
Association between 25-OH Vitamin D Deficiency and COVID-19 Severity in Pregnant Women

 ,
,  ,
,  ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Description of the Cohort and Characteristics of the Study Population
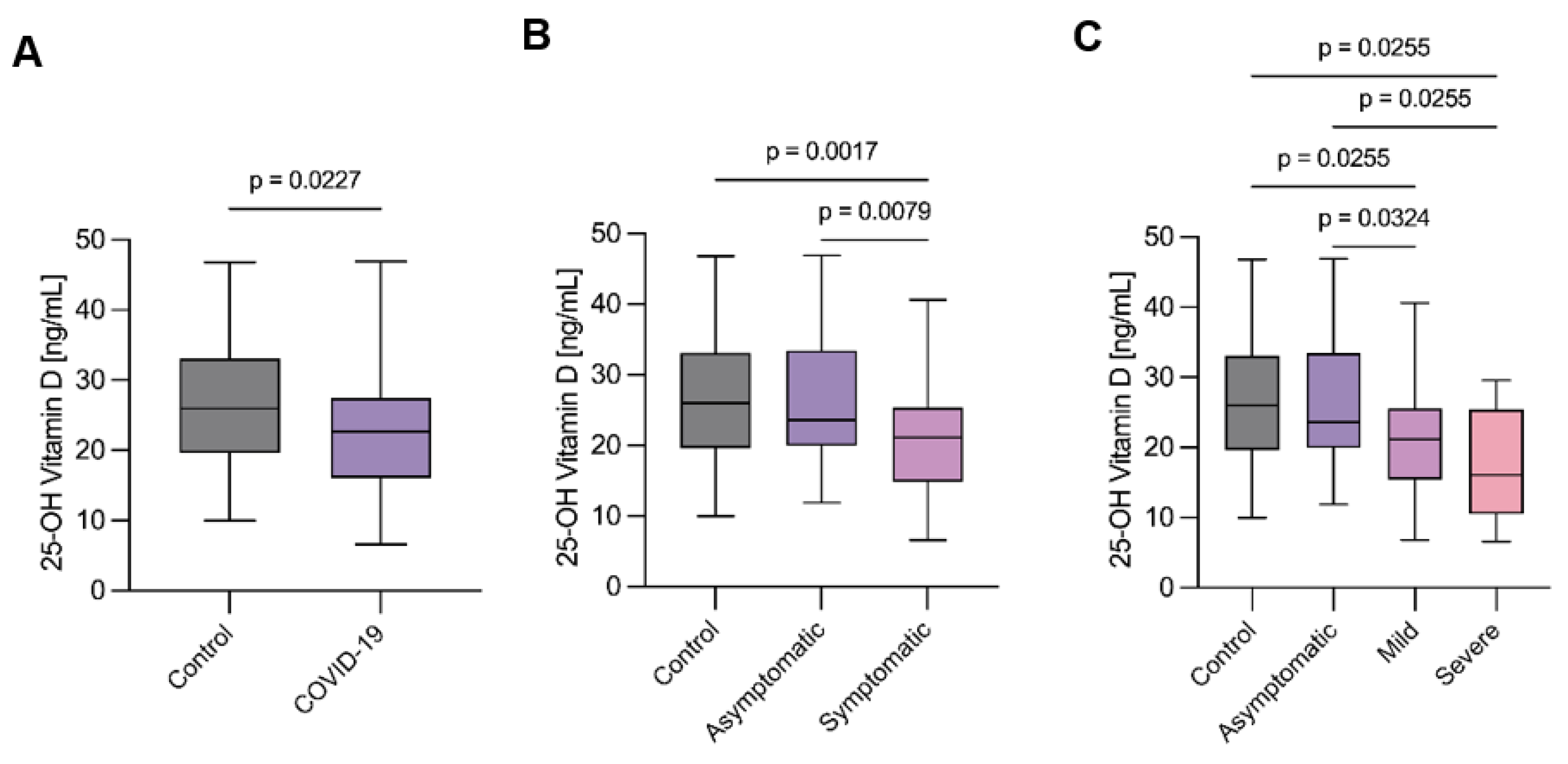
2.2. Vitamin D Status According to COVID-19 Categories
2.3. Distribution of the Patients According to 25-OH Vitamin D Levels
2.4. Association between 25-OH Vitamin D and COVID-19 Severity
2.5. Performance of Lasso Regression Comparable to Traditional Statistical Models
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Quantification of 25-OH Vitamin D
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cui, X.; Zhao, Z.; Zhang, T.; Guo, W.; Guo, W.; Zheng, J.; Zhang, J.; Dong, C.; Na, R.; Zheng, L.; et al. A systematic review and meta-analysis of children with coronavirus disease 2019 (COVID-19). J. Med. Virol. 2021, 93, 1057–1069. [Google Scholar] [CrossRef]
- Dadras, O.; SeyedAlinaghi, S.; Karimi, A.; Shamsabadi, A.; Qaderi, K.; NRamezani, M.; Mirghaderi, S.P.; Mahdiabadi, S.; Vahedi, F.; Saeid, S.; et al. COVID-19 mortality and its predictors in the elderly: A systematic review. Health Sci. Rep. 2022, 5, e657. [Google Scholar] [CrossRef]
- Meyyazhagan, A.; Pushparaj, K.; Balasubramanian, B.; Bhotla, H.K.; Pappusamy, M.; Arumugam, V.A.; Easwaran, M.; Pottail, L.; Mani, P.; Tsibizova, V.; et al. COVID-19 in pregnant women and children: Insights on clinical manifestations, complexities, and pathogenesis. Int. J. Gynaecol. Obstet. 2022, 156, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Mor, G.; Aldo, P.; Alvero, A.B. The unique immunological and microbial aspects of pregnancy. Nat. Rev. Immunol. 2017, 17, 469–482. [Google Scholar] [CrossRef] [PubMed]
- Sappenfield, E.; Jamieson, D.J.; Kourtis, A.P. Pregnancy and susceptibility to infectious diseases. Infect. Dis. Obstet. Gynecol. 2013, 2013, 752852. [Google Scholar] [CrossRef]
- Beigi, R.H. Emerging Infectious Diseases in Pregnancy. Obstet. Gynecol. 2017, 129, 896–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ovies, C.; Semmes, E.C.; Coyne, C.B. Pregnancy influences immune responses to SARS-CoV-2. Sci. Transl. Med. 2021, 13, eabm2070. [Google Scholar] [CrossRef]
- Torres-Torres, J.; Martinez-Portilla, R.J.; Espino Y Sosa, S.; Solis-Paredes, J.M.; Hernández-Pacheco, J.A.; Mateu-Rogell, P.; Cravioto-Sapien, A.; Zamora-Madrazo, A.; Estrada-Gutierrez, G.; Nares-Torices, M.A.; et al. Maternal Death by COVID-19 Associated with Elevated Troponin T Levels. Viruses 2022, 14, 271. [Google Scholar] [CrossRef]
- Wei, S.Q.; Bilodeau-Bertrand, M.; Liu, S.; Auger, N. The impact of COVID-19 on pregnancy outcomes: A systematic review and meta-analysis. CMAJ 2021, 193, E540–E548. [Google Scholar] [CrossRef]
