
Growth Differentiation Factor 15 (GDF-15): A Novel Biomarker Associated with Poorer Respiratory Function in COVID-19

 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of Patients with COVID-19 on Admission
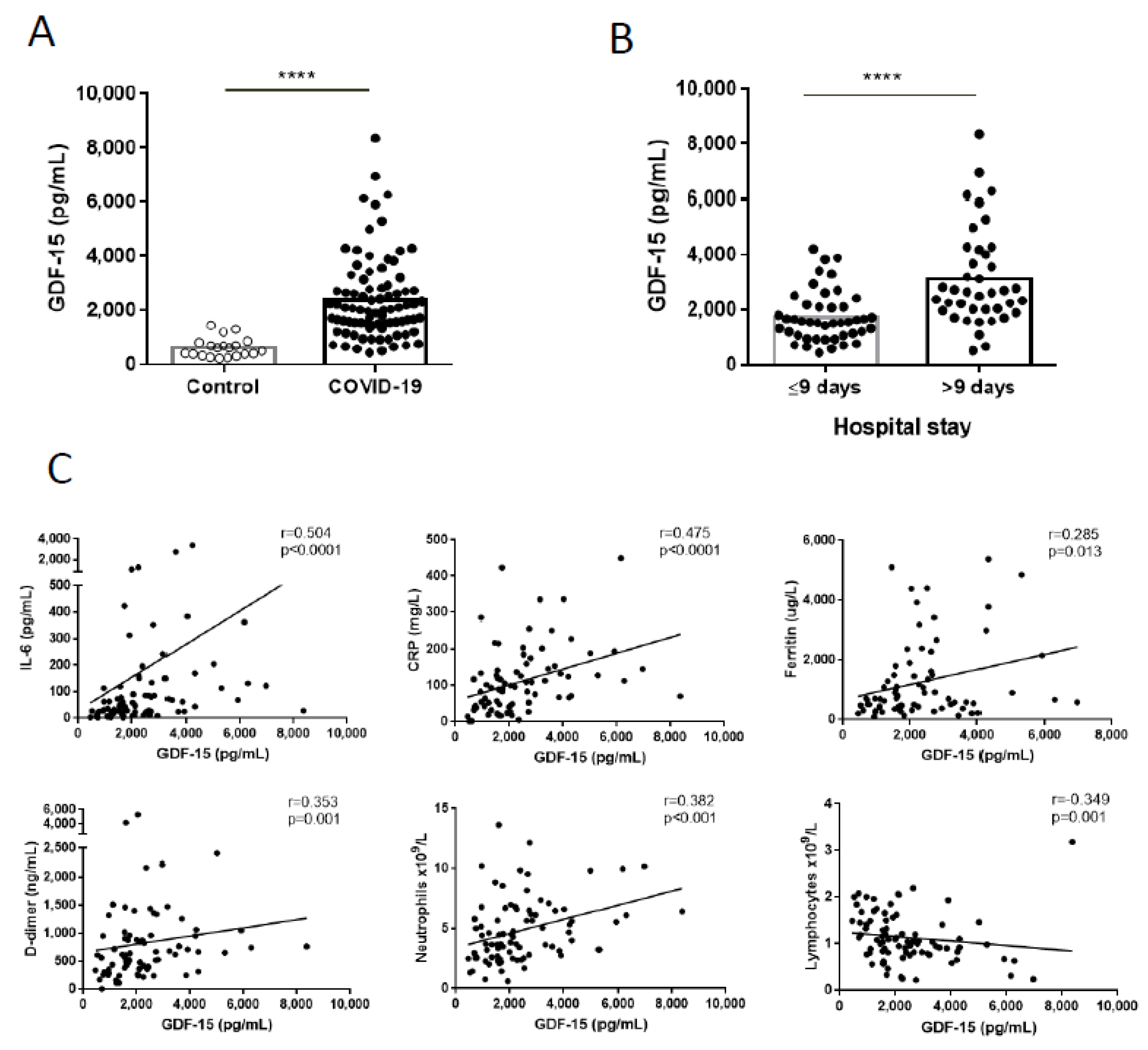
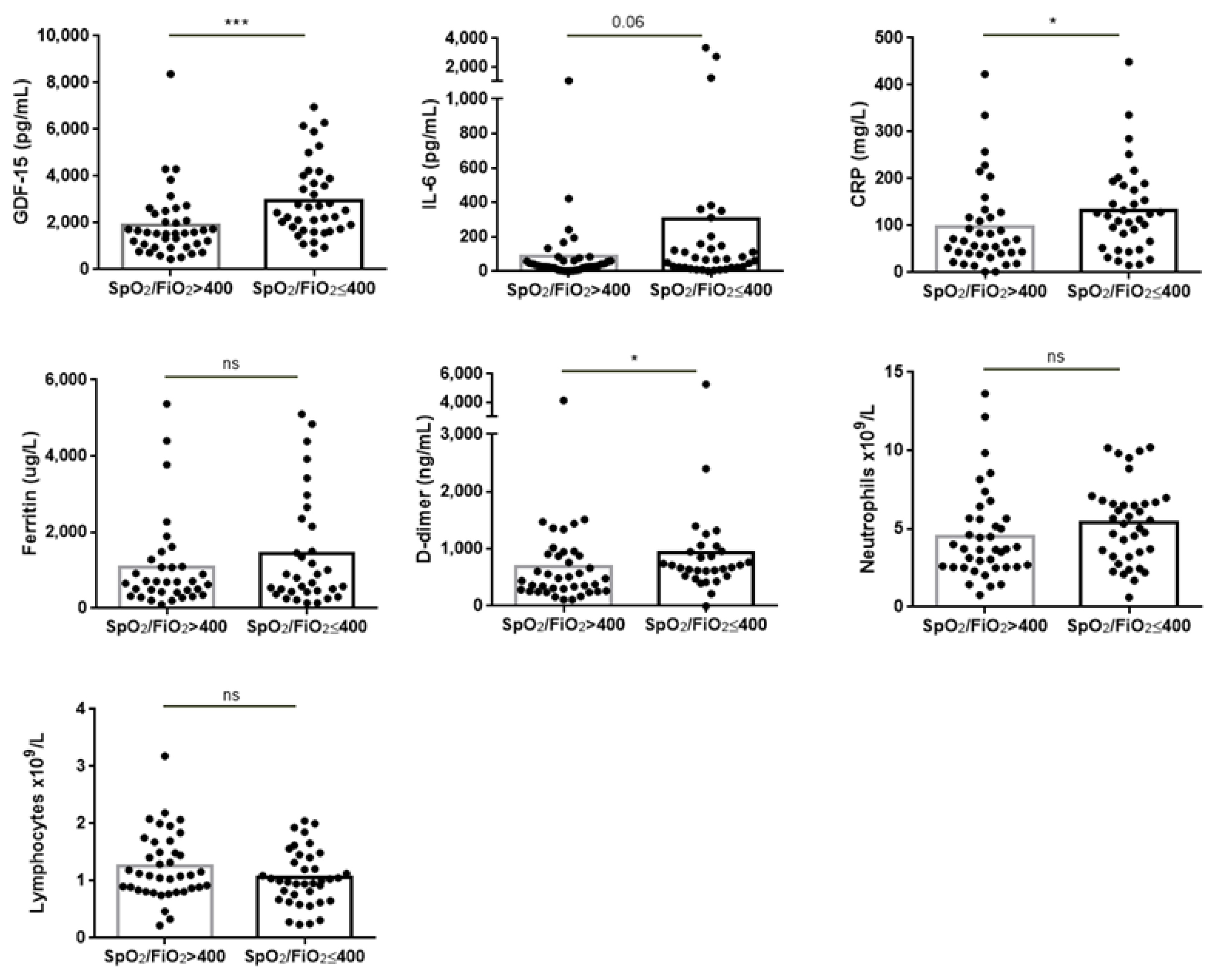
3.2. Association between GDF-15 and Clinical Severity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paces, J.; Strizova, Z.; Smrz, D.; Cerny, J. COVID-19 and the immune system. Physiol. Res. 2020, 9973, 379–388. [Google Scholar] [CrossRef]
- Park, M.D. Macrophages: A Trojan horse in COVID-19? Nat. Rev. Immunol. 2020, 20, 351. [Google Scholar] [CrossRef] [PubMed]
- Ponti, G.; Maccaferri, M.; Ruini, C.; Tomasi, A.; Ozben, T. Biomarkers associated with COVID-19 disease progression. Crit. Rev. Clin. Lab. Sci. 2020, 57, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal Coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wischhusen, J.; Melero, I.; Fridman, W.H. Growth/Differentiation Factor-15 (GDF-15): From Biomarker to Novel Targetable Immune Checkpoint. Front. Immunol. 2020, 11, 951. [Google Scholar] [CrossRef] [PubMed]
- Verhamme, F.M.; Freeman, C.M.; Brusselle, G.; Bracke, K.; Curtis, J.L. GDF-15 in Pulmonary and Critical Care Medicine. Am. J. Respir. Cell Mol. Biol. 2019, 60, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Kempf, T.; Eden, M.; Strelau, J.; Naguib, M.; Willenbockel, C.; Tongers, J.; Heineke, J.; Kotlarz, D.; Xu, J.; Molkentin, J.; et al. The Transforming Growth Factor-β Superfamily Member Growth-Differentiation Factor-15 