, B. Exploring the acceptance of COVID-19 vaccine among healthcare workers and general population using health belief model. J. Eval. Clin. Pract. 2021, 27, 1112–1122. [Google Scholar] [CrossRef]
- Carpenter, C.J. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Abouzid, M.; Ahmed, A.A.; El-Sherif, D.M.; Alonazi, W.B.; Eatmann, A.I.; Alshehri, M.M.; Saleh, R.N.; Ahmed, M.H.; Aziz, I.A.; Abdelslam, A.E.; et al. Attitudes toward Receiving COVID-19 Booster Dose in the Middle East and North Africa (MENA) Region: A Cross-Sectional Study of 3041 Fully Vaccinated Participants. Vaccines 2022, 10, 1270. [Google Scholar] [CrossRef]
- Lai, X.; Zhu, H.; Wang, J.; Huang, Y.; Jing, R.; Lyu, Y.; Zhang, H.; Feng, H.; Guo, J.; Fang, H. Public perceptions and acceptance of COVID-19 booster vaccination in China: A cross-sectional study. Vaccines 2021, 9, 1461. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Wang, R.; Tao, L.; Liu, M.; Liu, J. Acceptance of a third dose of COVID-19 vaccine and associated factors in China based on Health Belief Model: A national cross-sectional study. Vaccines 2022, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Al-Qerem, W.; Al Bawab, A.Q.; Hammad, A.; Ling, J.; Alasmari, F. Willingness of the Jordanian population to receive a COVID-19 booster dose: A cross-sectional study. Vaccines 2022, 10, 410. [Google Scholar] [CrossRef]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef]
- Wang, H.; Huang, Y.-M.; Su, X.-Y.; Xiao, W.-J.; Si, M.-Y.; Wang, W.-J.; Gu, X.-F.; Ma, L.; Li, L.; Zhang, S.-K. Acceptance of the COVID-19 vaccine based on the health belief model: A multicenter national survey among medical care workers in China. Hum. Vaccines Immunother. 2022, 18, 2076523. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Ai, J.; Zhang, Y.; Zhang, H.; Zhang, Q.; Fu, Z.; Lin, K.; Song, J.; Zhao, Y.; Fan, M.; Wang, H. Safety and immunogenicity of a third-dose homologous BBIBP-CorV boosting vaccination: Interim results from a prospective open-label study. Emerg. Microbes Infect. 2022, 11, 639–647. [Google Scholar] [CrossRef]
- Ashmawy, R.; Hamdy, N.A.; Elhadi, Y.A.M.; Alqutub, S.T.; Esmail, O.F.; Abdou, M.S.M.; Reyad, O.A.; El-Ganainy, S.O.; Gad, B.K.; Nour El-Deen, A.E.-S. A Meta-Analysis on the Safety and Immunogenicity of CovId-19 vaccines. J. Prim. Care Community Health 2022, 13, 21501319221089255. [Google Scholar] [CrossRef] [PubMed]
- Ghazy, R.M.; Ashmawy, R.; Hamdy, N.A.; Elhadi, Y.A.M.; Reyad, O.A.; Elmalawany, D.; Almaghraby, A.; Shaaban, R.; Taha, S.H.N. Efficacy and Effectiveness of SARS-CoV-2 Vaccines: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 350. [Google Scholar] [CrossRef] [PubMed]
- Moawad, A.M.; Taha, S.H.N.; Ghazy, R.M.; Abdelhalim, W.A. Assessment of Self-Treatment Knowledge, Beliefs and Practice during COVID-19 Pandemic among Egyptian Population: A Cross-Sectional Study. Egypt. J. Hosp. Med. 2022, 89, 4516–4525. [Google Scholar]
- Briand, S.C.; Cinelli, M.; Nguyen, T.; Lewis, R.; Prybylski, D.; Valensise, C.M.; Colizza, V.; Tozzi, A.E.; Perra, N.; Baronchelli, A.; et al. Infodemics: A new challenge for public health. Cell 2021, 184, 6010–6014. [Google Scholar] [CrossRef]