- Metz, T.D.; Clifton, R.G.; Hughes, B.L.; Sandoval, G.J.; Grobman, W.A.; Saade, G.R.; Manuck, T.A.; Longo, M.; Sowles, A.; Clark, K.; et al. Association of SARS-CoV-2 Infection With Serious Maternal Morbidity and Mortality From Obstetric Complications. JAMA 2022, 327, 748–759. [Google Scholar] [CrossRef]
- Vásquez-Procopio, J.; Espejel-Nuñez, A.; Torres-Torres, J.; Martinez-Portilla, R.F.; Espino Y Sosa, S.; Mateu-Rogell, P.; Ortega-Castillo, V.; Tolentino-Dolores, M.; Perichart-Perera, O.; Franco-Gallardo, J.O.; et al. Inflammatory-Metal Profile as a Hallmark for COVID-19 Severity During Pregnancy. Front. Cell Dev. Biol. 2022, 10, 935363. [Google Scholar] [CrossRef]
- Kulda, V. Vitamin D metabolism. Vnitr Lek 2012, 58, 400–404. [Google Scholar]
- DeLuca, H.F. Overview of general physiologic features and functions of vitamin D. Am. J. Clin. Nutr. 2004, 80 (Suppl. 6), 1689s–1696s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ismailova, A.; White, J.H. Vitamin D, infections and immunity. Rev. Endocr. Metab. Disord. 2022, 23, 265–277. [Google Scholar] [CrossRef]
- Umar, M.; Sastry, K.S.; Chouchane, A.I. Role of Vitamin D Beyond the Skeletal Function: A Review of the Molecular and Clinical Studies. Int. J. Mol. Sci. 2018, 19, 1618. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Biol. 2014, 144 Pt A, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Hossein-nezhad, A.; Holick, M.F. Vitamin D for health: A global perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef] [Green Version]
- Kastora, S.; Patel, M.; Carter, B.; Delibegovic, M.; Myint, P.K. Impact of diabetes on COVID-19 mortality and hospital outcomes from a global perspective: An umbrella systematic review and meta-analysis. Endocrinol. Diabetes Metab. 2022, 5, e00338. [Google Scholar] [CrossRef]
- El Mouhayyar, C.; Dewald, J.; Cabrales, J.; Tighiouart, H.; Moraco, A.H.; Jaber, B.L.; Balakrishnan, B.S. Factors Associated with Severity of Acute Kidney Injury and Adverse Outcomes in Critically Ill Patients with COVID-19. Nephron 2022, 1–9. [Google Scholar] [CrossRef]
- Venkatakrishnan, A.J.; Pawlowski, C.; Zemmour, D.; Hughes, T.; Anand, A.; Berner, G.; Kayal, N.; Puranik, A.; Conrad, I.; Bade, S.; et al. Mapping each pre-existing condition’s association to short-term and long-term COVID-19 complications. NPJ Digit. Med. 2021, 4, 117. [Google Scholar] [CrossRef]
- Blaney, G.P.; Albert, P.J.; Proal, A.D. Vitamin D metabolites as clinical markers in autoimmune and chronic disease. Ann. N. Y. Acad. Sci. 2009, 1173, 384–390. [Google Scholar] [CrossRef]
- Holick, F.M.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080s–1086s. [Google Scholar] [CrossRef] [Green Version]
- Pham, H.; Rahman, A.; Majidi, A.; Waterhouse, M.; Neale, R.E. Acute Respiratory Tract Infection and 25-Hydroxyvitamin D Concentration: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3020. [Google Scholar] [CrossRef] [Green Version]
- Ali, N. Role of vitamin D in preventing of COVID-19 infection, progression and severity. J. Infect. Public Health 2020, 13, 1373–1380. [Google Scholar] [CrossRef] [PubMed]