Protects the Heart from Ischemia/Reperfusion Injury. Circ. Res. 2006, 98, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Notz, Q.; Schmalzing, M.; Wedekink, F.; Schlesinger, T.; Gernert, M.; Herrmann, J.; Sorger, L.; Weismann, D.; Schmid, B.; Sitter, M.; et al. Pro- and Anti-Inflammatory Responses in Severe COVID-19-Induced Acute Respiratory Distress Syndrome—An Observational Pilot Study. Front. Immunol. 2020, 11, 581338. [Google Scholar] [CrossRef] [PubMed]
- Myre, P.L. Growth Differentiation Factor 15 provides prognostic information superior to established cardiovascular and inflammatory biomarkers in unselected patients hospitalized with COVID-19. Circulation 2020, 142, 2128–2137. [Google Scholar] [CrossRef] [PubMed]
- de Guadiana Romualdo, L.G.; Mulero, M.D.R.; Olivo, M.H.; Rojas, C.R.; Arenas, V.R.; Morales, M.G.; Abellán, A.B.; Conesa-Zamora, P.; García-García, J.; Hernández, A.C.; et al. Circulating levels of GDF-15 and calprotectin for prediction of in-hospital mortality in COVID-19 patients: A case series. J. Infect. 2021, 82, e40–e42. [Google Scholar] [CrossRef] [PubMed]
- Rice, T.W.; Wheeler, A.P.; Bernard, G.R.; Hayden, D.L.; Schoenfeld, D.A.; Ware, L.B. Comparison of the SpO2/FiO2 Ratio and the PaO2/FiO2 Ratio in Patients with Acute Lung Injury or ARDS. Chest 2007, 132, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Wiklund, F.E.; Bennet, A.M.; Magnusson, P.; Eriksson, U.K.; Lindmark, F.; Wu, L.; Yaghoutyfam, N.; Marquis, C.; Stattin, P.; Pedersen, N.L.; et al. Macrophage inhibitory cytokine-1 (MIC-1/GDF15): A new marker of all-cause