- Shaaban, R.; Ghazy, R.M.; Elsherif, F.; Ali, N.; Yakoub, Y.; Aly, M.O.; ElMakhzangy, R.; Abdou, M.S.; McKinna, B.; Elzorkany, A.M.; et al. COVID-19 Vaccine Acceptance among Social Media Users: A Content Analysis, Multi-Continent Study. Int. J. Environ. Res. Public Health 2022, 19, 5737. [Google Scholar] [CrossRef]
- Pacific, W.; Hasan, S.A.W. Interim Statement on Booster Doses for COVID-19 Vaccination; WHO: Geneva, Switzerland, 2021; Update. [Google Scholar]
- Jairoun, A.A.; Al-Hemyari, S.S.; El-Dahiyat, F.; Jairoun, M.; Shahwan, M.; Al Ani, M.; Habeb, M.; Babar, Z.-U.-D. Assessing public knowledge, attitudes and determinants of third COVID-19 vaccine booster dose acceptance: Current scenario and future perspectives. J. Pharm. Policy Pract. 2022, 15, 26. [Google Scholar] [CrossRef]
- Patwary, M.M.; Alam, M.A.; Bardhan, M.; Disha, A.S.; Haque, M.Z.; Billah, S.M.; Kabir, M.P.; Browning, M.H.; Rahman, M.M.; Parsa, A.D. COVID-19 Vaccine Acceptance among Low-and Lower-Middle-Income Countries: A Rapid Systematic Review and Meta-Analysis. Vaccines 2022, 10, 427. [Google Scholar] [CrossRef]
- Wang, R.; Zhang, Q.; Ge, J.; Ren, W.; Zhang, R.; Lan, J.; Ju, B.; Su, B.; Yu, F.; Chen, P. Analysis of SARS-CoV-2 variant mutations reveals neutralization escape mechanisms and the ability to use ACE2 receptors from additional species. Immunity 2021, 54, 1611–1621.e5. [Google Scholar] [CrossRef]
- Eysenbach, G.; Wyatt, J. Using the Internet for surveys and health research. J. Med. Internet Res. 2002, 4, e862. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) | |
|---|---|---|
| Sex | Males | 548 (37.3) |
| Females | 920 (62.7) | |
| Age | Mean ± SD (min-max) | 36.53 ± 13.45 (18.0–88.0) |
| Marital status | Single | 596 (40.6) |
| Married | 811 (55.2) | |
| Divorced | 42 (2.9) | |
| Widow | 19 (1.3) | |
| Education | Diploma | 87 (5.9) |
| Secondary education | 171 (11.6) | |
| University students | 705 (48.0) | |
| Postgraduate | 505 (34.4) | |
| Working | I do not work | 186 (12.7) |
| Retired | 50 (3.4) | |
| Students | 293 (20.0) | |
| Working in the medical field | 526 (35.8) | |
| Working outside the medical field | 413 (28.1) | |
| Chronic Disease | Yes | 237 (16.1) |
| No | 1231 (83.9) | |
| Previous COVID-19 infection | Yes | 750 (51.1) |
| No | 718 (48.9) | |
| A relative had a COVID-19 infection | Yes | 1268 (86.4) |
| No | 200 (13.6) | |
| Immunocompromised relative | Yes | 210 (14.3) |
| No | 1258 (85.7) | |
| Dependent (Vaccination) | Total | Accept Vaccination (n = 1093) | Reject Vaccination (n = 375) | p | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||
| Sex | Female | 920 | 658 | 71.5 | 262 | 28.5 | 0.001 |
| Male | 548 | 435 | 79.4 | 113 | 20.6 | ||
| Age | Mean ± SD | 37.5 ± 13.8 | 33.9 ± 12.0 | <0.001 | |||
| Body mass index | Mean ± SD | 26.2 ± 5.5 | 25.6 ± 5.8 | 0.075 | |||
| Marital status | Married | 811 | 630 | 77.7 | 181 | 22.3 | 0.002 |
| Single # | 657 | 463 | 69.6 | 194 | 30.4 | ||
| Education | Secondary education | 171 | 143 | 83.6 | 28 | 16.4 | 0.002 |
| Diploma/Art | 87 | 73 | 83.9 | 14 | 16.1 | ||
| University | 705 | 517 | 73.3 | 188 | 26.7 | ||
| Higher Education | 505 | 360 | 71.3 | 145 | 28.7 | ||
| Previous COVID-19 infection | No | 718 | 560 | 78.0 | 158 | 22.0 | 0.003 |