- Merzon, E.; Tworowski, D.; Gorohovski, A.; Vinker, S.; Cohen, A.G.; Green, I.; Frenkel-Morgenstern, M. Low plasma 25(OH) vitamin D level is associated with increased risk of COVID-19 infection: An Israeli population-based study. FEBS J. 2020, 287, 3693–3702. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, D.O.; Best, T.J.; Zhang, H.; Vokes, T.; Arora, V.M.; Solway, J. Association of Vitamin D Levels, Race/Ethnicity, and Clinical Characteristics With COVID-19 Test Results. JAMA Netw. Open 2021, 4, e214117. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.N.; Raju, M.N.P.; da Graca, B.; Wang, D.; Mohamed, N.A.; Mutnal, M.B.; Rao, A.; Bennett, B.; Gokingco, M.; Pham, H.; et al. 25-hydroxyvitamin D is a predictor of COVID-19 severity of hospitalized patients. PLoS ONE 2022, 17, e0268038. [Google Scholar] [CrossRef]
- Ramirez-Sandoval, J.C.; Castillos-Ávalos, V.J.; Paz-Cortés, A.; Santillan-Ceron, A.; Hernandez-Jimenez, S.; Mehta, R.; Correa-Rotter, R. Very Low Vitamin D Levels are a Strong Independent Predictor of Mortality in Hospitalized Patients with Severe COVID-19. Arch. Med. Res. 2022, 53, 215–222. [Google Scholar] [CrossRef]
- Vanegas-Cedillo, P.E.; Bello-Chavolla, O.Y.; Ramírez-Pedraza, N.; Encinas, B.R.; Pérez Carrión, C.I.; Jasso-Ávila, M.I.; Valladares-García, J.C.; Hernández-Juárez, D.; Vargas-Vázquez, A.; Antonio-Villa, N.E.; et al. Serum Vitamin D Levels Are Associated With Increased COVID-19 Severity and Mortality Independent of Whole-Body and Visceral Adiposity. Front. Nutr. 2022, 9, 813485. [Google Scholar] [CrossRef]
- Bae, J.H.; Choe, H.J.; Holick, M.F.; Lim, S. Association of vitamin D status with COVID-19 and its severity: Vitamin D and COVID-19: A narrative review. Rev. Endocr. Metab. Disord. 2022, 23, 579–599. [Google Scholar] [CrossRef]
- Drucker, D.J. Coronavirus Infections and Type 2 Diabetes-Shared Pathways with Therapeutic Implications. Endocr. Rev. 2020, 41, bnaa011. [Google Scholar] [CrossRef]
- Takase, T.; Tsugawa, N.; Sugiyama, T.; Ikesue, H.; Eto, M.; Hashida, T.; Tomii, K.; Muroi, N. Association between 25-hydroxyvitamin D levels and COVID-19 severity. Clin. Nutr. ESPEN 2022, 49, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Mei, K.; Xie, L.; Yuan, P.; Ma, J.; Yu, P.; Zhu, W.; Zheng, C.; Liu, X. Low vitamin D levels do not aggravate COVID-19 risk or death, and vitamin D supplementation does not improve outcomes in hospitalized patients with COVID-19: A meta-analysis and GRADE assessment of cohort studies and RCTs. Nutr. J. 2021, 20, 89. [Google Scholar] [CrossRef] [PubMed]
- Jevalikar, G.; Mithal, A.; Singh, A.; Sharma, R.; Farooqui, K.F.; Mahendru, S.; Dewan, A.; Budhiraja, S. Lack of association of baseline 25-hydroxyvitamin D levels with disease severity and mortality in Indian patients hospitalized for COVID-19. Sci. Rep. 2021, 11, 6258. [Google Scholar] [CrossRef] [PubMed]
