
Longitudinal Analysis of Antiphospholipid Antibody Dynamics after Infection with SARS-CoV-2 or Vaccination with BNT162b2

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. The Induction of aPL during Infection with SARS-CoV-2
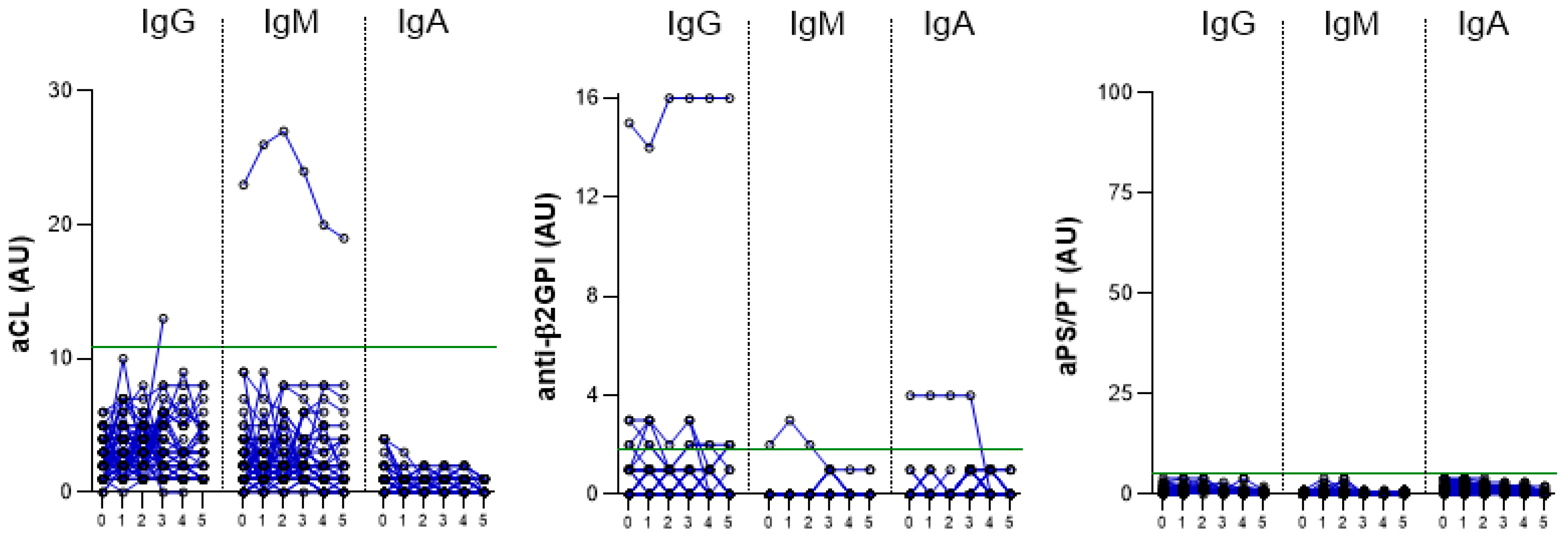
2.2. The Induction of aPL in HCPs after Vaccination
2.3. The Prevalence of aPL in Vaccinated HCPs, COVID-19 and APS Patients
2.4. The aPL Levels in Vaccinated HCPs, COVID-19 and APS Patients
2.5. Clinical Manifestations Related to APS in Vaccinated HCPs and COVID-19 Patients
3. Discussion
4. Materials and Methods
4.1. Study Design and Participants
4.2. Laboratory Tests
4.3. Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Oliver, S.E.; Gargano, J.W.; Marin, M.; Wallace, M.; Curran, K.G.; Chamberland, M.; McClung, N.; Campos-Outcalt, D.; Morgan, R.L.; Mbaeyi, S.; et al. The Advisory Committee on Immunization Practices’ Interim Recommendation for Use of Pfizer-BioNTech COVID-19 Vaccine—United States, December 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 1922–1924. [Google Scholar] [CrossRef] [PubMed]
- Cavalli, E.; Bramanti, A.; Ciurleo, R.; Tchorbanov, A.I.; Giordano, A.; Fagone, P.; Belizna, C.; Bramanti, P.; Shoenfeld, Y.; Nicoletti, F. Entangling COVID-19 associated thrombosis into a secondary antiphospholipid antibody syndrome: Diagnostic and therapeutic perspectives (Review). Int. J. Mol. Med. 2020, 46, 903–912. [Google Scholar] [CrossRef] [PubMed]
- Ehrenfeld, M.; Tincani, A.; Andreoli, L.; Cattalini, M.; Greenbaum, A.; Kanduc, D.; Alijotas-Reig, J.; Zinserling, V.; Semenova, N.; Amital, H.; et al. COVID-19 and autoimmunity. Autoimmun. Rev. 2020, 19, 102597. [Google Scholar] [CrossRef]
- Marietta, M.; Coluccio, V.; Luppi, M. COVID-19, coagulopathy and venous thromboembolism: More questions than answers. Intern. Emerg. Med. 2020, 1375–1387. [Google Scholar] [CrossRef]
- Lakota, K.; Perdan-Pirkmajer, K.; Hočevar, A.; Sodin-Semrl, S.; Rotar, Ž.; Čučnik, S.; Žigon, P. COVID-19 in Association With Development, Course, and Treatment of Systemic Autoimmune Rheumatic Diseases. Front. Immunol. 2020, 11, 611318. [Google Scholar] [CrossRef]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; Derksen, R.H.; PG, D.E.G.; Koike, T.; Meroni, P.L.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef]
- Zohoury, N.; Bertolaccini, M.L.; Rodriguez-Garcia, J.L.; Shums, Z.; Ateka-Barrutia, O.; Sorice, M.; Norman, G.L.; Khamashta, M. Closing the Serological Gap in the Antiphospholipid Syndrome: The Value of “Non-criteria” Antiphospholipid Antibodies. J. Rheumatol. 2017, 44, 1597–1602. [Google Scholar] [CrossRef] [Green Version]