| Yes | 750 | 533 | 71.1 | 217 | 28.9 | ||
| Immunocompromised relative | No | 1258 | 950 | 75.5 | 308 | 24.5 | 0.028 |
| Yes | 210 | 143 | 68.1 | 67 | 31.9 | ||
| Dependent: Vaccination | Total (n = 1468) | Accept Vaccination | Reject Vaccination | p | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||
| Social media | No | 646 (44.0) | 469 | 72.6 | 177 | 27.4 | 0.166 |
| Yes | 822 (56.0) | 624 | 75.9 | 198 | 24.1 | ||
| Relative and friends | No | 1122 (76.4) | 835 | 74.4 | 287 | 25.6 | 1 |
| Yes | 346 (23.6) | 258 | 74.6 | 88 | 25.4 | ||
| Literature | No | 816 (55.6) | 613 | 75.1 | 203 | 24.9 | 0.551 |
| Yes | 652 (45.4) | 480 | 73.6 | 172 | 26.4 | ||
| Ministry of Health website | No | 863 (58.7) | 375 | 66.6 | 188 | 33.4 | <0.001 |
| Yes | 905 (41.3) | 718 | 79.3 | 187 | 20.7 | ||
| CDC website | No | 681 (46.4) | 854 | 74.0 | 300 | 26.0 | 0.492 |
| Yes | 787 (53.6) | 239 | 76.1 | 75 | 23.9 | ||
| WHO website | No | 1154 (78.6) | 492 | 72.3 | 189 | 27.8 | 0.081 |
| Yes | 314 (21.4) | 601 | 76.34 | 186 | 23.6 | ||
| Other | No | 1452 (98.9) | 1082 | 74.6 | 369 | 25.4 | 0.517 |
| Yes | 17 (1.1) | 11 | 64.7 | 6 | 35.3 | ||
| Dependent: Vaccination | Question/Category | Total | Accept Vaccination | Reject Vaccination | p | Cronbach Alpha | |||
|---|---|---|---|---|---|---|---|---|---|
| n | n | % | n | % | 0.68 | ||||
| Perceived susceptibility | Q1: I think there is a risk of COVID-19 infection | High | 601 | 74 | 12.3 | 527 | 87.7 | <0.001 | 0.65 |
| Low | 387 | 137 | 35.4 | 250 | 64.6 | ||||
| Neutral | 480 | 164 | 34.2 | 316 | 65.8 | ||||
| Q2: I think COVID-19 variants have a higher risk of infection than the existing strains | High | 600 | 93 | 15.5 | 507 | 84.5 | 0.65 | ||
| Low | 447 | 157 | 35.1 | 290 | 64.9 | ||||
| Neutral | 421 | 125 | 29.7 | 296 | 70.3 | ||||
| Perceived severity | Q3: I think COVID-19 infection is a severe disease | High | 709 | 113 | 15.9 | 596 | 84.1 | <0.001 | 0.65 |
| Low | 304 | 127 | 41.8 | 177 | 58.2 | ||||
| Neutral | 455 | 135 | 29.7 | 320 | 70.3 | ||||
| Q4: I agree that COVID-19 variants can cause more severe illness than the existing strains | High | 553 | 112 | 20.3 | 441 | 79.7 | <0.001 | 0.66 | |
| Low | 391 | 138 | 35.3 | 253 | 64.7 | ||||
| Neutral | 524 | 125 | 23.9 | 399 | 76.1 | ||||
| Perceived benefit | Q5: I believe the COVID-19 boosters are effective against early circulating COVID-19 strains | High | 654 | 43 | 6.6 | 611 | 93.4 | <0.001 | 0.63 |
| Low | 399 | 219 | 54.9 | 180 | 45.1 | ||||
| Neutral | 415 | 113 | 27.2 | 302 | 72.8 | ||||
| Q6: I believe the COVID-19 boosters are effective to extend protection against COVID-19 infection. | High | 699 | 54 | 7.7 | 645 | 92.3 | <0.001 | 0.63 | |
| Low | 369 | 221 | 59.9 | 148 | 40.1 | ||||
| Neutral | 400 | 100 | 25.0 | 300 | 75.0 | ||||
| Q7: I believe the COVID-19 boosters are effective against COVID-19 variants | High | 612 | 39 | 6.4 | 573 | 93.6 | <0.001 | 0.63 | |
| Low | 421 | 229 | 54.4 | 192 | 45.6 | ||||
| Neutral | 435 | 107 | 24.6 | 328 | 75.4 | ||||
| Perceived barriers | Q8: I think COVID-19 vaccine boosters are safe | High | 594 | 39 | 6.6 | 555 | 93.4 | <0.001 | 0.65 |
| Low | 426 | 228 | 53.5 | 198 | 46.5 | ||||
| Neutral | 448 | 108 | 24.1 | 340 | 75.9 | ||||