- Hastie, C.E.; Mackay, D.F.; Ho, F.; Celis-Morales, C.A.; Katikireddi, S.V.; Niedzwiedz, C.L.; Jani, B.D.; Welsh, P.; Mair, F.S.; Gray, S.R.; et al. Vitamin D concentrations and COVID-19 infection in UK Biobank. Diabetes Metab. Syndr. 2020, 14, 561–565. [Google Scholar] [CrossRef]
- Lin, L.Y.; Mulick, A.; Mathur, R.; Smeeth, L.; Warren-Gash, C.; Langan, S.M. The association between vitamin D status and COVID-19 in England: A cohort study using UK Biobank. PLoS ONE 2022, 17, e0269064. [Google Scholar] [CrossRef]
- Hernández, J.L.; Nan, D.; Fernandez-Ayala, M.; García-Unzueta, M.; Hernández-Hernández, M.A.; López-Hoyos, M.; Muñoz-Cacho, P.; Olmos, J.M.; Gutiérrez-Cuadra, M.; Ruiz-Cubillán, J.J.; et al. Vitamin D Status in Hospitalized Patients with SARS-CoV-2 Infection. J. Clin. Endocrinol. Metab. 2021, 106, e1343–e1353. [Google Scholar] [CrossRef]
- Shin, J.S.; Choi, M.Y.; Longtine, M.S.; Nelson, D.M. Vitamin D effects on pregnancy and the placenta. Placenta 2010, 31, 1027–1034. [Google Scholar] [CrossRef] [Green Version]
- Nema, J.; Sundrani, D.; Joshi, S. Role of vitamin D in influencing angiogenesis in preeclampsia. Hypertens. Pregnancy 2019, 38, 201–207. [Google Scholar] [CrossRef]
- Cyprian, F.; Lefkou, E.; Varoudi, K.; Girardi, G. Immunomodulatory Effects of Vitamin D in Pregnancy and Beyond. Front. Immunol. 2019, 10, 2739. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.Q.; Bilodeau, J.F.; Julien, P.; Luo, Z.C.; Abenhaim, H.A.; Bi, W.G.; Nuyt, A.M.; Leduc, L.; Audibert, F.; Fraser, W.D. Maternal vitamin D, oxidative stress, and pre-eclampsia. Int. J. Gynaecol. Obstet. 2021, 154, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.D.; Pang, T.T.; Li, P.S.; Zhou, Z.X.; Lin, D.X.; Fan, D.Z.; Guo, X.L.; Liu, Z.P. Early pregnancy vitamin D and the risk of adverse maternal and infant outcomes: A retrospective cohort study. BMC Pregnancy Childbirth 2020, 20, 465. [Google Scholar] [CrossRef]
- Mansur, J.L.; Oliveri, B.; Giacoia, E.; Fusaro, D.; Costanzo, P.R. Vitamin D: Before, during and after Pregnancy: Effect on Neonates and Children. Nutrients 2022, 14, 1900. [Google Scholar] [CrossRef]
- Belderbos, M.E.; Houben, M.L.; Wilbrink, B.; Lentjes, E.; Bloemen, E.M.; Kimpen, J.L.L.; Rovers, M.; Bont, L. Cord blood vitamin D deficiency is associated with respiratory syncytial virus bronchiolitis. Pediatrics 2011, 127, e1513–e1520. [Google Scholar] [CrossRef]
- Loy, S.L.; Lek, N.; Yap, F.; Soh, S.E.; Padmapriya, N.; Tan, K.H.; Biswas, A.; Yeo, G.S.H.; Kwek, K.; Gluckman, P.D.; et al. Association of Maternal Vitamin D Status with Glucose Tolerance and Caesarean Section in a Multi-Ethnic Asian Cohort: The Growing Up in Singapore Towards Healthy Outcomes Study. PLoS ONE 2015, 10, e0142239. [Google Scholar] [CrossRef]