mortality. Aging Cell 2010, 9, 1057–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Yuan, X.; Wang, B.; Gu, R.; Li, W.; Xiang, X.; Tang, L.; Sun, H. Severe Acute Respiratory Syndrome Coronavirus 2: From Gene Structure to Pathogenic Mechanisms and Potential Therapy. Front. Microbiol. 2020, 11, 1576. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Healthy Controls (n = 20) | COVID-19 Patients (n = 84) | |
|---|---|---|
| Female % (n) | 60 (12) | 40.5 (34) |
| Age, years (mean±SD) | 58.6 (±13.9) | 55 (±11.8) |
| Previous pulmonary pathology | ||
| Asthma % (n) | 2.38 (2) | |
| COPD % (n) | 2.38 (2) | |
| Pulmonary malignancy % (n) | 1.19 (1) | |
| Non-specific interstitial pneumonia % (n) | 1.19 (1) | |
| Other comorbidities | ||
| Smoker % (n) | 1.2 (1) | |
| Ex-smoker % (n) | 19 (16) | |
| SAD % (n) | 8.3 (7) | |
| DM % (n) | 11.9 (10) | |
| HT % (n) | 34.5 (29) | |
| DLP % (n) | 27.4 (23) | |
| Laboratory parameters | ||
| IL-6 (pg/mL) | 47.27 (23.61–119.1) | |
| CRP (mg/L) | 92.95 (44.1–145.2) | |
| Ferritin (ug/L) | 695.5 (405–1526) | |
| D-dimer (ng/mL) | 623 (359–958) | |
| Neutrophil count (×109/L) | 4.36 (2.70–6.46) | |
| Lymphocyte count (×109/L) | 1.04 (0.81–1.45) | |
| Ventilation | ||
| Air % (n) | 35.71 (30) | |
| Oxygen requirement % (n) | 60.71 (51) | |
| Invasive ventilation % (n) | 3.57 (3) |
| ROC AUC (95% CI) | p-Value | |
|---|---|---|
| GDF-15 | 0.729 (0.602–0.857) | 0.002 |
| IL-6 | 0.615 (0.466–0.763) | 0.126 |
| CRP | 0.642 (0.498–0.786) | 0.580 |
| Ferritin | 0.590 (0.444–0.736) | 0.230 |