| Q9: I am worried about the serious adverse reaction after vaccination | High | 411 | 197 | 47.9 | 214 | 52.1 | <0.001 | 0.67 | |
| Low | 711 | 98 | 13.8 | 613 | 86.2 | ||||
| Neutral | 346 | 80 | 23.1 | 266 | 76.9 | ||||
| Q10: I know persons had severe side effects after being vaccinated | High | 362 | 158 | 43.6 | 204 | 56.4 | <0.001 | 0.68 | |
| Low | 788 | 126 | 16.0 | 662 | 84.0 | ||||
| Neutral | 318 | 91 | 28.6 | 227 | 71.4 | ||||
| Perceived Efficacy | Q11: It is easy for me to get the COVID-19 vaccine if I wanted to | High | 1056 | 251 | 23.8 | 805 | 76.2 | 0.042 | 0.67 |
| Low | 120 | 35 | 29.2 | 85 | 70.8 | ||||
| Neutral | 292 | 89 | 30.5 | 203 | 69.5 | ||||
| Cues to action | Q12: Did you use to have confirmed or suspected cases in your daily close contacts? | No | 772 | 595 | 77.1 | 177 | 22.9 | 0.018 | 0.70 |
| Yes | 696 | 498 | 71.6 | 198 | 28.4 | ||||
| Q13: Do you know about the following COVID-19 variants? | All Types | 321 | 249 | 77.6 | 72 | 22.4 | 0.257 | 0.73 | |
| Four Types | 115 | 82 | 71.3 | 33 | 28.7 | ||||
| I Don’t Know | 160 | 123 | 76.9 | 37 | 23.1 | ||||
| One Type | 354 | 270 | 76.3 | 84 | 23.7 | ||||
| Three Types | 198 | 144 | 72.7 | 54 | 27.3 | ||||
| Two Types | 320 | 225 | 70.3 | 95 | 29.7 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghazy, R.M.; Abdou, M.S.; Awaidy, S.; Sallam, M.; Elbarazi, I.; Youssef, N.; Fiidow, O.A.; Mehdad, S.; Hussein, M.F.; Adam, M.F.; et al. Acceptance of COVID-19 Vaccine Booster Doses Using the Health Belief Model: A Cross-Sectional Study in Low-Middle- and High-Income Countries of the East Mediterranean Region. Int. J. Environ. Res. Public Health 2022, 19, 12136. https://doi.org/10.3390/ijerph191912136
Ghazy RM, Abdou MS, Awaidy S, Sallam M, Elbarazi I, Youssef N, Fiidow OA, Mehdad S, Hussein MF, Adam MF, et al. Acceptance of COVID-19 Vaccine Booster Doses Using the Health Belief Model: A Cross-Sectional Study in Low-Middle- and High-Income Countries of the East Mediterranean Region. International Journal of Environmental Research and Public Health. 2022; 19(19):12136. https://doi.org/10.3390/ijerph191912136
Chicago/Turabian StyleGhazy, Ramy Mohamed, Marwa Shawky Abdou, Salah Awaidy, Malik Sallam, Iffat Elbarazi, Naglaa Youssef, Osman Abubakar Fiidow, Slimane Mehdad, Mohamed Fakhry Hussein, Mohammed Fathelrahman Adam, and et al. 2022. "Acceptance of COVID-19 Vaccine Booster Doses Using the Health Belief Model: A Cross-Sectional Study in Low-Middle- and High-Income Countries of the East Mediterranean Region" International Journal of Environmental Research and Public Health 19, no. 19: 12136. https://doi.org/10.3390/ijerph191912136
APA StyleGhazy, R. M., Abdou, M. S., Awaidy, S., Sallam, M., Elbarazi, I., Youssef, N., Fiidow, O. A., Mehdad, S., Hussein, M. F., Adam, M. F., Abdullah, F. S. A., Rebai, W. K., Raad, E. B., Hussein, M., Shehata, S. F., Ismail, I. I., Salam, A. A., & Samhouri, D. (2022). Acceptance of COVID-19 Vaccine Booster Doses Using the Health Belief Model: A Cross-Sectional Study in Low-Middle- and High-Income Countries of the East Mediterranean Region. International Journal of Environmental Research and Public Health, 19(19), 12136. https://doi.org/10.3390/ijerph191912136