- Dobson, R.; Giovannoni, G.; Ramagopalan, S. The month of birth effect in multiple sclerosis: Systematic review, meta-analysis and effect of latitude. J. Neurol. Neurosurg. Psychiatry 2013, 84, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Ergür, A.T.; Berberoğlu, M.; Atasay, B.; Şıklar, Z.; Bilir, P.; Arsan, S.; Söylemez, F.; Öcal, G. Vitamin D deficiency in Turkish mothers and their neonates and in women of reproductive age. J. Clin. Res. Pediatr. Endocrinol. 2009, 1, 266–269. [Google Scholar] [CrossRef]
- Christoph, P.; Challande, P.; Raio, L.; Surbek, D. High prevalence of severe vitamin D deficiency during the first trimester in pregnant women in Switzerland and its potential contributions to adverse outcomes in the pregnancy. Swiss Med. Wkly. 2020, 150, w20238. [Google Scholar] [CrossRef]
- Perichart-Perera, O.; González-Leyva, C.P.; González-Ludlow, I.; Tolentino-Dolores, M.; Solis-Paredes, M.; Reyes-Muñoz, E.; Borboa-Olivares, H.; Sánchez-Martínez, M.; Parra-Hernández, S.; Monterrubio-Flores, E.; et al. Vitamin D Deficiency in Mexican Pregnant Women: Is Supplementation with ≤400 IU/day Enough? Nutrients 2020, 12, 2517. [Google Scholar] [CrossRef] [PubMed]
- Sinaci, S.; Ocal, D.F.; Yetiskin, D.F.Y.; Hendem, D.U.; Buyuk, G.N.; Ayhan, S.G.; Tanacan, A.; Erdinc, A.S.O.; Tekin, O.M.; Sahin, D. Impact of vitamin D on the course of COVID-19 during pregnancy: A case control study. J. Steroid Biochem. Mol. Biol. 2021, 213, 105964. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, G.; Labdouni, S.; Soulimani, R.; Delamare, C.; Bouayed, J. Oxidative stress status and vitamin D levels of asymptomatic to mild symptomatic COVID-19 infections during the third trimester of pregnancy: A retrospective study in Metz, France. J. Med. Virol. 2022, 94, 2167–2173. [Google Scholar] [CrossRef]
- Seven, B.; Gunduz, O.; Erdinc, A.S.O.; Sahin, D.; Tekin, O.M.; Keskin, H.L. Correlation between 25-hydroxy vitamin D levels and COVID-19 severity in pregnant women: A cross-sectional study. J. Matern. Fetal Neonatal Med. 2021, 35, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Tekin, A.B.; Yassa, M.; Birol, P.; Unlu, S.N.; Sahin, T.; Buran, A.M.; Ayanoglu, E.; Tug, N. Vitamin D status is not associated with clinical severity of COVID-19 in pregnant women. Eur. J. Nutr. 2022, 61, 1035–1041. [Google Scholar] [CrossRef]
- Ferrer-Sánchez, N.; Díaz-Goicoechea, M.; Mayoral-Cesar, V.; García-Solbas, S.; Nievas-Soriano, B.J.; Parrón-Carreño, T.; Fernández-Alonso, A.M. Serum 25(OH) Vitamin D Levels in Pregnant Women with Coronavirus Disease 2019 (COVID-19): A Case-Control Study. Int. J. Environ. Res. Public Health 2022, 19, 3965. [Google Scholar] [CrossRef]
- Annweiler, C.; Hanotte, B.; l’Eprevier, C.G.D.; Sabatier, J.M.; Lafaie, L.; Célarier, T. Vitamin D and survival in COVID-19 patients: A quasi-experimental study. J. Steroid Biochem. Mol. Biol. 2020, 204, 105771. [Google Scholar] [CrossRef] [PubMed]