- Žigon, P.; Čučnik, S.; Ambrožič, A.; Sodin Semrl, S.; Kveder, T.; Božič, B. Antibodies to phosphatidylserine/prothrombin complex as an additional diagnostic marker of APS? Lupus 2012, 21, 790–792. [Google Scholar] [CrossRef]
- Žigon, P.; Podovšovnik, A.; Ambrožič, A.; Tomšič, M.; Hočevar, A.; Gašperšič, N.; Rotar, Ž.; Praprotnik, S.; Šemrl, S.S.; Čučnik, S. Added value of non-criteria antiphospholipid antibodies for antiphospholipid syndrome: Lessons learned from year-long routine measurements. Clin. Rheumatol. 2019, 38, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Cervera, R.; Asherson, R.A.; Acevedo, M.L.; Gomez-Puerta, J.A.; Espinosa, G.; De La Red, G.; Gil, V.; Ramos-Casals, M.; Garcia-Carrasco, M.; Ingelmo, M.; et al. Antiphospholipid syndrome associated with infections: Clinical and microbiological characteristics of 100 patients. Ann. Rheum. Dis. 2004, 63, 1312–1317. [Google Scholar] [CrossRef] [PubMed]
- Gkrouzman, E.; Barbhaiya, M.; Erkan, D.; Lockshin, M.D. Reality Check on Antiphospholipid Antibodies in COVID-19-Associated Coagulopathy. Arthritis Rheumatol. 2021, 73, 173–174. [Google Scholar] [CrossRef] [PubMed]
- Bertin, D.; Brodovitch, A.; Beziane, A.; Hug, S.; Bouamri, A.; Mege, J.L.; Heim, X.; Bardin, N. Anticardiolipin IgG Autoantibody Level Is an Independent Risk Factor for COVID-19 Severity. Arthritis Rheumatol. 2020, 72, 1953–1955. [Google Scholar] [CrossRef]
- Devreese, K.M.J.; Linskens, E.A.; Benoit, D.; Peperstraete, H. Antiphospholipid antibodies in patients with COVID-19: A relevant observation? J. Thromb. Haemost. 2020, 18, 2191–2201. [Google Scholar] [CrossRef] [PubMed]
- Taha, M.; Samavati, L. Antiphospholipid antibodies in COVID-19: A meta-analysis and systematic review. RMD Open 2021, 7, e001580. [Google Scholar] [CrossRef]
- Novelli, L.; Motta, F.; De Santis, M.; Ansari, A.A.; Gershwin, M.E.; Selmi, C. The JANUS of chronic inflammatory and autoimmune diseases onset during COVID-19—A systematic review of the literature. J. Autoimmun. 2021, 117, 102592. [Google Scholar] [CrossRef]
- Favaloro, E.J.; Henry, B.M.; Lippi, G. COVID-19 and Antiphospholipid Antibodies: Time for a Reality Check? Semin. Thromb. Hemost. 2022, 48, 72–92. [Google Scholar] [CrossRef]
- Vojdani, A.; Vojdani, E.; Kharrazian, D. Reaction of Human Monoclonal Antibodies to SARS-CoV-2 Proteins With Tissue Antigens: Implications for Autoimmune Diseases. Front. Immunol. 2020, 11, 617089. [Google Scholar] [CrossRef]