| D-dimer | 0.671 (0.535–0.807) | 0.230 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alserawan, L.; Peñacoba, P.; Orozco Echevarría, S.E.; Castillo, D.; Ortiz, E.; Martínez-Martínez, L.; Moga Naranjo, E.; Domingo, P.; Castellví, I.; Juárez, C.; et al. Growth Differentiation Factor 15 (GDF-15): A Novel Biomarker Associated with Poorer Respiratory Function in COVID-19. Diagnostics 2021, 11, 1998. https://doi.org/10.3390/diagnostics11111998
Alserawan L, Peñacoba P, Orozco Echevarría SE, Castillo D, Ortiz E, Martínez-Martínez L, Moga Naranjo E, Domingo P, Castellví I, Juárez C, et al. Growth Differentiation Factor 15 (GDF-15): A Novel Biomarker Associated with Poorer Respiratory Function in COVID-19. Diagnostics. 2021; 11(11):1998. https://doi.org/10.3390/diagnostics11111998
Chicago/Turabian StyleAlserawan, Leticia, Patricia Peñacoba, Sandra Elizabet Orozco Echevarría, Diego Castillo, Esther Ortiz, Laura Martínez-Martínez, Esther Moga Naranjo, Pere Domingo, Ivan Castellví, Cándido Juárez, and et al. 2021. "Growth Differentiation Factor 15 (GDF-15): A Novel Biomarker Associated with Poorer Respiratory Function in COVID-19" Diagnostics 11, no. 11: 1998. https://doi.org/10.3390/diagnostics11111998
APA StyleAlserawan, L., Peñacoba, P., Orozco Echevarría, S. E., Castillo, D., Ortiz, E., Martínez-Martínez, L., Moga Naranjo, E., Domingo, P., Castellví, I., Juárez, C., & Mariscal, A. (2021). Growth Differentiation Factor 15 (GDF-15): A Novel Biomarker Associated with Poorer Respiratory Function in COVID-19. Diagnostics, 11(11), 1998. https://doi.org/10.3390/diagnostics11111998