- AlKhafaji, D.; Argan, R.A.; Albaker, Q.; Elq, A.A.; Hariri, M.A.; AlSaid, A.; Alwaheed, A.; Alqatari, S.; Alzaki, A.; Alwarthan, S.; et al. The Impact of Vitamin D Level on the Severity and Outcome of Hospitalized Patients with COVID-19 Disease. Int. J. Gen. Med. 2022, 15, 343–352. [Google Scholar] [CrossRef]
- Bushnaq, T.; Algethami, F.; Qadhi, A.; Mustafa, R.; Ghafouri, K.; Azhar, W.; Malki, A.A. The Impact of Vitamin D Status on COVID-19 Severity among Hospitalized Patients in the Western Region of Saudi Arabia: A Retrospective Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1901. [Google Scholar] [CrossRef]
- Wei, S.Q.; Qi, H.P.; Luo, Z.C.; Fraser, W.D. Maternal vitamin D status and adverse pregnancy outcomes: A systematic review and meta-analysis. J. Matern. Fetal Neonatal Med. 2013, 26, 889–899. [Google Scholar] [CrossRef]
- Roffe-Vazquez, D.N.; Huerta-Delgado, A.S.; Castillo, E.C.; Villarreal-Calderón, J.R.; Gonzalez-Gil, A.M.; Enriquez, C.; Garcia-Rivas, G.; Elizondo-Montemayor, L. Correlation of Vitamin D with Inflammatory Cytokines, Atherosclerotic Parameters, and Lifestyle Factors in the Setting of Heart Failure: A 12-Month Follow-Up Study. Int. J. Mol. Sci. 2019, 20, 5811. [Google Scholar] [CrossRef] [Green Version]
- Tiwari, S.; Pratyush, D.D.; Gupta, S.K.; Singh, S.K. Vitamin D deficiency is associated with inflammatory cytokine concentrations in patients with diabetic foot infection. Br. J. Nutr. 2014, 112, 1938–1943. [Google Scholar] [CrossRef]
- Hewison, M. Vitamin D and immune function: Autocrine, paracrine or endocrine? Scand. J. Clin. Lab. Investig. Suppl. 2012, 243, 92–102. [Google Scholar]
- Rastogi, A.; Bhansali, A.; Khare, N.; Suri, V.; Yaddanapudi, N.; Sachdeva, N.; Puri, G.D. Short term, high-dose vitamin D supplementation for COVID-19 disease: A randomised, placebo-controlled, study (SHADE study). Postgrad. Med. J. 2022, 98, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Annweiler, C.; Beaudenon, M.; Simon, R.; Guenet, M.; Otekpo, M.; Célarier, T.; Gautier, J. Vitamin D supplementation prior to or during COVID-19 associated with better 3-month survival in geriatric patients: Extension phase of the GERIA-COVID study. J. Steroid Biochem. Mol. Biol. 2021, 213, 105958. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Zuno, G.A.; González-Estevez, G.; Matuz-Flores, M.G.; Macedo-Ojeda, G.; Hernández-Bello, J.; Mora-Mora, J.C.; Pérez-Guerrero, E.E.; García-Chagollán, M.; Vega-Magaña, N.; Turrubiates-Hernández, F.J.; et al. Vitamin D Levels in COVID-19 Outpatients from Western Mexico: Clinical Correlation and Effect of Its Supplementation. J. Clin. Med. 2021, 10, 2378. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Camargo, A.C., Jr.; Sluyter, J.D.; Aglipay, M.; Aloia, J.F.; Ganmaa, D.; Bergman, P.; Ferrari, H.A.B.; Borzutzky, A.; Damsgaard, C.T.; et al. Vitamin D supplementation to prevent acute respiratory infections: A systematic review and meta-analysis of aggregate data from randomised controlled trials. Lancet Diabetes Endocrinol. 2021, 9, 276–292. [Google Scholar] [CrossRef]