- Kanduc, D.; Shoenfeld, Y. Molecular mimicry between SARS-CoV-2 spike glycoprotein and mammalian proteomes: Implications for the vaccine. Immunol. Res. 2020, 68, 310–313. [Google Scholar] [CrossRef]
- Burja, B.; Hočevar, A.; Šekoranja, D.; Živec, K.; Rotar, Ž.; Shoenfeld, Y.; Praprotnik, S. PR3-ANCA vasculitis as manifestation of ASIA syndrome following aesthetic breast augmentation: A new kid on the block? Clin. Exp. Rheumatol. 2022, 40, 865–866. [Google Scholar] [CrossRef]
- Talotta, R. Do COVID-19 RNA-based vaccines put at risk of immune-mediated diseases? In reply to “potential antigenic cross-reactivity between SARS-CoV-2 and human tissue with a possible link to an increase in autoimmune diseases”. Clin. Immunol. 2021, 224, 108665. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- La Cava, A. Antiphospholipid antibodies and COVID-19. Autoimmun. Rev. 2021, 20, 102910. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.; Estes, S.K.; Ali, R.A.; Gandhi, A.A.; Yalavarthi, S.; Shi, H.; Sule, G.; Gockman, K.; Madison, J.A.; Zuo, M.; et al. Prothrombotic autoantibodies in serum from patients hospitalized with COVID-19. Sci. Transl. Med. 2020, 12. [Google Scholar] [CrossRef]
- Trahtemberg, U.; Rottapel, R.; Dos Santos, C.C.; Slutsky, A.S.; Baker, A.; Fritzler, M.J. Anticardiolipin and other antiphospholipid antibodies in critically ill COVID-19 positive and negative patients. Ann. Rheum. Dis. 2021, 80, 1236–1240. [Google Scholar] [CrossRef]
- Knight, J.S.; Caricchio, R.; Casanova, J.L.; Combes, A.J.; Diamond, B.; Fox, S.E.; Hanauer, D.A.; James, J.A.; Kanthi, Y.; Ladd, V.; et al. The intersection of COVID-19 and autoimmunity. J. Clin. Investig. 2021, 131, e154886. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with COVID-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef]
- Serrano, M.; Espinosa, G.; Serrano, A.; Cervera, R. COVID-19 and the antiphospholipid syndrome. Autoimmun. Rev. 2022, 21, 103206. [Google Scholar] [CrossRef]
- Khawaja, M.; Magder, L.; Goldman, D.; Petri, M.A. Loss of antiphospholipid antibody positivity post-thrombosis in SLE. Lupus Sci. Med. 2020, 7, e000423. [Google Scholar] [CrossRef]
- Espinosa, G.; Zamora-Martínez, C.; Pérez-Isidro, A.; Neto, D.; Bravo-Gallego, L.Y.; Prieto-González, S.; Viñas, O.; Moreno-Castaño, A.B.; Ruiz-Ortiz, E.; Cervera, R. Persistent Antiphospholipid Antibodies Are Not Associated With Worse Clinical Outcomes in a Prospective Cohort of Hospitalised Patients With SARS-CoV-2 Infection. Front. Immunol. 2022, 13, 911979. [Google Scholar] [CrossRef] [PubMed]
- Arcani, R.; Cauchois, R.; Suchon, P.; Weber, S.; Jean, R.; Jarrot, P.-A.; Rey, L.; Venton, G.; Koubi, M.; Muller, R.; et al. “True” Antiphospholipid Syndrome in COVID-19: Contribution of the Follow-up of Antiphospholipid Autoantibodies. Semin. Thromb. Hemost. 2022; online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Forastiero, R. Multiple antiphospholipid antibodies positivity and antiphospholipid syndrome criteria re-evaluation. Lupus 2014, 23, 1252–1254. [Google Scholar] [CrossRef] [PubMed]
- Pengo, V.; Ruffatti, A.; Legnani, C.; Testa, S.; Fierro, T.; Marongiu, F.; De Micheli, V.; Gresele, P.; Tonello, M.; Ghirarduzzi, A.; et al. Incidence of a first thromboembolic event in asymptomatic carriers of high-risk antiphospholipid antibody profile: A multicenter prospective study. Blood 2011, 118, 4714–4718. [Google Scholar] [CrossRef] [Green Version]
- Ruffatti, A.; Del Ross, T.; Ciprian, M.; Bertero, M.T.; Sciascia, S.; Scarpato, S.; Montecucco, C.; Rossi, S.; Caramaschi, P.; Biasi, D.; et al. Risk factors for a first thrombotic event in antiphospholipid antibody carriers: A prospective multicentre follow-up study. Ann. Rheum. Dis. 2011, 70, 1083–1086. [Google Scholar] [CrossRef] [PubMed]
- Dabit, J.Y.; Valenzuela-Almada, M.O.; Vallejo-Ramos, S.; Duarte-García, A. Epidemiology of Antiphospholipid Syndrome in the General Population. Curr. Rheumatol. Rep. 2022, 23, 85. [Google Scholar] [CrossRef]
- Borghi, M.O.; Bombaci, M.; Bodio, C.; Lonati, P.A.; Gobbini, A.; Lorenzo, M.; Torresani, E.; Dubini, A.; Bulgarelli, I.; Solari, F.; et al. Anti-Phospholipid Antibodies and Coronavirus Disease 2019: Vaccination Does Not Trigger Early Autoantibody Production in Healthcare Workers. Front Immunol 2022, 13, 930074. [Google Scholar] [CrossRef]
- Noureldine, H.A.; Maamari, J.; El Helou, M.O.; Chedid, G.; Farra, A.; Husni, R.; Mokhbat, J.E. The effect of the BNT162b2 vaccine on antinuclear antibody and antiphospholipid antibody levels. Immunol. Res. 2022, 70, 800–810. [Google Scholar] [CrossRef]
- Thurm, C.; Reinhold, A.; Borucki, K.; Kahlfuss, S.; Feist, E.; Schreiber, J.; Reinhold, D.; Schraven, B. Homologous and Heterologous Anti-COVID-19 Vaccination Does Not Induce New-Onset Formation of Autoantibodies Typically Accompanying Lupus Erythematodes, Rheumatoid Arthritis, Celiac Disease and Antiphospholipid Syndrome. Vaccines 2022, 10, 333. [Google Scholar] [CrossRef]
- Gatto, M.; Agmon-Levin, N.; Soriano, A.; Manna, R.; Maoz-Segal, R.; Kivity, S.; Doria, A.; Shoenfeld, Y. Human papillomavirus vaccine and systemic lupus erythematosus. Clin. Rheumatol. 2013, 32, 1301–1307. [Google Scholar] [CrossRef]