- Maugeri, A.; Barchitta, M.; Blanco, I.; Agodi, A. Effects of Vitamin D Supplementation During Pregnancy on Birth Size: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2019, 11, 442. [Google Scholar] [CrossRef] [Green Version]
- Palacios, C.; Kostiuk, L.K.; Peña-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2019, 7, Cd008873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguilar-Cordero, M.J.; Lasserrot-Cuadrado, A.; Mur-Villar, N.; León-Ríos, X.A.; Rivero-Blanco, T.; Pérez-Castillo, I.M. Vitamin D, preeclampsia and prematurity: A systematic review and meta-analysis of observational and interventional studies. Midwifery 2020, 87, 102707. [Google Scholar] [CrossRef]
- Bui, L.; Zhu, Z.; Hawkins, S.; Cortez-Resendiz, A.; Bellon, A. Vitamin D regulation of the immune system and its implications for COVID-19: A mini review. SAGE Open Med. 2021, 9, 20503121211014073. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, R.T.; Lynch, J.B.; del Rio, C. Mild or Moderate COVID-19. N. Engl. J. Med. 2020, 383, 1757–1766. [Google Scholar] [CrossRef]
- Kucirka, L.M.; Norton, A.; Sheffield, J.S. Severity of COVID-19 in pregnancy: A review of current evidence. Am. J. Reprod. Immunol. 2020, 84, e13332. [Google Scholar] [CrossRef] [PubMed]
- Furqan, M.S.; Siyal, M.Y. Elastic-Net Copula Granger Causality for Inference of Biological Networks. PLoS ONE 2016, 11, e0165612. [Google Scholar] [CrossRef] [PubMed]
- Gong, C.; Zhou, M.; Hu, Y.; Ren, Z.; Ren, J.; Yao, M. Elastic net-based identification of GAMT as potential diagnostic marker for early-stage gastric cancer. Biochem. Biophys. Res. Commun. 2022, 591, 7–12. [Google Scholar] [CrossRef]


{kind=link}
| Variable | COVID-19 Negative (n = 79) | COVID-19 Positive | |||
|---|---|---|---|---|---|
| Asymptomatic (n = 32) | Mild (n = 44) | Severe (n = 10) | p-Value | ||
| Age, median (IQR), years | 29 (25–33) | 31 (24–37) | 30 (27–34) | 31 (28–36) | 0.209 |
| Gestational week, median (IQR) | 38.3 (38.0–38.5) | 38.6 (38.0–39.3) | 38 (35.8–39.0) | 33.3 (28.4–36) | 0.0001 **** |
| Pre-pregnancy BMI (kg/m2), mean ± SD | 27.0 (24.0–30.0) | 28.0 (23.0–32.5) | 28.7 (24.8–31.1) | 28.7 (22.5–35.4) | 0.315 |
| Pre-pregnancy obesity n (%) | 19 (24%) | 9 (28%) | 21 (48%) | 4 (40%) | 0.053 |
| Hypertension, n (%) | 2 (3%) | 3 (9%) | 4 (9.09%) | 1 (10%) | 0.105 |
| Diabetes, n (%) | 1 (1%) | 1 (3%) | 0 | 0 | 0.556 |
| Hypothyroidism, n (%) | 16 (20%) | 6 (18%) | 6 (13%) | 0 | 0.381 |
| Preeclampsia, n (%) | 11 (14%) | 1 (3%) | 4 (9%) | 1 (10%) | 0.371 |
| Gestational diabetes, n (%) | 8 (10%) | 4 (12%) | 6 (13%) | 1 (10%) | 0.670 |
| 25-OH Vitamin D, median (IQR), ng/mL | 26 (19.6–33.1) | 23.6 (19.9–32.8) | 21.1 (15.4–25.4) | 16.1 (11.0–25.2) | 0.003 *** |