- Segal, Y.; Dahan, S.; Calabrò, M.; Kanduc, D.; Shoenfeld, Y. HPV and systemic lupus erythematosus: A mosaic of potential crossreactions. Immunol. Res. 2017, 65, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, B.; Poddighe, D.; Vadalà, M.; Laurino, C.; Carnovale, C.; Clementi, E. Severe somatoform and dysautonomic syndromes after HPV vaccination: Case series and review of literature. Immunol. Res. 2017, 65, 106–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toplak, N.; Kveder, T.; Trampus-Bakija, A.; Subelj, V.; Cucnik, S.; Avcin, T. Autoimmune response following annual influenza vaccination in 92 apparently healthy adults. Autoimmun. Rev. 2008, 8, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Khamaisi, M.; Shoenfeld, Y.; Orbach, H. Guillain-Barré syndrome following hepatitis B vaccination. Clin. Exp. Rheumatol. 2004, 22, 767–770. [Google Scholar] [PubMed]
- Squeri, F. HPV vaccine and autoimmune diseases: Systematic review and meta-analysis of the literature. J. Prev. Med. Hyg. 2018, 59, E194–E199. [Google Scholar] [CrossRef]
- Watanabe, T.; Minaga, K.; Hara, A.; Yoshikawa, T.; Kamata, K.; Kudo, M. Case Report: New-Onset Rheumatoid Arthritis Following COVID-19 Vaccination. Front. Immunol. 2022, 13, 859926. [Google Scholar] [CrossRef]
- Suzuki, M.; Sekiguchi, Y.; Sasaki, M.; Inaba, S.; Oyama, S.; Inoue, Y.; Warabi, M.; Ohashi, K.; Inoshita, S. Antineutrophil Cytoplasmic Antibody-associated Vasculitis after COVID-19 Vaccination with Pfizer-BioNTech. Intern. Med. 2022, 61, 2925–2929. [Google Scholar] [CrossRef]
- Shakoor, M.T.; Birkenbach, M.P.; Lynch, M. ANCA-Associated Vasculitis Following Pfizer-BioNTech COVID-19 Vaccine. Am. J. Kidney Dis. 2021, 78, 611–613. [Google Scholar] [CrossRef]
- So, D.; Min, K.W.; Jung, W.Y.; Han, S.W.; Yu, M.Y. Microscopic Polyangiitis Following mRNA COVID-19 Vaccination: A Case Report. J. Korean Med. Sci. 2022, 37, e154. [Google Scholar] [CrossRef]
- Ogrič, M.; Žigon, P.; Podovšovnik, E.; Lakota, K.; Sodin-Semrl, S.; Rotar, Ž.; Čučnik, S. Differences in SARS-CoV-2-Specific Antibody Responses After the First, Second, and Third Doses of BNT162b2 in Naïve and Previously Infected Individuals: A 1-Year Observational Study in Healthcare Professionals. Front. Immunol. 2022, 13, 876533. [Google Scholar] [CrossRef]
- Božič, B.; Kveder, T.; Stegnar, M.; Morosini-Berus, E.; Kos-Golja, M.; Peternel, P.; Rozman, B. Influence of degraded phosphatidylserine on binding of antiphospholipid antibodies. Int. Arch. Allergy Immunol. 1997, 112, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Žigon, P.; Ambrožič, A.; Čučnik, S.; Kveder, T.; Rozman, B.; Božič, B. Modified phosphatidylserine-dependent antiprothrombin ELISA enables identification of patients negative for other antiphospholipid antibodies and also detects low avidity antibodies. Clin. Chem. Lab. Med. 2011, 49, 1573. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group I HCPs | Group II COVID-19 ICU | Group III COVID-19 Non-ICU | Group IV APS | p | |
|---|---|---|---|---|---|
| No. of Participants | 58 | 45 | 89 | 52 | |
| Age (years) | |||||
| Median (IQR), (min–max) | 46 (35–55) (24–64) | 70 (58–78) (42–85) | 62 (52–67) (27–78) | 39 (34–56) (23–80) | p < 0.0001 * HCPs-COVID-19 group II: p < 0.0001, HCPs-COVID-19 group III: p < 0.0001, HCPs-APS: ns, COVID-19 group II-APS: p < 0.0001. COVID-19 group III-APS: p < 0.0001. COVID-19 group II–COVID-19 group III: p = 0.02. |
| Sex (n) | |||||
| Female | 45 | 8 | 31 | 36 | p < 0.0001 ** HCPs-COVID-19 group II: p < 0.0001, HCPs-COVID-19 group III: p < 0.0001, HCPs-APS: ns, COVID-19 group II-APS: p < 0.0001. COVID-19 group III-APS: p < 0.0001. COVID-19 group II-COVID-19 group III: p = 0.04. |
| Male | 13 | 37 | 58 | 16 |
| Group I | Group II | Group III | Group IV | ||||
|---|---|---|---|---|---|---|---|
| HCPs (n = 58) | COVID-19 Patients Hospitalized in ICU (n = 45) | COVID-19 Patients Hospitalized in Non-ICU (n = 89) | APS Patients (n = 52) | ||||
| Time Points | Before Vaccination | After Vaccination * | During Hospitalization | At Hospital Admission | At Hospital Discharge | 3 Months after Discharge | |
| aPL | No. of positive (%) | ||||||
| aCL IgG | 0 | 1 (1.7) | 7 (15.6) | 10 (11.2) | 26 (29.2) | 13 (14.6) | 24 (46.2) |
| aCL IgM | 1 (1.7) | 1 (1.7) | 1 (2.2) | 4 (4.5) | 18 (20.2) | 5 (5.6) | 19 (36.5) |
| aCL IgA | 0 | 0 | 0 | 3 (3.4) | 0 | 0 | 1 (1.9) |
| anti-β2GPI IgG | 5 (8.6) | 7 (12.1) | 3 (6.7) | 10 (11.2) | 7 (7.9) | 5 (5.6) | 22 (42.3) |
| anti-β2GPI IgM | 1 (1.7) | 1 (1.7) | 0 | 1 (1.1) | 1 (1.1) | 3 (3.4) | 9 (17.3) |
| anti-β2GPI IgA | 1 (1.7) | 1 (1.7) | 5 (11.1) | 4 (4.5) | 4 (4.5) | 4 (4.5) | 7 (13.5) |
| aPS/PT IgG | 0 | 0 | 1 (2.2) | 0 | 0 | 0 | 22 (42.3) |
| aPS/PT IgM | 0 | 0 | 0 | 5 (5.6) | 5 (5.6) | 3 (3.4) | 19 (36.5) |
| aPS/PT IgA | 0 | 0 | 5 (11.1) | 1 (1.1) | 3 (3.4) | 1 (1.1) | 15 (28.8) |
| at least one positive aPL | 7 (12.1) | 10 (17.2) | 15 (33.3) | 23 (25.8) | 44 (49.4) | 23 (25.8) | 44 (84.6) |
| single aPL positivity ** | 6 (10.3) | 9 (15.5) | 12 (26.7) | 18 (20.2) | 35 (39.3) | 17 (19.1) | 20 (38.5) |
| double aPL positivity ** | 1 (1.7) | 1 (1.7) | 2 (4.4) | 3 (3.4) | 8 (9.0) | 5 (5.6) | 7 (13.5) |
| triple aPL positivity ** | 0 | 0 | 1 (2.2) | 2 (2.2) | 1 (1.1) | 1 (1.1) | 17 (32.7) |