| Magnesium, median (IQR), mmol/L | 0.50 (0.44–0.56) | 0.60 (0.52–0.68) | 0.66 (0.56–0.70) | 0.63 (0.55–0.63) | 0.0001 **** |
| Calcium, median (IQR), mmol/L | 1.35 (1.26–1.44) | 1.48 (1.37–1.61) | 1.51 (1.39–1.63) | 1.45 (1.34–1.58) | 0.003 *** |
| Phosphorus, median (IQR), mmol/L | 3.38 (2.95–3.80) | 3.80 (3.22–4.20) | 3.77 (3.00–4.50) | 3.41 (3.00–4.02) | 0.247 |
| Group | COVID-19 Negative n (%) | Asymptomatic COVID-19 n (%) | Mild COVID-19 n (%) | Severe COVID-19 n (%) | p-Value |
|---|---|---|---|---|---|
| Sufficiency ≥ 30 ng/mL | 30 (39%) | 10 (31%) | 6 (14%) | 0 | 0.015 |
| Insufficiency 20–30 ng/mL | 29 (37%) | 14 (44%) | 18 (41%) | 4 (40%) | |
| Deficiency < 20 ng/mL | 20 (25%) | 8 (25%) | 20 (45%) | 6 (60%) |
| Severe COVID-19 | OR | 95% CI | p-Value |
|---|---|---|---|
| 25-OH vitamin D deficiency | 5.818 | 1.108–30.541 | 0.037 |
| BMI | 0.995 | 0.878–1.127 | 0.941 |
| Hypertension | 0.933 | 0.089–9.781 | 0.954 |
| Gestational diabetes | 1.189 | 0.111–12.694 | 0.886 |
| Maternal age | 1.02 | 0.905–1.149 | 0.739 |
| Magnesium | 0.102 | 0.002–36.830 | 0.448 |
| Calcium | 0.307 | 0.003–25.681 | 0.601 |
| Regression Model | Coefficient | 95% CI | p-Value | R2 |
|---|---|---|---|---|
| Logistic | 5.818 | 1.108–30.541 | 0.037 | 0.0818 |
| Lasso | 12.513 | 4.097–20.929 | 0.004 | 0.3289 |
| Regression Model | AUC 95% CI | DR at 10% FPR (95% CI) | DR at 15% FPR (95% CI) |
|---|---|---|---|
| Logistic model | 0.911 (0.849–0.972) | 0.687 (0.244–0.900) | 0.7 (0.400–1.00) |
| Lasso model | 0.895 (0.800–0.991) | 0.444 (0.111–1.000) | 0.667 (0.222–1.000) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vásquez-Procopio, J.; Torres-Torres, J.; Borboa-Olivares, H.; Sosa, S.E.Y.; Martínez-Portilla, R.J.; Solis-Paredes, M.; Tolentino-Dolores, M.-C.; Helguera-Repetto, A.C.; Marrufo-Gallegos, K.C.; Missirlis, F.; et al. Association between 25-OH Vitamin D Deficiency and COVID-19 Severity in Pregnant Women. Int. J. Mol. Sci. 2022, 23, 15188. https://doi.org/10.3390/ijms232315188
Vásquez-Procopio J, Torres-Torres J, Borboa-Olivares H, Sosa SEY, Martínez-Portilla RJ, Solis-Paredes M, Tolentino-Dolores M-C, Helguera-Repetto AC, Marrufo-Gallegos KC, Missirlis F, et al. Association between 25-OH Vitamin D Deficiency and COVID-19 Severity in Pregnant Women. International Journal of Molecular Sciences. 2022; 23(23):15188. https://doi.org/10.3390/ijms232315188
Chicago/Turabian StyleVásquez-Procopio, Johana, Johnatan Torres-Torres, Hector Borboa-Olivares, Salvador Espino Y Sosa, Raigam Jafet Martínez-Portilla, Mario Solis-Paredes, Mari-Cruz Tolentino-Dolores, Addy Cecilia Helguera-Repetto, Karla Cecilia Marrufo-Gallegos, Fanis Missirlis, and et al. 2022. "Association between 25-OH Vitamin D Deficiency and COVID-19 Severity in Pregnant Women" International Journal of Molecular Sciences 23, no. 23: 15188. https://doi.org/10.3390/ijms232315188