| Longitudinal Trends between Time Points at Admission, at Hospital Discharge, and at Follow-Up | aCL | Anti-β2GPI | aPS/PT | |
|---|---|---|---|---|
| No. of Samples (%) | No. of Samples (%) | No. of Samples (%) | ||
| Samples negative at all time points | 44 (49.4) | 70 (78.7) | 82 (92.1) | |
| Samples positive at least at one time point | 45 (50.6) | 19 (21.3) | 7 (7.9) | |
| Trend 1: Levels increased during hospitalization and persisted at follow-up | / ‾ | 8 (17.8) | 2 (10.5) | 0 |
| Trend 2: Levels increased during hospitalization and decreased at follow-up | / \ | 25 (55.6) | 1 (5.3) | 1 (14.3) |
| Trend 3: Levels were negative during hospitalization and increased at follow-up | _ / | 7 (15.6) | 3 (15.8) | 0 |
| Trend 4: Levels decreased during hospitalization and remained negative at follow-up | \ _ | 3 (6.7) | 8 (42.1) | 3 (42.9) |
| Trend 5: Levels were positive at all three time points | ‾ ‾ | 2 (4.4) | 3 (15.8) | 2 (28.6) |
| Trend 6: Mixed trend | 0 | 2 (10.5) | 1 (14.3) | |
| HCPs | Autoantibodies that Tested Positive after Vaccination | Time Points | |||||
|---|---|---|---|---|---|---|---|
| Before Vaccination | 3 Weeks after Vaccination | 3 Months after Vaccination | 6 Months after Vaccination | 9 Months after Vaccination | 3 Weeks after the Third Dose | ||
| HCP-60 | aCL IgG (AUG) | 3 | 1 | 4 | 13 | ms | ms |
| HCP-21 | anti-β2GPI IgG (AUG) | 1 | 2 | 1 | 2 | 2 | 2 |
| HCP-65 | anti-β2GPI IgG (AUG) | 1 | 3 | 2 | 3 | 1 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogrič, M.; Žigon, P.; Sodin-Semrl, S.; Zlatković-Švenda, M.; Zdravković, M.; Ovuka, M.; Švec, T.; Lakota, K.; Radšel, P.; Rotar, Ž.; et al. Longitudinal Analysis of Antiphospholipid Antibody Dynamics after Infection with SARS-CoV-2 or Vaccination with BNT162b2. Int. J. Mol. Sci. 2023, 24, 211. https://doi.org/10.3390/ijms24010211
Ogrič M, Žigon P, Sodin-Semrl S, Zlatković-Švenda M, Zdravković M, Ovuka M, Švec T, Lakota K, Radšel P, Rotar Ž, et al. Longitudinal Analysis of Antiphospholipid Antibody Dynamics after Infection with SARS-CoV-2 or Vaccination with BNT162b2. International Journal of Molecular Sciences. 2023; 24(1):211. https://doi.org/10.3390/ijms24010211
Chicago/Turabian StyleOgrič, Manca, Polona Žigon, Snezna Sodin-Semrl, Mirjana Zlatković-Švenda, Marija Zdravković, Milica Ovuka, Tinka Švec, Katja Lakota, Peter Radšel, Žiga Rotar, and et al. 2023. "Longitudinal Analysis of Antiphospholipid Antibody Dynamics after Infection with SARS-CoV-2 or Vaccination with BNT162b2" International Journal of Molecular Sciences 24, no. 1: 211. https://doi.org/10.3390/ijms24010211